


Balloon Venoplasty for Right Heart Catheterization From the Arm in Patients With Subclavian Vein Stenosis
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Abstract
Objectives. In the transradial era, arm venous access for right heart catheterization (RHC) is rising. Procedural success is affected by many factors, including subclavian/innominate vein stenosis (SVS) and pre-existing wires or catheters. In a study published previously by the same authors, 2% of cases had unsuccessful RHC through the arm, predominantly due to SVS. Since that study, techniques to improve RHC success rates have been developed, including crossing the stenosis with a coronary guidewire, followed by balloon dilatation. We aimed to determine whether subclavian/innominate venoplasty allows successful RHC in patients with SVS.
Methods. Our retrospective study included patients who had RHC from the arm between November 1, 2019 and December 31, 2022 that was unsuccessful due to the inability to pass a catheter through the SVS, and then underwent balloon venoplasty. The success rate of completed RHC was then assessed.
Results. Out of 2506 RHCs via arm access, 2488 were successful with a catheter alone or over a guidewire. In 18 patients, venoplasty was needed for catheter passage over a guidewire. Post-dilatation, all 18 cases (100%) had successful RHC with a mean procedural time of 35.2 (SD = 15.5) minutes. The most common stenosis site was the subclavian vein in 13 patients (72.2%), and 12 patients (66.7%) had pacemaker/ implantable cardioverter defibrillator wires present.
Conclusions. Balloon dilatation of SVS is an efficacious method to improve the success rate of RHC from the arm. It is a safe technique that may prevent cross-over to a different access site, thereby improving patient satisfaction and reducing the possibility of alternate site complications.
Introduction
With the increasing use of radial access for coronary angiography and percutaneous interventions, arm access for right heart catheterization (RHC) is rising. Venous arm access is safe, highly successful,1 and avoids jugular and femoral venous access complications.2 Previous studies of ultrasound-guided arm venous access for RHC have shown failure rates of approximately 2% to 8%.1,2 Pacemaker/implantable cardioverter defibrillator (ICD) wires and/or subclavian/innominate vein stenoses (SVS) cause most of these failures.1 There have been reports of subclavian and innominate vein balloon venoplasty to overcome these stenoses for implantation of a permanent pacemaker.3-5 To our knowledge, no studies have reviewed the possible benefits of venoplasty to achieve higher success rates of RHC from the arm in patients with SVS.
The primary objective of our study was to explore if balloon dilatation/venoplasty of SVS would allow successful RHC through arm access in cases when a standard balloon-tip right heart catheter would not pass. The secondary objective was to record complications associated with balloon venoplasty.
Methods
Study population and data. We conducted a retrospective observational study at Memorial Healthcare System (MHS) in Hollywood, Florida; the study was approved by the MHS Institutional Review Board and consent was waived. The study included all patients who underwent failed RHC due to SVS preventing successful passage of a catheter over a wire and who subsequently had venous balloon dilatation from November 1, 2019 to December 31, 2022. Patient demographics (age, gender, and body mass index), indications for RHC, prior use of antiplatelet/anticoagulation, previous ipsilateral upper extremity/chest surgery or trauma, and prior indwelling central venous catheters were recorded. Procedural details included the type of procedure (RHC or both left/RHC), heparin use, sheath size, access site, guidewire type and size, balloon type and size, maximum balloon diameter, balloon compliance, maximal inflation pressure, and duration of inflation at maximal pressure. Outcome data, including successful RHC, procedural time, and procedural complications, were also collected and entered into the database.
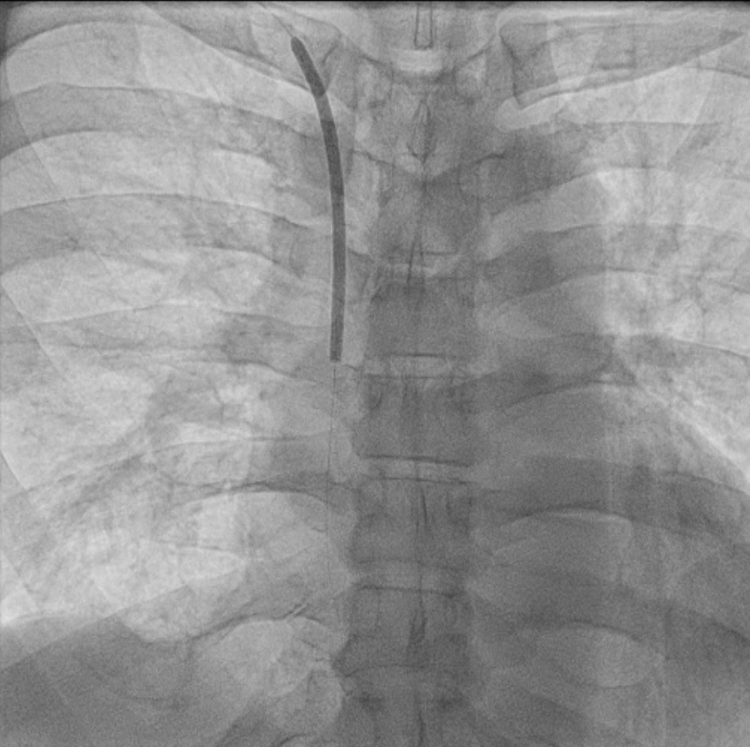
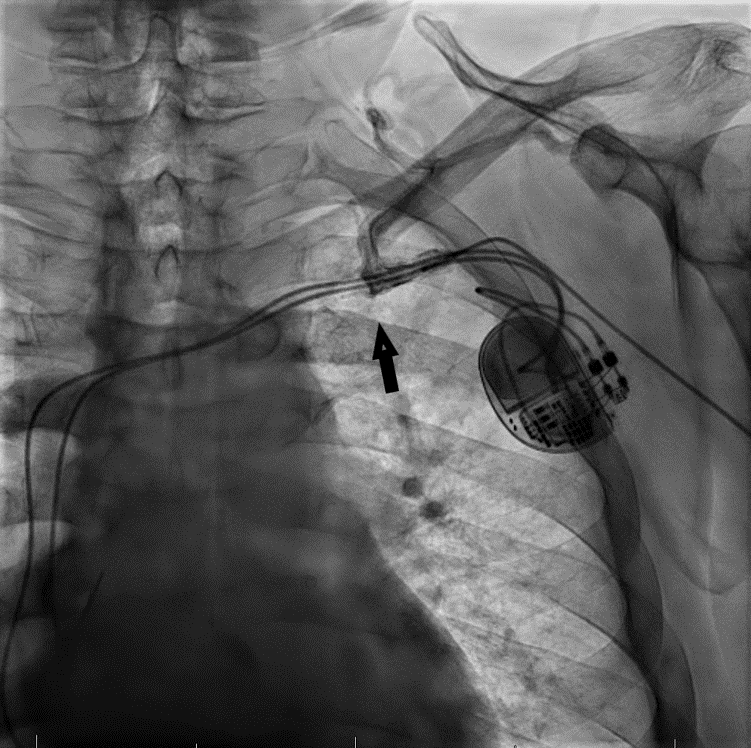
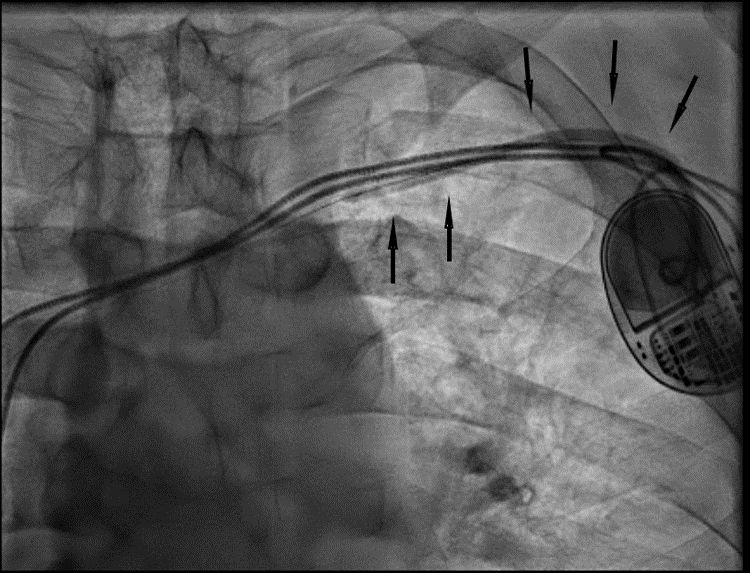
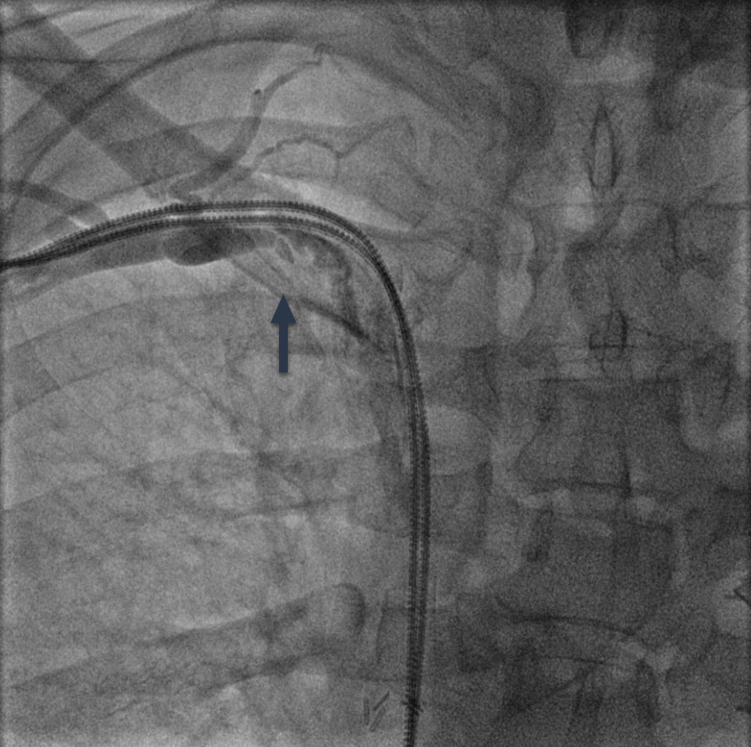
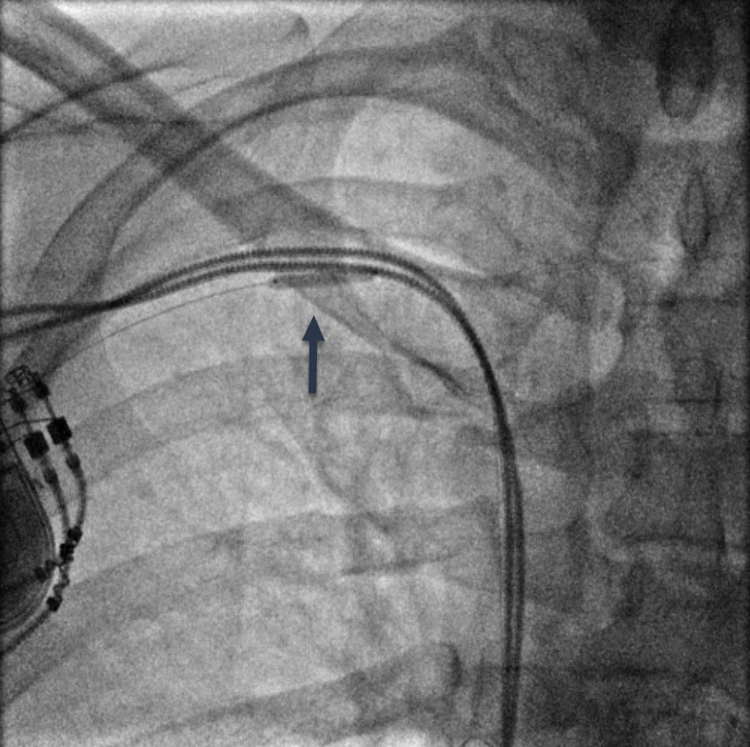
RHC procedure. Arm venous access was obtained with ultrasound guidance in all cases. After successful ‘radial’ sheath insertion, a 5-French (Fr) or 6-Fr balloon flotation right heart catheter was advanced (either by itself or over a 0.014-inch coronary guidewire based on operator preference) through the sheath and then into the pulmonary artery (PA). If resistance to catheter passage was encountered, a venogram (Figures 1A, 2A, and 3A) was performed using diluted contrast (50% saline) to determine the venous anatomy, the location, and the extent of stenosis, and to guide further wire/catheter advancement. In some cases, using different guidewires or catheters (eg, downsizing a 6 Fr to a 5 Fr) allowed RHC success. When a 0.014-inch wire was advanced into the superior vena cava (SVC) and the passage of a balloon-tip right heart catheter over the wire was unsuccessful due to a stenosis and/or pacemaker/ICD wires, a coronary balloon or 0.014-inch compatible peripheral balloon was then advanced over the wire and dilatation of the stenosis was performed (Figures 1B, 2B, and 3B). In some cases, a single balloon dilatation allowed passage of the RHC catheter. In others, a progressive increase in balloon diameters was needed. At the end of the procedure, the venous sheath was withdrawn, and manual compression was applied to the puncture site until hemostasis was attained.

Outcome measures. The primary endpoint of the study was the success rate of RHC following balloon dilatation of venous stenosis after a failed initial attempt at RHC catheter passage over a 0.014-inch coronary wire. Successful RHC was defined as the advancement of the catheter through the right heart chambers into the PA. Secondary endpoints were procedural time and complications. RHC procedure time was defined as the time between the first attempt to pass a guidewire or the right heart catheter (whichever was attempted first) through the venous sheath and then successful passage of the catheter into the PA. Complications were defined as access site hematoma, bleeding, and subclavian/brachiocephalic vein injuries, including dissection, rupture, or aneurysm/pseudo-aneurysm formation.
Statistical analysis. A descriptive analysis was performed to summarize the demographic and clinical characteristics of the patients. Data for continuous variables with normal distribution was expressed as means and standard deviations (SD) or, if variables were not normally distributed, as medians and ranges. The Shapiro-Wilk test was used to test for the normality of the data distribution. Categorical variables were expressed as numbers of patients and percentages.
Results
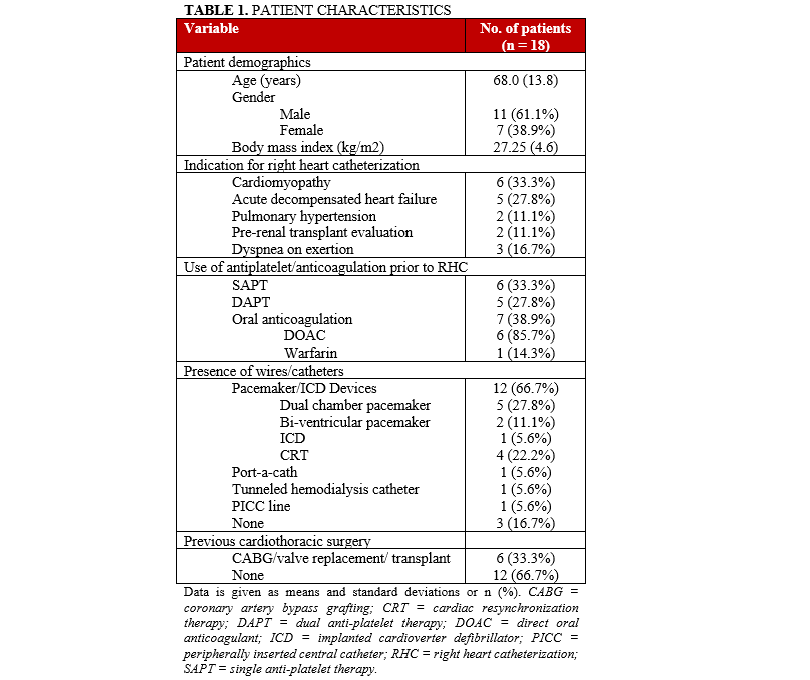
During the study period, a total of 2625 RHC procedures were recorded, out of which 2506 patients had arm access. Of the cases from the arm, 2488 (99%) had successful RHC by passage of a right heart catheter either by itself or over a guidewire into the pulmonary artery. The remaining 18 patients (1%) had unsuccessful attempts at passing a right heart catheter over a 0.014-inch coronary guidewire that was in the SVC or right atrium due to venous stenosis anywhere in the venous system from the brachial vein up to the SVC. Patient characteristics are listed in Table 1. Twelve patients (66.7%) had pacemaker/ICD wires, with 11 being on the left and 1 on the right side. Three patients (16.7%) had present or prior ipsilateral central venous catheters. One patient had a prior RHC from the ipsilateral extremity, which was performed successfully 1 week before this procedure without needing an intervention, however, the subsequent RHC required balloon dilatation.
Procedural characteristics are listed in Table 2. Access was obtained in the right arm in 7 patients (38.9%) and the left arm in 11 patients (61.1%), driven by the operator preference. In 1 case, a failed first attempt to obtain venous access was successfully switched to the contralateral side. The most common site of venous stenosis was the subclavian vein in 13 patients (72.2%). Other sites of venous stenoses were the innominate vein, the basilic vein, and the SVC, each in 1 patient, respectively; and multiple segments in 2 patients.
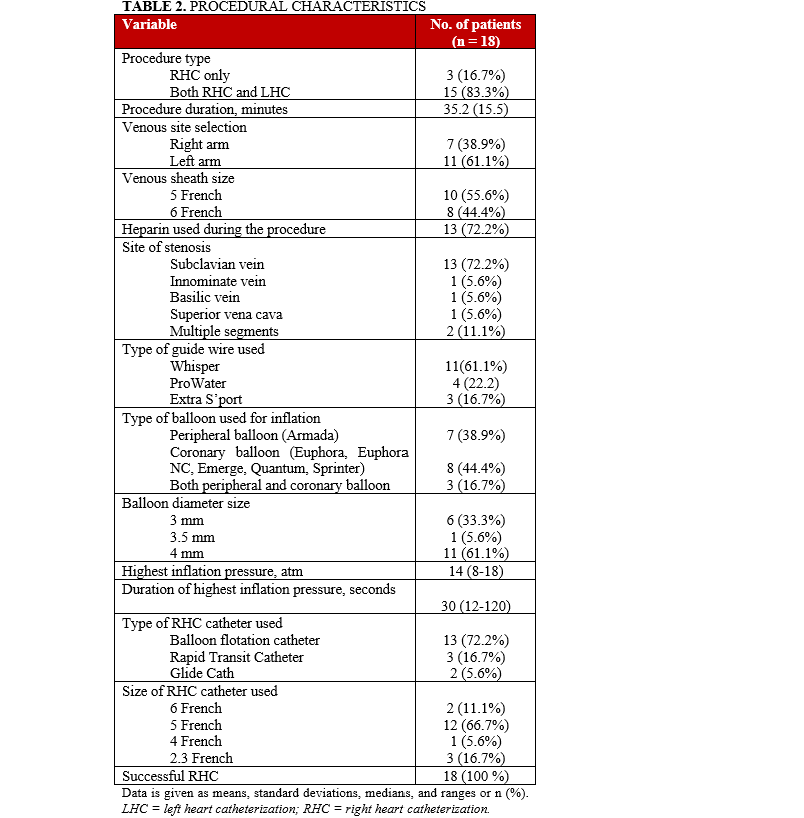
We were able to pass a guidewire through all stenoses. A coronary or peripheral balloon catheter was then passed over the guidewire, and dilatation was performed (Figures 1B, 2B, and 3B). Coronary angioplasty balloons were utilized in 8 (44.4%), peripheral balloons in 7 (38.9%), and both peripheral and coronary balloons in 3 patients (16.7%). The balloons used were predominantly non-compliant (83.3%). Eleven patients (61.1%) required only a single balloon for successful venoplasty, while 7 patients (38.9%) had at least 2 balloons used, upsizing from the previously used balloon. The balloons' median diameter and length were 4 mm (range, 3-4 mm) and 60 mm (range, 20-200 mm), respectively. The median highest inflation pressure used was 14 atm (range, 8-18). After SVS dilatation, we performed successful RHC in 100% of the cases with a catheter passed into the PA. The average length of the procedure for successful RHC was 35.2 ± 15.5 minutes. There were no complications at the end of the procedure in any of our patients.
Discussion
In 1929, Werner Forssmann accessed his left antecubital vein to perform his own RHC, the first-ever human cardiac catheterization.6 RHC has since become a regularly used technique for diagnosis and guiding therapy in various medical conditions.7 Central venous access through the femoral, internal jugular, and subclavian veins has traditionally been used because of large vessel diameters and easy accessibility. Accessing these central veins is usually associated with low mortality and morbidity rates when performed by skilled operators. Even so, with any of these approaches, RHC is still susceptible to complications, including inadvertent arterial access, hematoma, bleeding, arteriovenous fistula, infection, and delayed discharge due to extended bed rest.8
Arterial access for coronary and peripheral procedures has shifted from the femoral artery to the radial artery in many catheterization labs, due to the advantages it offers to patients and healthcare systems.8,9 Venous access has followed this shift to the arm, with RHC being increasingly performed from the arm in many centers. As techniques have evolved to improve success in radial procedures, thereby reducing crossover to a secondary arterial access site,10,11 techniques must evolve to improve success in RHC from the arm. Herein, we describe our simple method of venoplasty for improving success rates of RHC from the arm, thereby nearly eliminating crossover to secondary venous access.
Our very high success rate of arm venous access1 is secondary to real-time ultrasound-guided access,12 and we strongly recommend this technique. We preferentially access the deeper brachial and basilic veins, as these are usually ‘straighter shots’ up the medial aspect of the arm to the subclavian vein. However, we occasionally access the more superficial antecubital vein(s), and sometimes the deeper median or more lateral cephalic vein. In our catheterization lab, unsuccessful RHC from the arm is rarely due to the inability to obtain venous access in the arm. Instead, it is a result of failure to advance a wire and/or catheter through the SVS. In our study, the most common reason for SVS was the presence of wires for pacemaker/ICD devices, which occurred in 12 cases (66.7%). Three patients (16.7%) had either a port-a-cath, tunneled catheter for hemodialysis in place, or a history of prolonged peripherally inserted central catheter (PICC) line. Three patients (16.7%) had no pre-existing wires/catheters on the ipsilateral side, of which 2 patients had prior cardiac surgeries.
The incidence of venous obstruction in patients with cardiovascular implantable electronic devices or central venous catheters is variably reported. According to a recently published study in a large nationwide sample, the incidence of symptomatic lead-related venous obstruction is 5% after 5 years, impacting 1 out of every 20 patients with implantable devices.13 Devices with more than 1 lead are more likely to be associated with the development of lead-related venous obstruction. However, the actual incidence of venous stenosis/obstruction, especially when most cases are asymptomatic, is difficult to ascertain. It is estimated that 25% of the patient population post-catheter or device implantation demonstrates some degree of obstruction (> 70%) on subsequent venography studies, with less than 10% exhibiting total occlusion.14 The incidence ranges widely from 14% to 64%, depending on various studies.15-17 One study reported it to be 33%, where greater than 60% diameter narrowing was defined as obstruction,17 while another retrospective study showed that 51% of patients had greater than 50% stenosis after pacemaker/ICD implantation.18
Subclavian venoplasty is recognized by the Heart Rhythm Society Expert Consensus Statement as a safe and reliable procedure when venous stenoses hinder central venous access.19 One study included 130 patients who underwent percutaneous subclavian venoplasty (PSV) for lead-related subclavian vein stenoses.5 In patients with wire refractory obstruction, mechanical (microdissection) or power (laser or radiofrequency) assistance was utilized. In this study, PSV was not associated with any significant complication. Minor complications did occur, including balloon rupture with contrast extravasation in 3 patients, but there were no reported clinical implications. Our small single-center experience also demonstrated that subclavian vein balloon venoplasty is practical, effective, and safe. We purposely used balloon diameters (3-4 mm) that were significantly smaller than the diameter of the subclavian vein (10-20 mm) to prevent vein injury/perforation. Earlier in our experience, we would often initially perform venoplasty with a 3-mm diameter balloon. More than one-third of the time, a right heart catheter could not be passed in these cases, requiring subsequent dilatation with a larger 4-mm diameter balloon. Over time our technique evolved to initial use of 4-mm diameter balloons in most cases to improve the efficacy of venoplasty.
Although venoplasty of an SVS can be performed, its long-term effectiveness may be suboptimal because of elastic recoil and intimal injury, which cause thrombosis and/or intimal hyperplasia.20 Compared to conservative therapy, percutaneous revascularization in lead-related venous obstruction has not been linked to reduced healthcare utilization.13 This reinforces the notion that revascularization alone is insufficient for long-term patency and may only provide transient relief. Nevertheless, subclavian venoplasty in right heart catheterization offers a temporary ‘quick fix,’ which may be all that is needed to allow completion of the procedure and to prevent crossover to another venous access site. This avoids the need to prepare secondary access sites and instrumentation, thereby decreasing the risk of complications and patient discomfort. When balloon dilation was performed, the total length of the procedure in our study was longer (35.2 ± 15.5 minutes) compared with our prior case series of successful standard RHC from the arm (5.7 ± 3.4 minutes).1 This additional procedural time of approximately 30 minutes was expected because of the additional time needed for venoplasty. As our experience with venoplasty has increased, the procedural times have decreased. Of note, the operators performing RHC during this study were the same as in the previous study.
Limitations. The limitations of our study include that it is a single-center, retrospective, observational study. There was no contemporary control group of successful RHC, so we used data from a previous study as historical controls.1 Also, the operators in this study are very experienced radial operators who use ultrasound guidance for every arterial and venous access, and their results may not be replicated by operators who are accustomed to lower volume and are less experienced.
Conclusions
Subclavian venoplasty provides a safe and effective technique to complete RHC from the arm when subclavian venous stenoses impedes the advancement of a right heart catheter. This eliminates the need to switch to femoral or internal jugular venous access in our small case series, and thus avoids the complications associated with these alternative venous access sites. We believe this technique will improve patient satisfaction and safety when RHC is attempted from the arm and subclavian venous stenosis is encountered. Larger studies will be needed to assess the true safety and efficacy of subclavian venoplasty to allow completion of RHC from the arm.
Affiliations and Disclosures
From the 1Department of Cardiovascular Disease, Memorial Healthcare System, Florida, USA; 2Office of Human Research, Memorial Healthcare System, Florida, USA.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Kishor Khanal, MD, 2516 Centergate Dr., Apt. 305, Miramar, FL 33025, USA. Email: medicalresearch.kk@gmail.com; X: @kkhanalmd
References
1. Roberts JS, Niu J, Alexander C, Pastor-Cervantes JA. Real-time ultrasound-guided venous access of the arm for right heart catheterization. J Invasive Cardiol. 2019;31(7):E170-E176.
2. Roule V, Ailem S, Legallois D, et al. Antecubital vs femoral venous access for right heart catheterization: benefits of a flashback. Can J Cardiol. 2015;31(12):1497.e1-6. doi:10.1016/j.cjca.2015.04.026
3. Sudhakar BG. Left subclavian and innominate vein balloon venoplasty followed by permanent pacemaker implantation: a case report. J Innov Card Rhythm Manag. 2019;10(7):3738-3742. doi:10.19102/icrm.2019.100704
4. Chow DH, Choy CC, Chan NY. Idiopathic left innominate vein stenosis during pacemaker implantation with venoplasty in a retrograde approach. HeartRhythm Case Rep. 201628;2(4):310-312. doi: 10.1016/j.hrcr.2016.03.006
5. Worley SJ. Implant venoplasty: dilation of subclavian and coronary veins to facilitate device implantation: indications, frequency, methods, and complications. J Cardiovasc Electrophysiol. 2008;19(9):1004-1007. doi: 10.1111/j.1540-8167.2008.01217.x
6. Forssmann W. Die Sondierung des Rechten Herzens. Klin Wochenschr. 1929;8(45):2085-2087. doi:10.1007/BF01875120
7. Valle FH, Wainstein RV, Matte BS, et al. Ultrasound-guided antecubital vein approach for right heart catheterisation in a Brazilian tertiary centre. Open Heart. 2020;7(1):e001181. doi:10.1136/openhrt-2019-001181
8. D’Amario D, Burzotta F, Leone AM, et al. Feasibility and safety of right and left heart catheterization via an antecubital fossa vein and the radial artery in patients with heart failure. J Invasive Cardiol. 2017;29(9):301-308.
9. Pristipino C, Trani C, Nazzaro MS, et al. Major improvement of percutaneous cardiovascular procedure outcomes with radial artery catheterisation: results from the PREVAIL study. Heart. 2009;95(6):476-482. doi:10.1136/hrt.2008.150714
10. Mitchell MD, Hong JA, Lee BY, Umscheid CA, Bartsch SM, Don CW. Systematic review and cost–benefit analysis of radial artery access for coronary angiography and intervention. Circ Cardiovasc Qual Outcomes. 2012;5(4):454-462. doi:10.1161/CIRCOUTCOMES.112.965269
11. Baumann F, Roberts JS. Evolving techniques to improve radial/ulnar artery access: crossover rate of 0.3% in 1,000 consecutive patients undergoing cardiac catheterization and/or percutaneous coronary intervention via the wrist. J Interv Cardiol. 2015;28(4):396-404. doi:10.1111/joic.12213
12. Seto AH, Roberts JS, Abu-Fadel MS, et al. Real-time ultrasound guidance facilitates transradial access: RAUST (radial artery access with ultrasound trial). JACC Cardiovasc Interv. 2015;8(2):283-291. doi:10.1016/j.jcin.2014.05.036
13. Ferro EG, Kramer DB, Li S, et al. Incidence, treatment, and outcomes of symptomatic device lead-related venous obstruction. J Am Coll Cardiol. 2023;81(24):2328-2340. doi:10.1016/j.jacc.2023.04.017
14. Haghjoo M, Nikoo MH, Fazelifar AF, Alizadeh A, Emkanjoo Z, Sadr-Ameli MA. Predictors of venous obstruction following pacemaker or implantable cardioverter-defibrillator implantation: a contrast venographic study on 100 patients admitted for generator change, lead revision, or device upgrade. Europace. 2007;9(5):328-332. doi: 10.1093/europace/eum019
15. Da Costa SS, Scalabrini Neto A, Costa R, Caldas JG, Martinelli Filho M. Incidence and risk factors of upper extremity deep vein lesions after permanent transvenous pacemaker implant: a 6-month follow-up prospective study. Pacing Clin Electrophysiol. 2002;25(9):1301-1306. doi: 10.1046/j.1460-9592.2002.01301.x
16. Korkeila P, Nyman K, Ylitalo A, et al. Venous obstruction after pacemaker implantation. Pacing Clin Electrophysiol. 2007;30(2):199-206. doi:10.1111/j.1540-8159.2007.00650.x
17. Oginosawa Y, Abe H, Nakashima Y. The incidence and risk factors for venous obstruction after implantation of transvenous pacing leads. Pacing Clin Electrophysiol. 2002;25(11):1605-1611. doi:10.1046/j.1460-9592.2002.01605.x
18. Abu‐El‐Haija B, Bhave PD, Campbell DN, et al. Venous stenosis after transvenous lead placement: a study of outcomes and risk factors in 212 consecutive patients. J Am Heart Assoc. 2015;4(8):e001878. doi:10.1161/JAHA.115.001878
19. Kusumoto FM, Schoenfeld MH, Wilkoff BL, et al. 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm. 2017;14(12):e503-e551. doi:10.1016/j.hrthm.2017.09.001
20. Bolad I, Karanam S, Mathew D, John R, Piemonte T, Martin D. Percutaneous treatment of superior vena cava obstruction following transvenous device implantation. Catheter Cardiovasc Interv. 2005;65(1):54-59. doi:10.1002/ccd.20326










