

Comparison of Catheterization Versus Echocardiographic-Based Gradients in Balloon-Expandable Versus Self-Expanding Transcatheter Aortic Valve Implantation
Abstract
Objectives. In patients with transcatheter aortic valve implantation (TAVI), accurate assessment of gradients is important to assess valve function and durability, which drives clinical decision-making. We sought to evaluate discrepancies in aortic valve mean gradients with balloon-expandable and self-expanding TAVI. Methods. We retrospectively reviewed 507 patients that underwent TAVI and compared mean gradients by catheterization to transthoracic Doppler echocardiography. Results. Mean gradients by Doppler in balloon-expandable (11.0 ± 5.8 mm Hg) and self-expanding devices (8.7 ± 4.5 mm Hg) were significantly higher than catheterization (3.2 ± 4.0 mm Hg vs 3.5 ± 4.1 mm Hg, respectively; P<.001). In a subgroup analysis of skirted valves, Doppler gradients in balloon-expandable (9.8 ± 4.4 mm Hg) and self-expanding devices (8.6 ± 5.1 mm Hg) were significantly higher than catheterization (3.5 ± 4.1 mm Hg vs 4.2 ± 4.8 mm Hg, respectively; P<.001). When the effect of valve size on gradients was analyzed, Doppler gradients were significantly higher than catheterization for all comparisons. When indexed for valve size, patients with large aortas who received a balloon-expandable TAVI had greater pressure differential than those who received a self-expanding TAVI (8.24 ± 0.46 mm Hg vs 5.16 ± 0.66 mm Hg; P<.001). This trend was not seen in patients with a small aorta-to-valve index. Conclusion. Following TAVI, aortic valve mean gradients acquired by Doppler were higher than catheterization and the discrepancy was more pronounced in balloon-expandable than self-expanding prostheses. These differences persist in skirted valves and across valve sizes. These observations may reflect periprocedural hemodynamic changes, differences between prosthetic flow acceleration, and/or pressure recovery.
Keywords: aortic valve disease, diagnostic catheterization, transcatheter valve implantation
Transcatheter aortic valve implantation (TAVI) has transformed the treatment of symptomatic severe aortic stenosis. In recent years, indications for TAVI have expanded to include low and moderate surgical risk patient groups.1-3 Additional randomized controlled studies are currently underway evaluating TAVI in asymptomatic patients with severe aortic stenosis and in patients with moderate aortic stenosis with heart failure.4-6 The long-term durability of TAVI is an active field of study. Recent trial data from a low-risk surgical population who received TAVI signaled increased incidence of valve thrombosis and worsening aortic valve mean gradients after 1 year when compared with surgery.7 Given that TAVI utilization is expected to expand, as well as questions regarding long-term bioprosthetic durability in certain cohorts, obtaining reliable indices of device function and durability is essential for informed clinical decision-making.
Echocardiography is the cornerstone imaging modality for assessing valvular function and serial monitoring is important for surveillance of bioprosthetic valve dysfunction.8 Numerous echocardiography parameters, including mean gradient, peak velocity, dimensionless index, and aortic valve area/index (AVA/AVAi) derived via the continuity principle, among others, reveal important information regarding bioprosthetic function. Additional variables, such as flow, jet eccentricity, and pressure recovery, affect the interpretation of valvular hemodynamics, with the latter factor a recent focus of study.9-12 The reliability of these gradients is important as they often drive clinical decision making, particularly as higher aortic gradients after aortic valve replacement are associated with more biomechanical stress and valve deterioration.13 In this study, we sought to evaluate discrepancies in aortic valve gradients in a large cohort of patients who had undergone TAVI with first- and second-generation balloon-expandable (Sapien; Edwards Lifesciences) and self-expanding valves (CoreValve; Medtronic), derived by invasive and non-invasive means.
Methods
We retrospectively reviewed 507 patients who underwent commercial TAVI between January 2015 and November 2019 at The Ohio State University Wexner Medical Center. TAVI was performed via standard transfemoral approach under conscious sedation or general anesthesia. In a minority of patients (<10 cases), TAVI was performed with an alternate approach, such as subclavian access. Device and size selection were at the discretion of the implanting physicians. Following deployment, invasive gradients by catheterization were obtained via simultaneous recording of left ventricular and ascending aortic pressures. Central aortic measurements were obtained approximately 3 cm above the aortic valve annulus and averaged over 5 cardiac cycles. Within 24 hours of the procedure, a transthoracic echocardiogram was obtained. Doppler echocardiography was used to determine the aortic valve mean gradient derived from the modified Bernoulli equation using the acoustic window with the highest velocity and averaged over 3 cardiac cycles. Ascending aorta size was measured via cardiac computed tomography (CT) angiography according to our institution’s preoperative TAVI-CT protocol. Ascending aortic dimensions were reported as the minimum aortic diameter obtained 4 cm above the aortic valve annulus at end diastole.
First-generation valve models were defined as Edwards Sapien (Edward Lifesciences) and CoreValve Evolut (Medtronic) prostheses. Second-generation valve models—defined as Sapien XT, CoreValve Evolut Pro, and CoreValve Evolut R models—that incorporate a skirt design to reduce paravalvular leak were evaluated in a separate subgroup analysis. An additional subgroup analysis was performed based on prosthesis annular size. Furthermore, the effects of ascending aorta size on the difference between mean catheterization and Doppler gradients, henceforth denoted as “pressure differential,” were determined. To do so, the ascending aortas of patients who received either a balloon-expandable or a self-expanding TAVI were indexed to the transcatheter heart valve (THV) size. Patients were then stratified into 2 groups—“large” and “small”—based on this ratio; the cutoff was set at the average value measured between all patients. To confirm an ideal cutoff, the ratio was set at the maximum value to include all patients in 1 group then iteratively decreased until statistical significance was no longer noted in between-group comparisons. The resulting cutoff value was 1.19, which incidentally was the same as the average size ratio determined by arithmetic mean.
Between-group differences were analyzed using a Student’s t test for continuous variables and presented as mean value ± standard deviation. Linear regression analysis was employed to determine the correlation between invasively measured and Doppler-derived measurements. A 2-tailed P-value <.05 was considered statistically significant. All statistical analyses were performed using JMP Pro, version 15 (SAS).
Results
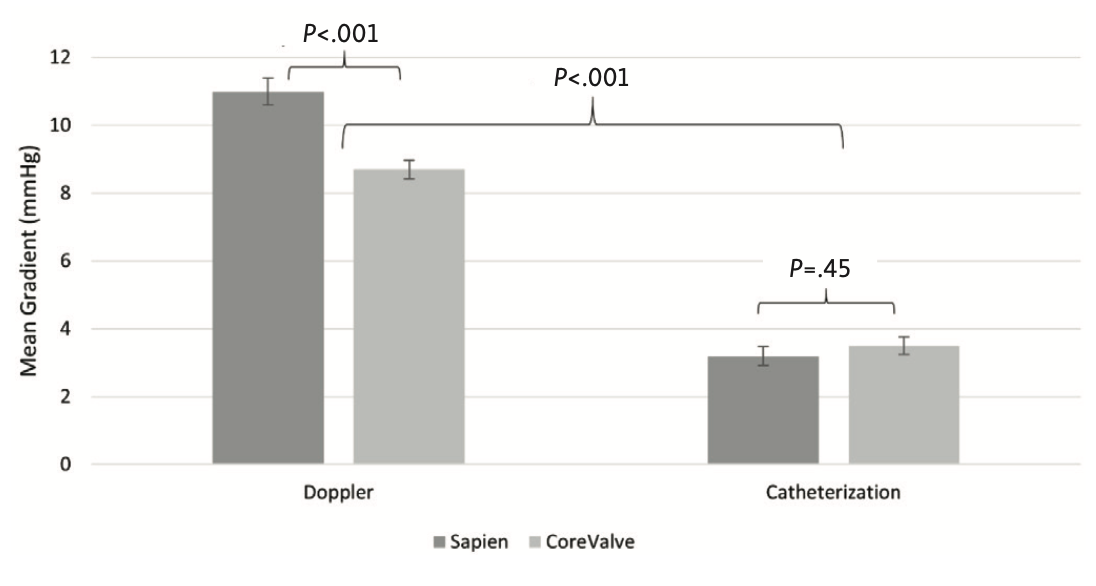
A total of 507 patients who underwent TAVI were reviewed, of which 41 were excluded due to incomplete reporting of data. The remaining cohort included 210 patients who received Sapien and 255 patients who received CoreValve prostheses. As shown in Figure 1, Doppler-derived mean gradients (Sapien 11.0 ± 5.8 mm Hg; CoreValve 8.7 ± 4.5 mm Hg) were significantly higher than gradients derived by catheterization (Sapien 3.2 ± 4.0 mm Hg; CoreValve 3.5 ± 4.1 mm Hg; P<.001). Additionally, Doppler-derived Sapien gradients were significantly higher than Doppler-derived CoreValve gradients (P<.001), although gradients derived from catheterization were not different between the 2 valve types (P=.45).
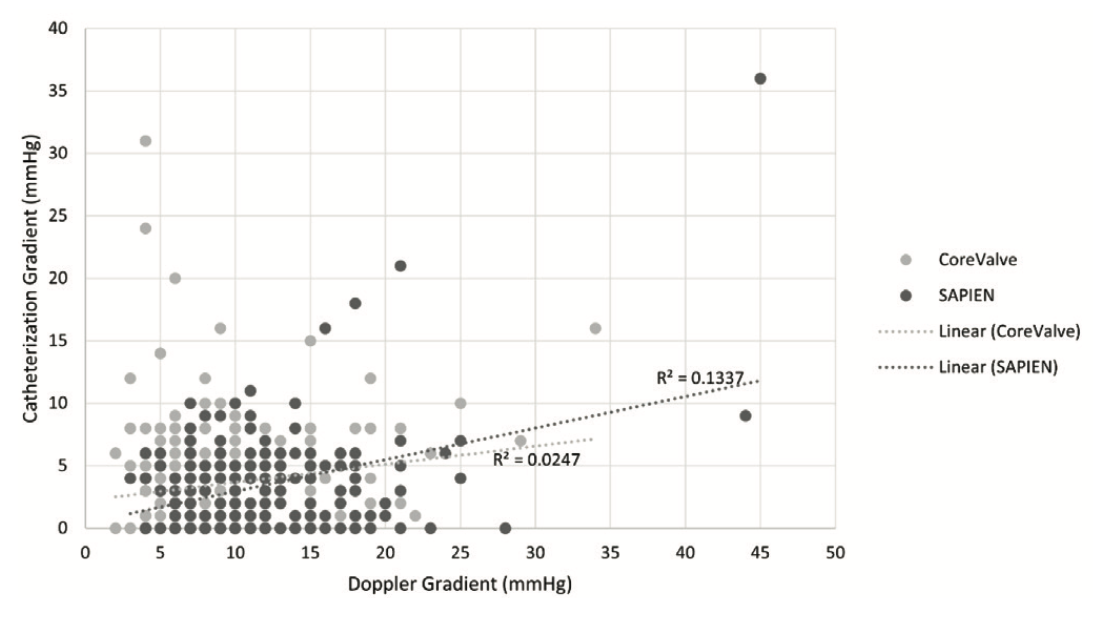
As shown in Figure 2, a poor correlation was found between catheterization- and Doppler-derived gradients across prosthesis type. Correlation was worse for Sapien valves than for CoreValve devices (R2=0.13 vs R2=0.02, respectively).
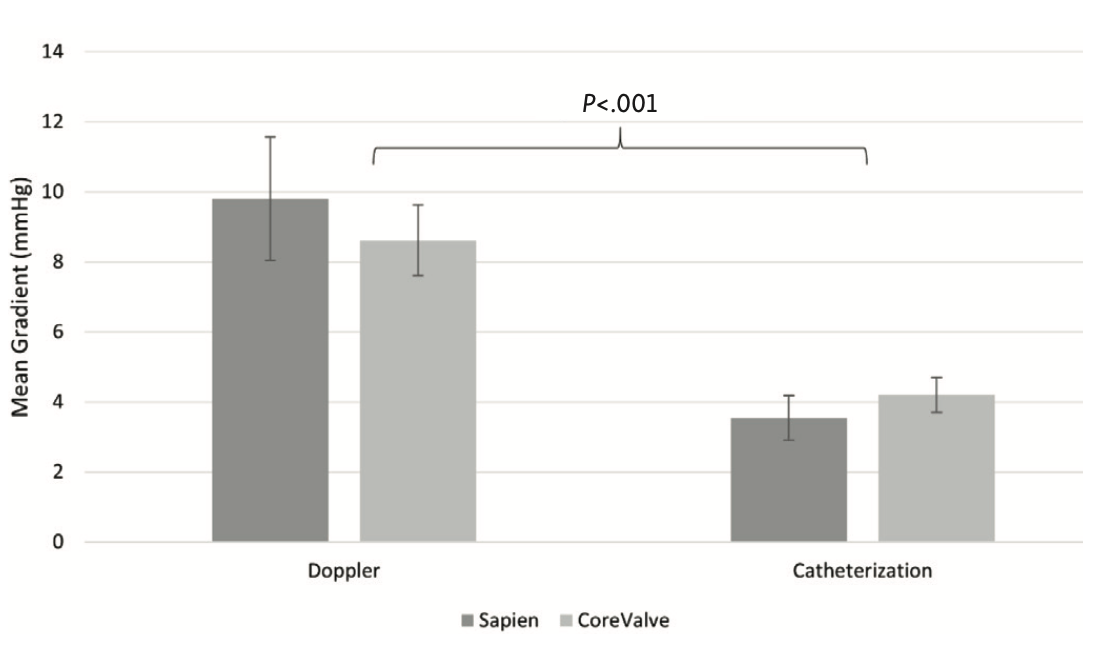
A subgroup analysis with second-generation skirted valves was performed and included 31 patients who received a Sapien XT valve and 73 patients who received either an Evolut Pro or Evolut R valve. No patients received a Sapien 3 valve in this cohort. As shown in Figure 3, Doppler-derived gradients (Sapien 9.8 ± 4.5 mm Hg vs CoreValve 8.6 ± 5.1 mm Hg) were significantly higher than those obtained by catheterization (Sapien 3.5 ± 4.1 mm Hg vs CoreValve 4.2 ± 5.1 mm Hg; P<.001 for both comparisons). Between-group invasive- and Doppler-derived mean gradients did not differ (P=.26).
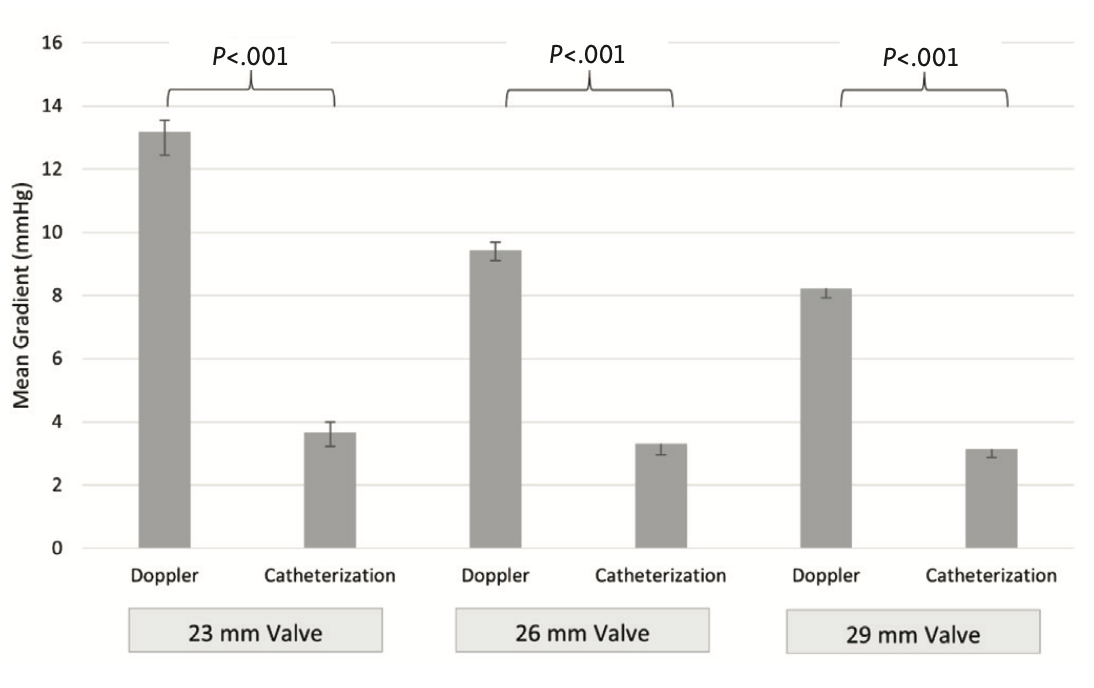
As shown in Figure 4, an additional subgroup analysis was performed assessing the relationship between aortic valve mean gradient and valve size stratified by 3 annular dimensions: 23 mm, 26 mm, and 29 mm. This analysis was performed in aggregate size and was further delineated by prosthetic size and type. Patients who received 20-mm, 31-mm, and 34-mm valves were excluded from subgroup analysis due to insufficient data to allow for direct comparison.
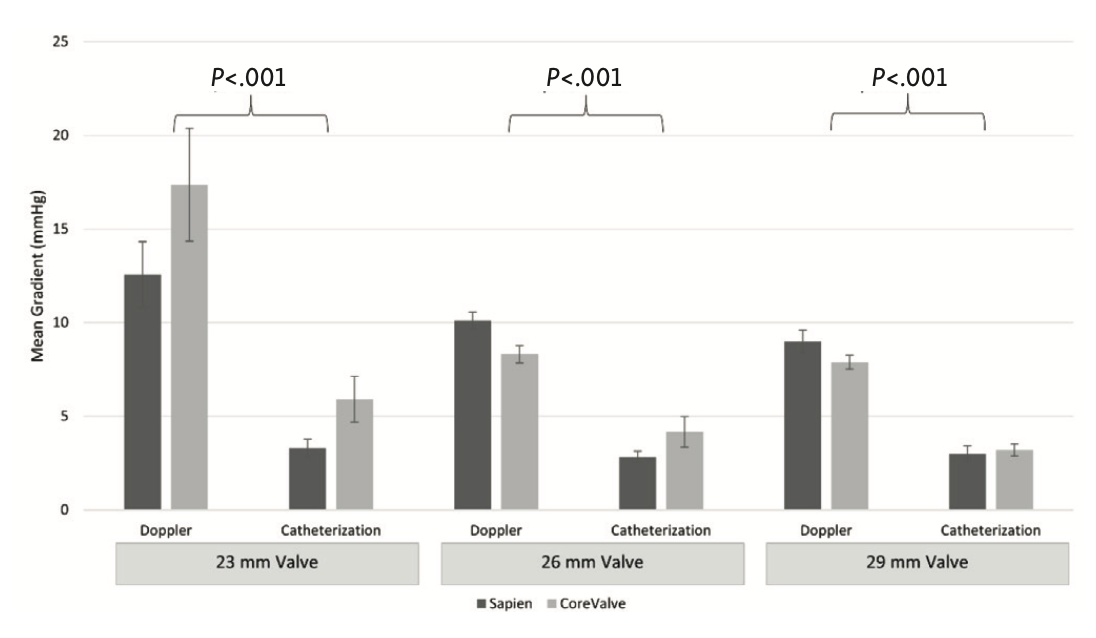
For 23-mm valves, mean Doppler-derived gradients were significantly higher in aggregate than those obtained by catherization (13.2 ± 0.7 mm Hg vs 3.7 ± 0.5 mm Hg; P<.001). When stratified by valve size and type, Doppler-derived gradients (Sapien 12.6 ± 6.2 mm Hg; CoreValve 17.4 ± 9.1 mm Hg) remained significantly higher than catheterization gradients (Sapien 3.3 ± 4.1 mm Hg; CoreValve 5.9 ± 4.1 mm Hg; P<.001), as shown in Figure 5. Between-group invasive-derived and Doppler-derived gradients were not statistically different.
For 26-mm valves, mean Doppler-derived gradients were significantly higher in aggregate than those obtained by catherization (9.44 ± 0.3 mm Hg vs 3.3 ± 0.4 mm Hg; P<.001). When stratified by valve size and type, mean gradients obtained by Doppler (Sapien 10.1 ± 4.0 mm Hg; CoreValve 8.3 ± 3.2 mm Hg) remained significantly higher than those obtained by catheterization (Sapien 2.8 ± 2.7 mm Hg; CoreValve 4.2 ± 5.6 mm Hg; P<.001). Between-group catheterization gradients were not significantly different (P=.12). However, between-group Doppler-derived gradients were significantly lower in the CoreValve group (P<.01).
In patients who received 29-mm valves, mean Doppler-derived gradients were significantly higher in aggregate than those obtained by catheterization (8.2 ± 0.3 mm Hg vs 3.1 ± 0.3 mm Hg; P<.001). When stratified by valve size and type, mean Doppler-derived gradients (Sapien 9.0 ± 4.3 mm Hg; CoreValve 7.9 ± 3.8 mm Hg) remained significantly higher than those obtained by catheterization (Sapien 3.0 ± 3.0 mm Hg; CoreValve 3.2 ± 3.4 mm Hg; P<.001). Between-group differences were not significant.
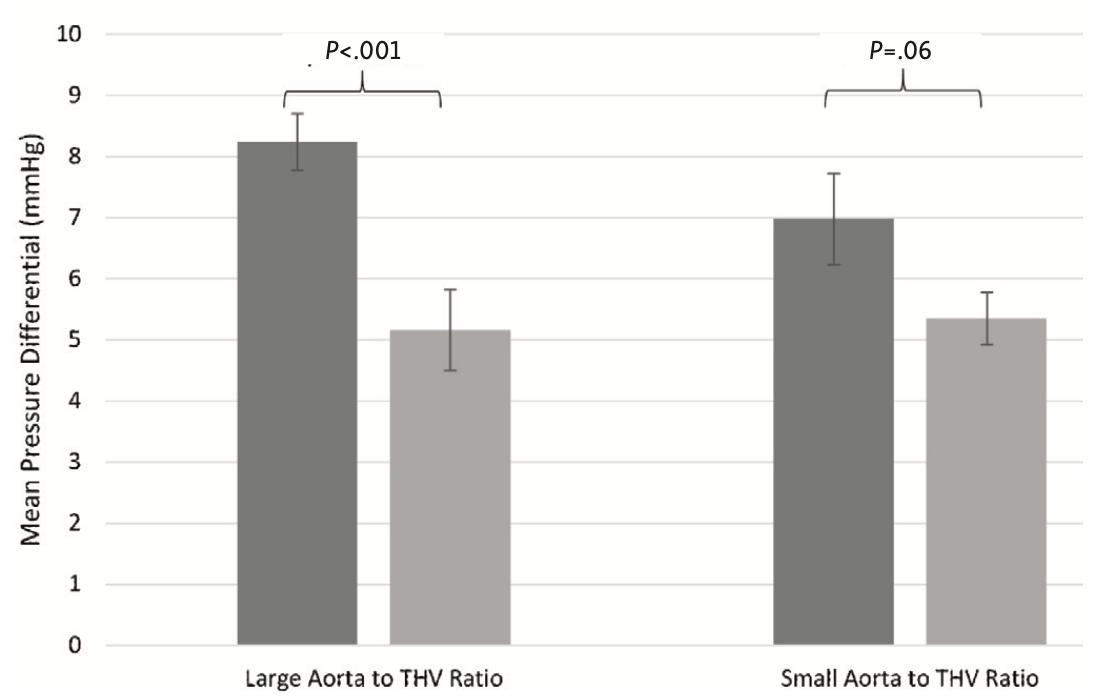
Lastly, the effect of indexed ascending aortic size on post-TAVI pressure differential, previously defined as the difference between mean catheterization gradient and mean Doppler gradient, was assessed. As shown in Figure 6, patients with a large aorta to THV ratio who received a Sapien valve demonstrated significantly larger pressure differential when compared with those who received a CoreValve prosthesis (8.24 ± 0.46 mm Hg vs 5.16 ± 0.66 mm Hg, respectively; P<.001). However, in patients with a small aorta to THV ratio, we found a trend toward larger pressure differential in the Sapien cohort, although this did not reach statistical significance (Sapien 6.98 ± 0.75 mm Hg vs CoreValve 5.35 ± 0.43 mm Hg; P=.06).
Discussion
Accurate assessment of valvular gradients is clinically important as it provides essential information regarding valve function and durability, and inaccurate indices may prompt additional testing or procedures. To our knowledge, this is the largest retrospective study that has investigated invasive and noninvasive gradient discrepancies in a post-TAVI population. This study demonstrates that aortic valve mean gradients determined by invasive catheterization are consistently lower than Doppler echocardiography irrespective of valve size or generation. Doppler-derived, but not catheterization-derived gradients, are higher in Sapien valves compared with CoreValve prostheses, although this relationship is not consistent throughout all valve sizes. Lastly, patients with a Sapien device and large aortas with respect to valve size demonstrate larger pressure differential than such patients with a CoreValve device.
It is postulated that the discrepancies between catheterization- and Doppler-derived gradients in this study are due to differences in hemodynamic profiles—namely, pressure recovery—inherent to CoreValve and Sapien TAVI designs. Pressure recovery is based on the principle that energy in a closed system is neither created nor destroyed. When blood accelerates across a restrictive orifice such as in severe aortic stenosis, pressure energy proximal to the stenosis is converted to kinetic energy. Distal to the stenosis, blood decelerates and this kinetic energy is recapitulated or “recovers” as pressure energy.14 Pressure recovery is most evident when blood flow is laminar, as tends to be the case in patients with smaller aortic diameters, particularly those <3 cm.15-17 In patients with dilated or aneurysmal ascending aortas, blood flow may be comparably more turbulent and this laminar blood flow is disrupted. In this circumstance, pressure energy is once again converted to kinetic energy or is lost as heat, and the proportional effect of pressure recovery is abrogated.
Continuous-wave Doppler echocardiography interrogates the maximal instantaneous velocity anywhere along the left ventricular outflow-aortic valve axis and this maximal velocity is converted to an estimated pressure gradient using the modified Bernoulli equation. Catheterization, in contrast, directly measures pressure several centimeters distal to the aortic valve after pressure recovery has occurred. Accordingly, pressure recovery is an element that confers a potential for Doppler echocardiography to overestimate valve gradients compared with invasive studies. Thus, the pressure measurements obtained via catheterization may better reflect the true hemodynamic stress that valve flow imparts on the rest of the body.15-17
In experimental models, pressure recovery has been shown to overestimate the mean gradient and can mischaracterize the severity of aortic stenosis in 10% of patients with native aortic stenosis.15,16 This has been confirmed clinically in the SEAS study, where 47% of patients classified as having severe native stenosis by AVAi were reclassified to non-severe aortic stenosis when pressure recovery was considered.18 Contemporary studies have confirmed that this relationship exists in the TAVI population as well; however, data have been discrepant regarding differences between balloon-expandable and self-expanding valves, as well as between valve sizes.9-12 Abdel-Wahab et al showed that echocardiogram-derived gradients were higher in balloon-expandable valves when compared with self-expanding valves.9 A similar trend was noted in this study, although this was not consistent across valve size when stratified by valve type.
Mando et al did not find differences in echocardiographic gradients between balloon-expandable and self-expanding devices, but they did report that simultaneously derived echocardiogram gradients were higher than invasive gradients. They also found that echocardiogram gradients increased as valve size decreased, a finding that was also observed in our study.10 Aalaei-Andabili et al reaffirmed that Doppler-derived gradients in balloon-expandable valves were higher compared with invasive gradients. Contrary to our findings, they noted that balloon-expandable valves were associated with lower invasive measurements than self-expanding valves, but conceded that this observation was based on small sample size and should be interpreted with caution.12
The CoreValve system incorporates a self-expanding, nitinol, stabilizing stent frame that extends into the ascending aorta. This differs from the Sapien valve design, which incorporates a comparably shorter nitinol stent-valve frame that does not extend as far into the ascending aorta. Hatoum et al have shown in a high-fidelity in vitro model that the CoreValve Evolut prosthesis, as a consequence of this elongated stent frame, is associated with increased turbulent flow, and in turn, less pressure recovery when compared with a Sapien 3 valve.11 Importantly, the authors noted lower peak and mean recovered pressure gradients in the Sapien 3 valve, which they suggested would not only affect accurate echocardiographic calculation of the aortic valve area, but also result in a lower net pressure imparted on the left ventricle, albeit of questionable clinical significance given an observed difference of up to 2 mm Hg. We propose that the difference in pressure recovery efficiency seen in these in vitro studies is one of the physiological mechanisms underpinning the observed clinical differences in our study. Although we specifically did not compare Sapien 3 valve designs in our cohort, these main differences in stent-valve frame design are largely the same across different valve generations, leading us to suspect that this hemodynamic effect is present in older design iterations as well.
To account for the effect of ascending aortic size on the pressure differential between catheterization and Doppler gradients in this study, the minimum ascending aortic diameter was indexed to the bioprosthetic implant size. It was found that in patients with comparably large aortas relative to device size, pressure differential was larger in the Sapien cohort than in the CoreValve group. A nonsignificant trend was noted in patients with smaller aortas comparable to device size. Because the ascending aorta diameter is routinely measured from the preoperative cardiac CT, this ratio can easily be factored into clinical planning. For example, in patients who are sized for smaller THVs based on annular dimensions, but also have large or dilated aortas, the choice of a Sapien device may prove to be more hemodynamically favorable from a pressure differential standpoint.
Study limitations. There are a few limitations to this retrospective, single-center study. Invasive catheterization data were not obtained simultaneously with Doppler-derived gradients; rather, the latter was obtained within 24 hours after valve replacement (although most often within 6 hours post implantation). It is well established that low-flow states can affect mean and peak gradients independent of effective orifice area.19 In the perioperative state, there are many factors, such as sedation, ventricular pacing, ectopy, and volume shifts, that affect cardiac output and/or systemic vascular resistance. Together, these factors may all conspire to create a transient hemodynamic state not apparent in recovery. As our Doppler gradients were not obtained simultaneously with the catheterization gradients, these data may reflect a different hemodynamic state.
To address this limitation, systolic and diastolic blood pressure measurements recorded immediately post TAVI deployment and during the postprocedure echocardiogram were reviewed. Complete data were available for 384 patients. Interestingly, there was no difference in mean systolic blood pressure recorded during catheterization and echocardiogram (134 mm Hg vs 132 mm Hg; P=.41). However, mean diastolic pressure was lower (54 mm Hg vs 64 mm Hg; P<.001). With these additional hemodynamic data, the magnitude of pressure changes between post-TAVI deployment in the catheterization lab and those derived noninvasively via echocardiogram were relatively modest. Additionally, other studies have reported similar discrepancies in mean gradients in TAVI despite performing simultaneous catheterization and echocardiographic measurements.10
Erroneous reading and equipment malfunction, sonographer acquisition error, and interpretation error are all potential causes for the observed differences. Attempts to mitigate these sources of error were undertaken by paying careful attention to data acquisition, including appropriate zeroing, resolution of whip or reverberation artifacts, and averaging mean gradients over a minimum of 3 cardiac cycles. Additionally, echocardiographic studies were over-read by experienced structural imaging cardiologists to limit interobserver variability. Lastly, the ascending aorta subgroup analysis was based on data derived from the minimal ascending aortic diameter noted on pre-TAVI cardiac CT studies. It is recognized that ascending aortas are not uniformly circular, particularly in patients with aortic stenosis, where dilated or aneurysmal aortas are common. Thus, in patients with eccentric anatomy, flow and pressure recovery characteristics may differ. Anecdotally, however, it was noted that maximum and minimum aortic dimensions were often within 1-2 mm in most of the patients studied; therefore, we suspect the contribution of this patient heterogeneity to our overall findings to be limited.
Conclusion
Doppler-derived gradients were elevated in the post-TAVI population when compared with catheterization-derived gradients and this difference persisted despite valvular size and generation of THV design. Additionally, Doppler-derived Sapien gradients were significantly larger than Doppler-derived CoreValve gradients. These discrepancies may be related to pressure recovery phenomenon manifesting inherent hemodynamic differences in valvular design. How these hemodynamic differences relate to long-term valvular integrity, and in turn, clinical outcomes warrant further study.
Affiliations and Disclosures
From the 1Division of Cardiovascular Medicine, Department of Medicine, The Ohio State University Wexner Medical Center, Columbus, Ohio; 2Michigan Technological University, Houghton, Michigan; and 3Georgia Institute of Technology/Emory University, Atlanta, Georgia.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript accepted September 23, 2021.
Address for correspondence: Scott Lilly, MD, PhD, The Ohio State University Wexner Medical Center, Division of Cardiovascular Medicine, Davis Heart & Lung Research Institute, 473 West 12th Avenue, Suite 200, Columbus, OH 43210. Email: Scott.lilly@osumc.edu
References
1. Mack MJ, Leon MB, Thourani VH, et al. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N Engl J Med. 2019;380(18):1695-1705. doi:10.1056/NEJMoa1814052
2. Reardon MJ, Van Mieghem NM, Popma JJ, et al. Surgical or transcatheter aortic-valve replacement in intermediate-risk patients. N Engl J Med. 2017;376(14):1321-1331. doi:10.1056/NEJMoa1700456
3. Halim SA, Edwards FH, Dai D, et al. Outcomes of transcatheter aortic valve replacement in patients with bicuspid aortic valve disease: a report from the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy Registry. Circulation. 2020;141(13):1071-1079. doi:10.1161/CIRCULATIONAHA.119.040333
4. Evaluation of transcatheter aortic valve replacement compared to surveillance for patients with asymptomatic severe aortic stenosis (EARLY TAVR). ClinicalTrials.gov Identifier: NCT03042104. Accessed May 17, 2022. https://clinicaltrials.gov/ct2/show/NCT03042104
5. Early valve replacement guided by biomarkers of LV decompensation in asymptomatic patients with severe AS (EVoLVeD). ClinicalTrials.gov Identifier: NCT03094143. Accessed May 17, 2022. https://clinicaltrials.gov/ct2/show/NCT03094143
6. Transcatheter aortic valve replacement to unload the left ventricle in patients with advanced heart failure (TAVR UNLOAD). ClinicalTrials.gov Identifier: NCT02661451. Accessed May 17, 2022. https://clinicaltrials.gov/ct2/show/NCT02661451
7. Leon MB, Mack MJ, Hahn RT, et al. Outcomes 2 years after transcatheter aortic valve replacement in patients at low surgical risk. J Am Coll Cardiol. 2021;77(9):1149-1161. doi:10.1016/j.jacc.2020.12.052
8. Nishimura RA, Otto CM, Bonow RO, et al. 2017 AHA/ACC Focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2017;70(2):252-289. doi:10.1016/j.jacc.2017.03.011
9. Abdel-Wahab M, Mehilli J, Frerker C, et al. Comparison of balloon-expandable vs self-expandable valves in patients undergoing transcatheter aortic valve replacement: the CHOICE randomized clinical trial. JAMA. 2014;311(15):1503-1514. doi:10.1001/jama.2014.3316
10. Mando R, Abbas AE, Gallagher M, et al. Echo overestimates trans-aortic gradients immediately post TAVR: a pressure recovery phenomenon in a simultaneous cath and echo study. J Am Coll Cardiol. 2019;73 (9 Suppl 1):1251. doi:10.1016/S0735-1097(19)31858-3
11. Hatoum H, Hahn RT, Lilly S, Dasi LP. Differences in pressure recovery between balloon expandable and self-expandable transcatheter aortic valves. Ann Biomed Eng. 2020;48(2):860-867. doi:10.1007/s10439-019-02425-8
12. Aalaei-Andabili SH, Park KE, Choi CY, et al. Relationship between invasive and echocardiographic transvalvular gradients after transcatheter aortic valve replacement. Cardiol Ther. 2020;9(1):201-206. doi:10.1007/s40119-020-00161-y
13. Søndergaard L, Ihlemann N, Capodanno D, et al. Durability of transcatheter and surgical bioprosthetic aortic valves in patients at lower surgical risk. J Am Coll Cardiol. 2019;73(5):546-553. doi:10.1016/j.jacc.2018.10.083
14. Bach DS. Echo/Doppler evaluation of hemodynamics after aortic valve replacement: principles of interrogation and evaluation of high gradients. JACC Cardiovasc Imaging. 2010;3(3):296-304. doi:10.1016/j.jcmg.2009.11.009
15. Garcia D, Dumesnil JG, Durand LG, Kadem L, Pibarot P. Discrepancies between catheter and Doppler estimates of valve effective orifice area can be predicted from the pressure recovery phenomenon: practical implications with regard to quantification of aortic stenosis severity. J Am Coll Cardiol. 2003;41(3):435-442. doi:10.1016/s0735-1097(02)02764-x
16. Niederberger J, Schima H, Maurer G, Baumgartner H. Importance of pressure recovery for the assessment of aortic stenosis by Doppler ultrasound. Role of aortic size, aortic valve area, and direction of the stenotic jet in vitro. Circulation. 1996;94(8):1934-1940. doi:10.1161/01.cir.94.8.1934
17. Baumgartner H, Stefenelli T, Niederberger J, Schima H, Maurer G. “Overestimation” of catheter gradients by Doppler ultrasound in patients with aortic stenosis: a predictable manifestation of pressure recovery. J Am Coll Cardiol. 1999;(6):1655-1661. doi:10.1016/s0735-1097(99)00066-2
18. Bahlmann E, Cramariuc D, Gerdts E, et al. Impact of pressure recovery on echocardiographic assessment of asymptomatic aortic stenosis: a SEAS substudy. JACC Cardiovasc Imaging. 2010;3(6):555-562. doi:10.1016/j.jcmg.2009.11.019
19. Otto CM. Aortic stenosis: treat the patient not the numbers. Heart. 2018;104(3):190-191. doi:10.1136/heartjnl-2017-312222
Related Articles
- Transcatheter Aortic Valve Replacement for Mixed Aortic Valve Disease: A Propensity Score-Adjusted Analysis From the RISPEVA Registry
- Generational Differences in Outcomes of Self-Expanding Valves for Transcatheter Aortic Valve Replacement
- Unplanned Hospital Readmissions After Transcatheter Aortic Valve Replacement in the Era of New-Generation Devices
- Reframing Optimal Implantation of the Sapien 3 Transcatheter Heart Valve













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}