

Percutaneous Closure of a Sinus Venosus Defect With Partial Anomalous Pulmonary Venous Return
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
A 73-year-old man with a history of hypertension, hyperlipidemia, and obesity presented for cardiovascular evaluation. He was experiencing mild fatigue and dyspnea on exertion. Transthoracic echocardiogram (TTE) showed right ventricular (RV) dilation, which was otherwise unremarkable. No bubble study was performed. A 7-day cardiac monitor obtained at that time showed 8 occurrences of supraventricular tachycardia with the longest episode of 11 beats. There was no atrial fibrillation.
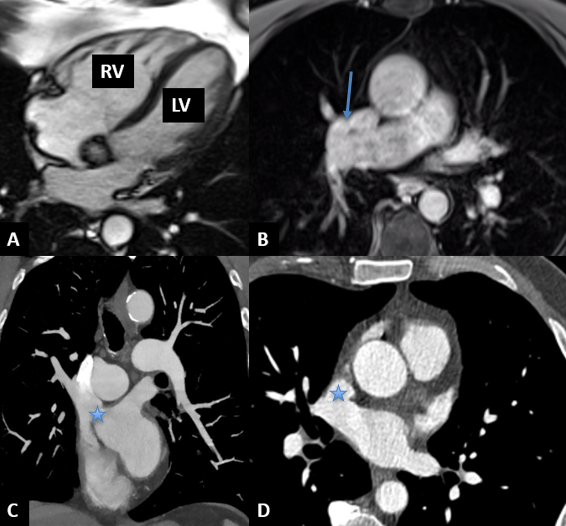
Given the right ventricular dilation shown in the TTE, a cardiac MRI was performed. The MRI showed moderate RV dilation with evidence of partial anomalous pulmonary venous drainage (PAPVR), with the right upper and middle pulmonary veins draining into the superior vena cava (SVC). There was evidence of significant left-to-right shunt with a Qp/Qs of 1.8. Cardiac computed tomography angiogram (CTA) showed a large superior sinus venosus atrial septal defect (SVASD) between the wall of the SVC, and the right middle pulmonary vein measuring 2.6 cm in the superior-inferior dimension and 1.7 cm in the right-left dimension. Right upper and middle pulmonary veins drained into the SVC just above the defect (Figure 1, Video 1). There was normal drainage of the remaining pulmonary veins.
Cardiac catheterization was performed, which revealed a Qp/Qs of 2.0 and confirmed the anomalous pulmonary venous drainage. There was no evidence of pulmonary hypertension, and the pulmonary vascular resistance was normal (1.0 Woods unit).
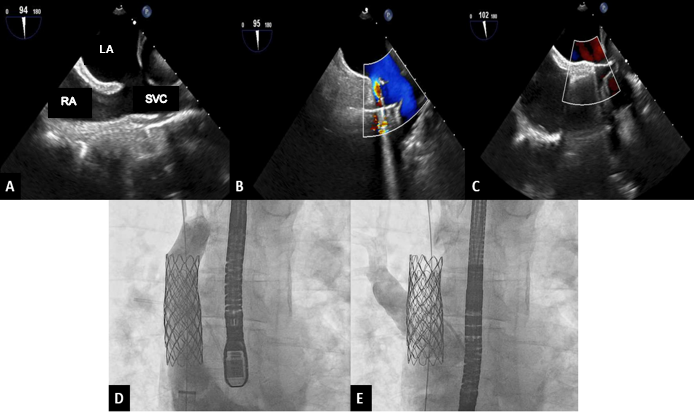
Upon review of the CTA, the defect appeared amenable to percutaneous closure with a covered stent in the SVC. The patient was counseled on options for closure, including surgical repair and a covered stent. Intraoperative TTE again showed the SVASD and anomalous pulmonary venous drainage. Two covered stents were placed; the first stent successfully routed the anomalous veins posteriorly across the defect to the left atrium without pulmonary venous obstruction (Video 2). There was a small residual ASD (4 mm) at the inferior portion of the stent, for which a second stent was placed. There was no residual left-to-right flow after the second stent and no pulmonary venous obstruction (Figure 2; Videos 3 and 4). At 1-month follow-up, the patient was asymptomatic and TTE demonstrated a significant decrease in right ventricular size.
SVASD is a rare variant, accounting for 5% to 10% of all ASDs.1 Surgical repair is the standard of care for SVASD with partial anomalous pulmonary venous drainage, although transcatheter closure has emerged as a feasible alternative to surgery in carefully selected patients. Questions remain about the long-term durability and the possibility of late complications with percutaneous closure.2
Affiliations and Disclosures
From the Zena and Michael A. Wiener Cardiovascular Institute, Icahn School of Medicine at Mount Sinai, New York, NY, USA.
Consent statement: The authors confirm that appropriate informed consent was obtained for the procedures performed, as well as the publication thereof.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Stamatios Lerakis, MD, PhD, Director of Imaging for Structural and Valve Interventions, Icahn School of Medicine at Mount Sinai, New York, NY 10029, USA. Email: Stamatios.Lerakis@mountsinai.org; X: @SWBienMD
References
- Qiu JK, Bamira D, Vainrib AF, et al. Multimodality imaging of sinus venosus atrial septal defect: a challenging diagnosis in adults. CASE (Phila). 2021;6(3):107-113. doi: 10.1016/j.case.2021.12.002
- Baruteau AE, Hascoet S, Malekzadeh-Milani S, et al. Transcatheter closure of superior sinus venosus defects. JACC Cardiovasc Interv. 2023;16(21):2587-2599. doi: 10.1016/j.jcin.2023.07.024










