


Clinically Significant Incidental Findings on CT Imaging During TAVI Work-up: A Systematic Review and Meta-Analysis
Abstract
Background. The transcatheter aortic valve implantation (TAVI) population is mostly elderly and frail. Clinically significant incidental findings (SIFs) are commonly encountered in the work-up of TAVI patients. This is a systematic review of current literature on the occurrence of SIFs on computed tomography (CT) imaging preceding TAVI and their association with mortality, delayed planning, and procedure cancellation. Methods. A systematic search on Medline, Embase, and Cochrane resulted in 19 retrospective studies (published from 2010-2020) reporting SIFs in the work-up for TAVI. A total of 6358 individuals from 19 studies were analyzed, with mean age of 80 years and sex equally divided. A random-effects meta-analysis was performed, with weighting based on study size. Results. Pooled prevalence of patients with SIF was 22.2% (95% confidence interval [CI], 17.8-26.6) and most findings (48.3%) were found in the lungs. Pooled prevalence of new malignancies was 3.4% (95% CI, 2.5-4.4). Higher mortality in patients with SIF was only found in studies with a follow-up period >4 years (hazard ratio, 1.5-1.7). TAVI was more frequently cancelled in patients with SIF vs those with no SIF (ranges, 10.1%-47.1% vs 5.2%-37.0%, respectively). SIF did not delay time to TAVI (ranges, 6-91 days in SIF patients vs 4-81 days in non-SIF patients). Conclusion. SIFs are common in patients screened for TAVI. SIF is associated with a higher risk of TAVI cancellation and with increased mortality risk over the long term, which should be taken into consideration in decision making. These findings may help inform patients and aid patient selection.
J INVASIVE CARDIOL 2022;34(3):E218-E225.
Key words: malignant incidental findings, meta-analysis, mortality, significant incidental findings, survival, TAVI
Introduction
Computed tomography (CT) scans prior to transcatheter aortic valve implantation (TAVI) are mandatory to assess the best access route and determine the size and type of the aortic valve prosthesis.1,2 Since most TAVI procedures are done in elderly patients, significant incidental findings (SIFs) in preprocedural imaging are common and are frequently discussed in heart team meetings. Many of these findings (eg, cysts) have no or little clinical impact. However, various findings (mostly malignancies or potentially malignant findings) might have important clinical implications, warranting further investigation and potentially causing delay of the TAVI procedure. Current guidelines recommend an estimated life expectancy of at least 1 year for receiving a TAVI procedure, which might be influenced by SIFs.3 Since long-term survival after TAVI is also dependent on non-cardiac causes,4 it is of great importance to pay attention to SIFs during TAVI work-up to optimize patient preparation and selection for the best long-term benefit of TAVI. Although studies have reported the incidence of SIFs in their cohorts, a complete overview of current studies reporting SIFs and their follow-up is lacking. The objective of the current study was to systematically assess the current literature for the occurrence of SIFs during TAVI work-up and to evaluate whether SIFs are associated with higher mortality and delayed planning or procedure cancellation.
Methods
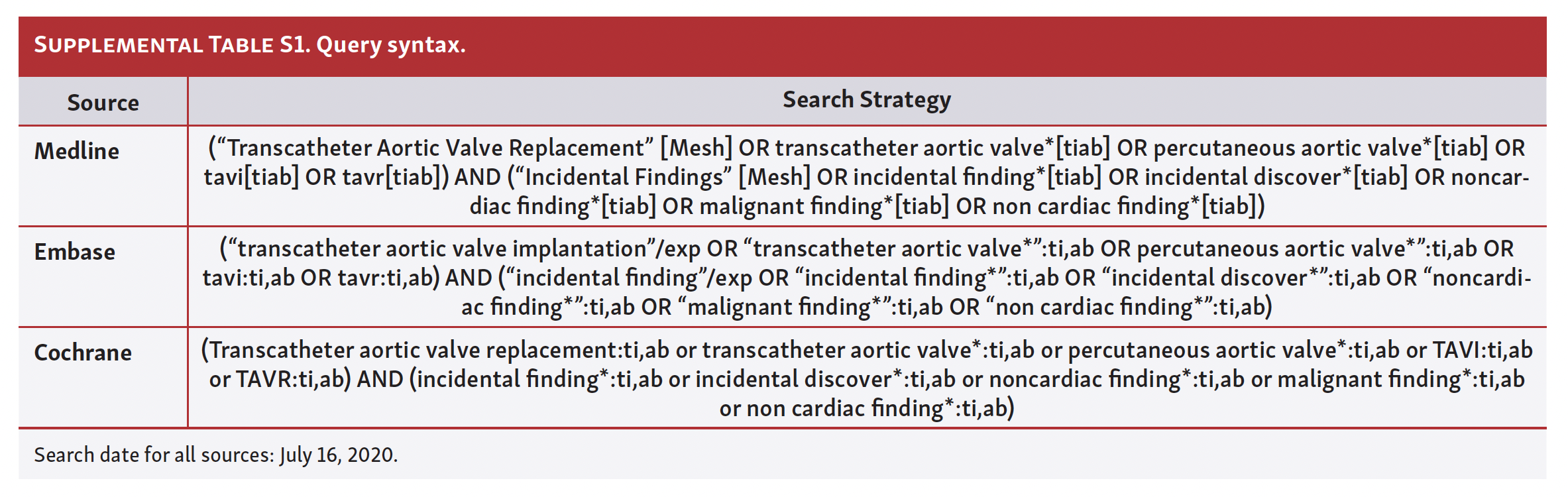
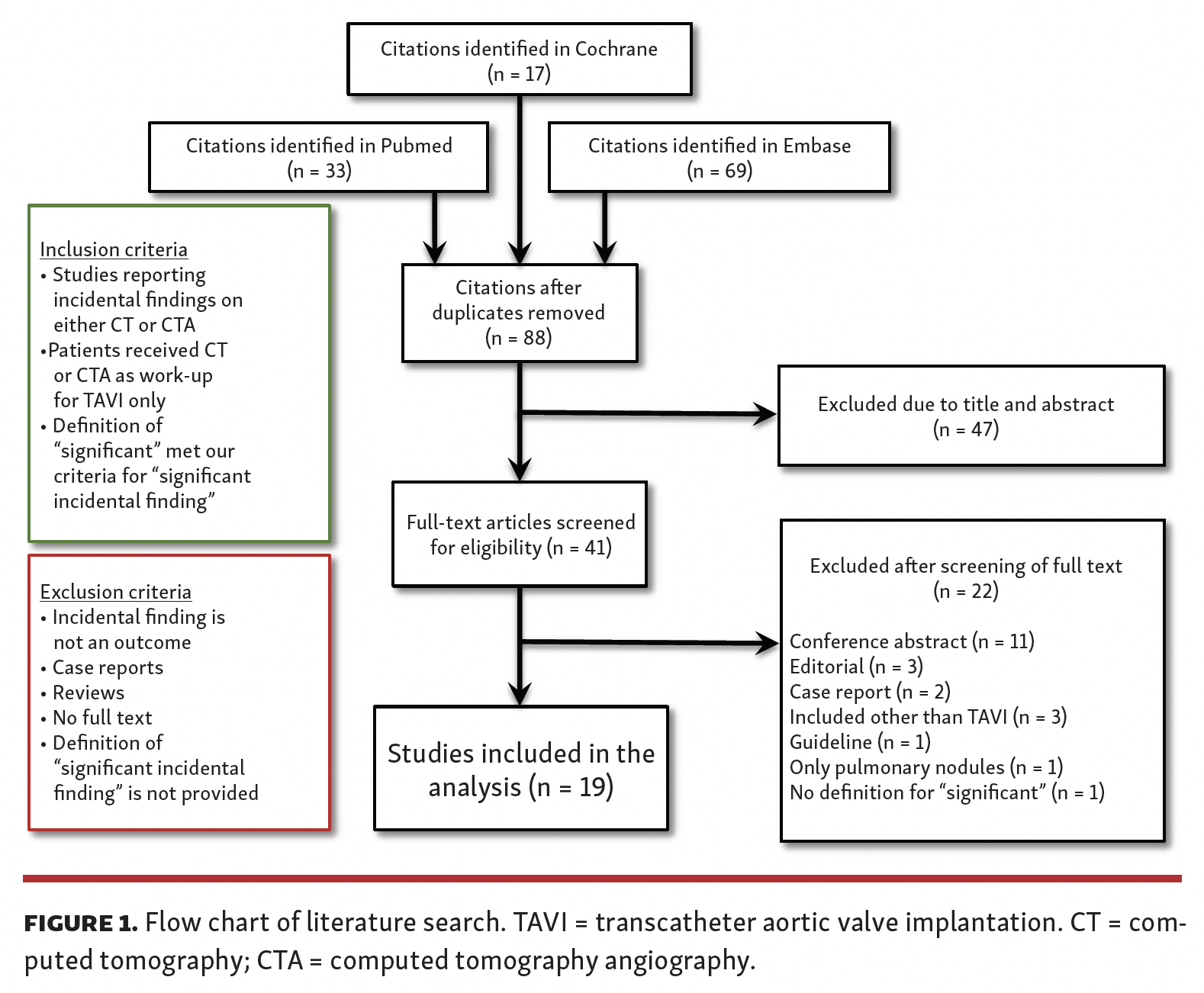
Literature search. A systematic search was performed on Medline, Embase, and Cochrane with synonyms for TAVI and incidental findings on July 16, 2020 without any language restrictions. The query syntax for each source is provided in Supplemental Table S1). A flow chart of the literature search and inclusion and exclusion criteria is shown in Figure 1. Titles and abstracts were assessed for eligibility by 2 researchers independently (KK and PPZ). A total of 19 retrospective cohort studies were selected for further analysis.5-23 A cross-reference check of all included studies did not lead to any additional relevant studies. There was no manual search performed for conference abstracts. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist24 was used as the framework for this study.
Definitions and data extraction. Significant incidental findings (SIFs) were defined as an incidental finding that was potentially pathological and required further diagnostics or treatment prior to the TAVI procedure that potentially influences the planning or indication for TAVI (eg, pulmonary nodules requiring CT scan follow-up or lymphadenopathy requiring biopsy). Malignant incidental findings (MIFs) were confirmed malignancies by histological biopsy and/or further imaging. Two researchers (KK and PPZ) independently screened included studies and extracted the variables of interest; sample size, age, sex, SIF rate, MIF rate, influence on mortality, and influence on TAVI planning, and stratified all SIFs per organ system. Data were filed in a standardized form.
Statistical analysis. All data were collected in Excel 2016 (Microsoft). Meta-analysis for pooling prevalence of SIF and MIF (depicted as percentages) was performed in R statistical software, version 3.1.2, and the additional metafor package. A random-effects model was used. Weighting was based on study size, with the weighing estimate being the inverse √n. Forest plots were generated for visualization. If necessary, a sensitivity analysis was performed to examine whether important differences between studies had an influence on the outcome of interest.
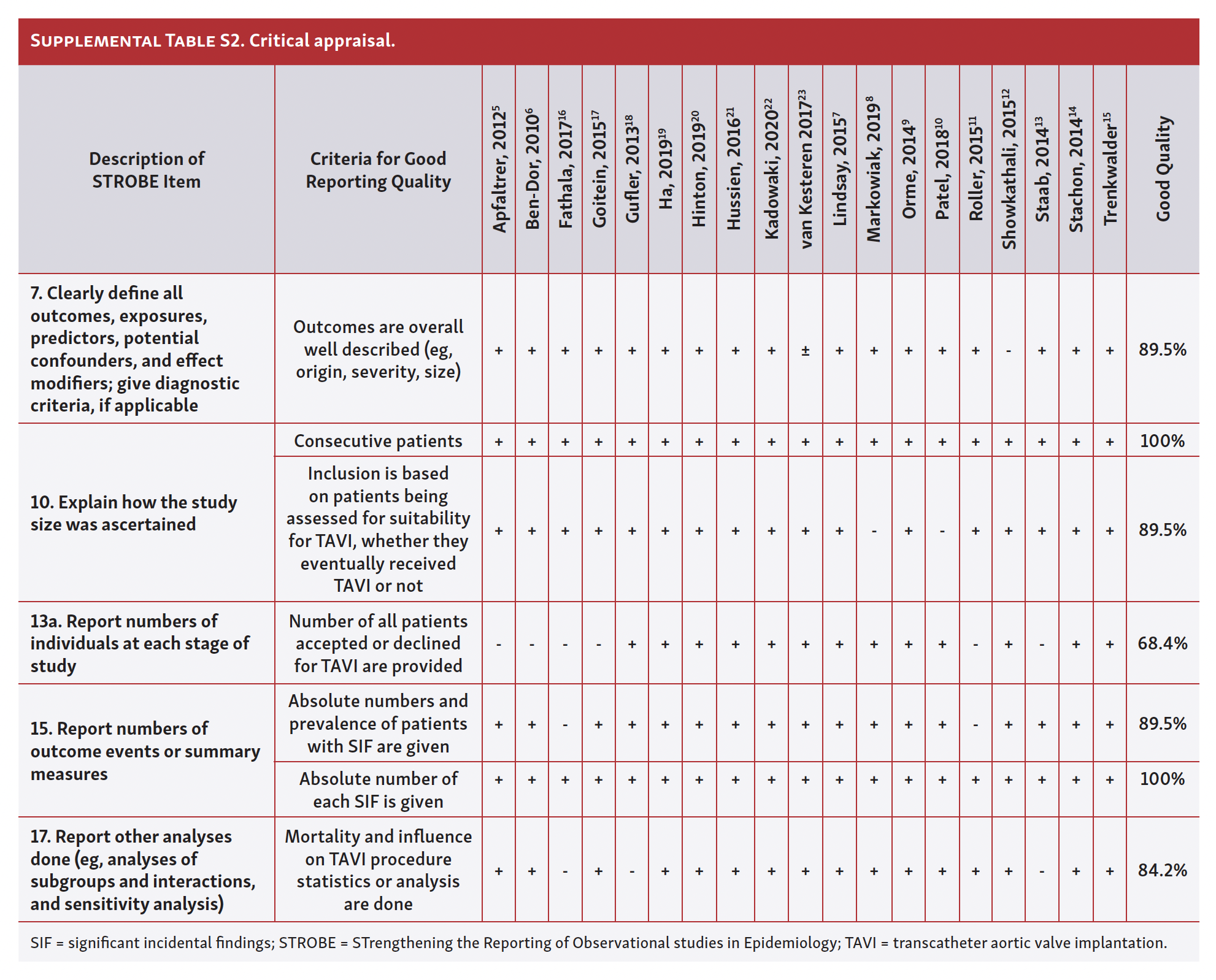
Critical appraisal of reporting quality. To assess the quality of included studies and their reporting, a modified checklist was derived from the STROBE (STrengthening the Reporting of Observational studies in Epidemiology) checklist.25 Applicable items for quality assessment were included, and STROBE items that were non-relevant to this study were excluded.
Criteria for high quality were defined for all items included in the modified checklist (Supplemental Table S2). Two researchers (KK and PPZ) independently assessed each study quality by using this tool.
Results
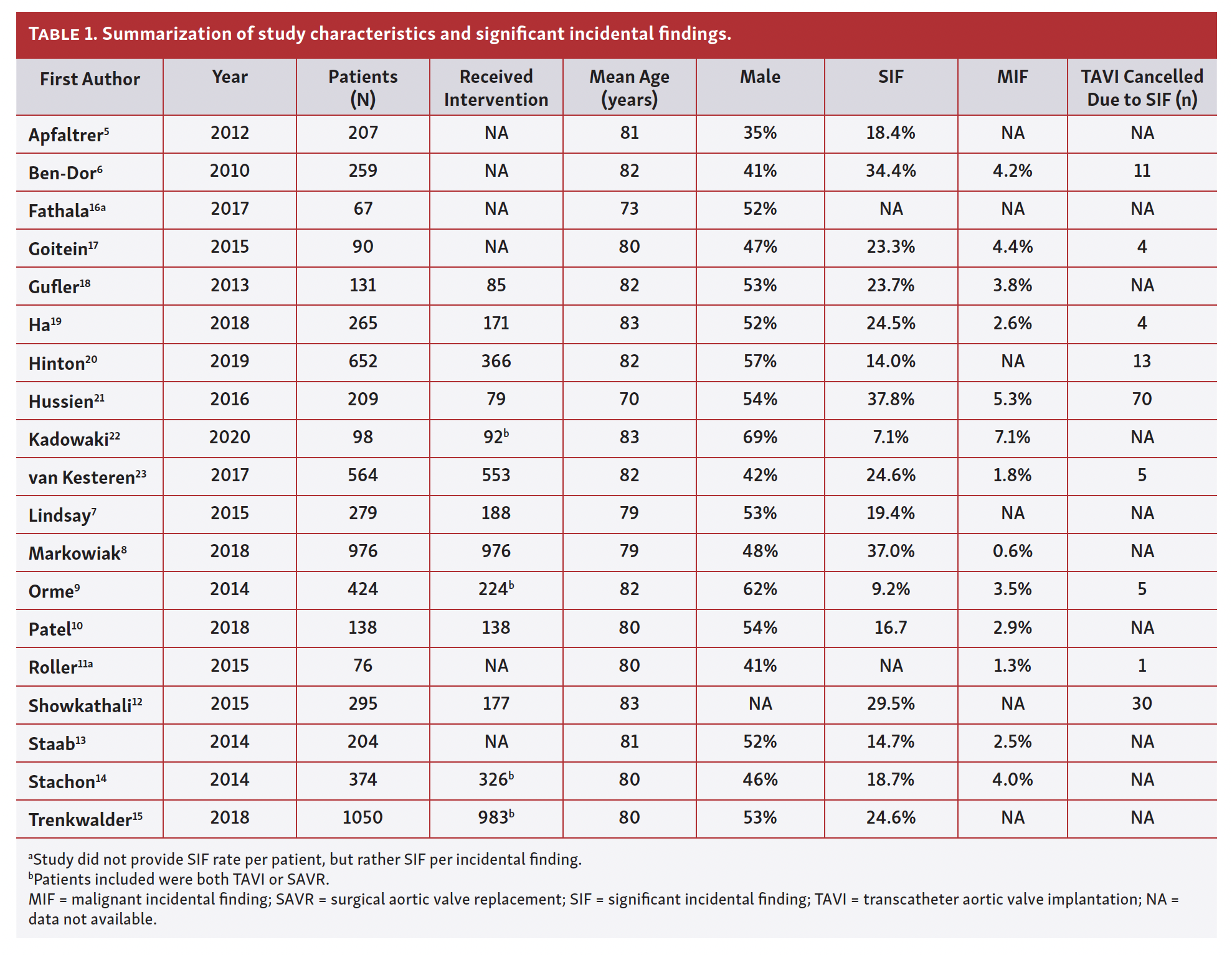
Baseline characteristics. The characteristics of the included studies are summarized in Table 1. A total of 6358 patients were included for analysis (mean patient age, 80 years; 51% male). All included studies performed a CT scan prior to TAVI. Most studies (17/19) included patients who received a CT scan to assess potential suitability for TAVI (regardless of actually undergoing the TAVI procedure), while 2 studies only included patients who already underwent TAVI.8,10 In 4 studies, all patients who proceeded to a treatment underwent TAVI (predominantly) or surgical aortic valve replacement.9,14,15,22
Critical appraisal of reporting quality. The general reporting quality of the available evidence was good (Supplemental Table S2). Roller et al reported SIFs, but this information was not the focus of the study,11 while van Kesteren et al reported the organ of SIF origin rather than the specific SIF (eg, lung instead of pulmonary nodule).23 Only 13/19 studies reported the number of all patients accepted or declined for an intervention, which were the studies included for assessment of influence on TAVI procedure.
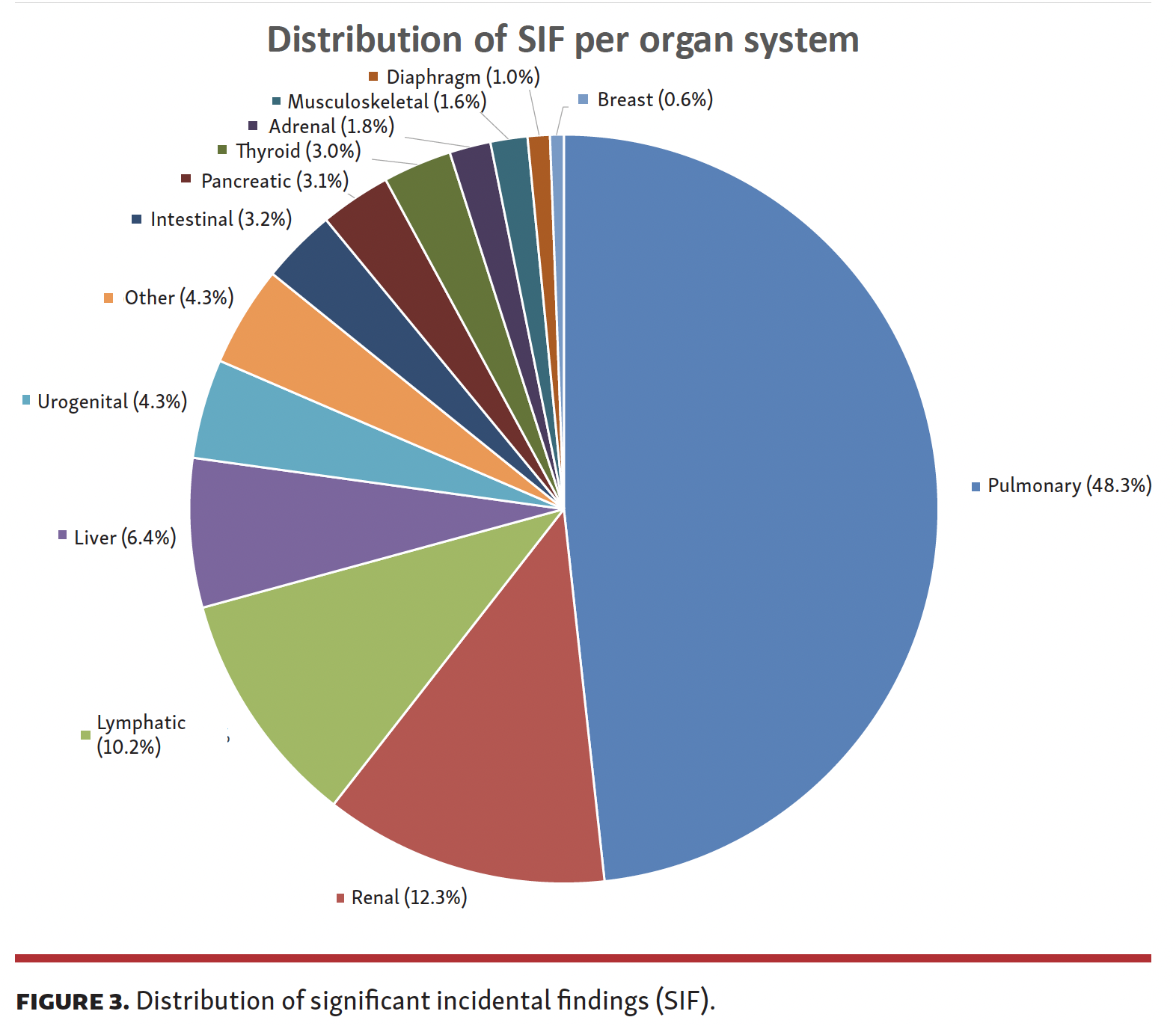
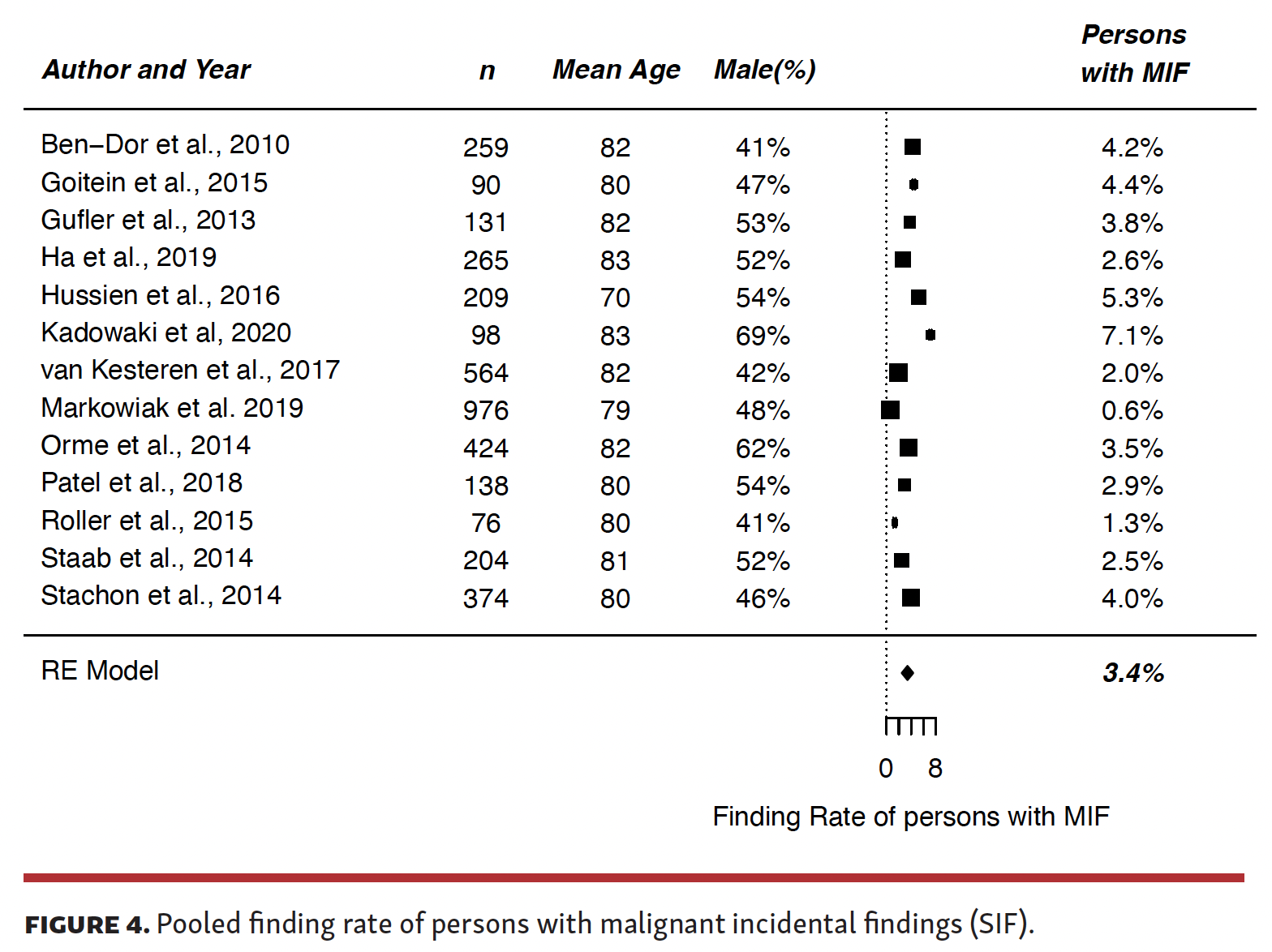
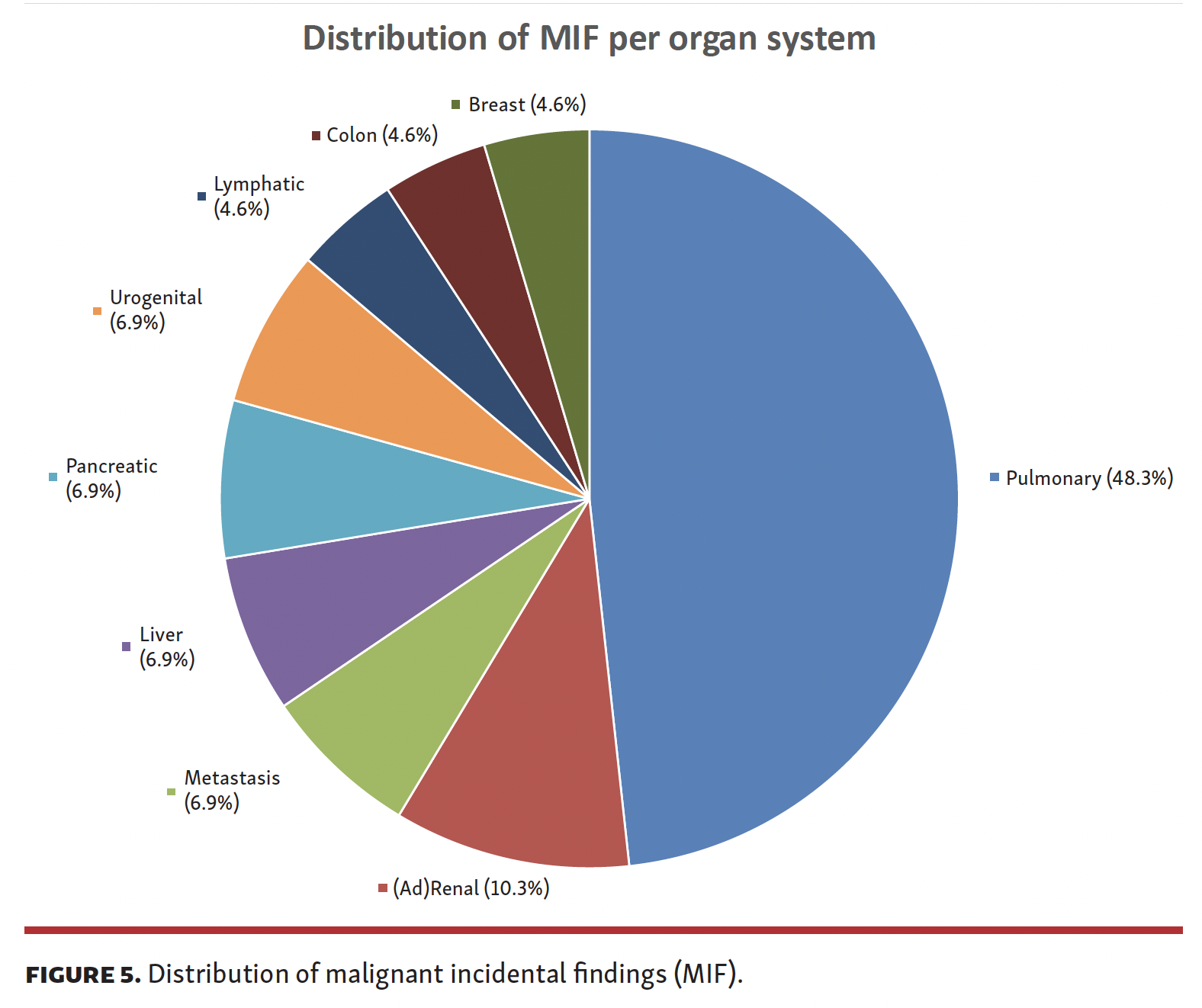
Primary outcome: SIF and MIF rates. Frequency of patients with SIF ranged from 9.2% to 37.8%. Pooled frequency of patients with a SIF was 22.2% (95% confidence interval [CI], 17.8-26.6) (Figure 2). There was an important difference in study population of the included studies, since there were 2 studies that included patients who already underwent TAVI.8,10 Therefore, a sensitivity analysis was performed and showed no significant difference (pooled frequency, 21.6%; 95% CI, 17.7-25.5). The distribution of SIF per organ system is shown in Figure 3. Most SIFs (48.3%) had a pulmonary origin and 52.9% of these (560/1058) were pulmonary nodules, accounting for 25.5% (560/2192) of all SIFs. Most of these nodules were benign and did not influence the TAVI procedure or prognosis. Frequency of MIF ranged from 0.6% to 7.1%. The pooled frequency of patients with MIF was 3.4% (Figure 4). Distribution of MIF per organ system is shown in Figure 5.

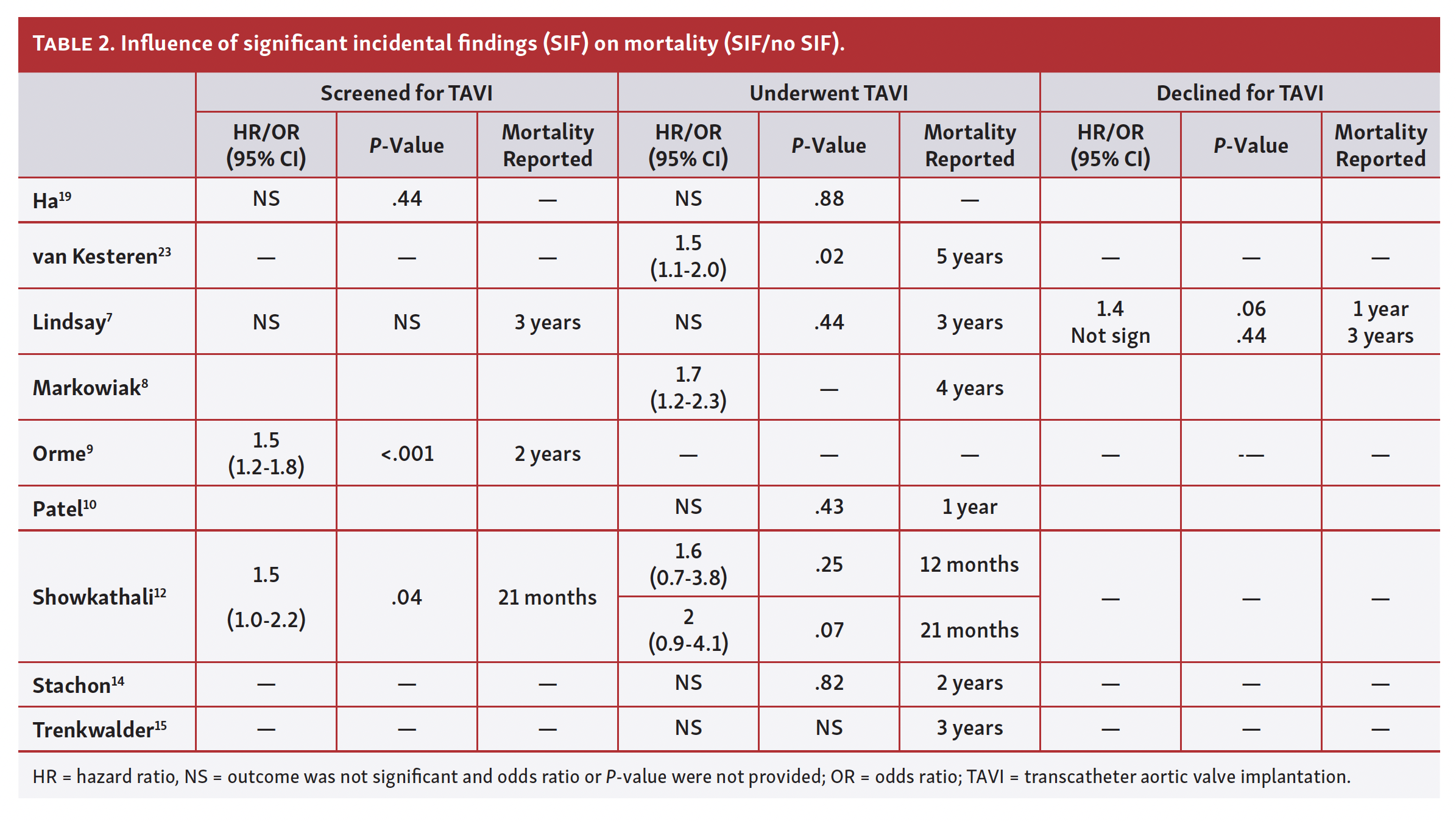
Secondary outcome: influence of SIF on mortality. Nine studies provided follow-up data for mortality analysis; the results are summarized in Table 2.7-10,12,14,15,19,23 There were 3 categories, ie, mortality of patients screened for TAVI, those who underwent TAVI, and those declined for TAVI. Two of 4 studies found SIF to be a risk factor for mortality in patients screened for TAVI.9,12 Lindsay et al showed an increased mortality risk in univariable analysis (hazard ratio, 1.6; 95% CI, 1.1-2.4; P=.02), but this was no longer an independent predictor for mortality in the multivariable analysis.7 Two of 8 studies found SIF as a risk factor for mortality in patients who underwent TAVI.8,23 Higher mortality in patients with SIF was only found if the follow-up period was more than 4 years. In patients who were declined for TAVI, only 1 study provided survival data and showed no difference in mortality for SIF.7
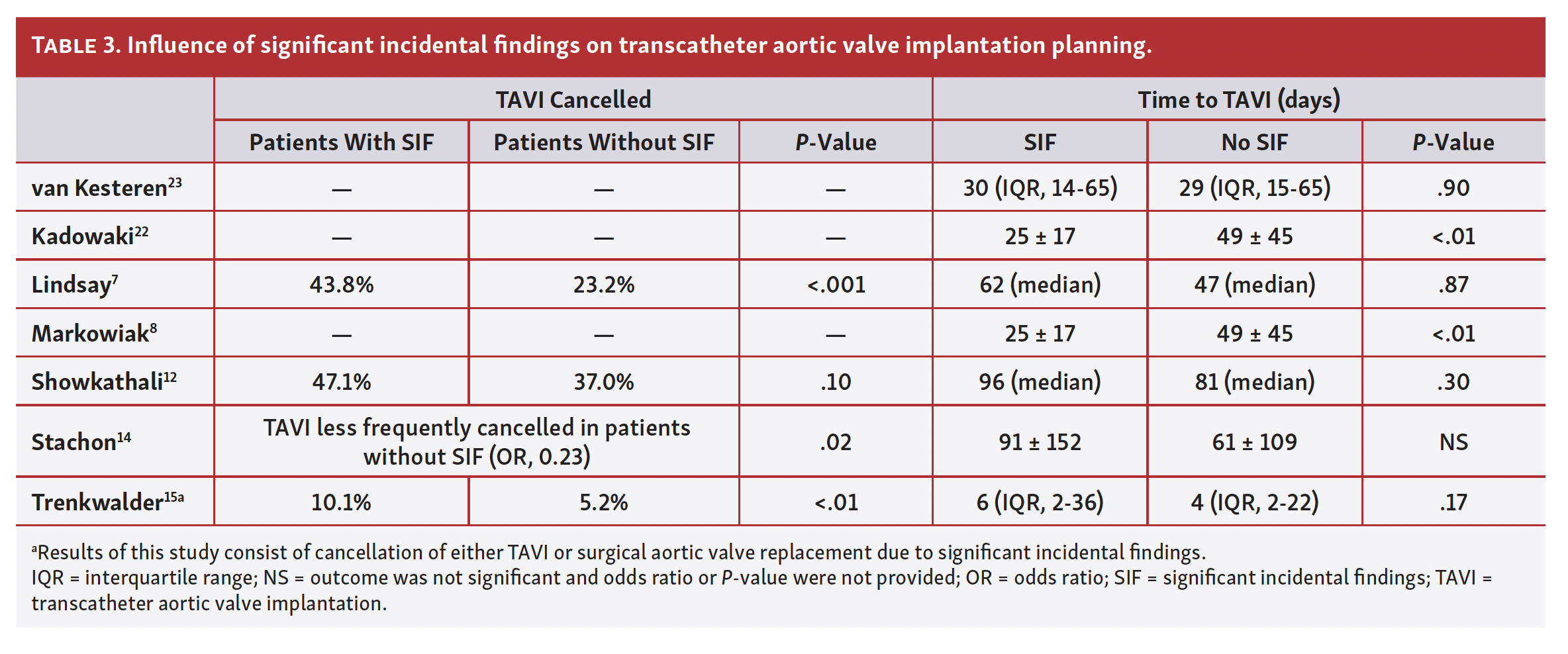
Secondary outcome: influence of SIF on TAVI planning. Four studies performed statistical analysis to determine whether SIF was associated with TAVI cancellation (Table 3).7,12,14,15 One study provided noncomparable results, but raw data were extracted in order to perform univariate analysis to provide comparable results to other studies.7 Three of 4 studies showed more TAVI cancellations in patients with SIF.7,14,15 Nine studies reported whether cancellation of TAVI was due to a SIF;6,9,11,12,17-21,23 of the total 2834 patients studied, 143 TAVI procedures were cancelled due to a SIF (5.0%). Seven studies reported a median or average time to TAVI, with 6 showing no difference in time to TAVI in patients with SIF7,8,12,14,15,23 and 1 demonstrating shorter time to TAVI in patients with SIF.22
Discussion
SIFs are common in the TAVI population, with a summarized frequency of 22.2% and a summarized frequency of 3.4% for new malignancies or relapse/progression of a known malignancy. These SIFs show no association with mortality in the short term (up to 3 years), but are associated with increased mortality when evaluated at ≥4 years. Time to TAVI was not prolonged in patients with SIFs. Since SIFs are frequently encountered, current guidelines recommend the screening for incidental findings on CT scans prior to TAVI.1,2
MIFs are commonly encountered and influence the 1-year life expectancy; therefore, they should be taken into consideration during heart team meetings. A delay of 2 to 4 weeks (to investigate any SIF or MIF) keeps patients longer in their current physical situation, which can be suboptimal if the aortic stenosis is severely symptomatic, albeit critical as the incidental finding might influence patient prognosis significantly. Interestingly, MIFs are reported at 0.7% in general populations who received a cardiac CT (for any reason),26 which is relatively low compared with the MIF rate in this study. This could be explained by the younger population (average age was about 60 years) and the restriction of imaging to the chest and upper abdomen in other studies, whereas CTA for a TAVI requires imaging from the thorax to the groin.
Consequences of SIFs depend on origin, severity, and follow-up setting. Some SIFs, like small masses or clearly benign findings, require long-term follow-up to monitor potential progression to malignant disease, according to current guidelines.27 Cardiologists should be aware of the likelihood of pulmonary nodules, with a reasonable chance of them being malignant, leading to poor prognosis and potential cancellation of TAVI. However, aggressive follow-up of these nodules (and the coinciding delay of any TAVI treatment planning) as stated in the current guidelines might be suboptimal, as a likely benign pulmonary finding will not influence prognosis as much as a severe aortic valve stenosis. Schmidt et al reported a risk of 2.3% for incidentally found pulmonary nodules (during TAVI screening and size >5 mm) turning into lung cancer at 15-month follow-up, which interestingly was not related to mortality in their multivariable analysis.28 Data from the NELSON trial showed no increased 2-year malignancy risk in patients with nodules <5 mm vs those without any pulmonary nodules. The same study also showed 2-year malignancy risk of 1.3% in 5-10 mm nodules and 15.2% in >10 mm nodules.29 Since there is no increased malignancy risk in small nodules, there is no need to delay TAVI in these patients. Larger nodules with mediastinal lymphadenopathy are more complicated. Although Schmidt et al did not find larger nodules (>8 mm) and lymphadenopathy as an independent predictor for mortality, there is not much literature available regarding these findings for patients screened for TAVI. Pulmonologists and radiologists should therefore be consulted in TAVI decision making whenever larger nodules (with or without lymphadenopathy) are found.28 Since it is of great importance to know the prognosis of these findings, prospective databases with well-defined definitions of SIF could further improve the process of patient selection.
Our meta-analysis confirms that SIF in patients screened for TAVI implies higher mortality. The heart team should therefore include these SIFs in their decision making. In patients who underwent TAVI, SIFs currently only seem to predict survival when follow-up was >4 years;8,23 the studies with shorter follow-up showed no significant association with SIFs in terms of mortality.7,12,14,15,19 These results reflect good decision making by the heart team in SIF patients selected for TAVI treatment. Regardless of whether SIFs predict long-term survival, patients who undergo TAVI have better quality of life, and a TAVI treatment might also benefit future interventions for SIF. Furthermore, since survival after TAVI is rather dependent on non-cardiac comorbidities,4 cardiologists should direct their attention to SIFs after valve implantation and refer these patients to other physicians for follow-up or treatment. One study reported a total of 5 SIF-related TAVI cancellations due to lack of life expectancy exceeding 1 year. All 5 patients (4 malignancies and 1 case of heart failure) died within 1 year of follow-up.23
Just as there is increasing awareness of the importance of incidental findings in the setting of a clinical trial,30 cardiologists should not only concentrate on the treatment of aortic valve stenosis but also be aware of the incidence and clinical implication of SIFs in the TAVI work-up. A decision algorithm for patient management in the presence of potentially malignant findings is provided by Pibarot.31 The key of this algorithm is a step-by-step approach based on the severity of the potential MIF and patient expected life expectancy. In general, we treat aortic valve stenosis in patients with confirmed malignancy if life expectancy exceeds 1 year. In line with this recommendation, there are case reports showing good results of lung cancer treatments after TAVI.32-34 In addition, the OCEAN-TAVI data showed no difference in mid-term (24-month) survival in patients with vs without active cancer35 and TOP-AS data showed equal survival in TAVI patients with stage I/II cancer vs no cancer, but reduced survival in TAVI patients with stage III/IV cancer vs no cancer.36 TAVI in patients with active cancer needs delicate risk-benefit analyses in which decision making is multidisciplinary and tailored to specific patient characteristics.
Study limitations. Judgment about the relevancy of an incidental finding is dependent on local hospital policy and the extensiveness of CT protocol and report. Most studies included in the current meta-analysis were published before the existence of guideline recommendations to systematically review incidental findings in the TAVI population. Reporting bias and heterogeneity are therefore expected to be high in our study, as can also be seen by the range of MIFs and SIFs reported in our studies. Nevertheless, the combined average gives us the best sense of the percentages we are dealing with as treating clinicians, which are important numbers in decision making.
Conclusion
SIFs are found in 22.2% and MIFs in 3.4% of patients screened for TAVI. The most common SIFs are pulmonary nodules. Cancellation due to SIF was necessary in 5.0% of patients. SIFs seem predictive for long-term mortality in the TAVI population and are therefore an important issue in patient selection. A holistic and multidisciplinary approach is recommended whenever TAVI treatment is considered. The results of this systematic review and meta-analysis enable cardiologists to inform potential TAVI patients about the risks of finding any significant health problems other than aortic valve stenosis, which can influence both short- and long-term outcome and/or postpone the TAVI procedure.
Affiliations and Disclosures
From the 1Department of Cardiology, University Medical Centre Utrecht, Utrecht, the Netherlands; and 2Department of Radiology, University Medical Centre Utrecht, Utrecht, the Netherlands.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript accepted May 18, 2021.
Address for correspondence: Adriaan Kraaijeveld, MD, PhD, Department of Cardiology, University Medical Centre Utrecht, Heidelberglaan 100, 3584 CX Utrecht, The Netherlands. Email: A.O.Kraaijeveld-3@umcutrecht.nl
Related Articles
- Orbital Atherectomy of the Ilio-Femoral Arteries Facilitates Large-Bore Access prior to Transfemoral Transcatheter Aortic Valve Replacement
- Transcatheter Aortic Valve Replacement in Nonagenarians: A Systematic Review and Meta-Analysis
- CT-Angiography Fusion During Coronary Chronic Total Occlusion PCI
- Coronary Computed Tomography Angiography (CCTA) vs Functional Imaging in the Evaluation of Stable Ischemic Heart Disease
- Safety, Efficacy, and Cost-Effectiveness of Same-Day Discharge for Left Atrial Appendage Occlusion
References
1. Francone M, Budde RPJ, Bremerich J, et al. CT and MR imaging prior to transcatheter aortic valve implantation: standardization of scanning protocols, measurements and reporting—a consensus document by the European Society of Cardiovascular Radiology (ESCR). Eur Radiol. 2020;30(5):2627-2650. Epub 2019 Sep 5. doi: 10.1007/s00330-019-06357-8
2. Blanke P, Weir-McCall JR, Achenbach S, et al. Computed tomography imaging in the context of transcatheter aortic valve implantation (TAVI)/transcatheter aortic valve replacement (TAVR): an expert consensus document of the Society of Cardiovascular Computed Tomography. JACC Cardiovasc Imaging. 2019;12(1):1-24. doi: 10.1016/j.jcmg.2018.12.003
3. Baumgartner H, Falk V, Bax JJ, et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739-2786. doi: 10.1093/eurheartj/ehx391
4. Rodés-Cabau J, Webb JG, Cheung A, et al. Long-term outcomes after transcatheter aortic valve implantation: Insights on prognostic factors and valve durability from the Canadian Multicenter Experience. J Am Coll Cardiol. 2012;60(19):1864-1875. doi: 10.1016/j.jacc.2012.08.960
5. Apfaltrer P, Schymik G, Reimer P, et al. Aortoiliac CT angiography for planning transcutaneous aortic valve implantation: aortic root anatomy and frequency of clinically significant incidental findings. AJR Am J Roentgenol. 2012;198(4):939-945. doi: 10.2214/AJR.11.7231
6. Ben-Dor I, Waksman R, Hanna NN, et al. Utility of radiologic review for noncardiac findings on multislice computed tomography in patients with severe aortic stenosis evaluated for transcatheter aortic valve implantation. Am J Cardiol. 2010;105(10):1461-1464. Epub 2010 Apr 2. doi: 10.1016/j.amjcard.2009.12.071.
7. Lindsay AC, Sriharan M, Lazoura O, et al. Clinical and economic consequences of non-cardiac incidental findings detected on cardiovascular computed tomography performed prior to transcatheter aortic valve implantation (TAVI). Int J Cardiovasc Imaging. 2015;31(7):1435-1446. Epub 2015 Jun 12. doi: 10.1007/s10554-015-0685-z
8. Markowiak T, Holzamer A, Hilker M, et al. Incidental thoracic findings in computed tomography scans before transcatheter aortic valve implantation. Interact Cardiovasc Thorac Surg. 2019;28(4):559-565. doi: 10.1093/icvts/ivy299
9. Orme NM, Wright TC, Harmon GE, et al. Imaging Pandora’s box: incidental findings in elderly patients evaluated for transcatheter aortic valve replacement. Mayo Clin Proc. 2014;89(6):747-753. doi: 10.1016/j.mayocp.2014.03.011
10. Patel A, Mahendran K, Collins M, et al. Incidental abnormal CT scan findings during transcatheter aortic valve implantation assessment: Incidence and implications. Open Hear. 2018;5(2):e000855. eCollection 2018. doi: 10.1136/openhrt-2018-000855
11. Roller FC, Schuhbaeck A, Achenbach S, et al. CT before transcatheter aortic valve replacement: value of venous phase imaging for detection and interpretation of findings with impact on the TAVR procedure. J Cardiovasc Comput Tomogr. 2015;9(5):422-427. Epub 2015 Apr 1. doi: 10.1016/j.jcct.2015.03.007
12. Showkathali R, Sen A, Brickham B, et al. “Incidental findings” during TAVI work-up: more than just an inconvenience. EuroIntervention. 2015;11(4):465-469. doi: 10.4244/EIJY14M06_04
13. Staab W, Bergau L, Lotz J, et al. Prevalence of noncardiac findings in computed tomography angiography before transcatheter aortic valve replacement. J Cardiovasc Comput Tomogr. 2014;8(3):222-229. doi: 10.1016/j.jcct.2014.03.004
14. Stachon P, Kaier K, Milde S, et al. Two-year survival of patients screened for transcatheter aortic valve replacement with potentially malignant incidental findings in initial body computed tomography. Eur Heart J Cardiovasc Imaging. 2015;16(7):731-737. Epub 2015 Mar 10. doi: 10.1093/ehjci/jev055
15. Trenkwalder T, Lahmann AL, Nowicka M, et al. Incidental findings in multislice computed tomography prior to transcatheter aortic valve implantation: frequency, clinical relevance and outcome. Int J Cardiovasc Imaging. 2018;34(6):985-992. Epub 2018 Feb 21. doi: 10.1007/s10554-018-1305-5
16. Fathala A, Bin Saeedan M, Zulfiqar A, et al. Non-cardiovascular computed tomography incidental findings in patients who underwent transaortic valve implantation procedure. Cardiol Res. 2017;8(1):13-19. Epub 2017 Mar 3. doi: 10.14740/cr445w
17. Goitein O, Di Segni E, Eshet Y, et al. Non-valvular findings before frans-catheter aortic valve implantation and their impact on the procedure. Isr Med Assoc J. 2015 Dec;17(12):764-767.
18. Gufler H, Schulze CG, Wagner S. Incidental findings in computed tomographic angiography for planning percutaneous aortic valve replacement: advanced age, increased cancer prevalence? Acta Radiol. 2014;55(4):420-426. Epub 2013 Aug 21. doi: 10.1177/0284185113500164
19. Ha FJ, Tham JLM, Paleri S, et al. Outcomes of incidental findings on multi-detector computed tomography for transcatheter aortic valve implantation assessment: a single-centre study and review of the literature. J Med Imaging Radiat Oncol. 2019;63(4):446-453. Epub 2019 Mar 15. doi: 10.1111/1754-9485.12872
20. Hinton J, Gough S, Ahmed H, et al. Frequency and impact of incidental findings on computed tomography during work-up for transcatheter aortic valve implantation: Single centre experience and review of the literature. Br J Radiol. 2019;92(1102):20190344. Epub 2019 Aug 12. doi: 10.1259/bjr.20190344
21. Hussien AF, Jeudy J, Kligerman SJ, et al. Thoracic incidental findings in preoperative computed tomography evaluation for transcatheter aortic valve implantation (TAVI). J Thorac Imaging. 2016;31(3):183-188. doi: 10.1097/RTI.0000000000000208
22. Kadowaki H, Yahagi K, Horiuchi Y, et al. Malignant findings in candidates for transcatheter aortic valve implantation. Heart Surg Forum. 2020;23(2):E250-E254. doi: 10.1532/hsf.2699
23. Van Kesteren F, Wiegerinck EMA, Mourik MS Van, et al. Impact of potentially malignant incidental findings by computed tomographic angiography on long-term survival after transcatheter aortic valve implantation. Am J Cardiol. 2017;120(6):994-1001. Epub 2017 Jun 29. doi: 10.1016/j.amjcard.2017.06.032
24. Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339(b2535). doi: 10.1136/bmj.b2535
25. White RG, Hakim AJ, Salganik MJ, et al. Strengthening the reporting of observational studies in epidemiology for respondent-driven sampling studies : “STROBE-RDS” statement. J Clin Epidemiol. 2015;68(12):1463-1471. Epub 2015 May 1. doi: 10.1016/j.jclinepi.2015.04.002
26. Flor N, Di Leo G, Squarza SAC, et al. Malignant incidental extracardiac findings on cardiac CT: systematic review and meta-analysis. AJR Am J Roentgenol. 2013;201(3):555-564. doi: 10.2214/AJR.12.10306
27. MacMahon H, Naidich DP, Goo JM, et al. Guidelines for management of incidental pulmonary nodules detected on CT images: from the Fleischner Society 2017. Radiology. 2017;284(1):228-243. Epub 2017 Feb 23. doi: 10.1148/radiol.2017161659
28. Schmidt LH, Vietmeier B, Kaleschke G, et al. Thoracic malignancies and pulmonary nodules in patients under evaluation for transcatheter aortic valve implantation (TAVI): Incidence, follow up and possible impact on treatment decision. PLoS One. 2016;11(5):1-14. eCollection 2016. doi: 10.1371/journal.pone.0155398
29. Horeweg N, van Rosmalen J, Heuvelmans MA, et al. Lung cancer probability in patients with CT-detected pulmonary nodules: a prespecified analysis of data from the NELSON trial of low-dose CT screening. Lancet Oncol. 2014;15(12):1332-1341. Epub 2014 Oct 1. doi: 10.1016/S1470-2045(14)70389-4
30. Oren O, Blankstein R, Bhatt DL. Incidental imaging findings in clinical trials. JAMA. 2020;323(7):603-604. doi: 10.1001/jama.2019.21813
31. Pibarot P. Incidental findings in patients screened for transcatheter aortic valve replacement: crystal ball or Pandora’s box? Eur Heart J Cardiovasc Imaging. 2015;16:721-722. Epub 2015 May 14. doi: 10.1093/ehjci/jev112
32. Drevet G, Maury J, Farhat F, et al. Transcatheter aortic valve implantation : a safe and efficient procedure to treat an aortic valve stenosis before lung cancer resection. Gen Thorac Cardiovasc Surg. 2019;67(3):321-323. Epub 2018 Feb 28. doi: 10.1007/s11748-018-0901-6
33. Komatsu H, Izumi N, Tsukioka T, et al. Pulmonary resection for lung cancer following transcatheter aortic valve implantation for severe aortic valve stenosis : a case report. Ann Thorac Cardiovasc Surg. 2018;26:1-4. Epub 2018 Apr 26. doi: 10.5761/atcs.cr.18-00028
34. Sakai T, Yahagi K, Miura S, et al. Transcatheter aortic valve implantation for patients with lung cancer and aortic valve stenosis. J Thorac Dis. 2018;10(5):E387-E390. doi: 10.21037/jtd.2018.04.83
35. Watanabe Y, Kozuma K, Hioki H, et al. Comparison of results of transcatheter aortic valve implantation in patients with versus without active cancer. Am J Cardiol. 2016;118(4):572-577. Epub 2016 May 28. doi: 10.1016/j.amjcard.2016.05.052
36. Landes U, Iakobishvili Z, Vronsky D, et al. Transcatheter aortic valve replacement in oncology patients with severe aortic stenosis. JACC Cardiovasc Interv. 2019;12(1):78-86. doi: 10.1016/j.jcin.2018.10.026













