


Balloon Angioplasty Versus Shockwave Intravascular Lithotripsy in Calcified Coronary Arteries: The BASIL Study
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Abstract
Objectives. Severe coronary calcification is a predictor for procedural failure during percutaneous coronary intervention (PCI). Intravascular lithotripsy (IVL) delivers acoustic pressure waves to modify coronary calcification to optimize stent results. The efficacy of IVL compared to conventional balloon angioplasty (BA) prior to drug-eluting stent (DES) implantation is largely unknown. This study aimed to compare pretreatment with IVL vs BA for severely calcified coronary lesions prior to DES implantation.
Methods. A total of 60 patients with severely calcified coronary disease undergoing PCI were randomly assigned (1:1 ratio) to conventional BA or IVL pretreatment groups. The primary efficacy endpoint was procedural success (successful stent implantation without bailout calcium modification devices, no major angiographic complications, and residual stenosis < 20%). The primary safety endpoint was freedom from in-hospital major adverse cardiovascular events (MACE) including death, periprocedural myocardial infarction, stroke, and target vessel revascularization/target lesion failure.
Results. Procedural success was achieved in 15 (55.6%) patients in the BA group and 24 (72.7%) patients in the IVL group (P = .165). Requirement for bailout calcium modification was higher in the BA group (22.2% vs 0.0%; P = .004). The primary safety endpoint was achieved in 26 (96.3%) patients in the BA group and 30 (90.9%) patients in the IVL group (P = .405).
Conclusions. In PCI of severely calcified coronary disease, no significant differences in procedural success or in-hospital MACE were identified when comparing IVL to conventional BA pretreatment. There was a higher need for additional dedicated calcium modification observed with conventional BA.
Introduction
Severe coronary calcification is increasingly encountered during percutaneous coronary intervention (PCI) due to an aging population and associated comorbidities such as hypertension, diabetes, and chronic kidney disease.1 PCI of heavily calcified stenoses is associated with an increased risk of acute procedural complications (eg, dissections or perforations) and late adverse outcomes such as stent thrombosis or restenosis.2,3 An important factor leading to poor outcomes is the inability to adequately modify the calcium prior to stent deployment, leading to underexpansion. Lesion preparation can be achieved with various balloon-based (cutting/scoring/non-compliant) or ablative (rotational/orbital/laser atherectomy) tools. Each modality has its own mechanism of action and inherent limitations. This includes the inability to modify deep calcium layers with balloon-based therapies, and periprocedural complications with atherectomy such as slow/no flow, atrioventricular block, dissections, or perforations.4,5
Intravascular lithotripsy (IVL) is a balloon-based technology that utilizes circumferential acoustic pressure waves to fracture calcium layers without affecting soft tissue because of its lesser density and greater elasticity.6 IVL has shown excellent safety and efficacy for treating severe coronary calcification in a series of single-arm studies, but randomized data have been limited.7-10 In this prospective, randomized controlled study, we aimed to investigate if procedural success in PCI of severely calcified lesions is superior when pre-treated with IVL compared with conventional balloon dilatation.
Methods
The BASIL (Balloon Angioplasty versus Shockwave Intravascular Lithotripsy) study was a prospective, single-center, randomized controlled trial (RCT) comparing treatment with conventional balloon angioplasty (BA) vs IVL before drug-eluting stent (DES) deployment in severely calcified coronary lesions. All patients undergoing PCI at North Shore Hospital in Auckland, New Zealand were screened for study enrollment.
Patients presenting for PCI with chronic or acute coronary syndromes and severely calcified coronary artery lesions were eligible for study enrollment. Patients had to be at least 18 years old, able to give consent for study participation, and have an indication for PCI in a native coronary artery with a reference diameter greater than or equal to 2.5mm. The main exclusions were culprit lesions of ST-elevation myocardial infarction, cardiogenic shock on presentation, and contraindication to dual antiplatelet therapy for at least 6 months. The inclusion criterion for the target lesion was a calcium arc greater than or equal to 270° on intravascular ultrasound (IVUS) or angiographically severe calcification (radiopacities without cardiac motion before contrast injection generally compromising both sides of the arterial lumen) if the IVUS catheter was unable to cross the lesion for baseline assessment.11 Only 1 target lesion per patient was allowed for the study. Patients requiring multivessel PCI first had their non-target lesion treated at the operator’s discretion, and then returned for study inclusion of the target lesion as a staged procedure.
The study was approved by the Northern A Health and Disability Ethics Committee and registered at the Australian New Zealand Clinical Trials Registry with the identifier ACTRN12620000086965.
Study procedures
Patients who signed an informed consent and had an appropriate indication for PCI were screened during their procedure. If there was a severely calcified stenosis that the operator felt was suitable for PCI facilitated by either conventional BA or IVL (eg, did not need upfront atherectomy), IVUS was used to assess the target lesion. IVUS pullbacks were performed using the Opticross HD 60MHz catheter (Boston Scientific) with a pullback speed of 0.5 mm/second. If the IVUS catheter could not cross the lesion, predilatation with a small diameter balloon (1.5-2.5 mm) at nominal pressure was allowed. If the lesion met the IVUS inclusion criteria, or if the calcification was angiographically severe for IVUS-uncrossable lesions, patients were randomized 1:1 using an online random number generator to either pretreatment with BA or IVL. BA was performed with standard non-compliant balloons, with sizing, inflation pressures, and the number of inflations at the operator’s discretion. Those randomized to IVL were treated with a C2 lithotripsy balloon (Shockwave Medical, Inc.) sized 1:1 to the reference vessel diameter and inflated to subnominal pressure (4 atmospheres) during pulse delivery cycles. The total number of IVL cycles and the use of non-compliant balloon dilatation afterwards was at the operator’s discretion. Failure of the randomized treatment modality to adequately modify the lesion was judged by the operator, and any bailout calcium modification devices were then allowed to be used. A second IVUS pullback was recommended before DES deployment. After stent post-dilatation, a final IVUS pullback was performed.
Endpoints
The primary efficacy endpoint was procedural success, defined as successful stenting without the use of bailout calcium modification techniques, without major angiographic complications (types D to F dissection, perforation), and a residual stent diameter stenosis of less than 20%. The primary safety endpoint was freedom from in-hospital major adverse cardiovascular events (MACE): death, periprocedural myocardial infarction (MI), stroke, and target vessel revascularization/target lesion failure. Periprocedural MI was defined according to the Fourth Universal definition of MI: an elevation of cardiac troponin (cTn) greater than 5 times the 99th percentile upper reference limit (URL) in patients with normal baseline values (in patients with an elevated preprocedure cTn, a post-procedure cTn rise greater than 20%, with an absolute value greater than 5 times the 99th percentile URL). Additionally, the patient must have at least one of the following: new ischemic electrocardiogram changes, development of new pathological Q waves, imaging evidence of new loss of viable myocardium or new regional wall motion abnormality, or angiographic findings consistent with procedural flow-limiting complication (major dissection, perforation, loss of significant side branch).12 Adjudication of procedural complications and MACE were independently conducted by 2 experienced cardiologists (BW and SEJ) who were blinded to the randomized treatment group.
The major secondary endpoints included MACE at 30 days after the index procedure, final IVUS minimal stent area (MSA), and stent expansion relative to the distal reference lumen area. Clinical follow-up was performed via telephone contact at 30 days in addition to reviewing the electronic hospital records to review any readmissions or new events. All study participants completed the 30-day follow-up.
The angiograms and IVUS images were stored digitally. Quantitative coronary angiography (QCA) and IVUS analysis were performed by an independent core laboratory (Cardialysis).
Statistical analysis
Categorical variables are presented as absolute numbers and population percentages. Continuous variables are presented as mean ± SD or median with interquartile range (IQR). Comparisons between groups were made using Student’s t-test for continuous variables and Pearson’s chi-squared test for categorical variables. Two-sided P-values of less than 0.05 were considered statistically significant. Formal power calculation was not undertaken, as the BASIL study was designed as a pilot single-center randomized controlled trial. Additionally, the design of the study occurred before studies describing clinical use and outcomes of IVL became widely available. Statistical analysis was with IBM SPSS Statistics for Windows, version 25.0 (IBM Corp.).
Results
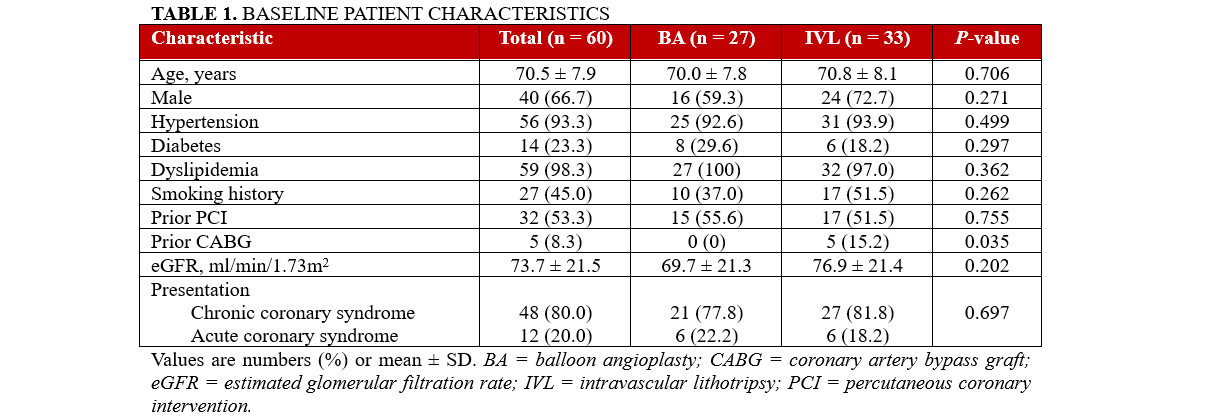
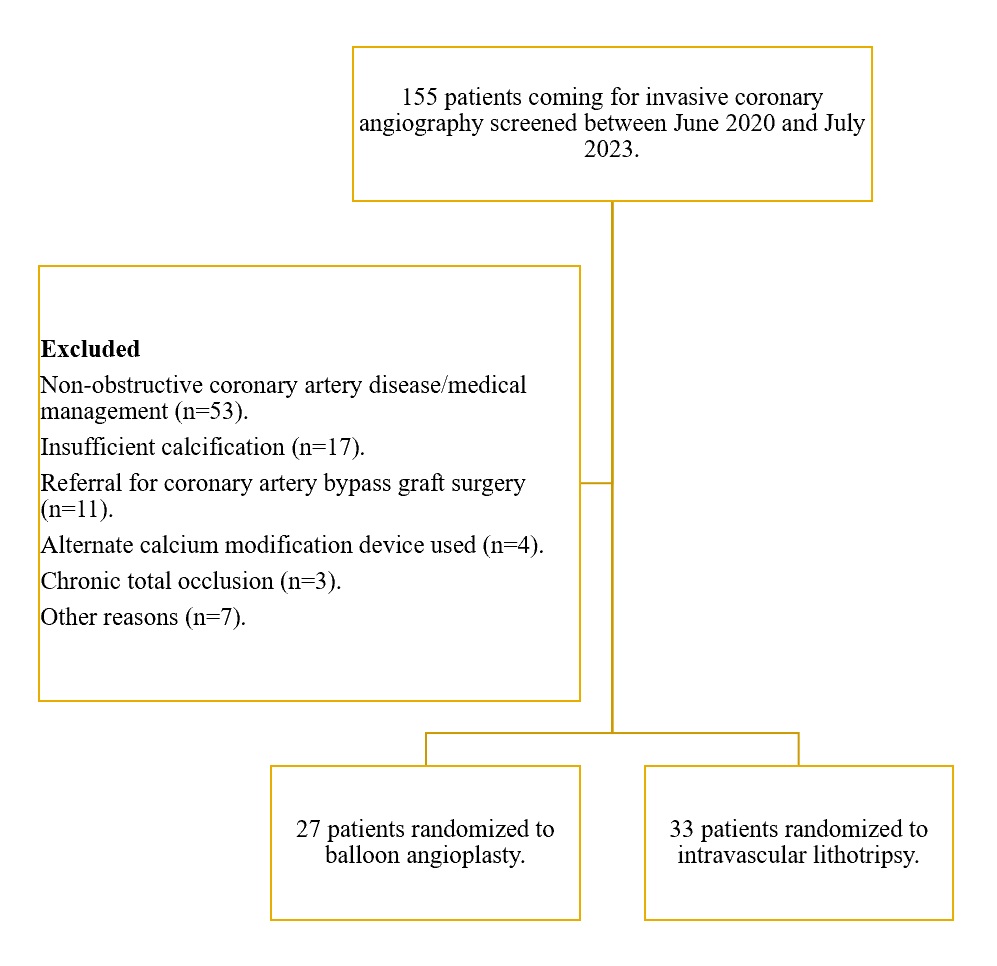
Between June 2020 and July 2023, a total of 155 patients were screened for the BASIL study, and 95 were excluded (Figure). Sixty patients were randomized to either BA (n = 27) or IVL (n = 33). The baseline demographics of the study population are shown in Table 1. The mean age was 70.5 ± 7.9 years and 40 (66.7%) were men. There were no significant differences between the groups, except more patients in the IVL group had a history of prior coronary artery bypass graft surgery. Most of the study participants underwent elective PCI for chronic coronary syndrome (n = 48, 80.0%).
Procedural characteristics
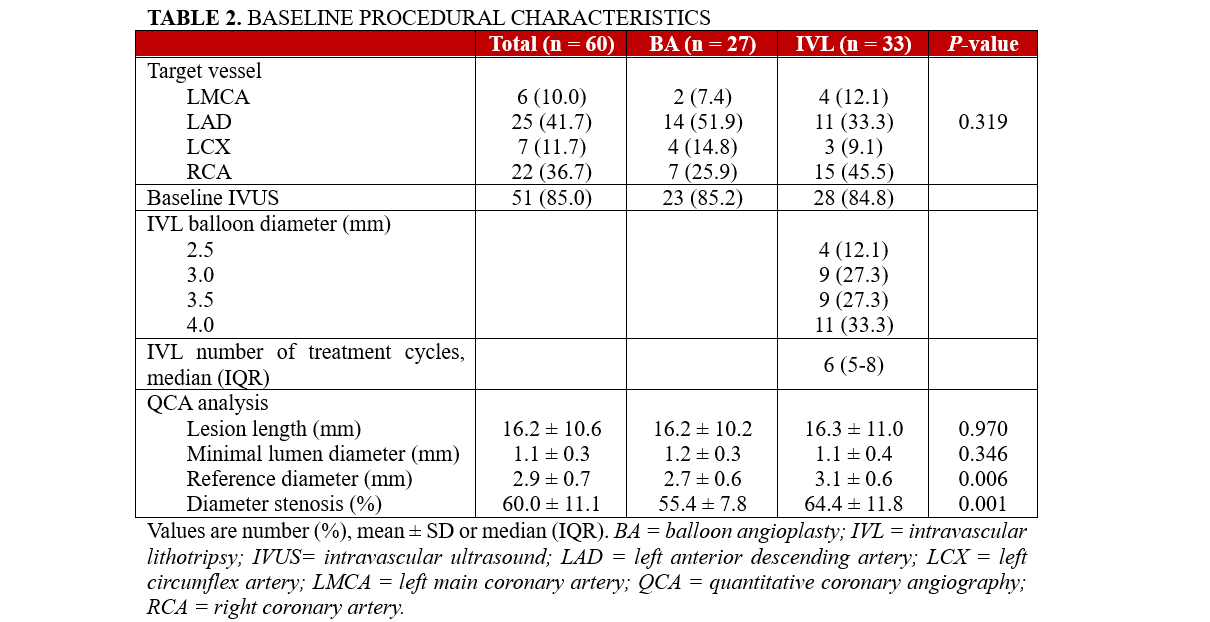
The left anterior descending artery (LAD) was the most common target vessel (42.7%), followed by the right coronary (RCA, 36.7%), left circumflex (LCX, 11.7%), and left main coronary arteries (LMCA, 10.0%). A baseline IVUS was performed in 51 patients (85.0%), with 9 patients (15.0%) included based on angiographic calcification. The mean minimal lumen diameter was 1.1 ± 0.3 mm, and the lesion length was 16.2 ± 10.6 mm on QCA analysis (Table 2). The IVL group had a larger reference vessel diameter than the BA group (3.1 ± 0.6 mm vs 2.7 ± 0.6 mm, P = .006), as well as a higher degree of diameter stenosis (64.4 ± 11.8% vs 55.4 ± 7.8%, P = .001). In the IVL group, the most used balloon catheter was 4.0 x 12 mm (33.3%), and the median number of lithotripsy cycles used was 6 (IQR 5-8).
Primary endpoints
The primary efficacy endpoint of procedural success was achieved in 15 of 27 (55.6%) patients in the BA group and 24 of 33 (72.7%) patients in the IVL group (P = .165). Significantly more patients treated with BA (n = 6 [22.2%]) required bailout calcium modification devices compared with IVL (n = 0 [0.0%]) (Table 3). Bailout calcium modification was performed either with cutting balloons (n = 5 [83.3%]) or IVL (n = 1 [16.7%]). Each group had 1 case of significant coronary artery dissection, and there were no perforations.
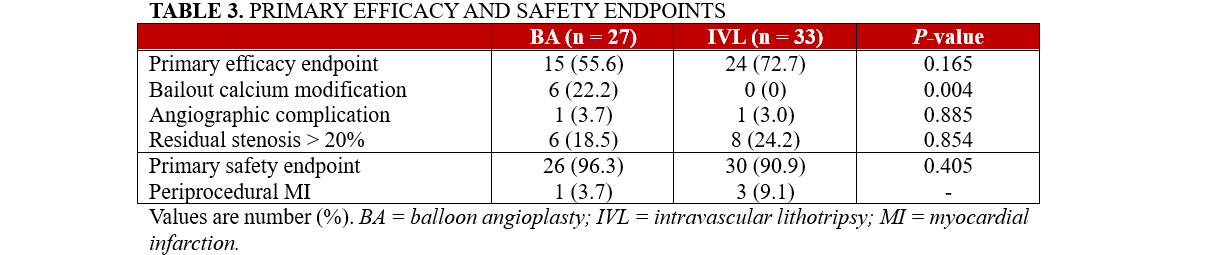
The primary safety endpoint of freedom from in-hospital MACE was achieved in 96.3% of the BA group and 90.9% of the IVL group (P = .405). One case of periprocedural MI occurred in the BA group and 3 cases occurred in the IVL group.
Secondary endpoints and IVUS characteristics
The baseline IVUS parameters are shown in Table 4 for the 51 patients with IVUS-crossable lesions. The minimal lumen area (MLA) was 2.55 ± 1.66 mm2, with no significant differences between groups. The IVL group had a greater maximum calcium arc (327.73 ± 55.04° vs 284.20 ± 87.02°, P = .035) and longer calcium length (33.83 ± 15.17 mm vs 23.37 ± 12.27 mm, P = .01) than the BA group.
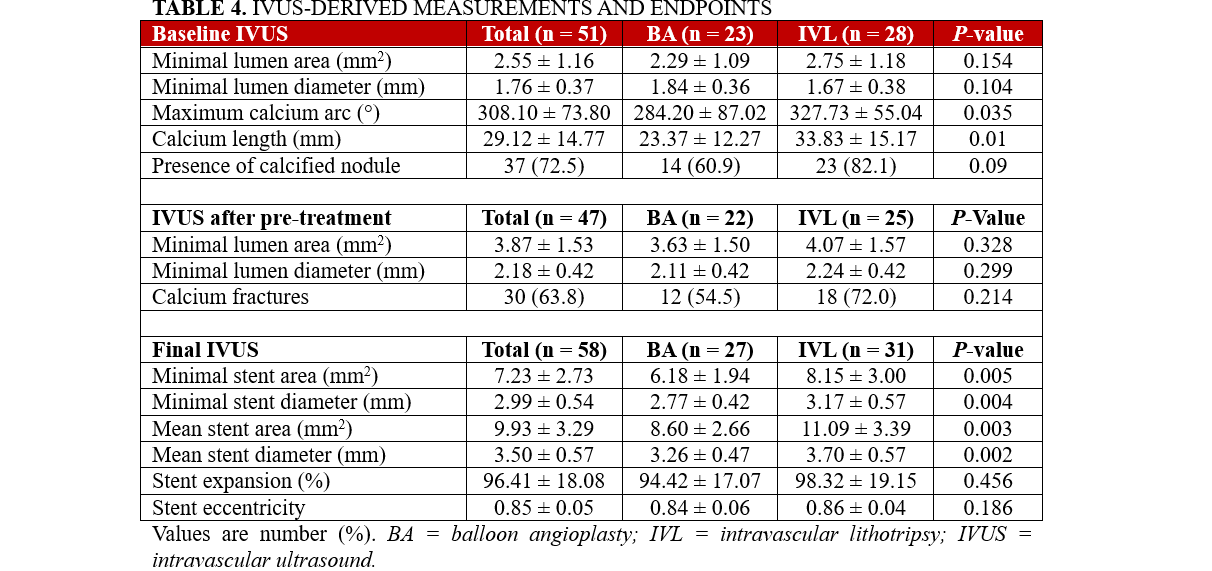
IVUS pullback after pre-treatment was performed on 47 patients. The MLA was 3.87 ± 1.53 mm. More calcium fractures were seen in the IVL group, though the difference was not statistically significant (72.0% vs 54.5%, P = .214).
Final IVUS pullbacks were analyzed in 58 patients; 2 patients in the IVL group had suboptimal IVUS for core laboratory analysis. The minimal stent area was significantly larger in the IVL group than in the BA group (8.15 mm2 vs 6.18 mm2, P = .005). The stent expansion was excellent in both groups (BA: 94.4 ± 17.1% vs IVL: 98.3 ± 19.1%, P = .456).
At 30-day follow-up, no additional MACE occurred following the index admission.
Discussion
To date, the BASIL study is the largest prospective RCT comparing IVL to BA during PCI. It is also the first RCT investigating IVL to utilize an independent core laboratory for QCA and IVUS analysis. Although the primary endpoint of procedural success did not reach statistical significance, there was a 17.1% absolute difference favoring treatment with IVL over BA prior to stenting. This could be a type II statistical error due to the small sample size. The 6 cases inadequately treated with BA and requiring bailout devices reflect real-world practice where an escalation in calcium modification is often necessary to achieve optimal stent outcomes. No bailout strategies were needed in the IVL group. The procedural success rate of 72.7% in the IVL group is lower than in the Disrupt CAD III study (92.4%) and the ORBIT II study of orbital atherectomy (88.9%).9,13 This is possibly due to the relatively strict criterion of a less than 20% post-stent residual stenosis used in the primary efficacy endpoint for the BASIL study compared with less than 50% in the other studies, which were designed for US Food and Drug Administration device approval.
The rates of freedom from in-hospital MACE for the BA and IVL groups were 96.3% and 90.1%, respectively; there were no 30-day MACE in either group. As IVL was a new device early in the BASIL study, operators were still learning the nuances of its use and potential pitfalls. One of the cases of periprocedural MI in the IVL group occurred in the treatment of an unprotected LMCA, where transient hemodynamic compromise occurred during treatment cycles. After such experiences, our operators now often retract the IVL balloon into the guiding catheter between treatment cycles when treating the LMCA to avoid prolonged ischemia, particularly when access to mechanical circulatory support devices is limited.
An interesting observation is the relatively mild diameter stenosis of the target lesions (60 ± 11.1%). Previous studies have shown that operators often overestimate diameter stenosis compared with subsequent core laboratory QCA.14 However, the mean target lesion MLA of 2.55 ± 1.16 mm2 at baseline strongly supports the functional significance of the treated lesions by IVUS-defined criteria.15-17
IVUS-defined optimal stent outcomes of MSA greater than 5.5 mm2 and stent expansion (MSA/distal reference lumen area) greater than 90% have been shown to improve clinical outcomes including cardiac death, stent thrombosis, and target lesion failure.18-20 The final MSA in the IVL group was significantly larger than the BA group in the BASIL study. Although the finding is at least partially explained by the larger reference vessel size in the IVL group, it is promising to see this despite the IVL group having a larger calcium arc, longer calcium length, and higher number of calcified nodules. Stent expansion was similar between the study groups and is a useful endpoint that is independent of differences in reference vessel size. Our findings are consistent with other small RCTs comparing IVL to BA and rotational atherectomy.21, 22
Although this was a small RCT, recruitment for the 60 patients took approximately 3 years because of several factors. First, the ethics committee required patient consent for trial inclusion to be conducted before their invasive coronary angiogram. Therefore, patients who were screened were those who had calcified disease on previous invasive or computed tomography coronary angiograms or had multiple risk factors associated with coronary calcification. Resource limitations did not allow for every patient who was referred for an invasive angiogram to be screened, and many patients could not give an informed consent on a stipulation of finding calcific disease on upcoming angiography. Secondly, the COVID pandemic affected the scheduling of many elective procedures, which accounted for most of our study population. Thirdly, the COVID pandemic also at times affected the supply of IVUS catheters, resulting in restrictions on use.
There are several strengths of the BASIL study. First, IVL is a balloon-based device, which allowed the cardiologists adjudicating angiographic complications to be properly blinded to the treatment group, as the angiographic appearance is similar to non-compliant balloons. Secondly, the choice of IVUS over optical coherence tomography allowed the inclusion of more patients with baseline imaging pullbacks without aggressive predilatation, as IVUS acquisition is not dependent on adequate blood clearance and flow in severely stenosed lesions. It also allowed for a greater subset of patients to be included in the study, including those with LMCA disease, renal failure, and aorto-ostial disease, which is reflective of a real-world cohort. Moreover, the trial was designed to compare IVL and BA while allowing operator-driven bailout calcium modification for patient safety. This allows for a more representative assessment of IVL, rather than upfront comparisons with other advanced calcium modification techniques. Lastly, the use of an independent core laboratory for QCA and IVUS removes the potential bias of measurements done by investigators, which may affect results, particularly in a small study.
Limitations
The present study has several limitations. First, formal power calculation was not done, as the small number of enrolled patients was not expected to show a difference in major clinical endpoints in the BASIL study. The study population size of 60 patients was chosen to match the size of the DISRUPT CAD I study, the only published data on IVL at the time of study design. Therefore, the results of the present study should be interpreted with caution. Secondly, predilatation with small balloons to allow passage of the IVUS catheter will have a small impact on baseline measurements; furthermore, some patients did not get baseline IVUS assessment. Third, the failure of BA as the randomized treatment was at the operator’s discretion, including balloon size and inflation pressures.
Conclusions
In the prospective, randomized BASIL study, IVL did not differ from BA in achieving procedural success during PCI in severely calcified lesions. Both treatment strategies were safe and achieved excellent stent expansion. Lesions pretreated by IVL resulted in a larger final MSA compared with conventional BA.
Affiliations and Disclosures
Bernard Wong, MBChB; Guy Armstrong, MBChB; Timothy Glenie, MBChB; Ali Khan, MBBS; Ruth Newcombe, DCR; Hector Gonzales, BSN; Seif El-Jack, MBBS
From the Cardiovascular Unit, North Shore Hospital, Auckland, New Zealand.
Acknowledgments: The authors would like to thank the staff at the Cardiovascular Unit at North Shore Hospital for their assistance during the recruitment period. Dr Wong would like to thank the New Zealand Heart Foundation and A.H. Couch Auckland Heart Trust for their support during his doctoral studies.
Disclosures: Dr Wong has received speaker honoraria from Bio-Excel. Dr. Armstrong is a shareholder in Shockwave Medical Inc. Dr El-Jack is a shareholder in Shockwave Medical Inc. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Funding: The BASIL study was supported by an investigator-initiated research grant from Shockwave Medical, Inc. Shockwave Medical, Inc. had no influence on the study design, data analysis, or manuscript writing.
Address for correspondence: Bernard Wong, MBChB, Department of Cardiology, North Shore Hospital, 124 Shakespeare Road, Takapuna, Auckland 0620, New Zealand. Email: bernardwong@hotmail.co.nz. X: @Bernard_TW_Wong
References
1. Hennessey B, Pareek N, Macaya F, et al. Contemporary percutaneous management of coronary calcification: current status and future directions. Open Heart. 2023;10(1):e002182. doi:10.1136/openhrt-2022-002182
2. Mosseri M, Satler LF, Pichard AD, Waksman R. Impact of vessel calcification on outcomes after coronary stenting. Cardiovasc Revasc Med. 2005;6(4):147-153. doi:10.1016/j.carrev.2005.08.008
3. Dangas GD, Claessen BE, Caixeta A, Sanidas EA, Mintz GS, Mehran R. In-stent restenosis in the drug-eluting stent era. J Am Coll Cardiol. 2010;56(23):1897-1907. doi:10.1016/j.jacc.2010.07.028
4. Sakakura K, Ako J, Wada H, et al. Comparison of frequency of complications with on-label versus off-label use of rotational atherectomy. Am J Cardiol. 2012;110(4):498-501. doi:10.1016/j.amjcard.2012.04.021
5. Sakakura K, Ito Y, Shibata Y, et al. Clinical expert consensus document on rotational atherectomy from the Japanese association of cardiovascular intervention and therapeutics: update 2023. Cardiovasc Interv Ther. 2023;38(2):141-162. doi:10.1007/s12928-022-00906-7
6. Kereiakes DJ, Virmani R, Hokama JY, et al. Principles of intravascular lithotripsy for calcific plaque modification. JACC Cardiovasc Interv. 2021;14(12):1275-1292. doi:10.1016/j.jcin.2021.03.036
7. Brinton TJ, Ali ZA, Hill JM, et al. Feasibility of Shockwave coronary intravascular lithotripsy for the treatment of calcified coronary stenoses. Circulation. 2019;139(6):834-836. doi:10.1161/CIRCULATIONAHA.118.036531
8. Ali ZA, Nef H, Escaned J, et al. Safety and effectiveness of coronary intravascular lithotripsy for treatment of severely calcified coronary stenoses: the Disrupt CAD II study. Circ Cardiovasc Interv. 2019;12(10):e008434. doi:10.1161/CIRCINTERVENTIONS.119.008434
9. Hill JM, Kereiakes DJ, Shlofmitz RA, et al; Disrupt CAD III Investigators. Intravascular lithotripsy for treatment of severely calcified coronary artery disease. J Am Coll Cardiol. 2020;76(22):2635-2646. doi:10.1016/j.jacc.2020.09.603
10. Wong B, El-Jack S, Newcombe R, Glenie T, Armstrong G, Khan A. Shockwave intravascular lithotripsy for calcified coronary lesions: first real-world experience. J Invasive Cardiol. 2019;31(3):46-48.
11. Mintz GS, Popma JJ, Pichard AD, et al. Patterns of calcification in coronary artery disease. A statistical analysis of intravascular ultrasound and coronary angiography in 1155 lesions. Circulation. 1995;91(7):1959-1965. doi:10.1161/01.cir.91.7.1959
12. Thygesen K, Alpert JS, Jaffe AS, et al; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth universal definition of myocardial infarction (2018). J Am Coll Cardiol. 2018;72(18):2231-2264. doi:10.1016/j.jacc.2018.08.1038
13. Chambers JW, Feldman RL, Himmelstein SI, et al. Pivotal trial to evaluate the safety and efficacy of the orbital atherectomy system in treating de novo, severely calcified coronary lesions (ORBIT II). JACC Cardiovasc Interv. 2014;7(5):510-518. doi:10.1016/j.jcin.2014.01.158
14. Nallamothu BK, Spertus JA, Lansky AJ, et al. Comparison of clinical interpretation with visual assessment and quantitative coronary angiography in patients undergoing percutaneous coronary intervention in contemporary practice: the Assessing Angiography (A2) project. Circulation. 2013;127(17):1793-1800. doi:10.1161/CIRCULATIONAHA.113.001952
15. Koo BK, Yang HM, Doh JH, et al. Optimal intravascular ultrasound criteria and their accuracy for defining the functional significance of intermediate coronary stenoses of dif 4ffa ferent ffa locations. JACC Cardiovasc Interv. 2011;4(7):803-811. doi:10.1016/j.jcin.2011.03.013
16. Waksman R, Legutko J, Singh J, et al. FIRST: fractional flow reserve and intravascular ultrasound relationship study. J Am Coll Cardiol. 2013;61(9):917-923. doi:10.1016/j.jacc.2012.12.012
17. Koo BK, Hu X, Kang J, et al; FLAVOUR Investigators. Fractional flow reserve or intravascular ultrasonography to guide PCI. N Engl J Med. 2022;387(9):779-789. doi:10.1056/NEJMoa2201546
18. Hong SJ, Kim BK, Shin DH, et al; IVUS-XPL Investigators. Effect of intravascular ultrasound-guided vs angiography-guided everolimus-eluting stent implantation: the IVUS-XPL randomized clinical trial. JAMA. 2015;314(20):2155-2163. doi:10.1001/jama.2015.15454
19. Zhang J, Gao X, Kan J, et al. Intravascular ultrasound versus angiography-guided drug-eluting stent implantation: the ULTIMATE trial. J Am Coll Cardiol. 2018;72(24):3126-3137.
20. Lee YJ, Zhang JJ, Mintz GS, et al. Impact of intravascular ultrasound–guided optimal stent expansion on 3-year hard clinical outcomes. Circ Cardiovasc Interv. 2021;14(10):e011124. doi:10.1161/CIRCINTERVENTIONS.121.011124
21. Blachutzik F, Meier S, Weissner M, et al. Comparison of coronary intravascular lithotripsy and rotational atherectomy in the modification of severely calcified stenoses. Am J Cardiol. 2023;197:93-100. doi:10.1016/j.amjcard.2023.02.028
22. Oomens T, Vos NS, van der Schaaf RJ, et al. EXpansion of stents after intravascular lithoTripsy versus conventional predilatation in CALCified coronary arteries. Int J Cardiol. 2023;386:24-29. doi:10.1016/j.ijcard.2023.05.012













