

Recreating the Crime Scene: A Three-Dimensional Model to Analyze the Mechanism of Orbital Atherectomy-Related Coronary Perforation
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
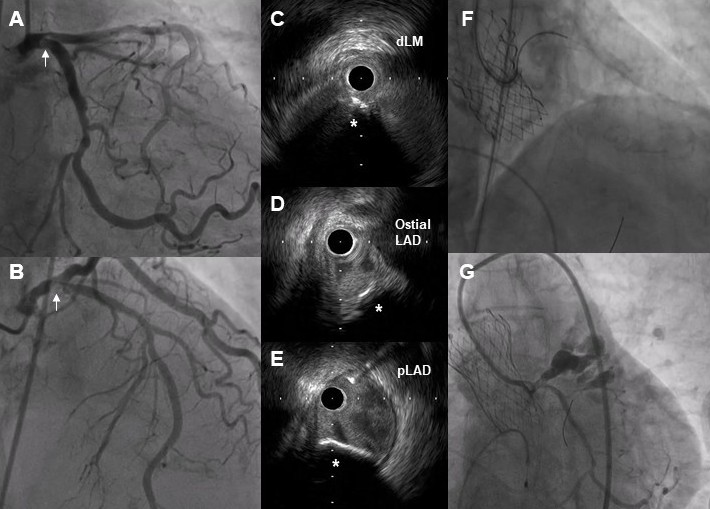
A 77-year-old woman with hypertension and diabetes presented with exertional angina and dyspnea. Subsequent workup showed severe aortic stenosis (AS) and severe calcified stenosis at the proximal left anterior descending artery (pLAD) (Figure 1A and B). After discussion with the heart team, the patient planned to undergo transcatheter aortic valve implantation (TAVI) to tackle the critical AS, followed by percutaneous coronary intervention with atherectomy in the same setting.
Under local anesthesia, a 26-mm Evolut FX+ valve (Medtronic) was implanted from the femoral approach. Subsequently, a 7F Judkins Left 4 guiding catheter engaged the left coronary artery from inside the TAVI valve. Intravascular ultrasound (IVUS) showed a huge calcified nodule extending from distal left main (dLM) to the pLAD (Figure 1C-E). Orbital atherectomy (OA) with a 1.25mm crown was performed from the dLM to the pLAD with two 80K runs antegrade and retrograde, followed by one 120K run antegrade and retrograde (Figure 1F). The patient developed severe hypotension, and contrast injection showed Ellis type III perforation at the pLAD (Figure 1G). Echocardiography confirmed cardiac tamponade, and pericardiocentesis was performed, which yielded fresh blood. Intracoronary balloon tamponade and covered stent implantation failed to achieve hemostasis. Emergency open heart surgery with TAVI explant, Bentall procedure, and coronary bypass were performed. The patient recovered and was discharged 9 days post-procedure.
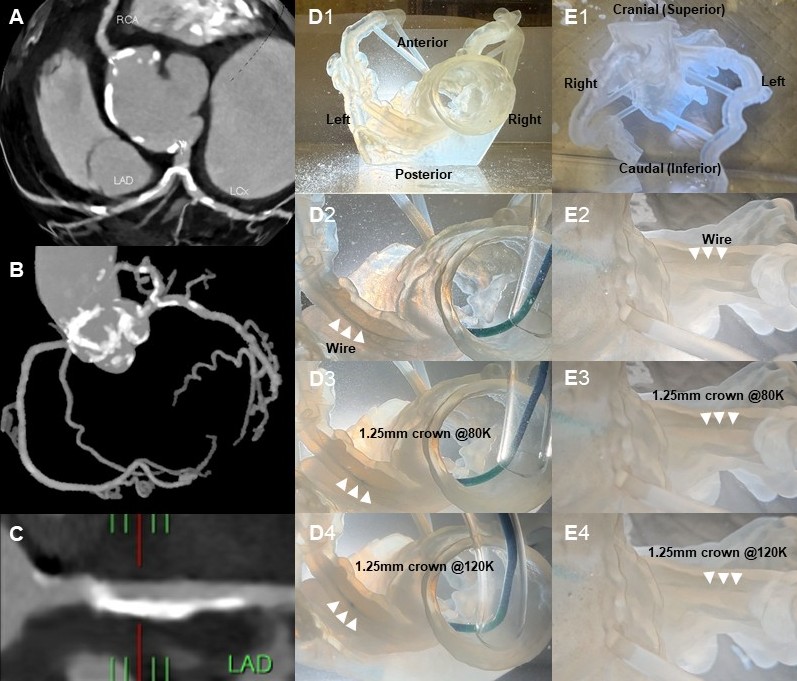
OA is an important tool for management of severe calcified coronary artery disease.1 Coronary perforation related to OA is an uncommon but acute complication. In this case, IVUS showed that the wire was heavily biased against the healthy vessel wall at the pLAD. The trajectory of the crown could cause injury to the vessel wall instead of ablating the calcified nodule.2 Using a coronary computed tomography angiogram (Figure 2A-C), we created a 3D-printed PolyJet heart model (Stratasys) to simulate the OA process. The calcified nodule was located at the infero-anterior side of the dLM to the pLAD, but the wire and OA were biased toward the supero-posterior side of the pLAD (Figure 2D and E, Video). This caused injury to the vessel wall and eventually led to perforation at the corresponding site. This case illustrates the possible mechanism of OA-associated vessel perforation and the importance of IVUS to identify the wire bias to guide atherectomy procedures.
Affiliations and Disclosures
Chor-Cheung Frankie Tam, MBBS1; Simon Lam, MBBS1; Michael Sze, MBBS1; Eric Chan, MBBS1; Chun Ka Wong, MBBS1; Chin Lung Wong, MBBS2; Christian Fang, MBBS2
From the 1Cardiology Division, Department of Medicine, Queen Mary Hospital, University of Hong Kong, Hong Kong SAR, China; 2Department of Orthopedics and Traumatology, Queen Mary Hospital, University of Hong Kong, Hong Kong SAR, China.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention described in the manuscript and for the publication thereof.
Address for correspondence: Chor-Cheung Frankie Tam, MBBS, Cardiology Division, Department of Medicine, The University of Hong Kong, K19, Queen Mary Hospital, 102# Pok Fu Lam Road, Hong Kong, China. Email: frankie.tamcc@gmail.com
References
- Shlofmitz E, Martinsen BJ, Lee M, et al. Orbital atherectomy for the treatment of severely calcified coronary lesions: evidence, technique, and best practices. Expert Rev Med Devices. 2017;14(11):867-879. doi:10.1080/17434440.2017.1384695
- Lee T, Ashikage T, Nozato T, et al. Predictors of coronary artery injury after orbital atherectomy as assessed by optical coherence tomography. Int J Cardiovasc Imaging. 2023;39(7):1367-1374. doi:10.1007/s10554-023-02837-7










