


Combined Rotational Excimer lASER Coronary Atherectomy (RASER) in Non-crossable, Non-dilatable Coronary Artery Disease: Observations From a Single Center
Abstract
Background. Balloon non-crossable stenoses represent a challenging subset of coronary artery disease (CAD). They are clinically associated with patients who are older, frailer, and with multimorbidity, and angiographically with increased tortuosity and coronary artery calcification. Combined rotational (RA) excimer laser coronary atherectomy (ELCA), or RASER, may facilitate stent delivery and deployment in non-crossable, non-dilatable, severely calcified lesions. In this study, we assessed preliminary safety and efficacy of the RASER hybrid technique.
Methods. RASER feasible percutaneous coronary intervention (PCI) procedures performed at a large tertiary hospital in the northeast of England were retrospectively analyzed from September 1, 2008 to February 28, 2022. Major endpoints were in-hospital death from any cause, as well as procedural and angiographic success, defined by stent delivery with less than 50% residual stenosis and without clinical or angiographic complications, respectively.
Results. From 74 unique cases, there were 28 RASER, 24 ELCA/RA, 16 balloon angioplasty with or without stenting, and 6 medically treated patients. In-hospital mortality rate was 5.2%, including 1 ELCA- and 3 RASER-treated patients. Successful stent delivery was achieved in significantly more RASER-treated patients compared to ELCA/RA- or balloon-treated patients: 96.4% (27/28), 25% (6/24), and 31.3% (5/16), respectively (P < .001).
Conclusions. In our retrospective, single center study, patients with CAD who were deemed appropriate for RASER PCI had a high peri-procedural mortality rate. In this context, adjunctive RASER therapy provides acceptable safety and efficacy as a bailout strategy, with at least 3 out of 5 patients achieving satisfactory procedural and angiographic results. Randomized controlled trials are needed to comprehensively compare the clinical outcomes of high-risk RASER PCI vs conservative medical therapy.
Introduction
Balloon non-crossable coronary artery stenoses are among the most difficult lesions to treat by percutaneous coronary intervention (PCI).1,2 Clinically, this pattern of coronary artery disease (CAD) is more frequently encountered in patients who are frail, older, with underlying comorbidities, who have left ventricular systolic dysfunction (LVSD), and who invariably are surgical turndowns.3-5 Angiographically, these lesions are long, tortuous, and heavily calcified. Severe coronary artery calcification leads to a lower likelihood of procedural success and a 3-fold higher risk of worse clinical outcomes following PCI.3-5 At a lesion level, calcification predisposes to vessel dissection and rupture, particularly at junctions of an arc of normal vessel and at the site of negative remodeling.3-6 In addition, there is a significant risk of stent under-expansion and compromised drug delivery to the vessel,3-6 and patients are more likely to experience major adverse cardiac events (MACE) due to stent thrombosis and in-stent restenosis.4
Treatment of non-crossable, non-dilatable, severely calcified lesions requires longer procedural times, increased volumes of contrast, higher radiation doses, and more complex plaque modification techniques. Examples include ultra-high pressure non-compliant balloons (OPN), cutting and scoring balloons (eg, Flextome [Boston Scientific Corp] and AngioSculpt [Philips]), and the more recent intravascular lithotripsy balloons (IVL).3,5 However, their bulkier delivery profile, especially in the setting of calcified, tortuous, and severely stenosed segments, often makes treatment of non-crossable, non-dilatable lesions nearly impossible.1,2
The combined use of 2 forms of athero-ablative technology, excimer laser coronary atherectomy (ELCA) and rotational atherectomy (RA), may circumvent this problem. ELCA delivers ultraviolet energy from a catheter with a short monorail mounted on a standard 0.014-inch guidewire to vaporize surrounding luminal calcium.7 In RA, a pneumatically powered burr is advanced over a specialized 0.009-inch guidewire to differentially drill superficially calcified, severely stenosed lesions.8 Importantly, both devices are available in very small diameter sizes, 0.9-mm catheter size and 1.25-mm burr size, respectively.3,7,8 In combined rotational excimer laser coronary atherectomy (RASER) therapy, ELCA creates an upstream pilot hole using a more deliverable coronary wire to facilitate the passage of the specialized RotaWire (Boston Scientific) for anticipated RA.
Of the 686 358 PCI procedures performed in the United Kingdom and comprehensively recorded in the British Society of Interventional Cardiology (BCIS) database from 2006 to 2016, only 153 (0.02%) involved RASER.9-14 In contrast, 1% of PCI in stable CAD involve non-crossable, non-dilatable coronary lesions.1,2 The utility of RASER therapy in this challenging subset of CAD may be underappreciated; therefore, collective knowledge of procedural and clinical outcomes is limited. The aim of this retrospective observational study is to share the experience of RASER therapy in non-crossable, non-dilatable, severely calcified CAD from a single center, addressing the feasibility, safety, and efficacy outcomes of RASER therapy.
Methods
Study population and design. We performed a retrospective analysis of prospectively collected data on all patients who were considered for RASER-assisted PCI between September 1, 2008 and February 28, 2022 at the Freeman Hospital, a tertiary cardiac center in the northeast of England. Eligible patients were admitted either with an acute coronary syndrome (ACS), or electively for percutaneous treatment of medication refractory stable angina, and were found to have non-crossable, non-dilatable, severely calcified coronary artery stenoses. Non-crossable, non-dilatable stenoses were defined as lesions that could not be crossed by semi-compliant balloons at least 2 mm in diameter, despite advancement of the guidewire distal to the lesion.1,2 Severe calcification was assessed fluoroscopically by the operator and was conventionally defined by radiopacities in the vascular wall on either side of the lesion noted without cardiac motion prior to contrast injection.15 The important exclusion criterion was repeat RASER-assisted PCI.
Patients treated by RASER-assisted PCI (RASER) were compared to (1) patients whose culprit coronary lesions were treated with either modality (ELCA or RA); (2) patients who were treated with low-profile 0.85- to 1.5-mm diameter semi-compliant balloons ± stenting; and (3) patients who were treated medically after failure to deliver standard semi-compliant balloons. Reports of locally performed procedures containing the key terms “RASER," "ELCA," “RA,” or a combination were sourced from the National Cardiac Audit Programme (NCAP) on Adult PCI hosted by the National Institute of Cardiovascular Outcomes Research (NICOR) and the British Cardiovascular Interventional Society (BCIS). Missing information was populated through review of the local electronic patient record system and the wider Great North Care Record, a platform that integrates primary and secondary care patient information.16
Relevant data were patient-specific variables including age, sex, cardiovascular risk factors, comorbidities, medications, and procedural details, including access route, use of intravascular imaging (either intravascular ultrasound [IVUS] or optical coherence tomography [OCT]), types of balloon treatment and advanced calcium modification techniques (eg, IVL) to prepare the lesion, number and length of drug-eluting stents (DES), and complications.
Procedure details. All patients were considered for bailout RASER therapy when the culprit coronary lesion could not be crossed with standard semi-compliant balloons after angiography and before stent deployment. Once the coronary lesion was crossed with an operator-selected coronary guidewire, the ELCA coronary laser atherectomy system (Philips) was used to deliver ultraviolet light therapy using an appropriately sized fiber-optic catheter (available in 0.9-, 1.4-, 1.7-, and 2.0-mm diameter) with fluence 30 to 80 mJ/mm2 and pulse frequency 25 to 80 Hz in 5- to 10-second cycle lengths.7 Thereafter, with the support of a microcatheter, a specialized RotaWire was passed through the new channel before the lesion was debulked with an RA burr size of 1.25 to 2.50 mm on the RotaPro system.8 Intravascular imaging, further lesion preparation, choice and number of stents, and post-stent optimization were at the discretion of the operator.
Outcomes. We examined the following endpoints:
- Procedural success, defined as stent delivery with angiographically-assessed residual stenosis of less than 50% and without clinical complications2,17-19
- Angiographic success, defined as stent delivery with less than 50% residual stenosis and without serious angiographic complications2,17-19
- Clinical and angiographic complication rates
- Death from any cause in-hospital, at 30 days and 1 year
Clinical complications included in-hospital death and periprocedural major and minor bleeding, acute pulmonary edema, cardiac tamponade, arrhythmias, and acute kidney injury (AKI). Bleeding events were classified according to the Thrombolysis in Myocardial Infarction (TIMI) criteria.20 Major bleeding was any intracranial bleeding, clinically overt signs of hemorrhage with a Hb drop of greater than or equal to 50 g/L, or fatal bleeding.20 Minor bleeding was clinically overt signs of hemorrhage with a Hb drop of 30 to 50 g/L, or any overt sign of hemorrhage that required intervention and/or prolonging of hospitalization.20 Periprocedural complications must have occurred within 48 hours of the PCI.
Angiographic complications included iatrogenic coronary dissections according to the National Heart, Lung and Blood Institute (NHLBI) classification system, coronary perforations by Ellis classification, abrupt vessel closure, persistent slow flow-no reflow, and stent/device loss that required further intervention.21,22
Statistical analysis. Numerical continuous and discrete variables were presented as mean ± standard deviation (SD) or median (minimum, maximum). Categorical variables were summarized as proportions. Analysis of variance (ANOVA) or the Kruskal-Wallis by ranks test for multiple group comparisons and the Pearson’s χ2 test compared patient and procedural characteristics and outcomes across the 4 groups: RASER, ELCA/RA, balloon pre-dilation ± stenting, and medical therapy. Statistical significance was assessed at the conventional 2-sided 5% level (P < .05). The analysis was performed using SPSS version 29.0 (IBM Corp).
Results
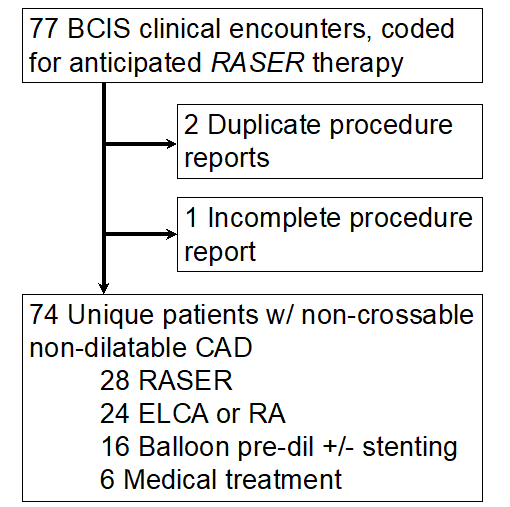
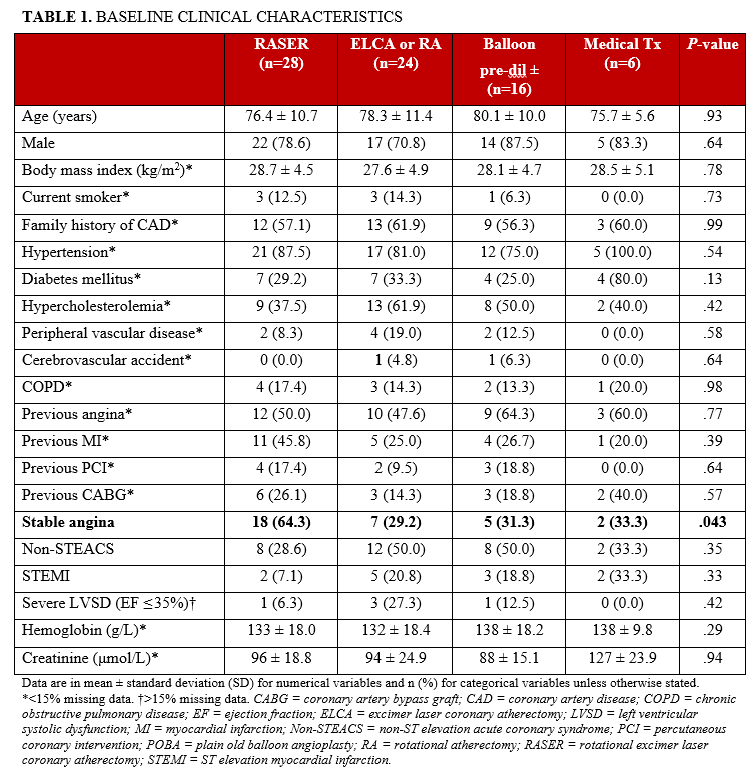
After exclusions, 74 unique patients for whom RASER-assisted PCI was considered were identified: 28 proceeded to RASER therapy, 24 to either ELCA or RA, 16 to balloon pre-dilation ± stenting, and 6 received medical therapy (Figure). The patients were 77.8 ± 10.4 years of age, and 58 (78.4%) were male. The prevalence of hypercholesterolemia, hypertension, and diabetes mellitus was 48.5%, 83.3%, and 33.3%, respectively. Patients frequently had a history of previous angina (53.1%), MI (32.8%), PCI (13.8%), and/or coronary artery bypass graft (CABG) (21.5%). Of the 74 patients, 42 (56.7%) were ACS presentations, including 12 (28.6%) with ST-elevation myocardial infarction (STEMI). More stable angina patients proceeded to RASER PCI compared with either ELCA/RA or balloon pre-dilation ± stenting (64.3% vs 29.2% and 31.3%). All patients were prescribed dual antiplatelet therapy (DAPT), a cholesterol-lowering agent, an inhibitor of the renin-angiotensin-aldosterone system, and a beta-blocker. Table 1 summarizes the baseline clinical characteristics.
Procedural details are listed in Table 2. One in 3 patients had femoral arterial access. Approximately 50% of culprit lesions were in the left anterior descending artery (LAD) and less than 10% involved the left main coronary artery (LMCA). The most frequently delivered ELCA catheter and RA burr sizes were 0.9 mm (90.2%) and 1.5 mm (53.1%), respectively. Intravascular imaging was only used after RASER therapy to assess lesion preparation and stent optimization in approximately one-fourth of the patient population.
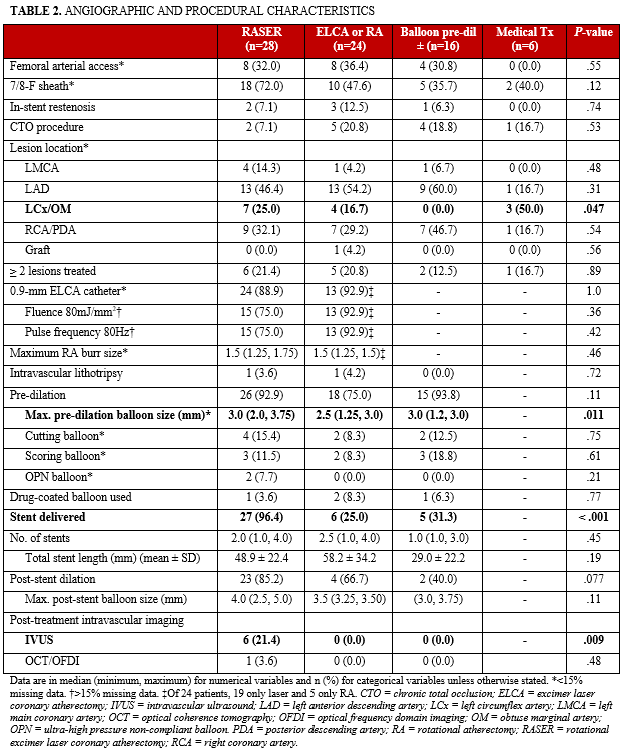
Target lesion pre-dilation was performed in 86.8% of PCI procedures. The median maximum balloon size was greater in RASER than in either ELCA/RA or balloon pre-dilation ± stenting groups (median [minimum, maximum] 3.0 [2.0, 3.75] mm vs 2.5 [1.25, 3.0] mm and 3.0 [1.2, 3.0] mm, respectively). RASER PCI facilitated the highest stent implantation rate (96.4% vs 25.0% and 31.3%), delivering an average of 2 stents per lesion. Post-stent balloon dilation was performed in 85.2% of RASER cases with median maximum balloon size of 4.0 mm vs 66.7% of ELCA/RA and 40.0% of balloon pre-dilation ± stenting cases with median maximum balloon size of 3.5 mm.
Safety and efficacy. Acute procedural success was obtained in 23 of 28 patients (82.1%) with RASER vs 5 of 24 patients (20.8%) with ELCA or RA and 1 of 16 patients (6.3%) with only balloon pre-dilation ± stenting (P < .001) (Table 3). There was no significant difference in clinical complication rates, including pulmonary edema, tamponade, arrhythmias, AKI, bleeding, and death from any cause. Angiographic success was achieved by 17 of 28 patients (60.7%) with RASER vs 3 of 24 patients (12.5%) with ELCA/RA and 0 of 16 patients (0.0%) with balloon pre-dilation ± stenting cases (P < .001) (Table 3). Overall, 20 of 68 (29.4%) procedures had a dissection, of which 50% required further intervention with stents. A further 3 of 68 (4.4%) had a conservatively managed coronary perforation, and 3 of 68 (4.4%) had slow flow-no reflow, managed with intracoronary vasodilators.
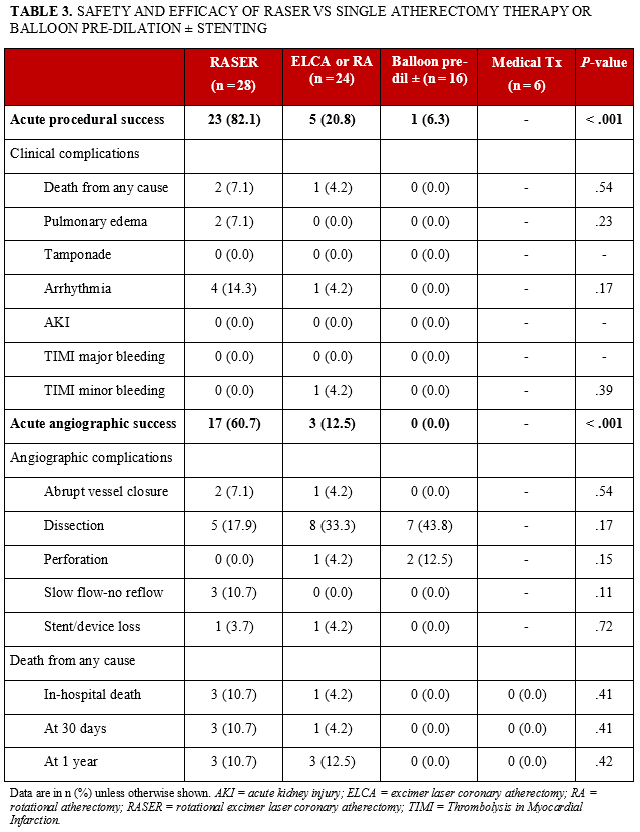
All-cause mortality. Of 74 patients with severely calcified, non-crossable, non-dilatable culprit coronary artery lesions, 4 (5.4%) died in-hospital, including 1 ELCA- and 3 RASER-treated patients. The overall mortality rate at 30 days and 1 year was 5.4% and 8.1%, respectively (Table 3). The 1 in-hospital death after ELCA-assisted PCI was a 100-year-old man who had severe LMCA-LAD disease involving in-stent restenosis with a sub-totally occluded obtuse marginal 1 (OM1) branch and right coronary artery (RCA). He was admitted with pulmonary edema, severe left ventricular systolic dysfunction, and global ischemia on electrocardiogram, and could not be resuscitated in the catheter lab. Two RASER-treated patients, admitted with non-STE myocardial infarction (NSTEMI), lost flow in their culprit LAD vessel during lesion preparation. Although stents were successfully delivered, pulmonary edema, ventricular arrhythmias, and death complicated their procedures. A 79-year-old elective patient had successful RASER PCI to a large OM1 branch in addition to PCI to his LAD and RCA but died 72 hours into his admission.
Discussion
Severely calcified, severely stenosed CAD remains a significant challenge in contemporary interventional cardiology.3 The diffuse pattern of disease is frequently encountered in patients who are frail, older, with comorbidities, and who are not candidates for first-line CABG revascularization.5,9,23 Combined RASER may have a niche role in treating non-crossable, non-dilatable, calcified coronary artery stenoses. The major findings from our single-center, retrospective, observational study of 28 patients with RASER PCI are as follows: (1) The in-hospital periprocedural mortality risk of these patients is high, with 1 in 10 not surviving to discharge; and (2) RASER-assisted PCI is a feasible rescue strategy in high-risk populations with balloon non-crossable, non-dilatable culprit coronary lesions, facilitating a stent delivery rate of greater than 95%.
Our early experience with adjunctive RASER therapy in complex PCI is consistent with the existing, albeit limited, published data. In a retrospective analysis of close to 700 000 PCI cases performed over a 10-year period in the UK, 153 (0.02%) used a RASER-based PCI strategy, often in older patients (73.4 vs 65.2 years of age) with a significantly higher burden of pre-existing ischemic heart disease, including previous MI (49.0% vs 27.6%), PCI (40.1% vs 23.7%), and CABG (37.7% vs 20.5%).9 Overall, this minority PCI was more complex, evidenced by greater use of intravascular imaging (29.5% vs 6.8%), cutting balloons (13.1% vs 3.2%), and ultimately more stents (2.5 vs 1.5 stents) of greater length (47.8 mm vs 25.6 mm).9 By comparison, studies of cutting/scoring balloons, intravascular lithotripsy, or stand-alone rotational/orbital atherectomy recruited patient cohorts who were at least 4 years younger and had at least 10 percentage points-fewer previous CABG, both of which are markers of less calcified, less complex CAD.17-19,24 Taken together, these observations underline that RASER-assisted PCI has often been reserved for the treatment of calcified, severely stenosed CAD in high-risk patients who were invariably surgical turndowns.
It is anticipated that RASER therapy will be used after first- and second-line calcium modification techniques have either failed or were not deliverable.3,5 In 10 case studies, ELCA was used to facilitate the delivery of a RotaWire for more comprehensive RA after the heavily calcified lesion was not crossable with a microcatheter.10-14 Similarly, we needed RASER therapy after provisional strategies of standard compliant, non-compliant, specialized cutting balloons and RA were either too bulky and/or did not adequately prepare the lesions prior to stent placement. Importantly, this hybrid technique facilitated a 3- to 4-fold higher stent delivery rate, as well as pre- and post-dilation with larger balloons.
We must caution that the significantly greater procedural and angiographic success rates of RASER therapy in comparison to either modality alone, balloon treatment, or medical therapy was driven by improved stent delivery, not reduced complication rates. RASER PCI had greater numbers of clinical complications, including arrhythmias, pulmonary edema, and death from any cause. We suspect that our study does not adequately describe the influence of various competing clinical factors on operator gestalt, favoring RASER and medical therapy in different patients presenting with non-crossable, non-dilatable culprit coronary artery stenoses. Factors likely included patient stability, contrast volume, procedural duration, and operator expertise, leading to significant selection and treatment bias. It is vital that long-term outcome data on MACE, including death from any cause, non-fatal MI, non-fatal stroke, and ischemia-driven repeat revascularization are compared between patients randomized to either RASER PCI or conservative medical management.
Nevertheless, in line with their clinical and angiographic risk profile, our total cohort had a high in-hospital mortality rate of 5.2% vs 1.7% in ROTAXUS (Rotational Atherectomy Prior to Taxus Stent Treatment for Complex Native Coronary Artery Disease), 0.2% in ORBIT II (Pivotal Trial to Evaluate the Safety and Efficacy of the Orbital Atherectomy System in Treating De Novo, Severely Calcified Coronary Lesions), and 0.3% in DISRUPT CAD III (Intravascular Lithotripsy for Treatment of Severely Calcified Coronary Artery Disease).17-19 Acknowledging variations in definition, our respective 80% and 60% RASER PCI procedural and angiographic success rates were also lower than the success rates in landmark RA, orbital atherectomy (OA), or IVL trials, which were all greater than 90%.17-19 We contend that our success rate with RASER-assisted PCI as a bailout revascularization strategy in higher risk patients is more than acceptable. It remains important that the optimal revascularization strategy is guided by the heart multidisciplinary team (MDT) and that the patient is appropriately consented for high-risk complex RASER PCI.5
Study limitations and strengths. Any conclusions are limited by a small sample size, long recruitment period, and the retrospective observational design of the study. We did not use IVUS- or OCT-based coronary calcification assessment as inclusion criteria, although failure to deliver low-profile balloons is indicative of significant coronary calcification. We did not include intravascular imaging-derived outcomes but contend that the results of greatest relevance are the clinical endpoints. The strength of our case series is derived from high-quality data sourcing using a nationally maintained database. Overall, our observations are hypothesis-generating and should provide useful information to other PCI operators when encountering CAD of similar complexity.
Conclusions
Severely calcified, severely stenosed CAD is an adverse prognostic marker associated with a high perioperative mortality risk due to both patient and procedural factors. Combined rotational excimer laser coronary atherectomy, or RASER, is a promising rescue strategy with high stent delivery rates in patients who are surgical turndowns and whose culprit coronary lesions are non-crossable and non-dilatable with conventional PCI techniques. Any decision should be guided by the heart MDT with patient involvement. Short- and long-term outcomes of RASER-assisted PCI need to be rigorously examined against conservative medical management in a randomized controlled trial setting. The hope is that by validating RASER as a bailout strategy in complex high-risk PCI, it may become the benchmark or standard of care in patients who would otherwise be managed medically.
Affiliations and Disclosures
From the 1James Cook University Hospital, Middlesbrough, United Kingdom; 2University of Birmingham, United Kingdom; 3University of Newcastle, United Kingdom; 4The Freeman Hospital, Newcastle Upon Tyne, United Kingdom; 5Queen Elizabeth Hospital, University Hospitals Birmingham, United Kingdom; 6Cardiovascular Research Foundation, New York, New York, USA.
Acknowledgments: The authors thank the staff at the Freeman Hospital for their high standard of care of the patients included in the study.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Kerrick Hesse, BMedSc, MBChB, MRCP, The James Cook University Hospital, Marton Road, Middlesbrough, TS4 3BW, UK. Email: Kerrick.hesse@nhs.net
References
1. McQuillan C, Jackson MWP, Brilakis ES, Egred M. Uncrossable and undilatable lesions-A practical approach to optimizing outcomes in PCI. Catheter Cardiovasc Interv. 2021;97(1):121-126. doi: 10.1002/ccd.29001
2. Karacsonyi J, Karmpaliotis D, Alaswad K, et al. Prevalence, indications and management of balloon uncrossable chronic total occlusions: Insights from a contemporary multicenter US registry. Catheter Cardiovasc Interv. 2017;90(1):12-20. doi: 10.1002/ccd.26780
3. Fan LM, Tong D, Mintz GS, Mamas MA, Javed A. Breaking the deadlock of calcified coronary artery lesions: A contemporary review. Catheter Cardiovasc Interv. 2021;97(1):108-120. doi: 10.1002/ccd.29221
4. Sharma SK, Bolduan RW, Patel MR, et al. Impact of calcification on percutaneous coronary intervention: MACE-Trial 1-year results. Catheter Cardiovasc Interv. 2019;94(2):187-194. doi: 10.1002/ccd.28099
5. Riley RF, Henry TD, Mahmud E, et al. SCAI position statement on optimal percutaneous coronary interventional therapy for complex coronary artery disease. Catheter Cardiovasc Interv. 2020;96(2):346-362. doi: 10.1002/ccd.28994
6. Wexler L, Brundage B, Crouse J , et al. Coronary artery calcification: pathophysiology, epidemiology, imaging methods, and clinical implications. A statement for health professionals from the American Heart Association. Writing Group. Circulation. 1996;94(5):1175-1192. doi: 10.1161/01.cir.94.5.1175
7. ELCA Coronary Laser Atherectomy Catheter Philips.Updated 2023. Accessed February 19, 2023. https://www.philips.co.uk/healthcare/product/HCIGTDELCALASR/elca-coronary-laser-atherectomy-catheter#features
8. Rotablator Rotational Atherectomy System. Boston Scientific Corporation. Updated 2023. Accessed February 19, 2023. https://www.bostonscientific.com/en-IN/products/atherectomy-systems/rotablator-rotational-atherectomy-system.html
9. Protty MB, Gallagher S, Farooq V, et al. Combined use of rotational and excimer lASER coronary atherectomy (RASER) during complex coronary angioplasty-An analysis of cases (2006-2016) from the British Cardiovascular Intervention Society database. Catheter Cardiovasc Interv. 2021;97(7):E911-E9188. doi: 10.1002/ccd.29377
10. Daniel M, Suneel T, Jokhi PP, et al. How should I treat severe coronary artery calcification when it is not possible to dilate a balloon or deliver a RotaWire™? EuroIntervention. 2011;6(6):779-783. doi: 10.4244/EIJV6I6A132
11. Egred M. RASER angioplasty. Catheterization and Cardiovascular Interventions. 2012;79(6):1009-1012. doi: 10.1002/ccd.23174
12. Fernandez JP, Hobson AR, McKenzie D, et al. Beyond the balloon: Excimer coronary laser atherectomy used alone or in combination with rotational atherectomy in the treatment of chronic total occlusions, non-crossable and non-expansible coronary lesions. EuroIntervention. 2013;9(2):243-250. doi: 10.4244/EIJV9I2A40
13. Fernandez JP, Hobson AR, McKenzie D, Talwar S, O’Kane P. Treatment of calcific coronary stenosis with the use of excimer laser coronary atherectomy and rotational atherectomy. Interv Cardiol. 2010;2(6):801-806. doi: 10.2217/ICA.10.83
14. Xue Y, Zhou B, Wang W, et al. An application of RASER technique in the treatment of chronic total occlusion accompanied with stent fracture in right coronary artery: A case report. BMC Cardiovasc Disord. 2019;19(1):273. doi: 10.1186/s12872-019-1258-1
15. Mintz GS, Popma JJ, Pichard AD, et al. Patterns of calcification in coronary artery disease. A statistical analysis of intravascular ultrasound and coronary angiography in 1155 lesions. Circulation. 1995;91(7):1959-1965. doi: 10.1161/01.cir.91.7.1959
16. What is the Great North Care Record? Great North Care Record. National Health Services. Accessed November 22, 2023. https://www.greatnorthcarerecord.org.uk.
17. Abdel-Wahab M, Richardt G, Joachim Büttner H, et al. High-speed rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions: The randomized ROTAXUS (Rotational Atherectomy Prior to Taxus Stent Treatment for Complex Native Coronary Artery Disease) trial. JACC Cardiovasc Interv. 2013;6(1):10-19. doi: 10.1016/j.jcin.2012.07.017
18. Chambers JW, Feldman RL, Himmelstein SI, et al. Pivotal trial to evaluate the safety and efficacy of the orbital atherectomy system in treating de novo, severely calcified coronary lesions (ORBIT II). JACC Cardiovasc Interv. 2014;7(5):510-518. doi: 10.1016/j.jcin.2014.01.158
19. Hill JM, Kereiakes DJ, Shlofmitz RA, et al. Intravascular lithotripsy for treatment of severely calcified coronary artery disease. J Am Coll Cardiol. 2020;76(22):2635-2646. doi: 10.1016/j.jacc.2020.09.603
20. Mehran R, Rao SV, Bhatt DL, et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the Bleeding Academic Research Consortium. Circulation. 2011;123(23):2736-2747. doi: 10.1161/CIRCULATIONAHA.110.009449
21. Huber MS, Mooney JF, Madison J, Mooney MR. Use of a morphologic classification to predict clinical outcome after dissection from coronary angioplasty. Am J Cardiol. 1991;68(5):467-71. doi: 10.1016/0002-9149(91)90780-o
22. Ellis SG, Ajluni S, Arnold AZ, et al. Increased coronary perforation in the new device era. Incidence, classification, management, and outcome. Circulation. 1994;90(6):2725-30. doi: 10.1161/01.cir.90.6.2725
23. Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87-165. doi: 10.1093/eurheartj/ehy394
24. Ozaki Y, Yamaguchi T, Suzuki T, et al. Impact of cutting balloon angioplasty (CBA) prior to bare metal stenting on restenosis. Circ J. 2007;71(1):1-8. doi: 10.1253/circj.71.1













