


Drug-Coated Balloon Strategy Following Intravascular Lithotripsy to Treat Coronary De Novo Lesion: Mid-Term Clinical Outcomes of a Preliminary Experience
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Abstract
Objectives. The management of patients with calcified de novo lesions remains a major clinical challenge even in the era of drug-eluting stents (DES). Drug-coated balloon (DCB) therapy has emerged as an alternative to DES to treat de novo lesions. Nevertheless, the management of calcified lesions using intravascular lithotripsy (IVL) combined with DCB to treat de novo lesions has not been investigated. The authors report the short-term results of our preliminary experience with this novel approach.
Methods. The authors conducted a multicenter retrospective study of 14 patients who underwent percutaneous coronary intervention for de novo lesions treated with IVL followed by DCB in 3 centers between September 2023 and July 2024.
Results. The mean age of the patients was 69 years, and 71% were male. At 30 days, 1 patient experienced non-cardiac death. No lesion site thrombosis, target lesion revascularization (TLR), or cardiac death occurred at the 30-day follow-up. At the 6-month follow-up, 2 (14.3%) patients experienced TLR.
Conclusions. This real-world data using IVL followed by DCB (in cases of acceptable lesion preparation) in patients with de novo calcified coronary lesions suggest that this strategy is feasible and appears to have an acceptable target lesion failure rate at mid-term follow-up. This proof of concept could be hypothesis-generating for larger studies.
Introduction
Percutaneous coronary intervention (PCI) of heavily calcified lesions continues to represent a significant clinical challenge, even with use of the latest generation drug-eluting stents (DES). Such lesions are associated with suboptimal procedural results and an increased incidence of major adverse cardiac events (MACE), target lesion revascularization (TLR), and stent thrombosis (ST).1 In addition, PCI using the latest DES in calcified lesions with insufficient lesion preparation can result in stent underexpansion, which exposes the patient to increased risk of TLR and ST.
Drug-coated balloons (DCB) represent an emergent tool for interventional cardiologists, allowing local delivery of antiproliferative drugs such as paclitaxel or sirolimus through a single, prolonged balloon inflation.2,3 By avoiding permanent device implantation, this approach may limit late inflammatory reactions to stent components while preserving the potential for positive vascular remodeling. Although the technology is still under development and its place in the treatment of coronary artery disease (CAD) remains under investigation, current evidence supports a DCB-only strategy in clinical situations such as in-stent restenosis (ISR) and small-vessel disease.4 In calcified de novo lesions, DCB could have the potential to overcome the issue of stent underexpansion and could potentially lower the risk of ST. Previous non-randomized retrospective studies have suggested that a strategy combining DCB with rotational or orbital atherectomy in calcified lesions achieves outcomes comparable to those observed with DES implantations after atherectomy.5-7 Recently, intravascular lithotripsy (IVL) has proven to be an efficient adjunctive device for lesion preparation in severely calcified vessels.8-10 Nevertheless, the association of IVL to DCB in de novo calcified lesions has not been extensively reported. Therefore, we sought to report the short-term outcomes of patients treated with such a strategy.
Methods
Study population
This was an observational, retrospective, multicenter, single-arm study of consecutive patients treated with a combination of IVL and DCB between September 2023 and July 2024. In the analysis, all consecutive patients treated with an association of IVL and DCB for de novo coronary lesions were included. The decision to treat the lesion with an association of IVL and DCB rather than a new generation DES was left to the operator’s discretion. The study was conducted according to the Declaration of Helsinki. As this was a retrospective analysis conducted per institutional guidelines for data security and privacy, a waiver of consent was granted. Data were anonymized by authors prior to analysis.
Procedures
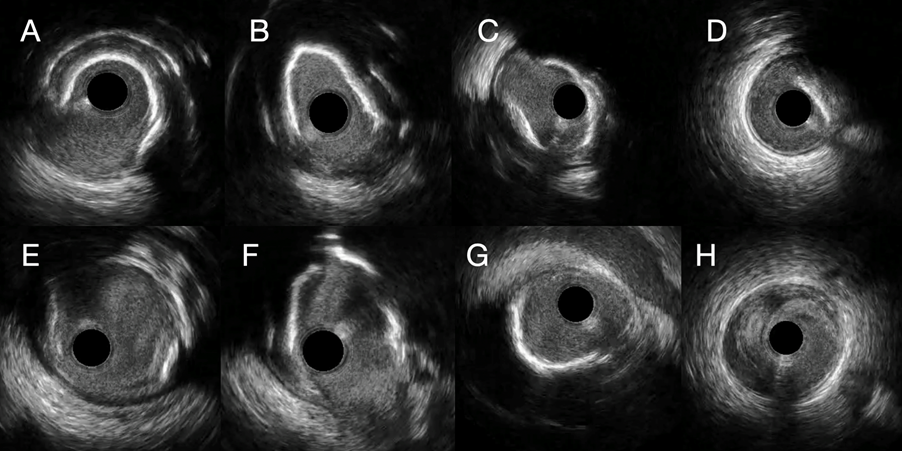
DCB applications were performed after lesion preparation using IVL. The use of plaque modifying balloons such as a cutting/scoring balloon or adjunctive atherectomy was left at operator’s decision. DCB application was performed as previously described.11 All DCBs used in this retrospective study were the paclitaxel-releasing SeQuent Please NEO (BBraun Medical). Intracoronary imaging with optical coherence tomography (OCT) (Ilumien Optis, Abbott) and intravascular ultrasound (IVUS) (AVVIGO+, Boston Scientific) pre- and/or post-DCB were at the operator’s discretion.
Follow-up and endpoints
Follow-up was performed via telephone or by clinical visits at 30 days and 6 months. Angiographic follow-up was not scheduled but performed only in case of symptom recurrence or non-invasive demonstration of inducible myocardial ischemia. The primary endpoint was a device-oriented composite endpoint (DOCE) of target lesion revascularization (TLR), lesion site thrombosis (LST), target vessel myocardial infarction (MI), and cardiac death.
Statistics
Discrete data are presented as frequencies and/or percentages, and continuous variables are presented as mean or median ± SD.
Results
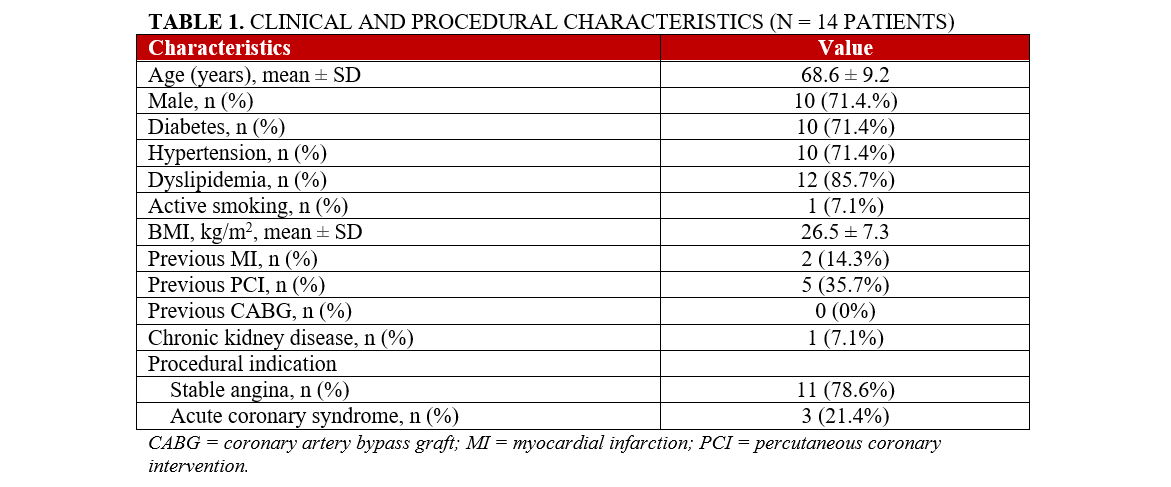
From September 2023 to July 2024, a total of 14 patients underwent PCI for de novo calcified lesions with the combination of IVL and DCB at 3 French institutions. Baseline clinical and demographic characteristics of the population are reported in Table 1.
Clinical and procedural characteristics
A total of 14 patients were included in the study, with a mean age of 68.6 ± 9.2 years. Ten (71.4%) patients were male and had high rates of cardiovascular risk factors, including 10 (71.4%) patients with diabetes, 10 (71.4%) with hypertension, and 12 (85.7%) with dyslipidemia. Active smoking was noted in only 1 (7.1%) patient, while 2 (14.3%) had a history of prior myocardial infarction (MI). Previous percutaneous coronary intervention (PCI) was reported in 5 (35.7%) patients, with no patient having undergone coronary artery bypass grafting (CABG). One patient (7.1%) had a history of chronic kidney disease. Chronic coronary syndrome was the most frequent procedural indication (11 patients, 78.6%), followed by acute coronary syndrome in 3 (21.4%) cases (Table 1).
Lesion and procedural characteristics
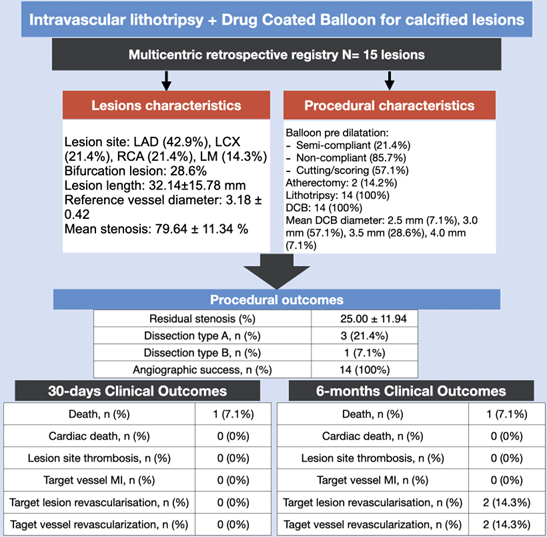
A total of 14 lesions were treated, with the most frequent lesion site being the left anterior descending artery (LAD) in 6 (42.9%) cases, followed by the left circumflex artery (LCx) and right coronary artery (RCA) (3 [21.4%] patients each), and the left main artery (LM) in 2 (14.3%) patients. Intravascular imaging was performed in 3 (21.4%) cases, and all procedures were performed through radial access. Bifurcation lesions involving the side branch were treated in 4 (28.6%) cases. The mean lesion length was 32.14 ± 15.78 mm, with a reference vessel diameter of 3.18 ± 0.42 mm. The mean stenosis was 79.64 ± 11.34% and ,after intervention, residual stenosis was reduced to 25.00 ± 11.94% (Table 2).
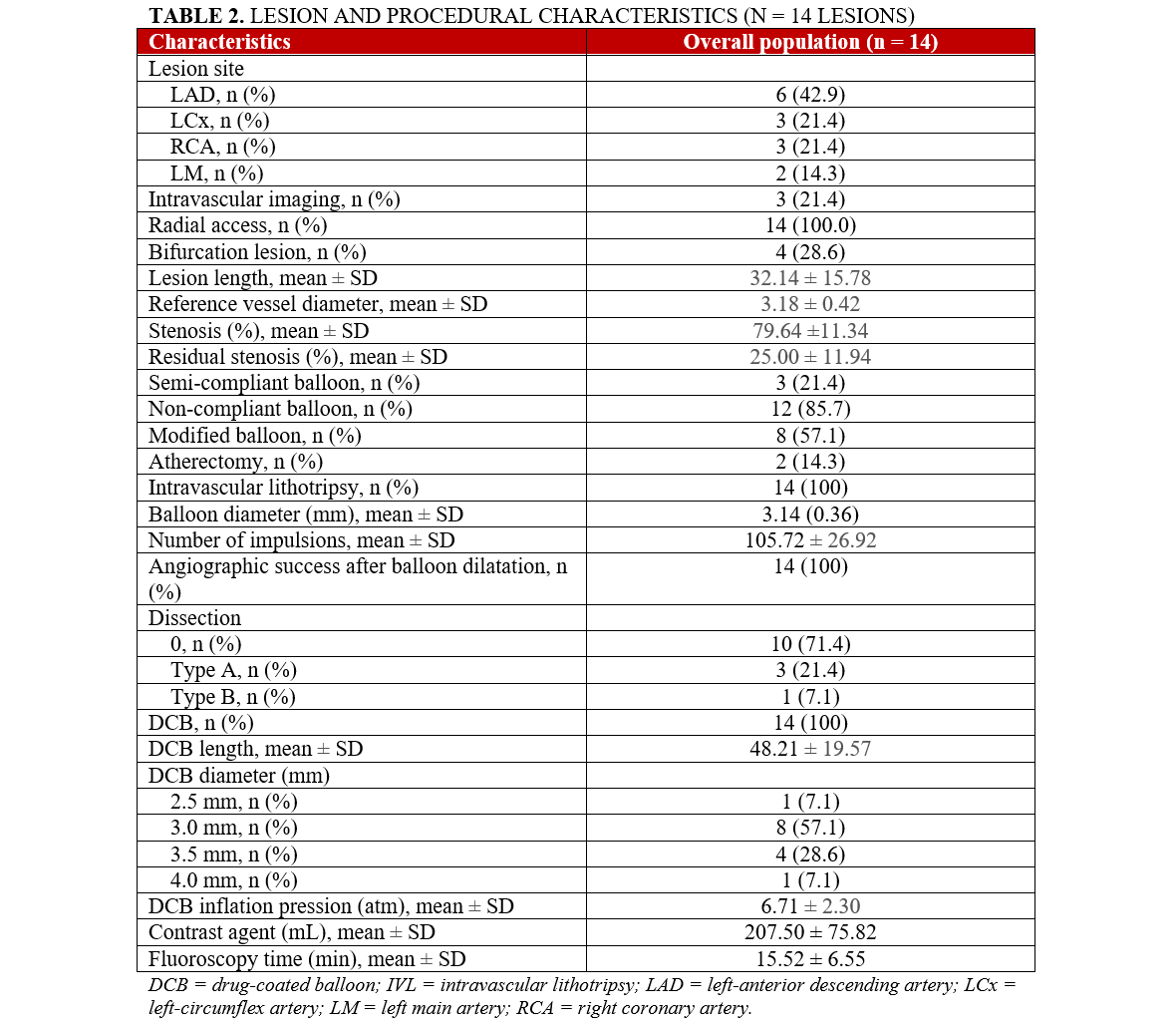
Lesion preparation with non-compliant balloons was used in 12 (85.7%) cases, while modified balloons (scoring/cutting) were used in 8 (57.1%) patients. Atherectomy was performed in 2 (14.3%) cases. All patients underwent lesion preparation using intravascular lithotripsy (IVL). The mean IVL balloon diameter was 3.14 ± 0.36 mm, and a mean of 105.72 ± 26.92 lithotripsy impulses were delivered per patient. Angiographic success following balloon dilatation was achieved in all patients. Dissection occurred in 4 (28.6%) patients, with 3 (21.4%) classified as Type A dissections and 1 (7.1%) as Type B.
Drug-coated balloons (DCB) were applied in all patients, with a mean DCB length of 48.21 ± 19.57 mm. Eight (57.1%) patients received a DCB with a diameter of 3.0 mm. The mean DCB inflation pressure was 6.71 ± 2.30 atm. The mean contrast agent volume used was 207.50 ± 75.82 mL, and the mean fluoroscopy time was 15.52 ± 6.55 minutes (Table 2).
Clinical outcomes
At the 30-day follow-up, 1 (7.1%) patient died of a non-cardiac cause. No patients experienced the primary endpoint, defined as lesion site thrombosis, target vessel MI, TLR, or target vessel revascularization (TVR) (Table 3). There were no reported cardiac deaths or device-related adverse events or complications during this period.
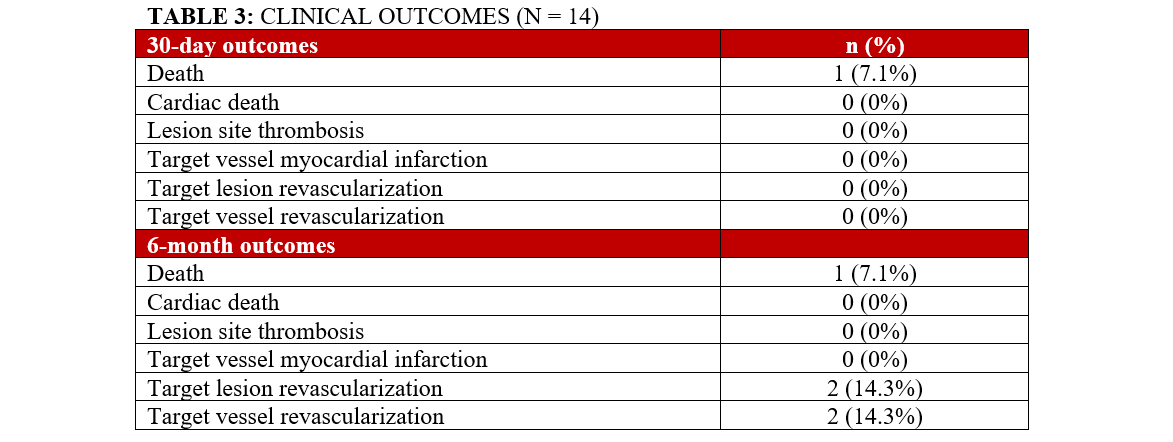
At 6 months, no cardiac deaths were reported. Four (28.6%) patients underwent control angiography at a median of 47 days (IQR: 22-94 days). Of these patients, 2 (14.3%) met the primary endpoint and required TLR.
Discussion
This retrospective multicenter study provides preliminary insight into the safety and feasibility of IVL with DCB angioplasty for the treatment of calcified de novo coronary lesions. Despite the complexity of treating calcified lesions, our findings demonstrate that this novel strategy is both safe and effective, with good angiographic and short-term clinical outcomes.
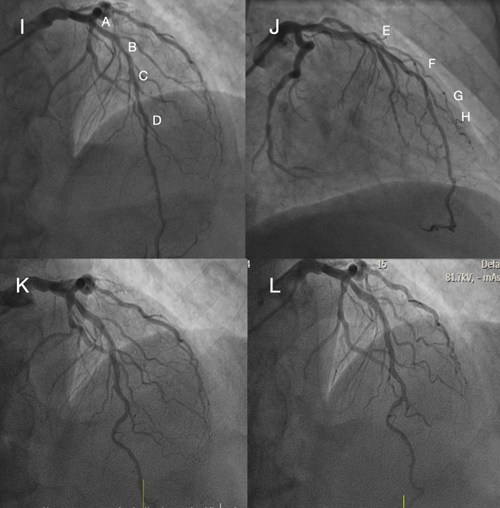
Lesion preparation is crucial in calcified CAD, as stent underexpansion due to calcification is a known predictor of target lesion failure. IVL uses sonic pressure waves to create microfractures in calcified plaques to allow more uniform plaque modification combined with balloon dilatation. In our study, all lesions were treated with IVL, achieving complete angiographic success (Figures 1 and 2). Importantly, there were no cases of lesion site thrombosis, even in these complex lesions after intensive lesion preparation and DCB alone without stent implantation.
DCBs offer an alternative to stent implantation in appropriately prepared lesions, allowing for drug delivery without leaving behind a permanent scaffold, which may reduce the risk of stent thrombosis and ISR. In calcified de novo lesions, the role of DCB remains understudied. While small, non-randomized trials have not found higher risk of target lesion failure with other DCB approaches using other modification techniques such as rotational atherectomy, this is the first report of the hybrid use of IVL and DCB. Our findings suggest that when combined with IVL for lesion preparation, DCB therapy provides excellent short-term outcomes with no acute vessel closure. All patients received the paclitaxel-releasing SeQuent Please NEO DCB, which is known to provide effective local drug delivery.
There was 1 non-cardiac death at the 30-day follow-up, but no patients experienced cardiac death, lesion site thrombosis, TLR, or TVR. These results compare favorably with other studies in complex lesion subsets, including those using rotational or orbital atherectomy followed by DES. At the 6-month follow-up, 4 (28.6%) patients had angiographic control and 2 (14.3%) had TLR. While the observed revascularization rate was higher than that reported in previous studies of IVL and DES PCI,12 the small sample size warrants cautious interpretation.
Limitations
First, this was a small, retrospective study with a relatively short follow-up period. As such, larger studies with longer follow-up are necessary to validate the findings and assess long-term outcomes, especially ISR. Second, the decision to use IVL and DCB was left to the operator’s discretion that could have led to selection bias. Additionally, the use of intracoronary imaging was low, mainly because of the cost limitations; larger use of intracoronary imaging could have had an impact on our results. Finally, the specific characteristics of lesions that are most suitable for this combination therapy remain to be clearly defined. Further research is needed to better identify which types of calcified lesions may benefit most from this approach and to develop more standardized criteria for its application.
Conclusions
In conclusion, the results of this multicenter study suggest that the association of IVL and DCB therapy to treat calcified de novo lesions is technically feasible and associated with low short-term clinical results in cases of acceptable lesion preparation. Given the limited sample size, these data could be considered hypothesis-generating for future trials to assess whether DCBs are equally effective as DES to treat calcified de novo lesions.
Affiliations and Disclosures
Fabien Picard, MD, PhD1; Vincent Pham, MD, MSc1; Sophia El Harrrouchi, MD2; Pierre Brami, MD1; Vincent Millien, MD3; Ludovic Meunier, MD2
From the 1Department of Cardiology, Cochin Hospital, Hôpitaux Universitaire Paris Centre, Assistance Publique - Hôpitaux de Paris, Paris, France; 2Department of Cardiology, Centre Hospitalier La Rochelle Ré Aunis, La Rochelle, France; 3Department of Cardiology, Centre Hospitalier de Saint-Quentin, Saint-Quentin, France.
Disclosures: Dr Picard reports research and consulting and speaking fees from AstraZeneca, Bayer, BBraun, Boehringer Ingelheim, Biotronik, BMS-Pfizer Alliance, Boston Scientific, Servier, and Sanofi, outside the submitted work. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Fabien Picard, Cardiology Department, Cochin Hospital, Hôpitaux Universitaire Paris Centre, Assistance Publique des Hôpitaux de Paris, 27 rue du Faubourg Saint-Jacques, Paris 75014, France. Email: Fabien.picard@aphp.fr; X: @picard_fabien
References
1. Bourantas CV, Zhang YJ, Garg S, et al. Prognostic implications of coronary calcification in patients with obstructive coronary artery disease treated by percutaneous coronary intervention: a patient-level pooled analysis of 7 contemporary stent trials. Heart. 2014;100(15):1158-1164. doi:10.1136/heartjnl-2013-305180
2. Jeger RV, Farah A, Ohlow MA, et al. Drug-coated balloons for small coronary artery disease (BASKET-SMALL 2): an open-label randomised non-inferiority trial. Lancet 2018;392:849-856. doi:10.1016/S0140-6736(18)31719-7
3. Rosenberg M, Waliszewski M, Chin K, et al. Prospective, large-scale multicenter trial for the use of drug-coated balloons in coronary lesions: the DCB-only All-Comers registry. Catheter Cardiovasc Interv. 2019;93(2):181-188. doi:10.1002/ccd.27724
4. Neumann FJ, Sousa-Uva M, Ahlsson A, et al; ESC Scientific Document Group. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87-165. doi:10.1093/eurheartj/ehy394
5. Kitani S, Igarashi Y, Tsuchikane E, et al. Efficacy of drug-coated balloon angioplasty after directional coronary atherectomy for coronary bifurcation lesions (DCA/DCB registry). Catheter Cardiovasc Interv. 2021;97(5):E614-E623. doi:10.1002/ccd.29185
6. Dong H, Shan Y, Gong S, et al. Clinical research of drug-coated balloon after rotational atherectomy for severe coronary artery calcification. BMC Cardiovasc Disord. 2023;23(1):40. doi:10.1186/s12872-023-03071-8
7. Okutsu M, Mitomo S, Ouchi T, et al. Impact of directional coronary atherectomy followed by drug-coated balloon strategy to avoid the complex stenting for bifurcation lesions. Heart Vessels. 2022;37(6):919-930. doi:10.1007/s00380-021-02000-z
8. Ali ZA, Nef H, Escaned J, et al. Safety and effectiveness of coronary intravascular lithotripsy for treatment of severely calcified coronary stenoses: the Disrupt CAD II study. Circ Cardiovasc Interv. 2019;12(10):e008434. doi:10.1161/CIRCINTERVENTIONS.119.008434
9. Brinton TJ, Ali ZA, Hill JM, et al. Feasibility of Shockwave coronary intravascular lithotripsy for the treatment of calcified coronary stenoses. Circulation. 2019;139(6):834-836. doi:10.1161/CIRCULATIONAHA.118.036531
10. Pham V, Bonnet M, Varenne O, et al. In-stent use of intravascular coronary lithotripsy for restenosis and stent underexpansion, a multicenter experience. Can J Cardiol. 2022;38(10):1474-1475. doi:10.1016/j.cjca.2022.05.0200.
11. Jeger RV, Eccleshall S, Wan Ahmad WA, et al; International DCB Consensus Group. Drug-coated balloons for coronary artery disease: third report of the International DCB Consensus Group. JACC Cardiovasc Interv. 2020;13(12):1391-1402. doi:10.1016/j.jcin.2020.02.043
12. Frampton J, Kearney KE, Abbott JD, et al. Coronary intravascular lithotripsy for treatment of severely calcified lesions: long-term sex-specific outcomes. J Soc Cardiovasc Angiogr Interv. 2023;2(6Part A):101069. doi:10.1016/j.jscai.2023.101069










