

Skyrocketing Troponin After a Motor Vehicle Crash: A Traumatic Dilemma
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
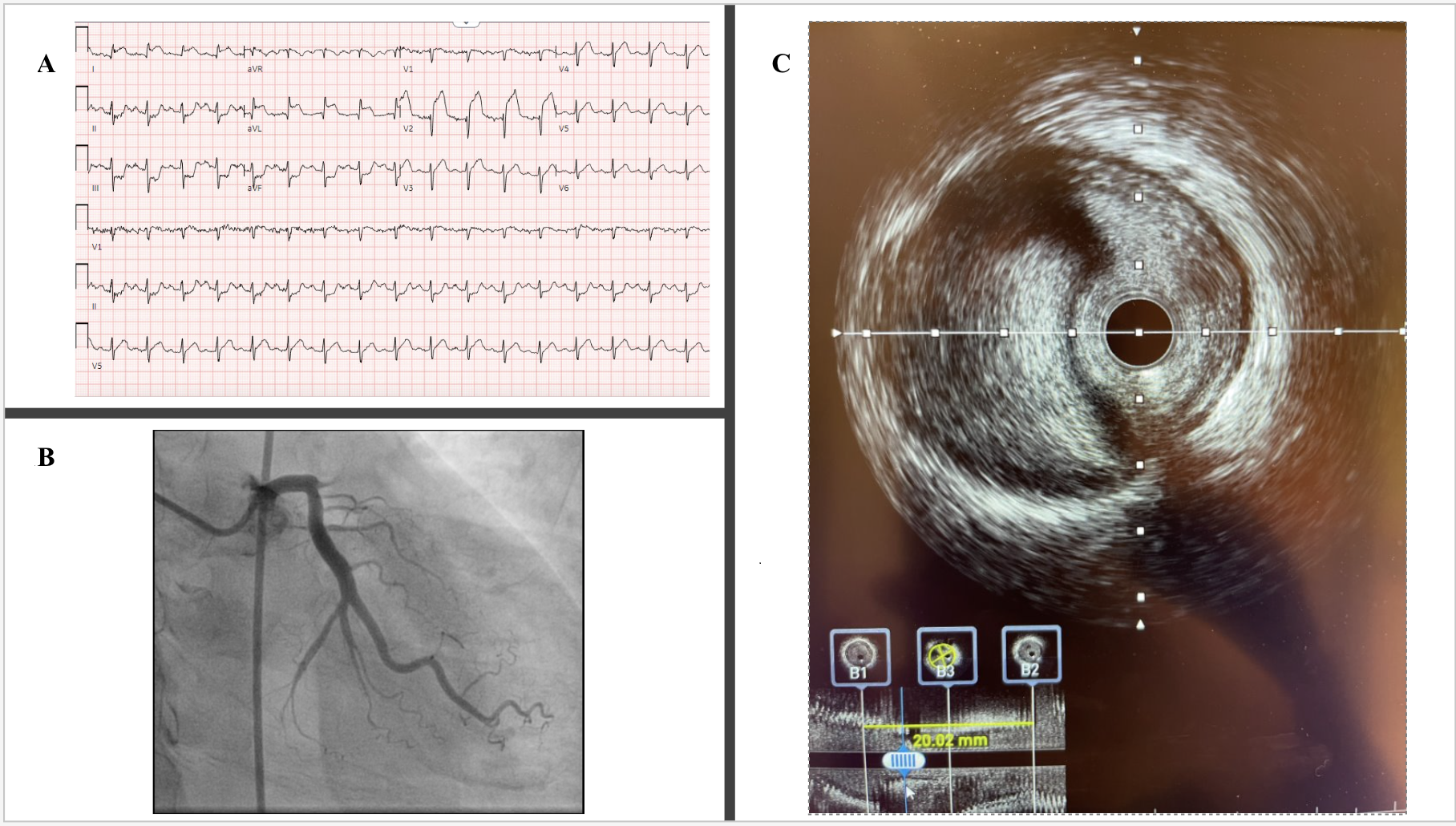
A 54-year-old man presented following a motor vehicle crash that resulted in a subarachnoid hemorrhage (SAH). Electrocardiogram showed anterolateral ST-segment elevations (Figure A). Troponin I was elevated at 3.19 ng/mL, and echocardiogram showed an antero-apical wall-motion abnormality with an ejection fraction of 20% to 25% (Video 1). Anticoagulation and dual antiplatelet therapy for acute coronary syndrome (ACS) were initially withheld given concern for SAH expansion. However, within 8 hours, troponin I rose to 87.20 ng/mL.
After discussion with the neurosurgical team, mono-platelet therapy with 81 mg of aspirin was initiated, and cardiac catheterization was performed via the right femoral artery. Angiography revealed an occluded ostial left anterior descending artery (LAD) (Figure B, Video 2). Given these findings, the patient was given 7000 units of unfractionated heparin and loaded with 600 mg of clopidogrel. The lesion was readily crossed with a wire and dilated with a compliant balloon, restoring Thrombosis in Myocardial Infarction-2 flow and revealing a 95% ostial-to-proximal LAD diffuse stenosis (Video 3). Intravascular ultrasound imaging demonstrated compression of the vessel lumen by an intramural hematoma, confirming a traumatic dissection (Figure C, Video 4). A cutting balloon was used to fenestrate the false lumen. Flow improved but remained suboptimal angiographically; thus, a single drug-eluting stent was deployed (Video 5). Dual-antiplatelet therapy (DAPT) with the addition of 75 mg of clopidogrel daily was started, with no further neurologic sequelae. Post-procedure echocardiogram showed a persistently reduced ejection fraction of 25% to 30%. Guideline-directed medical therapy (GDMT) was initiated, and the patient was discharged home with DAPT for 1 year followed by aspirin monotherapy thereafter. At follow-up in the cardiology clinic, the patient had been tolerating GDMT well and denied experiencing any subsequent angina.
The incidence of traumatic coronary artery dissection due to chest wall trauma is rare, with reported estimates as low as 0.1%.1 It is believed that the sudden dissipation of kinetic energy from the body smashing into an immobile object results in the shearing of the vessel layers.2 Intravascular imaging can prove key in making the diagnosis of traumatic dissection.3 Cutting balloon therapy might reduce the risk of hematoma propagation during stenting. Multidisciplinary collaboration allowed for the management of concurrent traumatic ACS and intracranial bleeding in this trauma patient.
Affiliations and Disclosures
Rahul Annabathula, MD; Rohit Menon, MD; Justin Brilliant, MD; Xin Wei, MD; Mukta Srivastava, MD
From the Division of Cardiovascular Medicine, University of Maryland School of Medicine, Baltimore, Maryland.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention(s) described in this manuscript and to the publication thereof.
Address for correspondence: Rahul Annabathula, MD, Division of Cardiovascular Medicine University of Maryland School of Medicine, 110 South Paca St., 7th Floor, Baltimore, MD 21201, USA. Email: Rannabathula@som.umaryland.edu
References
1. Haywood ST, Patel K, Gallo D, Silver K, Jouriles N. Throws of death: traumatic coronary artery dissection resulting from jiu jitsu training. J Emerg Med. 2020;58(1):63-66. doi:10.1016/j.jemermed.2019.09.037
2. Kurklu HA, Tan TS. Blast injury: a very rare cause of left coronary artery dissection. JACC Case Rep. 2021;3(18):1898-1902. doi:10.1016/j.jaccas.2021.09.015
3. Paulo M, Sandoval J, Lennie V, et al. Combined use of OCT and IVUS in spontaneous coronary artery dissection. JACC Cardiovasc Imaging. 2013;6(7):830-832. doi:10.1016/j.jcmg.2013.02.010











