Acute Coronary Occlusion and Percutaneous Coronary Intervention After Out-of-Hospital Cardiac Arrest
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Abstract
Objectives. Early coronary angiography (CAG) has been recommended in selected patients following out-of-hospital-cardiac-arrest (OHCA). We aimed to identify clinical features associated with acute coronary occlusion (ACO) and evaluate the associations between ACO, successful percutaneous coronary intervention (PCI) and outcomes in this population.
Methods. We included comatose OHCA patients treated with targeted temperature management (TTM) between December 2005 and September 2016 who underwent early CAG within 24 hours. The co-primary outcomes were all-cause 30-day mortality and good neurological outcome (modified Rankin Score [mRS] ≤2) at hospital discharge.
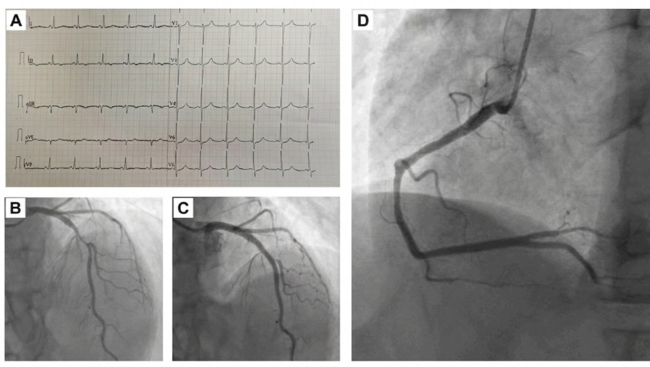
Results. Among 155 patients (93% shockable arrest rhythm, 55% with ST elevation), 133 (86%) had coronary artery stenosis ≥50% and 65 (42%) had ACO. ST elevation (sensitivity 74%, specificity 59%, OR 4.0, 95% CI 2.0-8.1) and elevated first troponin (sensitivity 88%, specificity 26%, OR 2.5, 95% CI 1.1-6.1) had limited sensitivity and specificity for ACO. Unadjusted 30-day mortality did not differ significantly by coronary disease severity or ACO. Successful PCI was associated with a lower risk of 30-day mortality (adjusted HR 0.5, 95% CI 0.2-0.9, P=.03), especially among patients with ACO (adjusted HR 0.4, 95% CI 0.1-0.9, P=0.03). After adjustment, ACO and PCI were not associated with the probability of good neurological outcome.
Conclusions. In this select cohort of resuscitated OHCA patients undergoing CAG, unstable coronary disease is highly prevalent and successful PCI was associated with a higher probability of 30-day survival, especially among those with ACO. Neither ACO nor successful PCI were independently associated with good neurological outcome.
Introduction
Coronary artery disease (CAD) is the most common treatable precipitant of out-of-hospital-cardiac-arrest (OHCA) without an obvious noncardiac cause.1,2 Observational studies of patients with OHCA who undergo CAG have reported a 70% prevalence of obstructive CAD, with up to 30%-50% of patients having acute coronary occlusion (ACO) or unstable lesions warranting PCI even in the absence of ST elevation (STE) on electrocardiogram.3-7
Observational studies and meta-analyses have suggested better neurological outcomes and overall survival for OHCA patients who undergo CAG within 24 hours after return of spontaneous circulation (ROSC).5,8-11 However, these results contrast with recent randomized controlled trials (RCTs) including COACT,12 PEARL,13 TOMAHAWK,14 and EMERGE,15 which did not demonstrate better survival with early CAG in hemodynamically stable OHCA patients without STE or shock. Important differences exist between RCT and observational, or “real-world”, study populations, raising questions about generalizability and selection bias, respectively.16 For instance, a recent analysis demonstrated that only 38% of patients in a large United Kingdom OHCA registry would have met inclusion criteria for the COACT study.17 Specifically, RCTs excluded patients with STEMI or shock, observing a markedly lower prevalence of ACO than observational studies.
This has led to uncertainty whether any sub-population of OHCA patients benefits from early CAG after resuscitation from OHCA. While it is logical to assume that OHCA patients with ACO are the most likely to benefit from CAG and PCI, this has not been clearly demonstrated and prediction of ACO remains challenging in clinical practice. We sought to identify clinical findings associated with ACO and to describe the associations between ACO and PCI with survival and favorable neurologic outcome in a real-world cohort of OHCA patients who underwent early CAG. Our hypothesis was that ACO would be associated with worse outcomes and PCI would have a more robust benefit in patients with ACO.
Methods
Study population. The Institutional Review Board of Mayo Clinic approved this retrospective cohort study as minimal risk to patients. Informed consent was waived for patients providing Minnesota Research Authorization. We included adult comatose patients admitted to Mayo Clinic cardiac intensive care unit (CICU) who underwent TTM and CAG following OHCA between December 2005 and September 2016; patients were predominantly treated using a target temperature of 33℃ per institutional guidelines with all care provided under guidance of the CICU team.18,19 Early CAG was defined as occurring within 24 hours of hospital admission, consistent with prior studies.20-23
Data sources. Data were extracted from the medical record electronically and manually. Available details of the OHCA event included initial rhythm (shockable versus non-shockable), witnessed, and bystander CPR; duration of CPR or therapies administered during resuscitation were not routinely available.22,24-27 Illness severity scores were obtained including the Sequential Organ Failure Assessment (SOFA) and Acute Physiology and Chronic Health Evaluation (APACHE) scores.28 Shockable rhythm was defined as an initial arrest rhythm of ventricular tachycardia or ventricular fibrillation. We recorded the initial and peak troponin-T (4th generation Roche Diagnostics assay, upper-reference-limit <0.01 ng/mL); if the first troponin level was determined using a different assay, we recorded whether this was above the upper reference. Peak simultaneous vasopressor and inotrope infusion doses were used to calculate the Vasoactive Inotropic Score (VIS).
Coronary angiogram reports were reviewed for procedural details. PCI was defined as angioplasty, stenting, or aspiration thrombectomy, and was defined as successful based on the impression of the interventional cardiologist. ACO was defined as 100% occlusion of a major epicardial coronary artery without characteristics of a chronic occlusion. Unstable CAD was defined as ACO or angiographic thrombus, and stable CAD was defined as ≥50% stenosis of a major epicardial coronary vessel without these features. CAD severity was graded using the validated Duke CAD Prognostic Index (CADPI), a hierarchical 0-100 score based on the number, location, and severity of coronary stenoses; the CADPI was not calculated in patients with prior coronary artery bypass grafting (CABG).29 Echocardiographic data were recorded when available.18,19
Statistical analyses. The co-primary outcomes of interest were all-cause 30-day mortality (including in-hospital deaths) and good neurological outcome, defined as a modified Rankin Score (mRS) ≤2 at hospital discharge. Continuous variables are summarized as median (interquartile range, IQR) and compared using the two-tailed Wilcoxon rank-sum test. Categorical variables are compared using two-tailed Fisher’s exact test. Odds ratio (OR) and 95% confidence interval (CI) values for prediction of good neurological outcome were determined using logistic regression, before and after multivariable adjustment. Kaplan-Meier curves were used to estimate 30-day survival, with groups compared using the log-rank test. Hazard-ratio (HR) and 95% CI values for 30-day mortality were determined using Cox-proportional hazard analysis, before and after multivariable adjustment. To account for known predictors of mortality, including the severity of anoxic brain injury and shock severity, we adjusted our multivariable models for peak neuron-specific enolase (NSE), maximum VIS,24 and the number of major risk factors for adverse outcome identified in the INTCAR registry, including non-shockable arrest rhythm, unwitnessed arrest, lack of bystander CPR, initial lactate >7 mmol/L, initial pH <7.2 and age >85.30 P-values <.05 were considered statistically significant for all comparisons. All statistical analyses were done using JMP Pro version 14.0 (SAS Institute).
Results
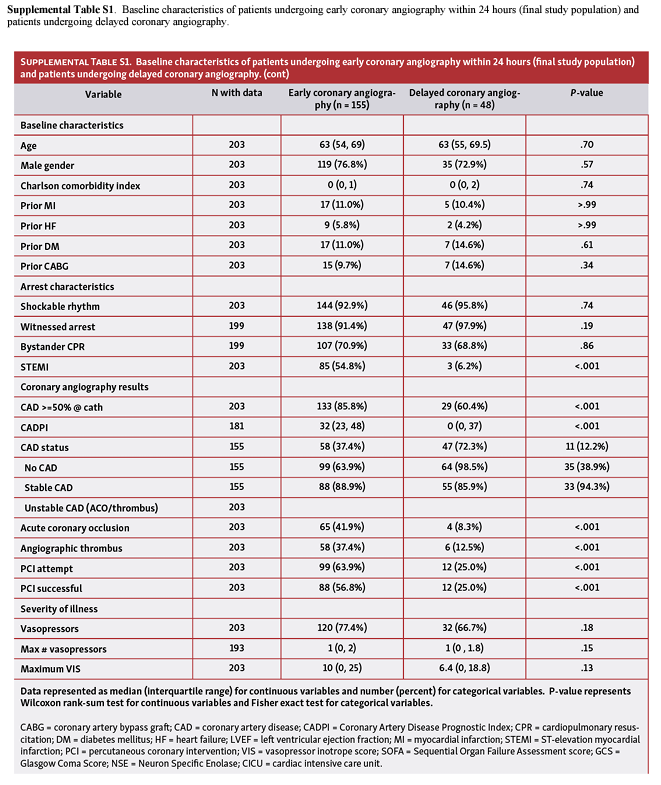
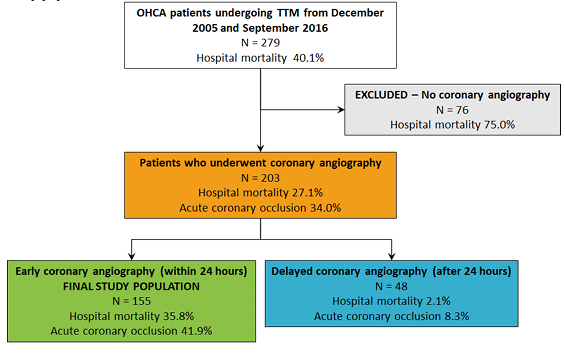
Study population. Out of 279 patients with OHCA undergoing TTM during the study period, 76 (27.2%) patients did not undergo CAG and were excluded (Supplemental Figure 1). Of 203 patients undergoing CAG, 155 (76.4%) underwent early CAG within 24 hours of hospital admission and comprised the final study population (Table 1).
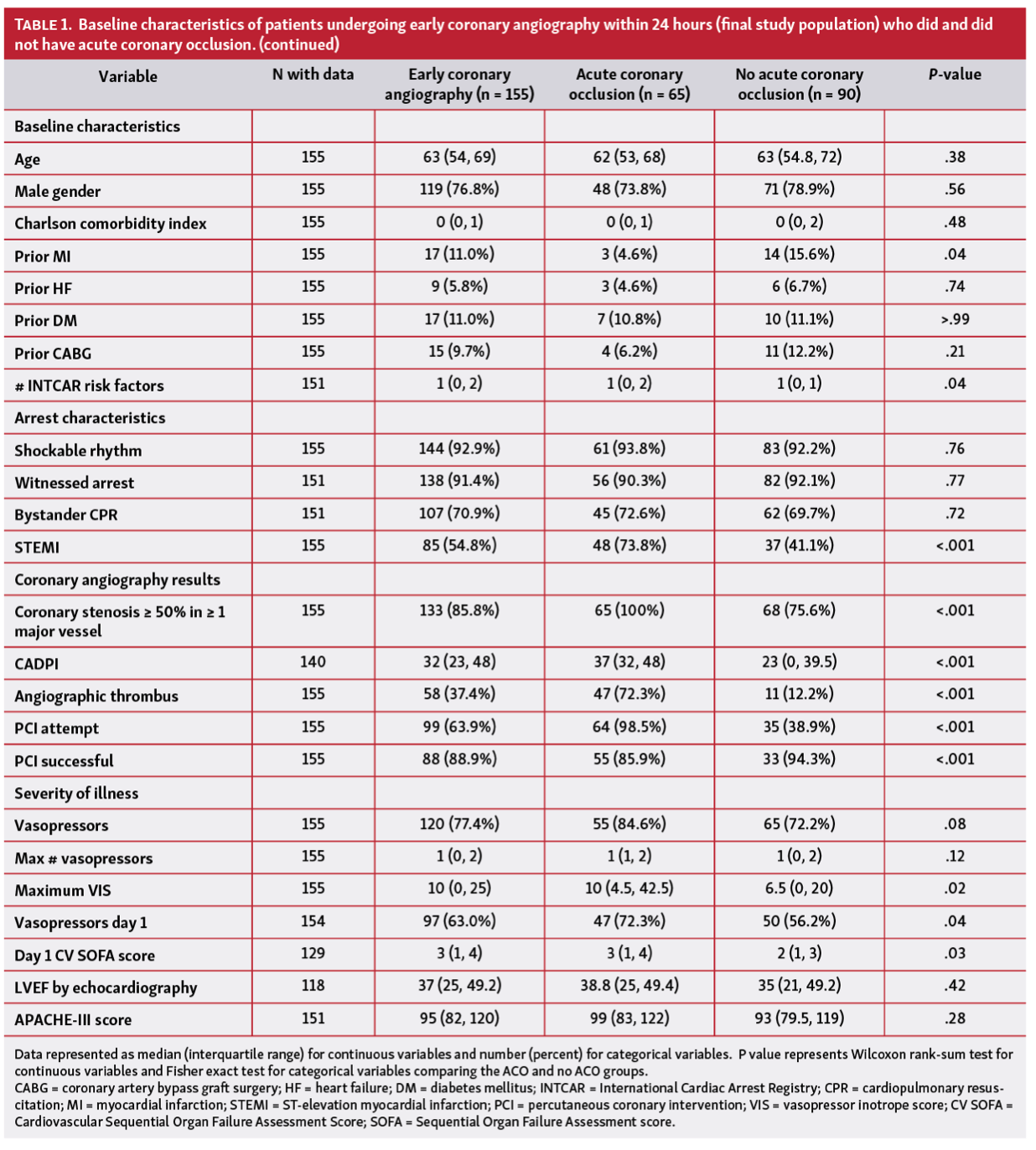
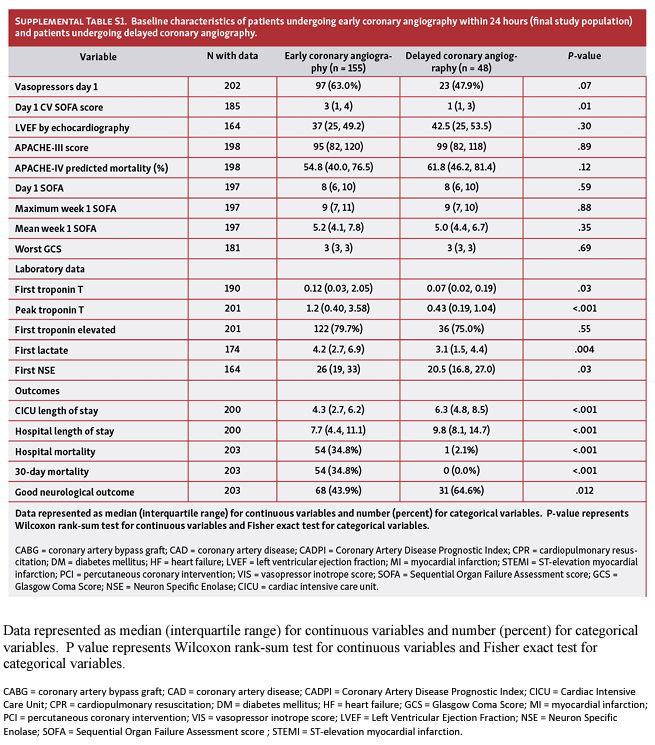
Baseline characteristics. Baseline characteristics of patients undergoing early CAG (final study population) are compared with excluded patients undergoing delayed CAG in Supplemental Table 1. Patients undergoing early CAG more frequently had STE, with a greater prevalence of CAD, ACO and use of PCI (all P<0.001), as well as higher troponin-T, lactate, and NSE levels (all P<.05). Arrest rhythm was shockable in 144 (92.9%), and most had a witnessed arrest with bystander CPR. The median CADPI was 32 (23-48) in the early CAG cohort; 76 (49.0%) had unstable CAD, 57 (36.8%) had stable CAD, and 22 (14.2%) had no significant CAD.
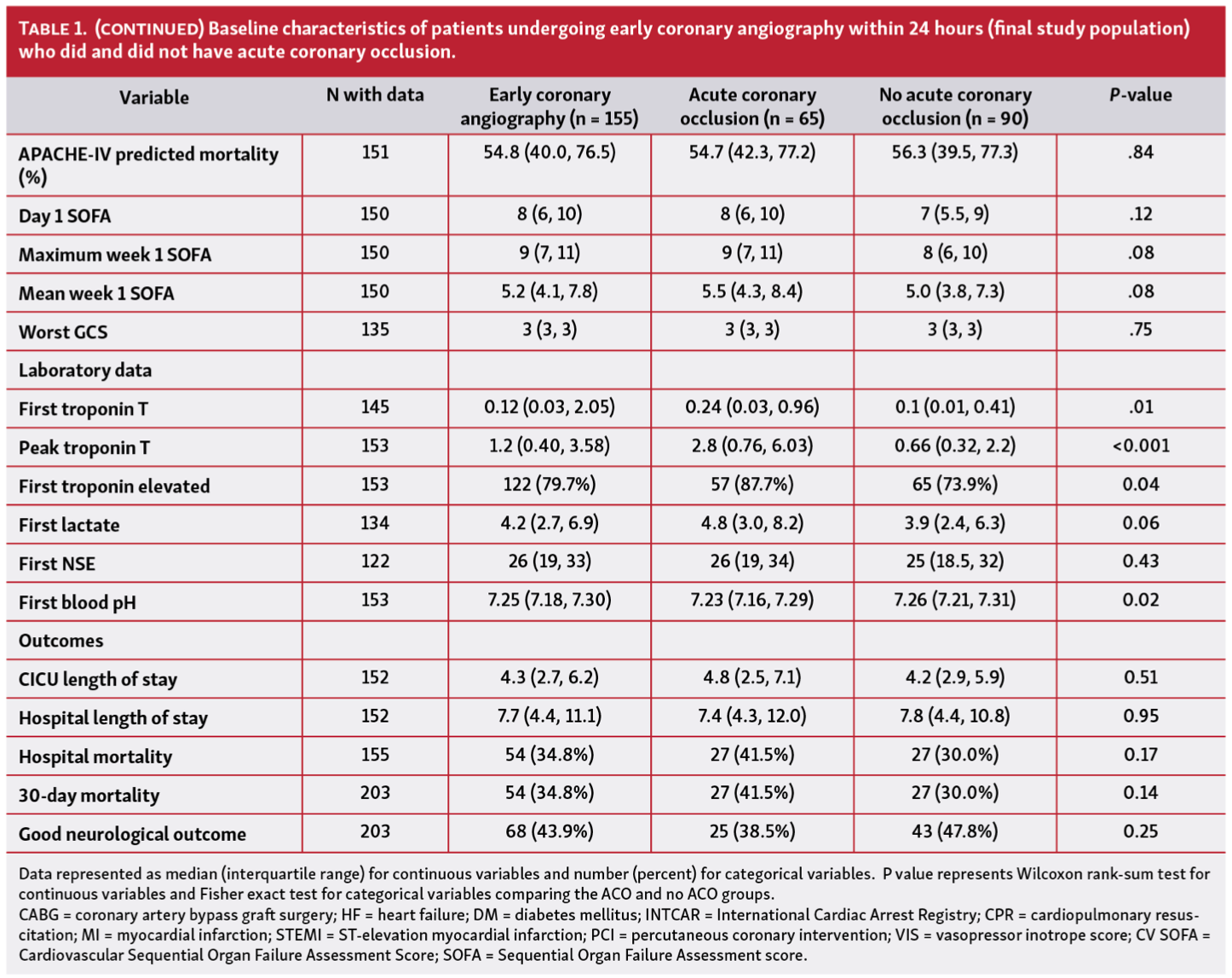
Predictors of acute coronary occlusion. ACO was present in 65 patients (41.9%), including 48 (73.8%) patients with STE and 17 (26.2%) patients without STE. Baseline characteristics of patients undergoing early CAG with and without ACO are compared in Table 1. Notably, patients with ACO had higher median CADPI, a greater median number of INTCAR risk factors, and higher initial and peak troponin-T values (all P<.05). Patients with ACO were more likely to receive vasopressors on Day 1 of hospitalization, and had higher peak VIS and Day 1 Cardiovascular SOFA score, although Day 1 SOFA or APACHE-III scores were not significantly different. Progressively higher troponin-T was observed in patients with no CAD, stable CAD, and unstable CAD. The first troponin was normal in 40.9% of patients with no CAD, 21.8% of patients with stable CAD, and 13.2% of patients with unstable CAD (including 8 [12.3%] patients with ACO). The prevalence of ACO was higher for patients who required vasopressors during the first 24 hours (48.5% vs 31.6%, P=.04), including when limited to those with STE (62.7% vs 42.3%, P=.08). Patients without STE who did not require vasopressors during the first 24 hours still had a 22.6% prevalence of ACO. Patients with SCAI Shock Stage D/E had a higher prevalence of ACO (52.3% vs 34.4%, P=.03).
STE (sensitivity 73.8%, specificity 58.9%, positive predictive value [PPV] 56.5%, negative predictive value [NPV] 75.7%, accuracy 65.2%, OR 4.04, 95% CI 2.02-8.10) and elevated first troponin (sensitivity 87.7%, specificity 26.1%, PPV 46.7%, NPV 74.2%, accuracy 52.3%, OR 2.52, 95% CI 1.05-6.08) were associated with the presence of ACO. The presence of either STE or elevated first troponin identified 62 of 65 (95.4%) patients with ACO on early CAG. The PPV of either STE or elevated first troponin for ACO was 45.6% and increased to 60.6% if both criteria were present; the NPV for ACO was 83.3% in the 18 (9.7%) patients without either STE or an elevated first troponin. Among the 3 patients with ACO in the absence of STE or a positive first troponin, only one did not require vasopressors during the first 24 hours.
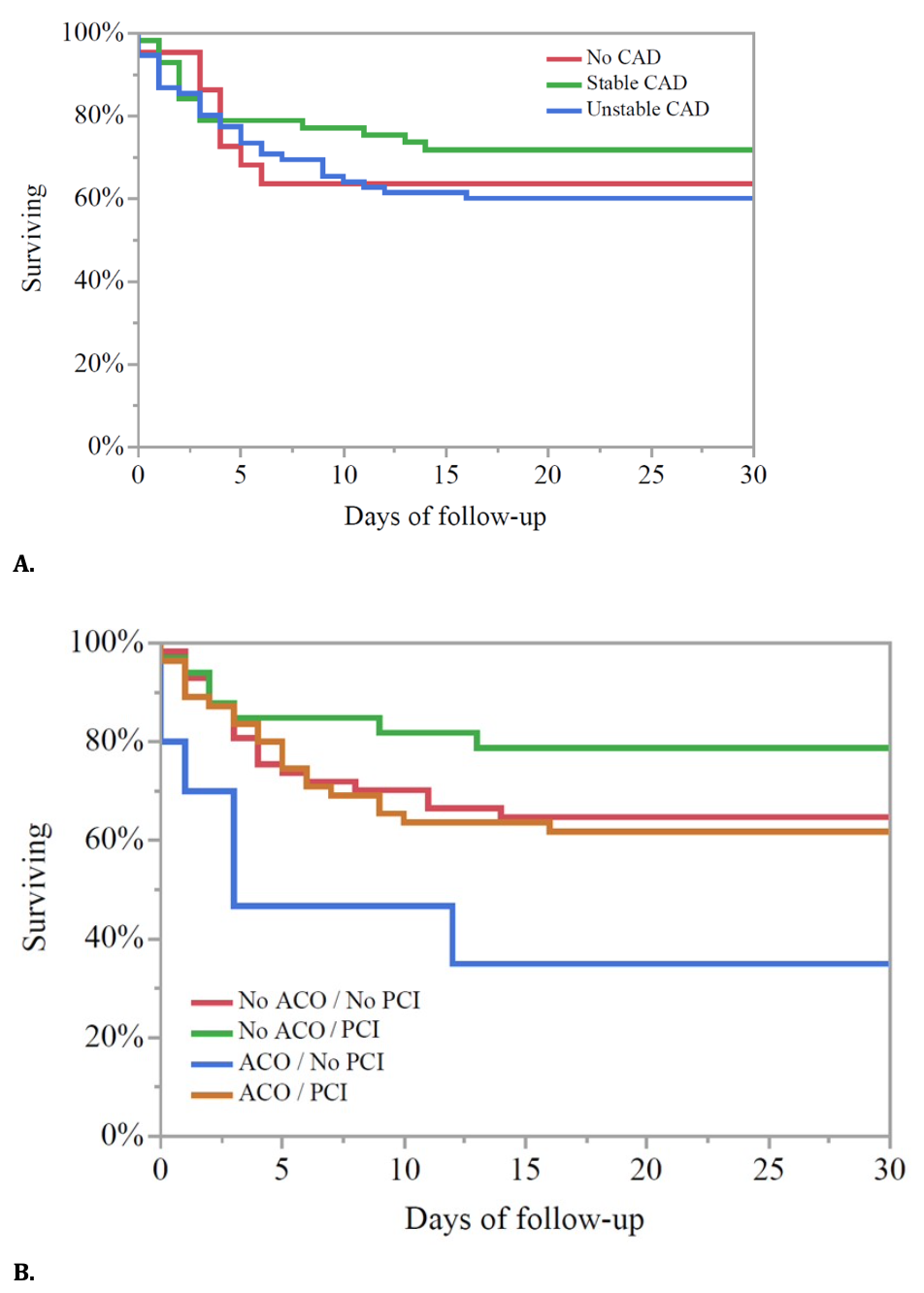
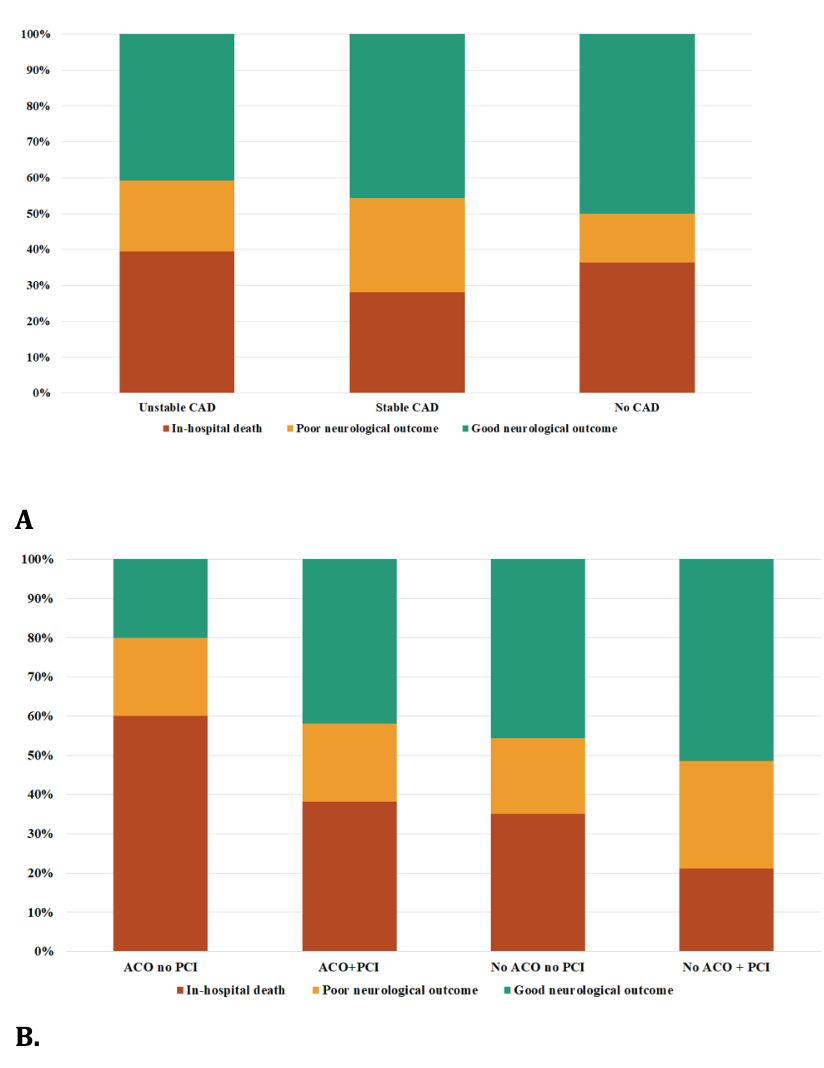
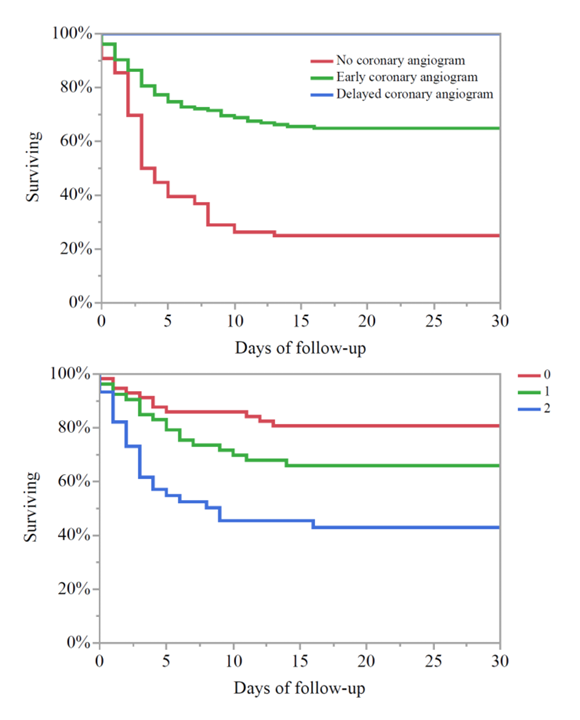
Thirty-day survival – unadjusted analysis. Fifty-four (34.8%) patients undergoing early CAG died within 30 days of admission (all during hospitalization). Kaplan-Meier estimates of 30-day survival were 25.0% for patients not undergoing CAG (excluded), 64.9% for patients undergoing early CAG (final study population), and 100% for patients undergoing delayed CAG (excluded) (Supplemental Figure 2A, P<0.001); one patient who received delayed coronary angiography died in hospital after more than 30 days. Among those undergoing early CAG, 30-day survival did not differ in patients with stable, unstable, or no CAD (Figure 1A), or between patients with and without STE, ACO, or successful PCI (all P>0.1 between groups). A higher number of INTCAR risk factors was incrementally associated with lower 30-day survival (Supplemental Figure 2B).
On unadjusted Cox-proportional hazards analysis, ACO (unadjusted HR 1.50, 95% CI 0.88-2.56, P=.14) and successful PCI (unadjusted HR 0.76, 95% CI 0.45-1.30, P=.32) were not significantly associated with the risk of 30-day mortality when considered individually. This finding held in patients with STE (unadjusted HR for successful PCI 0.62, 95% CI 0.28-1.40, P=.25) and without STE (unadjusted HR for successful PCI 0.68, 95% CI 0.27-1.72, P=.49). The risk of unadjusted 30-day mortality did not differ between patients with and without STE and for unstable, stable, or no CAD on Cox-proportional hazards analysis (all P>0.1 between groups); CADPI was not associated with 30-day mortality (P=.28). Among patients with ACO, 30-day mortality was lower for patients who received PCI, but this difference did not reach statistical significance (38.2% vs 65.0%, unadjusted HR 0.43, 95% CI 0.17-1.07, P=.07); similar findings were observed for patients without ACO (21.2% vs 35.3%, unadjusted HR 0.57, 95% CI 0.24-1.35, P=.20).
Patients were separated into four groups based on the presence of ACO and successful PCI: (i) ACO/PCI (n=55); (ii) ACO/no PCI (n=9); (iii) no ACO/PCI (n=33); (iv) no ACO/no PCI (n=57). Kaplan-Meier analysis demonstrated a difference in 30-day survival between these groups (Figure 1B, P=.03 by log-rank), with the lowest survival amongst the ACO/no PCI group. Using unadjusted Cox proportional-hazard analysis, patients with ACO/no PCI had higher 30-day mortality compared to no ACO/PCI (unadjusted HR 4.53, 95% CI 1.52-13.51, P=.007) and no ACO/no PCI (unadjusted HR 2.56, 95% CI 1.02-6.38, P=.04). There was a trend towards higher mortality in the ACO/no PCI group compared to patients with ACO/PCI (unadjusted HR 1.94, 95% CI 0.82-4.55, P=.07). All other between-groups comparisons were not significant (P>.1).
Thirty-day survival - adjusted analysis. After multivariable adjustment, successful PCI was associated with a lower risk of 30-day mortality (adjusted HR 0.48, 95% CI 0.24-0.95, P=.03), but the presence of ACO was not (adjusted HR 1.59, 95% CI 0.79-3.21, P=.19). After multivariable adjustment, patients with ACO/PCI had lower 30-day mortality than those with ACO/no PCI (adjusted HR 0.35, 95% CI 0.13-0.89, P=.03), while patients with ACO/no PCI had higher 30-day mortality than patients with no ACO/PCI (adjusted HR 3.47, 95% CI 1.15-5.45, P=.03). Other between-groups comparisons were not significant. Adjusted 30-day mortality was the same for patients with stable, unstable and no CAD (all P>.05). Each additional INTCAR risk factor was associated with higher 30-day mortality (adjusted HR 1.52, 95% CI 1.15-1.97, P=.002).
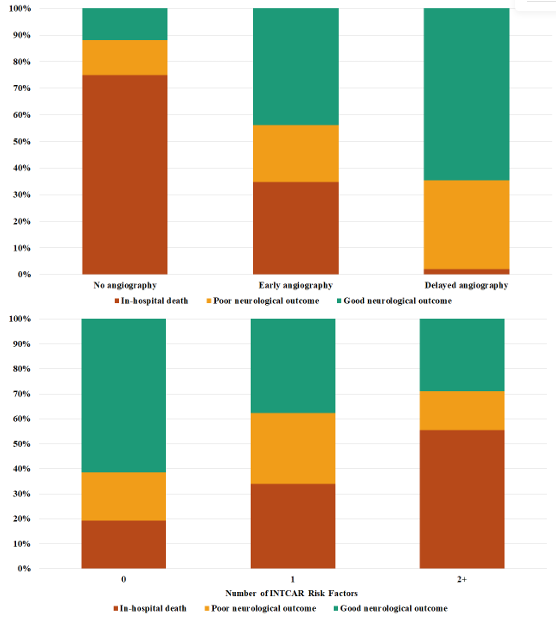
Neurological outcome. Among hospital survivors who underwent early CAG (n=101), 68 (67.3%) had a good neurological outcome (43.9% of the early CAG cohort including non-survivors); 64.6% of all patients who underwent delayed CAG (n=48) had a good neurological outcome, as did 11.8% of patients who did not undergo CAG (n=76) (Supplemental Figure 3A). On unadjusted analysis, good neurological outcome did not differ significantly based on the presence of unstable, stable, or no CAD (Figure 2A), ACO or successful PCI. However, the CADPI was inversely associated with the risk of a good neurological outcome (unadjusted OR 0.83 per 10 points, 95% CI 0.70-0.99, P=.04). Patients with ACO/no PCI had the lowest rate of good neurological outcome (20.0%), but this was not significantly different from other groups (all P>.05). Successful PCI was not associated with good neurological outcome for patients with or without ACO (Figure 2B). After multivariable adjustment, only CADPI was associated with the adjusted risk of good neurological outcome (adjusted OR 0.82 per 10 points, 95% CI 0.68-0.99, P=.04). A higher number of INTCAR risk factors was incrementally associated with worse neurological outcomes (Supplemental Figure 3B), but a significant association was not seen in the adjusted logistic regression models (all P>.05).
Discussion
In 155 comatose resuscitated OHCA patients receiving early CAG within 24 hours of ROSC, underlying CAD and ACO were common even among patients without STE or shock. The presence of either STE or an elevated first troponin identified most patients with ACO, but these variables lacked sensitivity and specificity when analyzed individually. ACO was associated with greater shock severity, and patients with severe shock (SCAI Shock Stage D/E) had a higher prevalence of ACO. Successful PCI was associated with lower adjusted 30-day mortality, especially in the subset of patients with ACO, while increasing CAD complexity was associated with a higher risk of poor neurologic outcome. These findings emphasize the significant prevalence of ACO and the potential benefit of successful PCI in a real-world OHCA cohort with a high prevalence of shockable arrest rhythm and hemodynamic instability including patients with and without STEMI.
Predicting acute coronary occlusion. The primary purpose of early CAG after OHCA is to identify and treat unstable CAD, particularly ACO. As such, it has been assumed that patients with a higher likelihood of ACO are more appropriate candidates for early CAG based on a greater potential benefit. Unfortunately, currently available heuristics lack sensitivity and specificity for ACO after OHCA. Available data (including our findings) suggest that the sensitivity of STE for ACO or a culprit vessel lesion warranting PCI after OHCA may be as low as 60%-70%.3-5 Our data confirm and expand on this observation by showing a substantial >20% prevalence of ACO even among OHCA patients without STE or vasopressor dependence. This is congruous with previous studies reporting a 20-30% prevalence of ACO in OHCA patients without STE, even for patients with non-shockable rhythms.5,11,31-35 Our study is among the first to examine the prevalence of ACO as a function of the presence and severity of shock, both of which were associated with a higher prevalence of ACO. The low specificity of elevated cardiac troponins may reflect diffuse myocardial hypoperfusion during arrest or non-ischemic myocardial injury related to defibrillation in the absence of CAD or ACO.36,37 Likewise, previous analyses have reported a high proportion of non-diagnostic ECGs after OHCA, with >1 in 10 patients with a normal ECG having an acute coronary lesion.38 Crucially, RCTs in OHCA patients without STE or shock have reported about half the prevalence of ACO (ranging from 17%-43%) that we and others have observed in observational analyses.12,14,39 It is likely that this represents a degree of selection bias whereby patients with suspected ACO preferentially received CAG. However, the high prevalence of STEMI and shock among OHCA patients in our study and other contemporary analyses emphasizes the need for a most robust strategy to identify ACO after OHCA in contemporary practice, particularly considering that a strategy of universal CAG has not been shown to be beneficial.
Identifying the benefit of PCI. Our hypothesis-generating finding that OHCA patients with ACO may have benefitted from successful PCI must be interpreted in the context of prior studies. Observational analyses have demonstrated better short-term and long-term survival among OHCA patients who receive PCI,3,9 although ours is among the first to examine this in the context of ACO. These observational studies must be reconciled with recent RCTs demonstrating a lack of benefit from universal early CAG in comatose OHCA patients without STE or shock, most of whom died from neurological injury.12-15 These RCTs excluded the patients felt to be most likely to benefit from CAG, who accounted for a substantial number of our patients. This, coupled with the low prevalence of ACO, may explain the lack of an improvement in survival with early CAG in these RCTs, recognizing that these studies do not generalize to many of the patient in contemporary OHCA cohorts.17 Unlike in AMI without OHCA, the dominant driver of mortality after OHCA is anoxic brain injury, which could eliminate the benefits of revascularization in many patients (particularly those without STE or shock) and may not be affected by CAG or PCI.40,41 Furthermore, extrapolating from the broader CAD literature, PCI is associated with a survival benefit only in the presence of unstable CAD,42 as compared to stable CAD.43,44 Similarly, a recently published post-hoc analysis of the CULPRIT-SHOCK trial demonstrated that culprit-vessel only revascularization is the preferred strategy to immediate multi-vessel PCI amongst OHCA patients with AMI-related cardiogenic shock.45 Therefore, to benefit from early CAG after OHCA, at least the following two conditions must be met: (1) the patient must have unstable CAD meriting urgent revascularization; and (2) the patient must not have sustained a non-survivable anoxic brain injury.
Importantly, our data did not show better neurological outcome in any subgroup defined by the presence of ACO or successful PCI despite higher survival in some subgroups. Given that neurologic outcome is a highly relevant patient-centered outcome in this cohort, this raises the question of whether identification and treatment of ACO after OHCA improves functional outcomes. Recent observational work by Pareek et al used shock severity and electrocardiography combined with an early neurologic prognostication score to retrospectively identify a subset of patients with low neurologic risk in whom immediate CAG was associated with improved neurologic outcome.46 Although not prospectively validated, this lends credence to the hypothesis that any potential benefit of early CAG is likely to be determined both by the probability of ACO and the risk of neurologic-etiology death.41 Many of the same risk factors examined by Pareek et al were included in the INTCAR risk score that we used for multivariable adjustment.30,34 This mirrors previous consensus statements regarding the appropriate use of CAG after OHCA, which have aimed to capture features associated with a greater severity of hypoxic neurologic insult.47
Limitations. Patients in our cohort were not formally selected for CAG based on a structured estimate of neurological risk (apart from the gestalt of the treating physician), introducing the possibility of bias regarding patient selection for CAG. All observational analyses of CAG after OHCA are fraught with this same selection bias, which may explain the divergent findings in observational and randomized analyses. We included a selected group of patients with largely shockable arrest rhythms at a single center over a prolonged period predating recent RCTs and clinical practice guidelines. Moreover, our analysis was intentionally limited to patients with predominantly shockable arrest rhythms in whom ACO was a suspected cause or contributor to OHCA (ie, those who underwent early CAG); a discussion of the various important non-coronary causes for OHCA was therefore beyond the scope of our study. Because of this, the conclusions derived from our analysis may not be generalizable when applied to a broader, more contemporary OHCA population. Furthermore, we lacked data regarding mode of death and duration of OHCA (including no-flow and low-flow times) prior to ROSC. The modest size of our cohort may have resulted in limited statistical power to detect between-group differences, particularly for good neurological outcome and among sub-groups (eg, STE vs no STE). Our analysis examined the performance of conventional (4th-generation) troponin-T assays for ACO, and it is likely that contemporary high-sensitivity (5th-generation) troponin assays would have different performance. While our study provides important data on the prevalence, prognosis and clinical variables associated with ACO and PCI following OHCA in a real word population, our limited cohort size precluded sub-group analyses among patients who did not have STE. As such, further research is needed to identify stable comatose OHCA patients without STE in whom the likelihood of ACO is high enough, and the probability of severe anoxic brain injury low enough, to justify early CAG.
Conclusions
Among comatose patients resuscitated after OHCA undergoing CAG, unstable CAD and ACO are highly prevalent even among patients without STE or shock. Patients with ACO had greater shock severity, and those with severe shock had a higher prevalence of ACO. The presence of STE or an elevated first troponin individually lacked high sensitivity or specificity for the presence of ACO, highlighting the need to identify more reliable markers. In this selected cohort of OHCA patients undergoing CAG, successful PCI was associated with a higher probability of 30-day survival, especially in those with ACO (most of whom had STE). Our work reinforces the need for more accurate identification of ACO and culprit vessel lesions in patients resuscitated from OHCA and a more nuanced approach to early CAG decisions in this population. Published RCTs do not support a strategy of universal early CAG in comatose OHCA patients without STE or shock (who had a higher prevalence of ACO in our analysis), and future research is needed to determine whether early CAG may still be beneficial in a subgroup of remaining patients with a high probability of ACO.
Affiliations and Disclosures
From the 1Department of Cardiovascular Medicine and the 2Department of Internal Medicine, Mayo Clinic, Rochester, MN, USA.
Disclosures: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Address for correspondence: Jacob C. Jentzer, MD, FACC, FAHA, Assistant Professor of Medicine, Department of Cardiovascular Medicine and Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, the Mayo Clinic, 200 First Street SW, Rochester, MN 55905. Email: jentzer.jacob@mayo.edu
Supplemental Material
References
References
- Fishman GI, Chugh SS, Dimarco JP, et al. Sudden cardiac death prediction and prevention: report from a National Heart, Lung, and Blood Institute and Heart Rhythm Society Workshop. Circulation. 2010;122(22):2335-2348. doi:10.1161/CIRCULATIONAHA.110.976092
- Radsel P, Knafelj R, Kocjancic S, Noc M. Angiographic characteristics of coronary disease and postresuscitation electrocardiograms in patients with aborted cardiac arrest outside a hospital. Am J Cardiol. 2011;108(5):634-638. doi:10.1016/j.amjcard.2011.04.008
- Dumas F, Cariou A, Manzo-Silberman S, et al. Immediate percutaneous coronary intervention is associated with better survival after out-of-hospital cardiac arrest: insights from the PROCAT (Parisian Region Out of hospital Cardiac ArresT) registry. Circ Cardiovasc Interv. 2010;3(3):200-207. doi:10.1161/CIRCINTERVENTIONS.109.913665
- Dumas F, Manzo-Silberman S, Fichet J, et al. Can early cardiac troponin I measurement help to predict recent coronary occlusion in out-of-hospital cardiac arrest survivors? Crit Care Med. 2012;40(6):1777-1784. doi:10.1097/CCM.0b013e3182474d5e
- Kern KB, Lotun K, Patel N, et al. Outcomes of comatose cardiac arrest survivors with and without ST-segment elevation myocardial infarction: importance of coronary angiography. JACC Cardiovasc Interv. 2015;8(8):1031-1040. doi:10.1016/j.jcin.2015.02.021
- Garcia S, Drexel T, Bekwelem W, et al. Early access to the cardiac catheterization laboratory for patients resuscitated from cardiac arrest due to a shockable rhythm: the Minnesota Resuscitation Consortium Twin Cities Unified Protocol. J Am Heart Assoc. 2016;5(1):e002670. doi:10.1161/JAHA.115.002670
- Dankiewicz J, Nielsen N, Annborn M, et al. Survival in patients without acute ST elevation after cardiac arrest and association with early coronary angiography: a post hoc analysis from the TTM trial. Intensive Care Med. 2015;41(5):856-864. doi:10.1007/s00134-015-3735-z
- Camuglia AC, Randhawa VK, Lavi S, Walters DL. Cardiac catheterization is associated with superior outcomes for survivors of out of hospital cardiac arrest: review and meta-analysis. Resuscitation. 2014;85(11):1533-1540. doi:10.1016/j.resuscitation.2014.08.025
- Welsford M, Bossard M, Shortt C, Pritchard J, Natarajan MK, Belley-Cote EP. Does early coronary angiography improve survival after out-of-hospital cardiac arrest? A systematic review with meta-analysis. Can J Cardiol. 2018;34(2):180-194. doi:10.1016/j.cjca.2017.09.012
- Khera R, CarlLee S, Blevins A, Schweizer M, Girotra S. Early coronary angiography and survival after out-of-hospital cardiac arrest: a systematic review and meta-analysis. Open Heart. 2018;5(2):e000809. doi:10.1136/openhrt-2018-000809
- Dumas F, Bougouin W, Geri G, et al. Emergency percutaneous coronary intervention in post-cardiac arrest patients without ST-segment elevation pattern: insights from the PROCAT II Registry. JACC Cardiovasc Interv. 2016;9(10):1011-1018. doi:10.1016/j.jcin.2016.02.001
- Lemkes JS, Janssens GN, van der Hoeven NW, et al. Coronary angiography after cardiac arrest without ST-segment elevation. N Engl J Med. 2019;380(15):1397-407. doi:10.1056/NEJMoa1816897
- Kern KB, Radsel P, Jentzer JC, et al. Randomized pilot clinical trial of early coronary angiography versus no early coronary angiography after cardiac arrest without ST-segment elevation: the PEARL Study. Circulation. 2020;142(21):2002-2012. doi:10.1161/CIRCULATIONAHA.120.049569
- Desch S, Freund A, Akin I, et al. Angiography after out-of-hospital cardiac arrest without ST-segment elevation. N Engl J Med. 2021;385(27):2544-2553. doi:10.1056/NEJMoa2101909
- Hauw-Berlemont C, Lamhaut L, Diehl JL, et al. Emergency vs delayed coronary angiogram in survivors of out-of-hospital cardiac arrest: results of the randomized, multicentric EMERGE trial. JAMA Cardiol. 2022;7(7):700-707. doi:10.1001/jamacardio.2022.1416
- Panchal AR, Bartos JA, Cabanas JG, et al. Part 3: adult basic and advanced life support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142(16_suppl_2):S366-S468. doi:10.1161/CIR.0000000000000916
- Roy R, Shah AM, MacCarthy P, Byrne J, Pareek N. Limited external applicability of the COACT and TOMAHAWK trials: a multicenter study. JACC Cardiovasc Interv. 2022;15(13):1388-1391. doi:10.1016/j.jcin.2022.04.036
- Jentzer JC, Anavekar NS, Mankad SV, et al. Echocardiographic left ventricular diastolic dysfunction predicts hospital mortality after out-of-hospital cardiac arrest. J Crit Care. 2018;47:114-120. doi:10.1016/j.jcrc.2018.06.016
- Tabi M, Burstein BJ, Anavekar NS, Kashani KB, Jentzer JC. Associations of vasopressor requirements with echocardiographic parameters after out-of-hospital cardiac arrest. J Intensive Care Med. 2022;37(4):518-527. doi:10.1177/0885066621998936.
- Callaway CW, Schmicker RH, Brown SP, et al. Early coronary angiography and induced hypothermia are associated with survival and functional recovery after out-of-hospital cardiac arrest. Resuscitation. 2014;85(5):657-663. doi:10.1016/j.resuscitation.2013.12.028
- Hollenbeck RD, McPherson JA, Mooney MR, et al. Early cardiac catheterization is associated with improved survival in comatose survivors of cardiac arrest without STEMI. Resuscitation. 2014;85(1):88-95. doi:10.1016/j.resuscitation.2013.07.027
- Jentzer JC, Scutella M, Pike F, et al. Early coronary angiography and percutaneous coronary intervention are associated with improved outcomes after out of hospital cardiac arrest. Resuscitation. 2018;123:15-21. doi:10.1016/j.resuscitation.2017.12.004
- Vyas A, Chan PS, Cram P, Nallamothu BK, McNally B, Girotra S. Early coronary angiography and survival after out-of-hospital cardiac arrest. Circ Cardiovasc Interv. 2015;8(10)):e002321. doi:10.1161/CIRCINTERVENTIONS.114.002321
- Tabi M, Burstein BJ, Ahmed A, Dezfulian C, Kashani KB, Jentzer JC. Shock severity and hospital mortality in out of hospital cardiac arrest patients treated with targeted temperature management. Shock. 2021;55(1):48-54. doi:10.1097/SHK.0000000000001600
- Sarma D, Pareek N, Kanyal R, et al. Clinical significance of early echocardiographic changes after resuscitated out-of-hospital cardiac arrest. Resuscitation. 2022;172:117-126. doi:10.1016/j.resuscitation.2021.12.014
- Sarma D, Tabi M, Jentzer JC. Society for cardiovascular angiography and intervention shock classification predicts mortality after out-of-hospital cardiac arrest. Resuscitation. 2022;172:101-105. doi:10.1016/j.resuscitation.2022.01.025
- Sarma D, Tabi M, Rabinstein AA, Kashani K, Jentzer JC. Urine output and mortality in patients resuscitated from out of hospital cardiac arrest. J Intensive Care Med. 2023;38(6):544-552. doi:10.1177/08850666221151014..
- Jentzer JC, van Diepen S, Murphree DH, et al. Admission diagnosis and mortality risk prediction in a contemporary cardiac intensive care unit population. Am Heart J. 2020;224:57-64. doi:10.1016/j.ahj.2020.02.018
- Mark DB, Nelson CL, Califf RM, et al. Continuing evolution of therapy for coronary artery disease. Initial results from the era of coronary angioplasty. Circulation. 1994;89(5):2015-2025. doi:10.1161/01.cir.89.5.2015
- Harhash AA, May TL, Hsu CH, et al. Risk stratification among survivors of cardiac arrest considered for coronary angiography. J Am Coll Cardiol. 2021;77(4):360-371. doi:10.1016/j.jacc.2020.11.043
- Spaulding CM, Joly LM, Rosenberg A, et al. Immediate coronary angiography in survivors of out-of-hospital cardiac arrest. N Engl J Med. 1997;336(23):1629-1633. doi:10.1056/NEJM199706053362302
- Anyfantakis ZA, Baron G, Aubry P, et al. Acute coronary angiographic findings in survivors of out-of-hospital cardiac arrest. Am Heart J. 2009;157(2):312-318. doi:10.1016/j.ahj.2008.09.016
- Gupta N, Kontos MC, Gupta A, et al. Characteristics and outcomes in patients undergoing percutaneous coronary intervention following cardiac arrest (from the NCDR). Am J Cardiol. 2014;113(7):1087-1092. doi:10.1016/j.amjcard.2013.12.014
- Kern KB, Lotun K, Patel N, et al. Outcomes of comatose cardiac arrest survivors with and without ST-segment elevation myocardial infarction: importance of coronary angiography. JACC Cardiovasc Interv. 2015;8(8):1031-1040. doi:10.1016/j.jcin.2015.02.021
- Harhash AA, May T, Hsu CH, et al. Incidence of cardiac interventions and associated cardiac arrest outcomes in patients with nonshockable initial rhythms and no ST elevation post resuscitation. Resuscitation. 2021;167:188-197. doi:10.1016/j.resuscitation.2021.08.026
- Jentzer JC, Chonde MD, Dezfulian C. Myocardial dysfunction and shock after cardiac arrest. Biomed Res Int. 2015;2015:314796. doi:10.1155/2015/314796
- Oh SH, Kim YM, Kim HJ, et al. Implication of cardiac marker elevation in patients who resuscitated from out-of-hospital cardiac arrest. Am J Emerg Med. 2012;30(3):464-471. doi:10.1016/j.ajem.2010.12.022
- Waldo SW, Chang L, Strom JB, O'Brien C, Pomerantsev E, Yeh RW. Predicting the Presence of an acute coronary lesion among patients resuscitated from cardiac arrest. Circ Cardiovasc Interv. 2015;8(10):e002198. doi:10.1161/CIRCINTERVENTIONS.114.002198.
- Larsen JM, Ravkilde J. Acute coronary angiography in patients resuscitated from out-of-hospital cardiac arrest--a systematic review and meta-analysis. Resuscitation. 2012;83(12):1427-1433. doi:10.1016/j.resuscitation.2012.08.337
- Jentzer JC, Henry TD, Barsness GW, Menon V, Baran DA, Van Diepen S. Influence of cardiac arrest and SCAI shock stage on cardiac intensive care unit mortality. Catheter Cardiovasc Interv. 2020;96(7):1350-1359. doi:10.1002/ccd.28854
- Jentzer JC, Herrmann J, Prasad A, Barsness GW, Bell MR. Utility and challenges of an early invasive strategy in patients resuscitated from out-of-hospital cardiac arrest. JACC Cardiovasc Interv. 2019;12(8):697-708. doi:10.1016/j.jcin.2019.01.245
- Bavry AA, Kumbhani DJ, Rassi AN, Bhatt DL, Askari AT. Benefit of early invasive therapy in acute coronary syndromes: a meta-analysis of contemporary randomized clinical trials. J Am Coll Cardiol. 2006;48(7):1319-1325. doi:10.1016/j.jacc.2006.06.050
- Maron DJ, Hochman JS, Reynolds HR, et al. Initial invasive or conservative strategy for stable coronary disease. N Engl J Med. 2020;382(15):1395-1407. doi:10.1056/NEJMoa1915922
- Boden WE, O'Rourke RA, Teo KK, et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007;356(15):1503-1516 .doi:10.1056/NEJMoa070829
- Zeymer U, Alushi B, Noc M, et al. Influence of culprit lesion intervention on outcomes in infarct-related cardiogenic shock with cardiac arrest. J Am Coll Cardiol. 2023;81(12):1165-1176. doi:10.1016/j.jacc.2023.01.029
- Pareek N, Beckley-Hoelscher N, Kanyal R, et al. MIRACLE2 score and SCAI grade to identify patients with out-of-hospital cardiac arrest for immediate coronary angiography. JACC Cardiovasc Interv. 2022;15(10):1074-1084. doi:10.1016/j.jcin.2022.03.035
- Noc M, Fajadet J, Lassen JF, et al. Invasive coronary treatment strategies for out-of-hospital cardiac arrest: a consensus statement from the European association for percutaneous cardiovascular interventions (EAPCI)/stent for life (SFL) groups. EuroIntervention. 2014;10(1):31-37. doi:10.4244/EIJV10I1A7