


A Comparison of In-Hospital Outcomes Between the Use of Impella and IABP in Acute Myocardial Infarction Cardiogenic Shock Undergoing Percutaneous Coronary Intervention
Abstract
Background. The use of Impella ventricular support systems and intra-aortic balloon pump (IABP) in acute myocardial infarction (AMI) complicated by cardiogenic shock (CS) has increased in recent years and expanded treatment options, although the comparative clinical outcomes and device safety remain unclear. Methods. We used the Nationwide Inpatient Sample database (2012-2017) to identify adults who were admitted for AMI complicated by CS and received percutaneous coronary intervention (PCI). The study sample was divided into Impella and IABP groups. Patient characteristics, hospital characteristics, and comorbidities were balanced between groups using propensity-score matching. Regression analysis was utilized to study outcome differences between groups. Results. We identified 51,150 patients, of whom 44,265 (86.54%) received IABP and 6885 (13.46%) received Impella. After propensity matching, compared with the Impella group (n = 1592), the IABP group (n = 8638) had lower rates of sepsis (6.44% vs 12.69%; P=.01), blood transfusion (8.92% vs 14.28%; P=.01), mortality (28.95% vs 49.59%; P<.01), and hospitalization costs ($49,420 vs $68,087; P<.001). The IABP group had similar rates of cardiac arrest (20.32% vs 22.22%; P=.32), in-hospital stroke (1.46% vs 1.59%; P=.37), and length-of-stay (8.56 days vs 8.64 days; P=.26) compared with the Impella group. Conclusion. In patients with CS complicating AMI who underwent PCI, Impella use compared with IABP was associated with higher mortality with no differences in in-hospital stroke and cardiac arrest rates, although study interpretation is limited by retrospective observational design and the potential for remaining confounders. Further prospective research is warranted to elucidate the optimal mechanical circulatory support device in these patients.
J INVASIVE CARDIOL 2022;34(2):E98-E103.
Key words: acute myocardial infarction, cardiogenic shock, mechanical circulatory support device, percutaneous coronary intervention
Introduction
The outcomes of acute myocardial infarction (AMI) have improved in the past decades,1 thanks to advances in pharmacological treatment and reperfusion with primary percutaneous coronary intervention (PCI) in particular.2 However, cardiogenic shock (CS) occurring in approximately 4%-12% of patients with AMI remains accompanied by 40%-50% mortality despite prompt revascularization and both pharmacologic and mechanical circulatory support.3 Intra-aortic balloon pump (IABP) has been widely used in the United States (US). However, the clinical benefit of IABP use in AMI-CS patients has been questioned by several investigations, specifically, the neutral results in 30-day mortality between IABP and optimal medical therapy from the IABP-SHOCK II trial, resulting in a downgrade in consensus guideline recommendations, and a decrease in its use for this indication.4-6 On the other hand, Impella ventricular support system (Abiomed) use in AMI-CS patients has increased since its approval by the US Food and Drug Administration (FDA) in 2008. With a potential for improved hemodynamic support, there has been an expectation that Impella use would result in better outcomes compared with IABP use in AMI-CS patients. Randomized controlled trials that have compared Impella with IABP demonstrated no statistically significant difference in 30-day mortality.7-10 However, these trials were underpowered. A recent observational study using registry data showed that Impella use was associated with a higher adjusted risk of in-hospital death and major bleeding complications compared with IABP.11 To add more information to this important topic, we constructed a larger retrospective cohort study using the National Inpatient Sample (NIS) database and utilized propensity matching to compare several relevant in-hospital outcomes between Impella and IABP.11
Methods
The NIS is the largest publicly available all-payer inpatient database in the US. It is maintained by the Agency for Healthcare Research and Quality (Rockville, Maryland), and represents an approximately 20% stratified sample of discharges from non-federal hospitals in the US, with more than 4000 hospitals and 7 million medical records each year. NIS is a billing-based database. It is structured with the International Classification of Diseases-9th Edition-Clinical Modification (ICD-9) before October 2015, International Classification of Diseases-10th Edition-Clinical Modification (ICD-10) after October 2015, and Clinical Classification Software codes. As NIS data are deidentified, this study was exempt from institutional review board evaluation.12
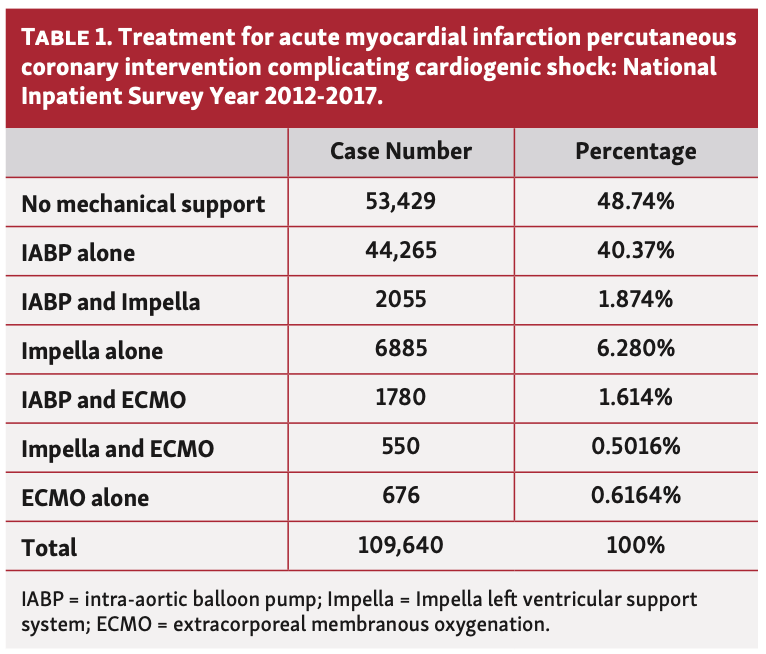
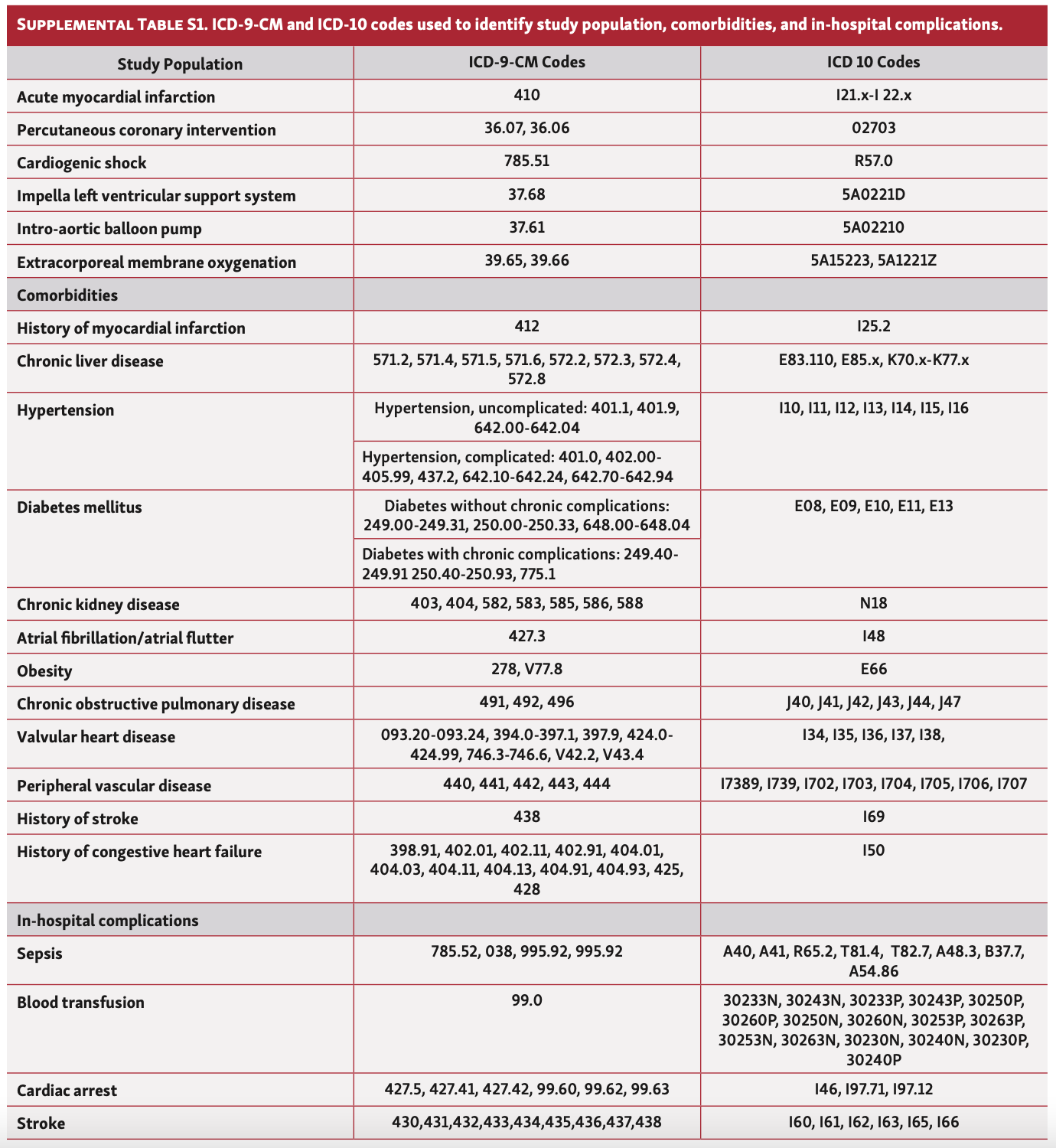
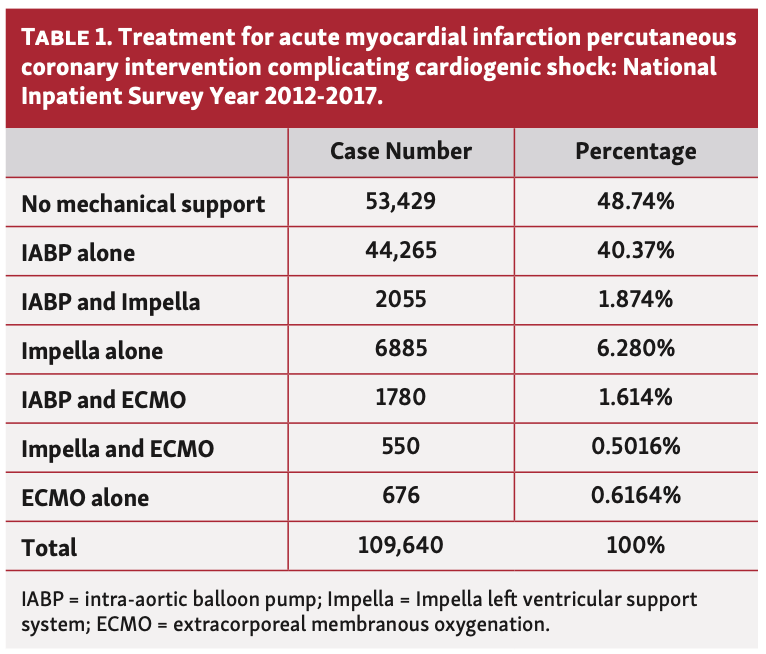
We used the 2012-2017 NIS database and identified all adult patients with a principal diagnosis of AMI, complicated by CS, who received PCI during the hospital course. Among these patients, we identified those who received either IABP or Impella support (Table 1).13 Patients who did not receive any mechanical support, who received both IABP and Impella, and who received other mechanical circulatory support devices including extracorporeal membrane oxygenation (ECMO) were excluded. Patient demographics (age, sex, race, etc), hospital characteristics (location, teaching status, and size), and comorbidities were identified with appropriate ICD-9 and ICD-10 codes (Supplemental Table S1). We also obtained the insurance status, length-of-stay (LOS), and total cost of hospital stays from the database.
The outcomes evaluated in this study were as follows: (1) in-patient mortality; (2) LOS and total cost of hospitalizations; and (3) in-hospital complications, including requirement for blood transfusion, sepsis, cardiac arrest, and in-hospital stroke.
Due to the survey design of the NIS, stratification, clustering, and weighting were applied during analysis to produce accurate estimates. To reduce the possibility of confounding by indication, we performed propensity-score matching using Kernel matching with common support to general propensity weights.14 Patient characteristics (age, race, sex, insurance, etc), hospital characteristics (location and size, etc), and comorbidities (history of congestive heart failure, atrial fibrillation, chronic kidney disease, etc) were incorporated into our propensity-score matching model. The balance was tested and most variables were satisfied between the Impella group and the IABP group. Unbalanced variables (history of congestive heart failure, diabetes mellitus, history of coronary artery disease, and location of hospital) despite propensity-score matching were included in the multivariable analysis model to further reduce bias.
Proportions were compared using the Chi-square test, and continuous variables were compared using the Student’s t-test. The normality assumption was evaluated by visual examination of histograms. Multivariable logistic regression analysis was used to adjust for potential confounders, including demographics, hospital characteristics, and comorbidities. Multivariate logistic regression was implemented for categorical outcome variables, including in-hospital mortality, the requirement for blood transfusion, sepsis, cardiac arrest, and in-hospital stroke. Linear regression was implemented for continuous outcome variables including LOS and total cost. Both regression analyses were implemented on both unadjusted and propensity-matched data, with adjustment of all patient characteristics, hospital characteristics, and baseline morbidities. Analyses were performed with Stata, version 14 (StataCorp LP). All P-values were 2-sided, with P-value <.05 as evidence to reject the null hypothesis.
Results
Between 2012 and 2017, a total of 109,640 patients had an AMI complicated by CS and had PCI, of which 53,429 patients (48.74%) did not receive mechanical circulatory support. A total of 44,265 patients (40.37%) received only an IABP and 6885 patients (6.28%) received only an Impella device. A total of 2055 patients (1.87%) received both IABP and Impella. A total of 3006 patients (2.73%) received ECMO treatment, either alone or with IABP or Impella during the same hospital stay. Only patients who received either an IABP or an Impella were included in our analysis (Table 1).
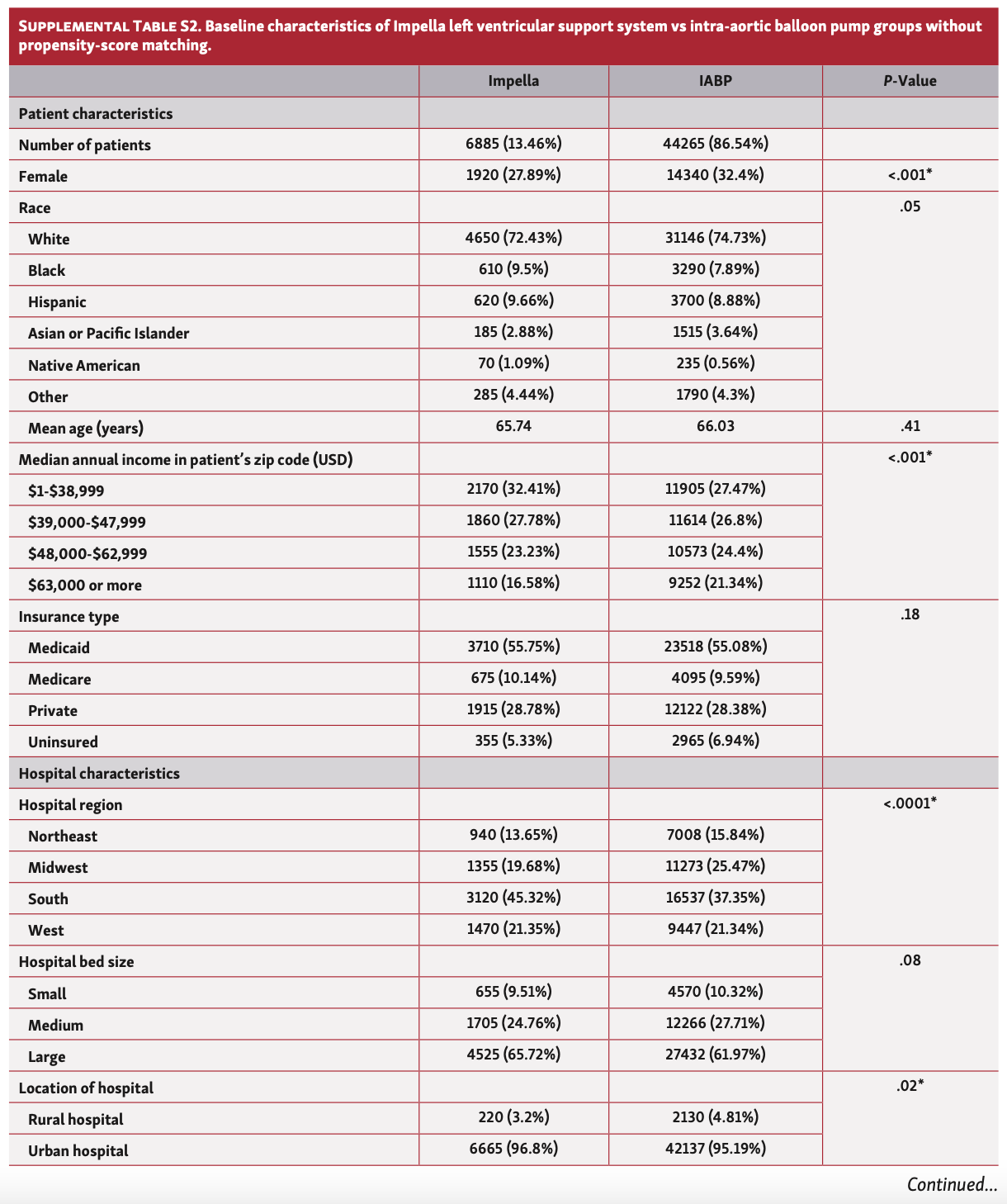
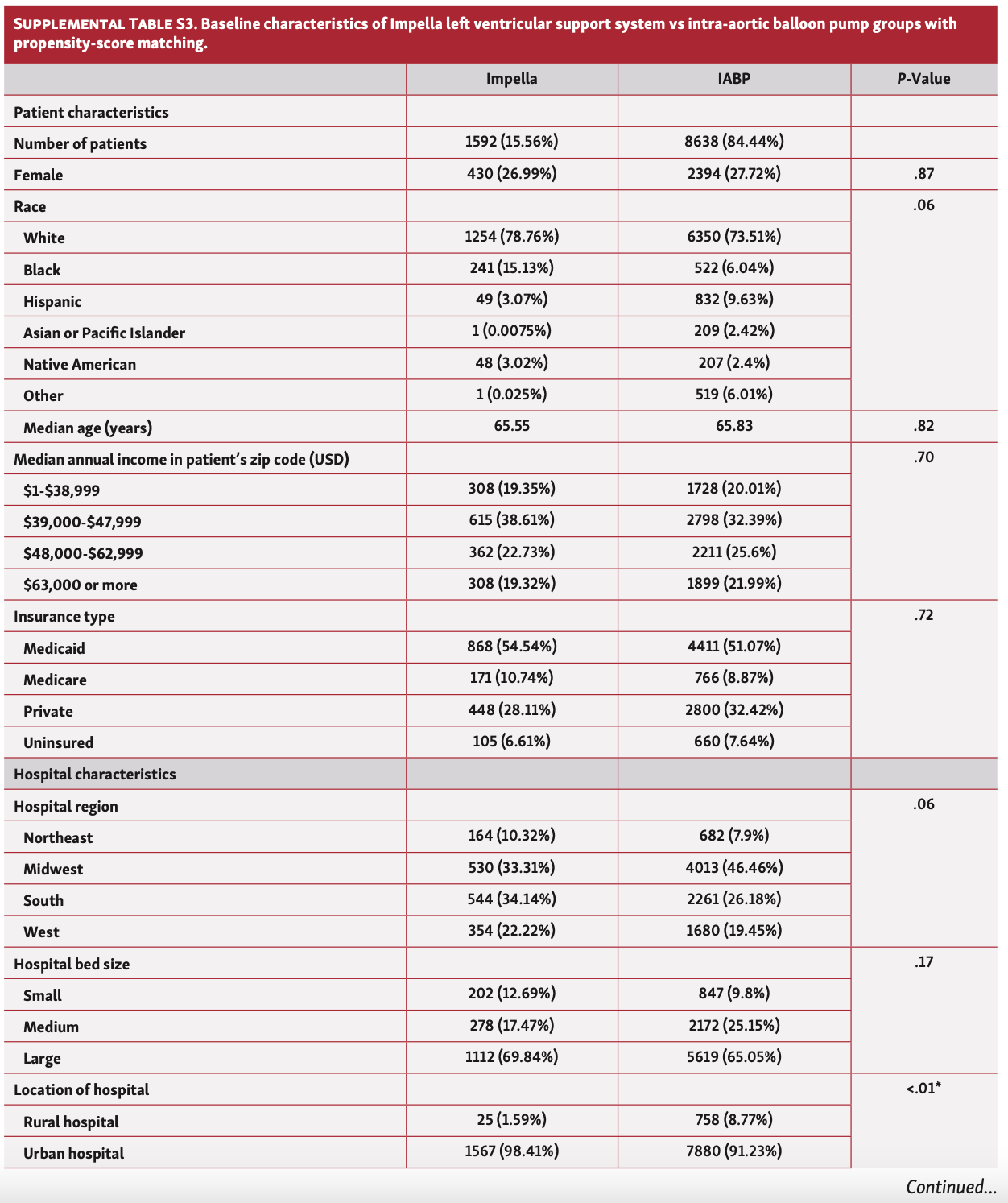
The IABP group was more likely to be female and hospitalized in non-teaching hospitals. There were no statistically significant differences in race, median age, insurance type, bed size, and location of the hospital between groups. Compared with patients who received an Impella device, those who received an IABP had lower rates of congestive heart failure (CHF), chronic liver disease, chronic kidney disease, chronic obstructive lung disease, history of prior myocardial infarction, peripheral vascular disease, hypertension, diabetes mellitus, atrial fibrillation or atrial flutter, and history of diagnosed coronary artery disease. There were no differences between groups in rates of obesity, history of prior stroke, and valvular heart disease (Supplemental Table S2).
With propensity score matching, 1592 patients (15.56%) who received Impella were matched with 8638 patients (84.44%) who received IABP support, resulting in a well-matched sample despite history of coronary artery disease, diabetes mellitus, and history of CHF not able to be successfully balanced (Supplemental Table S3). Further adjustment with patient characteristics, hospital characteristics, and baseline morbidities was implemented in regression analysis.
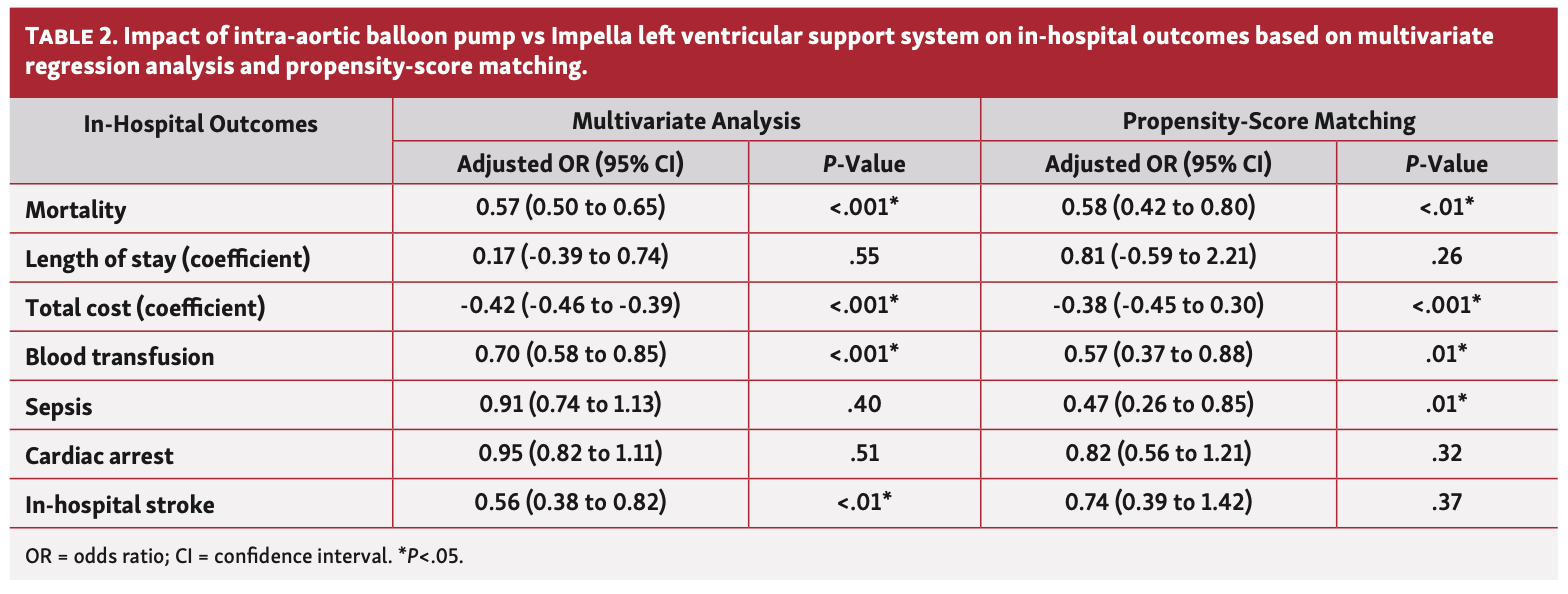
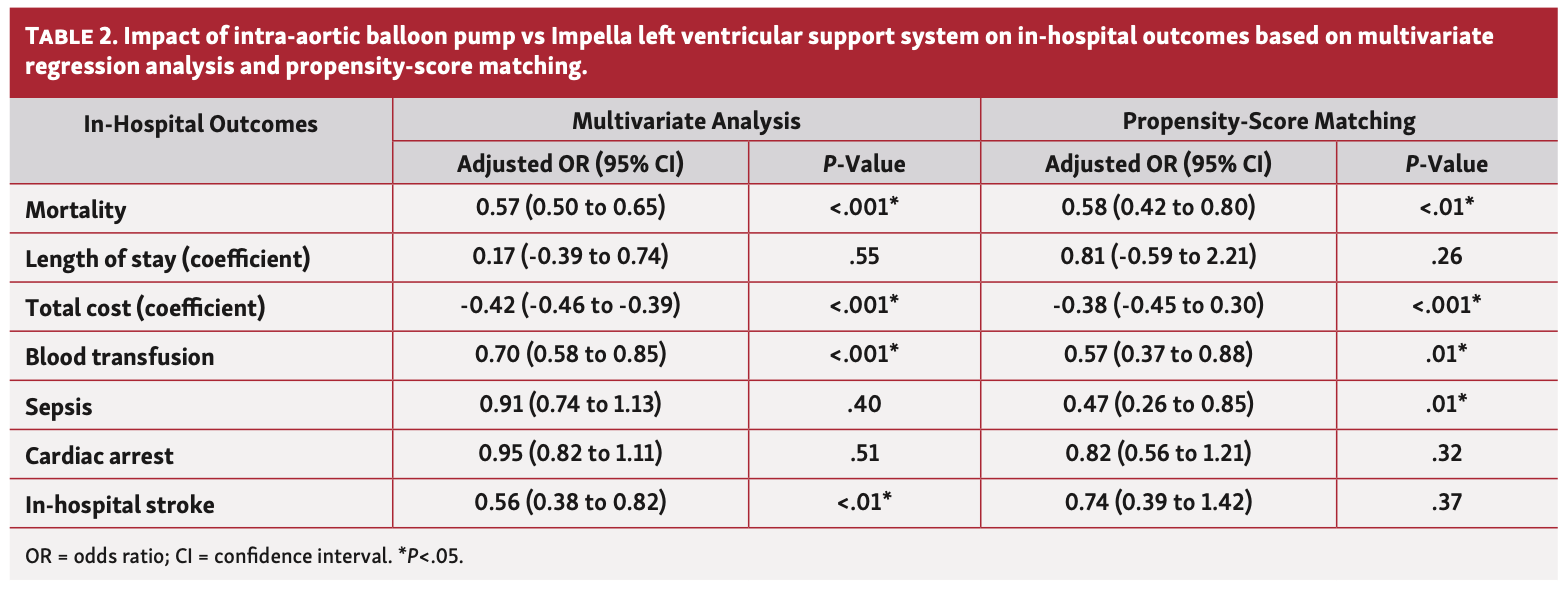
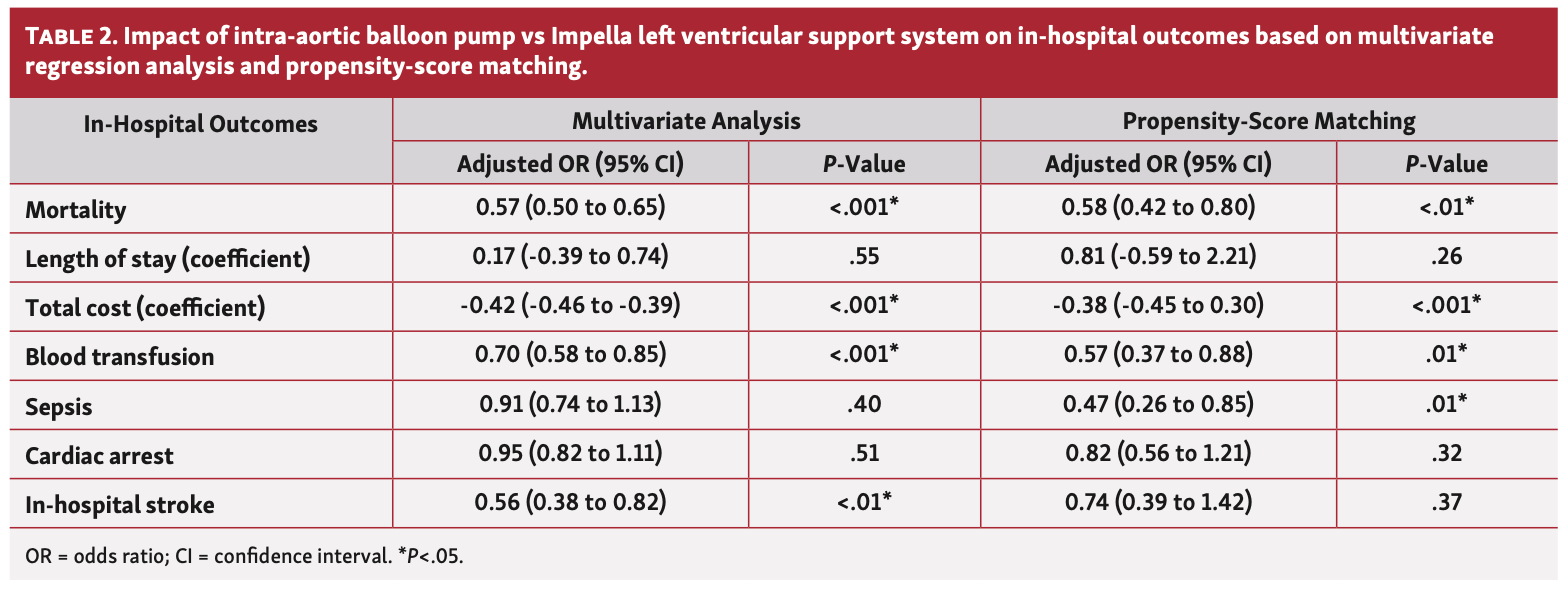
In the unadjusted analysis, mortality was 29.6% in the IABP group, which was significantly lower than the Impella group (42.87%; P<.001). Results were consistent after propensity matching; the IABP group had a significantly lower mortality rate compared with the Impella group (28.95% vs 49.59%; P<.01). (Table 2).
The unadjusted analysis showed that the mean LOS was 8.60 ± 0.096 days in the IABP group vs 8.91 ± 0.27 days in the Impella group. In the propensity-score matching model, no significant difference in LOS was found between the IABP group and the Impella group (8.56 ± 0.39 days vs 8.64 ± 0.76 days, respectively; P=.26).
The mean total hospitalization cost was $47,160 ± 466.17 (US dollars) in the IABP group vs $70,665 ± 1312.5 in the Impella group in unadjusted analysis. In the propensity-score matching model, the IABP group total hospitalization cost was significantly less than in the Impella group ($49,420 ± 1660.2 vs $68,087 ± 3436.7, respectively; P<.001) (Table 2).
In the unadjusted data, in-hospital complication rates were as follows: requirement of blood transfusion was 14.38% in the Impella group vs 10.32% in the IABP group (P<.001); rate of sepsis was 10.53% in the Impella group vs 6.89% in the IABP group (P=.40); rate of cardiac arrest was 23.38% in the Impella group vs 19.10% in the IABP group (P=.51); and rate of in-hospital stroke was 4.40% in the Impella group vs 1.27% in the IABP group (P<.01).
In the propensity-score matched model, there was no difference between the IABP group compared with the Impella group in cardiac arrest (20.32% vs 22.22%; P=.32) and in-hospital stroke (1.46% vs 1.59%; P=.37). However, the IABP group was associated with a lower risk of requirement for blood transfusion (8.92% vs 14.28%; P=.01) and sepsis (6.44% vs 12.69%; P=.01) (Table 2).
Discussion
In the present study, the largest of its kind, we used a national database to investigate the contemporary in-hospital outcomes in patients with AMI-CS who underwent revascularization with PCI during hospitalization and also required mechanical circulatory support with either Impella or IABP. After adjustment and in propensity-score matching, compared with Impella, IABP was associated with lower in-hospital mortality rates and lower cost. Also, there was evidence of lower rates of requirement for blood transfusion and sepsis, and no differences in in-hospital stroke or cardiac arrest rates.
Despite advancements in pharmacological therapies and interventional procedural techniques and devices, AMI-CS is associated with a significant mortality.3 Mechanical circulatory support devices have been developed to improve clinical outcomes. IABP could increase coronary blood flow and oxygen supply, as well as improve systemic perfusion.15 However, the IABP-SHOCK II trial in 2012 showed inferior survival and increased risk of major in-hospital bleeding in patients who received IABP compared with optimal medical treatment in AMI-CS. Subsequently, the routine use of IABP in CS has been downgraded in both the US and European guidelines.4-6
The Impella device is relatively new, with the first device approved by the US FDA in 2008. The device is positioned across the aortic valve via a peripheral artery and creates continuous forward blood flow from the left ventricle into the aorta by a rotary pump. Theoretically, it directly unloads the left ventricle while improving perfusion of critical organs to a larger extent than the IABP. Despite benefit in hemodynamic variables, all randomized clinical trials, including the PROTECT II trial (Impella 2.5 vs IABP), ISAR-SHOCK trial (Impella 2.5 vs IABP), IMPELLA-STIC (IABP vs IABP then switch to Impella 5.0), and IMPRESS in Severe Shock trial (Impella CP vs IABP), were not able to discern a survival benefit over IABP, with trials underpowered due to difficult enrollment in many cases. Nonetheless, the use of Impella has increased over the past few years,16 which was driven by observational data and FDA approval in defined subsets.7-9
More recently, the utility of Impella devices in this setting was questioned by a propensity-matched registry analysis by Dhruva et al.11 The study included 28,304 AMI patients complicated by CS who underwent PCI from October 2015 to December 2017 and found that the Impella device was associated with a significantly higher risk of in-hospital death (45.0% vs 34.1%; P<.001) and in-hospital bleeding (31.3% vs 16.0%; P<.001) compared with IABP.
In our study, we included a larger sample of 51,150 AMI-CS patients who underwent PCI and received either Impella or IABP. We found that the Impella was associated with a higher risk of in-hospital death and higher total cost after adjustment and propensity-score matching. However, we found there was no difference in length of hospital stay, in-hospital stroke, or cardiac arrest between the 2 groups. For the rates of requirement for blood transfusion and sepsis, there was evidence of higher risk with Impella, which may be attributed to the larger sheath used by Impella compared with the IABP.17
Our finding of higher mortality in the Impella group is consistent with other recent observational registry-based studies.11,16 This finding is contrary to all 4 available RCTs that directly compared IABP and Impella, which did not show an increased risk of mortality in the same group.7-10 One possible explanation is that the sample sizes of the randomized controlled trials were too small to demonstrate a difference in mortality benefit or harm, given that the largest sample size was less than 500 (PROTECT-II), and this was a high-risk PCI trial rather than one in patients with CS, while the other 3 enrolled less than 50 subjects. Another, more likely, explanation is that physicians tend to make the decision to implant Impella in patients who have a higher mortality risk as assessed by Society for Cardiovascular Angiography & Interventions (SCAI) shock stage, or in those who have already failed IABP implantation.18 Due to the retrospective nature of registry studies, it is impossible to obtain all clinical data to assess SCAI shock stage and perfectly match patients with comparable predicted mortality risk into IABP and Impella groups, therefore creating persistent selection bias despite our best efforts to adjust for baseline differences. Indeed, our propensity matching was unable to match by diabetes, CHF, or prior coronary disease, all variables that were higher in the Impella group and are known to increase mortality. The mortality rate of roughly 30% in the IABP group is well below the reported mortality for CS in the current era, and therefore it is likely that these were less sick patients that remained incompletely adjusted despite our best statistical methods and propensity-score matching.
From a complication standpoint, Impella 2.5 and Impella CP require a 13 or 14 Fr sheath compared with 7 or 8 Fr sheath for IABP, which therefore theoretically increases the risk of bleeding, vascular complications, and sepsis.17 The increased risk of major bleeding that required blood transfusion and sepsis with Impella was redemonstrated in our study. This result echoes the recent finding by Dhruva et al, but differs from the randomized controlled trial results.7-11
Our findings are also the first to relay no difference in stroke risk between Impella and IABP in patients with CS treated with PCI. A meta-analysis of IABP in CS found an increased risk of stroke compared with patients who did not receive an IABP, raising the possibility that retrograde atheroembolism during diastolic IABP inflation may promote stroke.19 The findings herein suggest by comparison that Impella may also increase the risk of stroke to a similar extent, although the mechanism remains unknown. It is also possible that hypoperfusion in patients receiving mechanical support of any type may increase the risk of stroke.20
The current study also relays that there appears to be no difference in LOS, but a higher cost with the use of Impella. The similar LOS perhaps argues against the Impella group being sicker; however, it is also likely that the higher mortality in the Impella group could have reduced the total LOS in these patients, making the overall difference insignificant between groups.
Study limitations. Although this is the largest study comparing IABP and Impella in patients with CS complicating AMI who underwent PCI during the same admission, there are limitations to our study. First, our study is retrospective in nature with inherent limitations regarding selection bias and confounders. Second, the NIS is a claim-based database with possible bias by erroneous coding, with no access to medications used, laboratory results, specific model of medical device implanted, and diagnostic test findings that may aid to further match patients appropriately to eliminate selection bias.18 Nonetheless, NIS powered us with a large number of cases and we used propensity-score matching to the best of our ability to decrease bias.
To date, registry-based retrospective observational studies (Premier Healthcare Database, National Inpatient Survey, CathPCI, and Chest Pain-MI) have all showed there is increased mortality compared with historic controls with Impella.16,21 However, none of the prior randomized controlled trials showed a difference in mortality.6-8,10 One prospective observational study (National Cardiogenic Shock Initiative) showed the use of Impella following a protocol-based approach has improved mortality in patients with CS complicating AMI compared with historic data in the SHOCK trial.22
Therefore, more evidence, especially well-powered randomized controlled trials in key SCAI shock stages C and D would be essential to further elucidate the role of Impella in patients with MI treated with PCI but complicated by CS. This would likely eliminate many of the IABP patients who do not fulfill the definition of shock, and therefore had lower mortality. The DanGer Shock trial (NCT01633502) is a prospective, multicenter, open-label randomized controlled trial started in Denmark and Germany that plans to enroll a total of 360 subjects and directly compares Impella with current guideline-driven therapy, making it the largest randomized controlled trial on this topic.23 Its primary outcome will be 6-month mortality. This study is likely to add valuable information and insight into the role of Impella in patients with AMI complicated by CS, especially if stratified in analysis by SCAI shock stage.
Conclusion
In patients with AMI complicated by CS who underwent PCI from 2012 to 2017, Impella use compared with IABP was associated with higher mortality but similar rates of stroke and cardiac arrest, although study interpretation is limited by retrospective observational design, inability to control for all known confounders, and a lower than expected mortality rate in the IABP group, indicating heterogeneity of shock definition between groups. Our study is the largest study to date to examine this subject, and it is the first to find no difference in in-hospital stroke or LOS while being associated with higher cost. Further prospective research in appropriately selected samples, particularly stratified by SCAI shock stage, is warranted to put these retrospective studies and available randomized controlled trials in context and elucidate the optimal mechanical circulatory support device in these patients.
Affiliations and Disclosures
From the 1Department of Medicine, Westchester Medical Center, Valhalla, New York; 2Department of Cardiology, Westchester Medical Center, Valhalla, New York; and 3Department of Internal Medicine, University of Iowa Carver College of Medicine, Iowa City, Iowa.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript accepted March 23, 2021.
Address for correspondence: Srihari S. Naidu, MD, FACC, FAHA, FSCAI, Department of Cardiology, Westchester Medical Center, Valhalla, New York. 100 Woods Road, Valhalla, NY 10595. Email: Srihari.Naidu@wmchealth.org
Related Articles
- The Single-Access Technique for Impella-Protected Percutaneous Coronary Intervention: A Single-Center Experience
- Protected Percutaneous Coronary Intervention of Unprotected Left Main Using Impella Ventricular Assist Device Before Transcatheter Aortic Valve Implantation: A Single-Center Experience
- VA-ECMO With IABP is Associated With Better Outcome Than VA-ECMO Alone in the Treatment of Cardiogenic Shock in ST-Elevation Myocardial Infarction
References
1. Goldberg RJ, Spencer FA, Gore JM, Lessard D, Yarzebski J. Thirty-year trends (1975 to 2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction: a population-based perspective. Circulation. 2009;119:1211-1219.
2. Aissaoui N, Puymirat E, Tabone X, et al. Improved outcome of cardiogenic shock at the acute stage of myocardial infarction: a report from the USIK 1995, USIC 2000, and FAST-MI French nationwide registries. Eur Heart J. 2012;33:2535-2543.
3. Patel H, Shivaraju A, Fonarow GC, et al. Temporal trends in the use of intraaortic balloon pump associated with percutaneous coronary intervention in the United States, 1998-2008. Am Heart J. 2014;168:363-373.e12.
4. Authors/Task Force members, Windecker S, Kolh P, et al. 2014 ESC/EACTS guidelines on myocardial revascularization: the task force on myocardial revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014;35:2541-2619.
5. O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61:e78-e140.
6. Thiele H, Zeymer U, Thelemann N, et al. Intraaortic balloon pump in cardiogenic shock complicating acute myocardial infarction: long-term 6-year outcome of the randomized IABP-SHOCK II Trial. Circulation. Nov 11 2018. Online ahead of print.
7. O'Neill WW, Kleiman NS, Moses J, et al. A prospective, randomized clinical trial of hemodynamic support with Impella 2.5 versus intra-aortic balloon pump in patients undergoing high-risk percutaneous coronary intervention: the PROTECT II study. Circulation. 2012;126:1717-1727.
8. Seyfarth M, Bauer I, Sibbing D, Bott-Flügel L, Kastrati A, Schömig A. A prospective and randomized trial to compare a left ventricular assist device (Impella LP2. 5) with IABP in patients with cardiogenic shock by acute myocardial infarction: the ISAR-SHOCK trial. J Am Coll Cardiol. 2008;52:1584-1588.
9. Bochaton T, Huot L, Elbaz M, et al. Mechanical circulatory support with the Impella® LP5.0 pump and an intra-aortic balloon pump for cardiogenic shock in acute myocardial infarction: The IMPELLA-STIC randomized study. Arch Cardiovasc Dis. 2020;113:237-243.
10. Ouweneel DM, Eriksen E, Sjauw KD, et al. Percutaneous mechanical circulatory support versus intra-aortic balloon pump in cardiogenic shock after acute myocardial infarction. J Am Coll Cardiol. 2017;69:278-287.
11. Dhruva SS, Ross JS, Mortazavi BJ, et al. Association of use of an intravascular microaxial left ventricular assist device vs intra-aortic balloon pump with in-hospital mortality and major bleeding among patients with acute myocardial infarction complicated by cardiogenic shock. JAMA. 2020;323:734-745.
12. NIS database. Accessed January 14, 2022. https://www.hcup-us.ahrq.gov/db/nation/nis/nisdbdocumentation.jsp
13. Pahuja M, Adegbala O, Mishra T, et al. Trends in the incidence of in-hospital mortality, cardiogenic shock, and utilization of mechanical circulatory support devices in myocarditis (Analysis of National Inpatient Sample Data, 2005-2014). J Card Fail. 2019;25:457-467.
14. DuGoff EH, Schuler M, Stuart EA. Generalizing observational study results: applying propensity score methods to complex surveys. Health Serv Res. 2014;49:284-303.
15. Taguchi I, Ogawa K, Kanaya T, Matsuda R, Kuga H, Nakatsugawa M. Effects of enhanced external counterpulsation on hemodynamics and its mechanism. Circulation. 2004;68:1030-1034.
16. Amin AP, Spertus JA, Curtis JP, et al. The evolving landscape of Impella use in the United States among patients undergoing percutaneous coronary intervention with mechanical circulatory support. Circulation. 2020;141:273-284.
17. Schrage B, Ibrahim K, Loehn T, et al. Impella support for acute myocardial infarction complicated by cardiogenic shock. Circulation. 2019;139:1249-1258.
18. Baran DA, Grines CL, Bailey S, et al. SCAI clinical expert consensus statement on the classification of cardiogenic shock. Catheter Cardiovasc Interv. 2019;94:29-37.
19. Fan Z-G, Gao X-F, Chen L-W, et al. The outcomes of intra-aortic balloon pump usage in patients with acute myocardial infarction: a comprehensive meta-analysis of 33 clinical trials and 18,889 patients. Patient Prefer Adherence. 2016;10:297-312.
20. Sjauw KD, Engström AE, Vis MM, et al. A systematic review and meta-analysis of intra-aortic balloon pump therapy in ST-elevation myocardial infarction: should we change the guidelines? Eur Heart J. 2009;30:459-468.
21. Dhruva SS, Ross JS, Mortazavi BJ, et al. Association of use of an intravascular microaxial left ventricular assist device vs Intra-aortic balloon pump with in-hospital mortality and major bleeding among patients with acute myocardial infarction complicated by cardiogenic shock. JAMA. 2020;323:734-745.
22. Basir MB, Kapur NK, Patel K, et al. Improved outcomes associated with the use of shock protocols: updates from the National Cardiogenic Shock Initiative. Catheter Cardiovasc Interv. 2019;93:1173-1183.
23. Udesen NJ, Møller JE, Lindholm MG, et al. Rationale and design of DanGer shock: Danish-German cardiogenic shock trial. Am Heart J. 2019;214:60-68.













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}