


Frailty Among Patients With Acute ST-Elevation Myocardial Infarction in the United States: The Impact of the Primary Percutaneous Coronary Intervention on In-Hospital Outcomes
Abstract
Objectives. To determine the average treatment effect (ATE) of primary percutaneous coronary intervention (pPCI) versus medical treatment (MT) on in-hospital outcomes across the spectrum of frailty in patients with ST-elevation myocardial infarction (STEMI). Methods. Adult patients hospitalized for STEMI between October 2015 until December 2017 from the National Inpatient Sample (NIS) database were retrospectively analyzed and stratified by the Hospital Frailty Risk Score into low, intermediate, and high frailty risk subgroups. Propensity score matching analysis was performed to estimate the ATE of pPCI in each frailty subgroup. The primary outcome was all-cause in-hospital death. Results. A total of 429,070 patients were included in the final analysis, with 28.4% at an increased frailty risk. Frail patients were significantly less likely to receive pPCI (85.6%, 47.2%, and 22.6% for low, intermediate, and high frailty risk groups). Rates of adverse in-hospital events including death, cerebrovascular event, and major bleeding were significantly higher in patients with increased frailty risk. pPCI was associated with a significant reduction of in-hospital death in low (-8.0%), intermediate (-14.6%), and high (-14.7%) frailty subgroups, compared to MT (P<.001). Conclusions. pPCI was associated with reduced rates of in-hospital death in patients with frailty presenting with STEMI. These findings suggest a benefit of pPCI in this complex patient population, although based on observational data. Long-term effects and safety need to be investigated in future studies.
J INVASIVE CARDIOL 2022;34(1):E55-E64.
Key words: frailty, hospital frailty risk score, optimal medical treatment, outcomes, primary percutaneous coronary intervention, ST-segment elevation myocardial infarction
Introduction
Frailty has been recognized as a predictor of poor prognosis among patients with cardiovascular (CV) diseases, including coronary artery disease (CAD), heart failure (HF), those undergoing cardiac surgery, and interventions for severe symptomatic aortic stenosis,1 thus is associated with increased all-cause mortality,2 prolonged hospitalizations,3 and unplanned hospital readmissions.4,5 Frail patients tend to be excluded from large clinical trials despite being increasingly encountered in contemporary real-world practice, due to a global aging of population. The efficacy and safety of many invasive treatments for CV conditions is unclear in frail patients, who often have complex comorbidities and are, therefore, at increased risk of sustaining complications from such procedures.6
Frail patients presenting with acute coronary syndrome (ACS) are less likely to be managed invasively and are known to have an increased likelihood of adverse in-hospital outcomes such as major bleeding.7 Observational data suggested immediate survival benefit of invasive management over conservative medical treatment (MT) in this population; however, residual confounders and potential selection bias should be taken into account when interpreting such results.8 Previous studies showed that many frail patients may benefit the most from coronary revascularization although are least likely to receive it.9,10,11 There is little known regarding the impact of primary PCI (pPCI) in frail patients with STEMI on relevant in-hospital outcomes.
Hence, we performed a propensity-score matched (PSM) analysis of patients hospitalized with STEMI in the United States (US) between 2015 and 2017 that were at different risks of frailty. Among these frailty risk categories, we sought to estimate the average treatment effect (ATE) of pPCI vs conservative MT on in-hospital death. Secondarily, we examined the in-hospital rates of major bleeding, acute renal failure, and cerebrovascular events across frailty risk categories and according to treatment type.
Methods
Study population and data source. In the present study, we retrospectively analyzed data from the National Inpatient Sample (NIS) which is the largest publicly available all-payer inpatient healthcare database in the United States (US). This database accounts for ~20% of all discharges from non-federal acute care hospitals in the US and contains anonymized data on primary and secondary discharge diagnoses and procedures undertaken in over 7 million hospital stays per year. The NIS database is sponsored by the Agency for Healthcare Research and Quality (AHRQ) and is a part of the Healthcare Cost and Utilization Project (HCUP). The NIS dataset includes sampling weights that help to reduce the margin of error and sampling bias and due to its multi-state nature is estimated to represent more than 97% of hospitalizations in the US.12
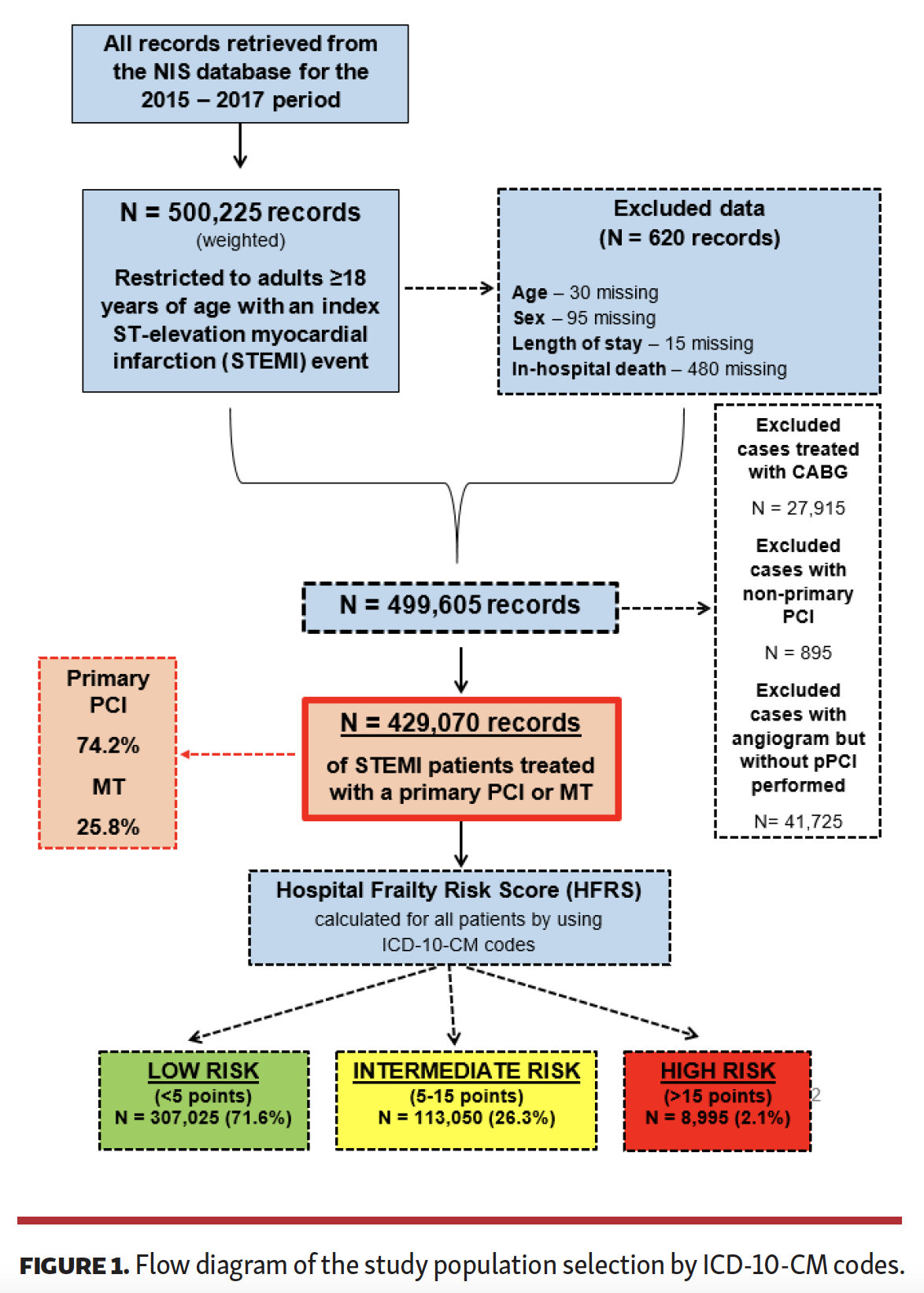
This patient sample included adults (≥18 years of age) hospitalized for the primary admission diagnosis of STEMI between October 2015 through December 2017. Patients that had missing data such as age, sex, length of stay (LoS), and in-hospital death were not included in the analysis. Patients treated with coronary artery bypass grafting (CABG) as the mode of revascularization, cases that had PCI performed but on days other than the first day of their admission (i.e., non-primary PCI) and patients that underwent diagnostic coronary angiography but did not receive PCI were excluded as well. The study flow chart is shown in Figure 1.
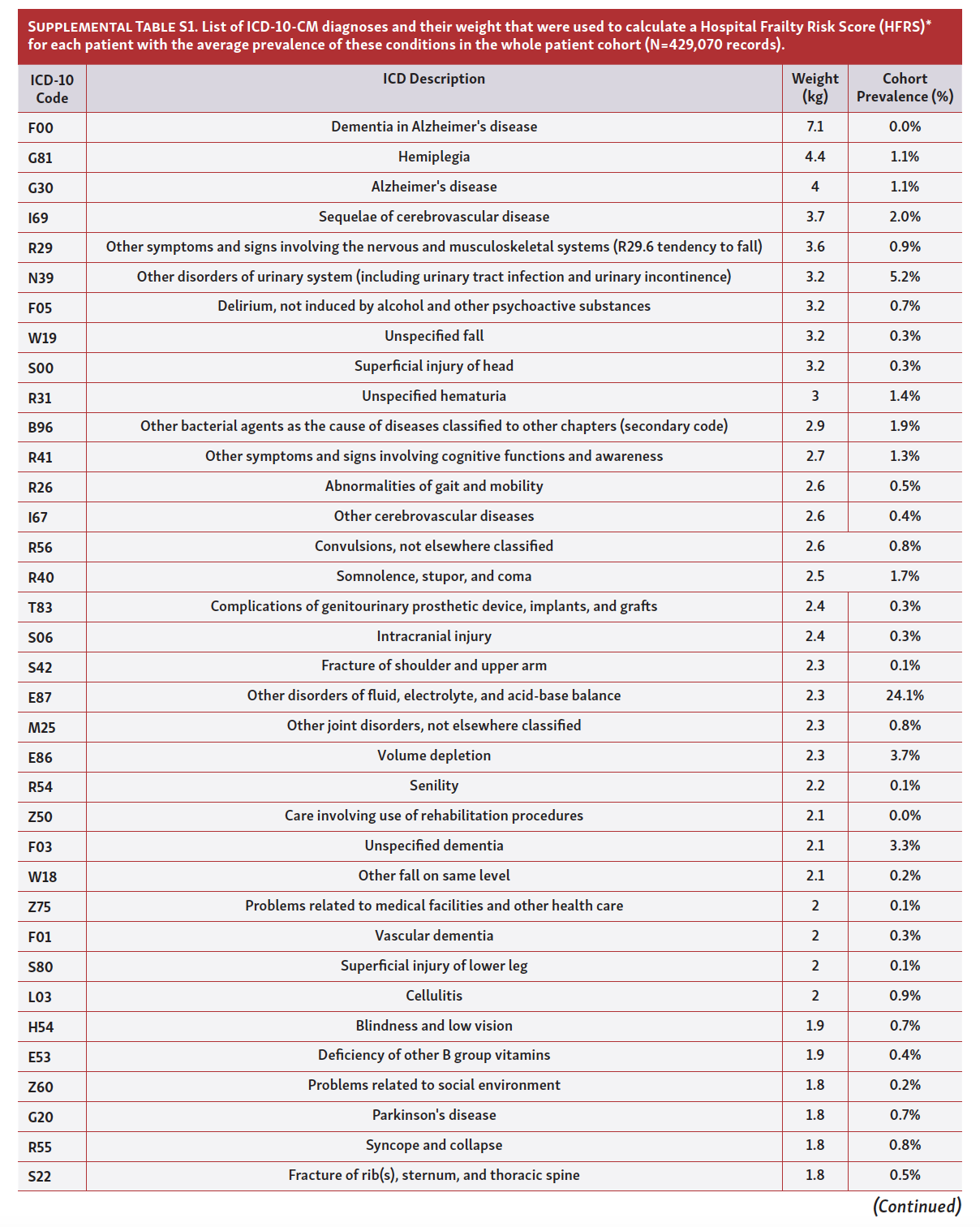
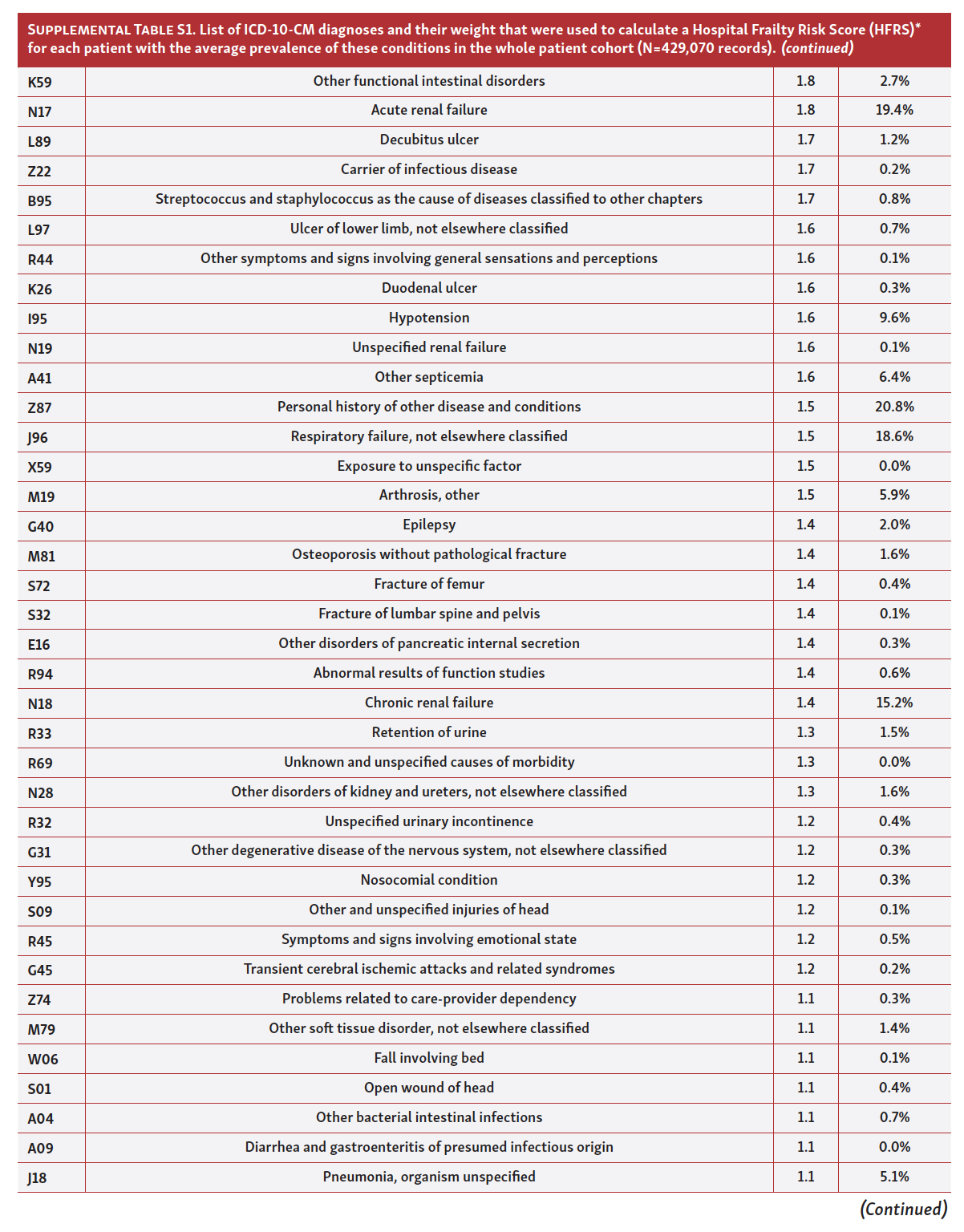
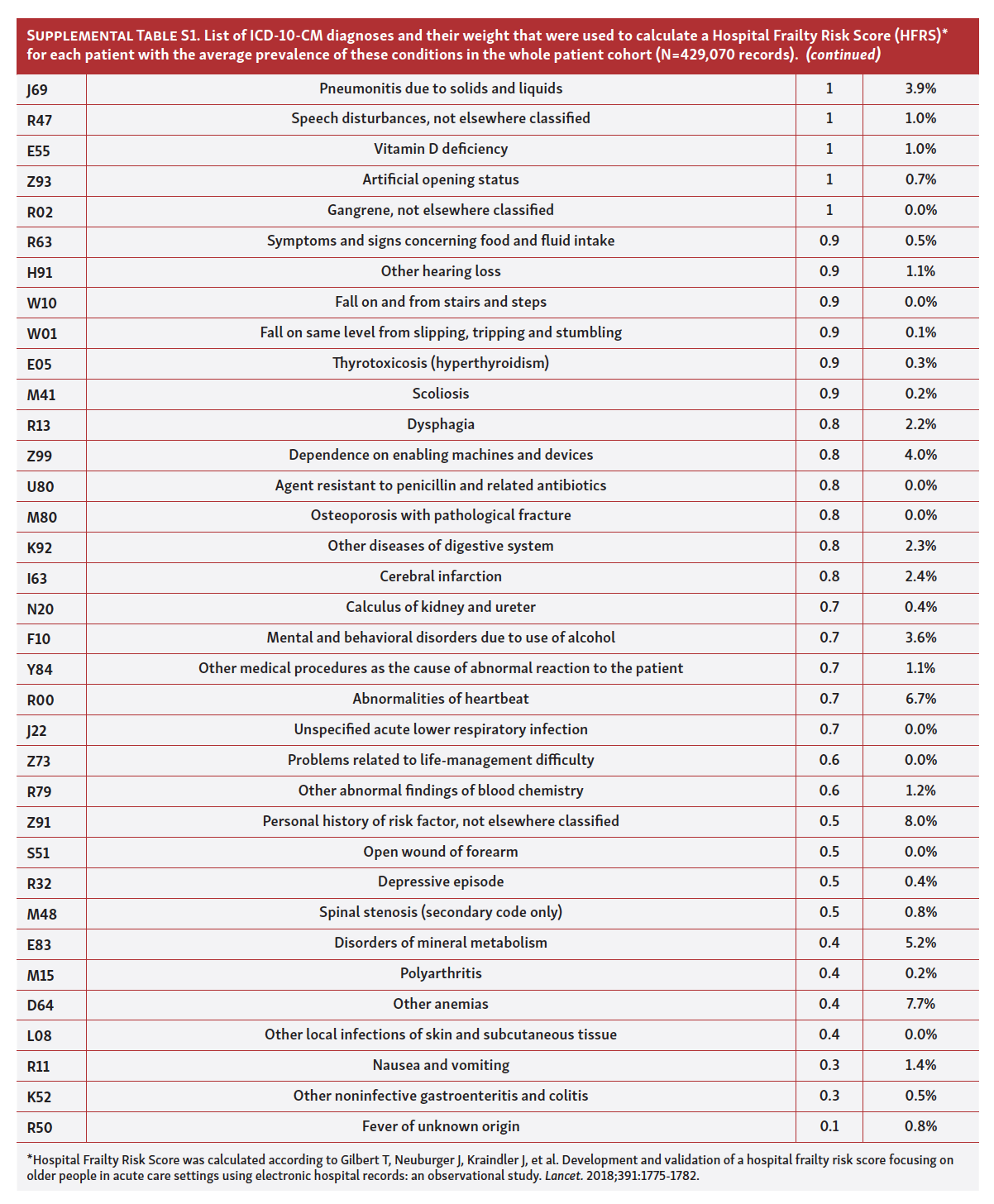
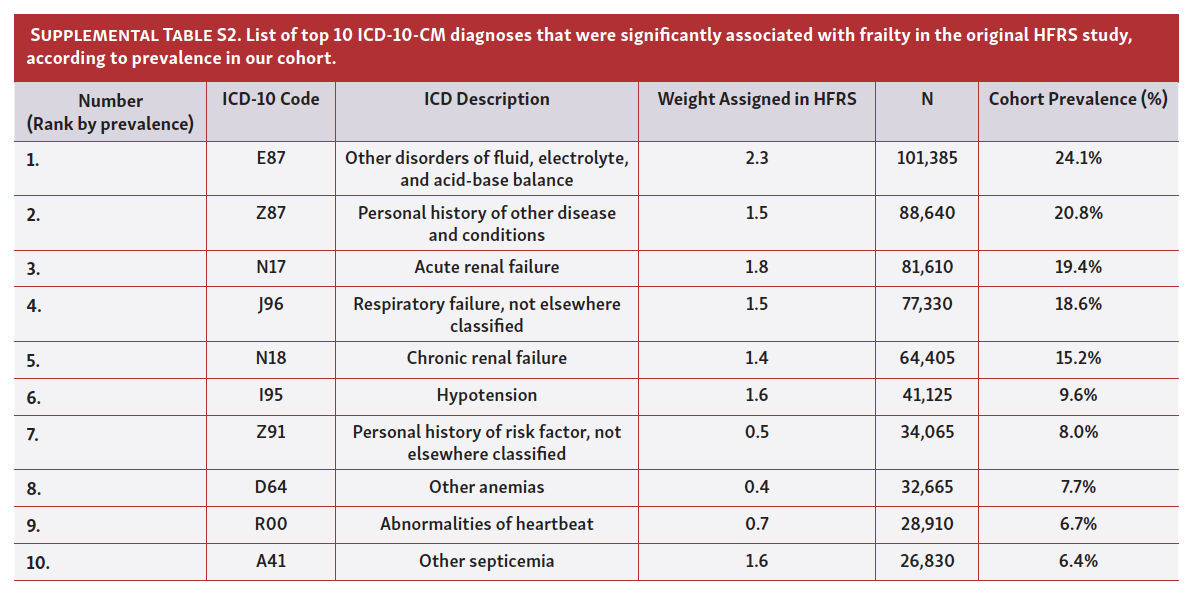
Definitions. Frailty risk in this study was estimated by stratifying patients into three risk categories by using a Hospital Frailty Risk Score (HFRS), a novel, standardized, and independently validated screening tool that utilizes data from electronic health records to identify frail patients who are at a greater risk of adverse outcomes.13,14 This score originally allowed for identification of frail individuals among inpatients with various causes of admission and it was significantly associated with an increased likelihood of all-cause 30-day mortality and hospital readmissions, a longer length of hospital stay and higher degree of functional impairment in data obtained from large hospital databases.13,14 HFRS is designed as a low-cost systematic tool that automatically calculates frailty risk based on information collected from hospital electronic health records that use the International Classification of Diseases 10th Revision Clinical Modification (ICD-10-CM) diagnostic codes. From these data, HFRS accounts for all diagnoses and clusters of conditions that were associated with high resource use and diagnoses significantly related to frailty in the original study while each diagnosis is weighted according to its relative contribution to frailty. The original study identified 50 such conditions with their corresponding prevalences in a frail population such as dementia, Alzheimer’s disease, history of traumatic falls, chronic kidney disease, atrial fibrillation, presence of a cataract, and similar. Consequently, the final obtained score stratifies patients into three frailty categories: low-risk (HFRS <5 points), intermediate-risk (HFRS 5-15 points), and high-risk (HFRS >15 points). The list of ICD-10-CM diagnostic codes used to build HFRS and their prevalence in the analyzed cohort of STEMI patients are provided in Supplemental Table S1 (Part 1, Part 2, Part 3). The list of top 10 ICD-10-CM diagnoses by their prevalence in the HFRS is provided in Supplemental Table S2.
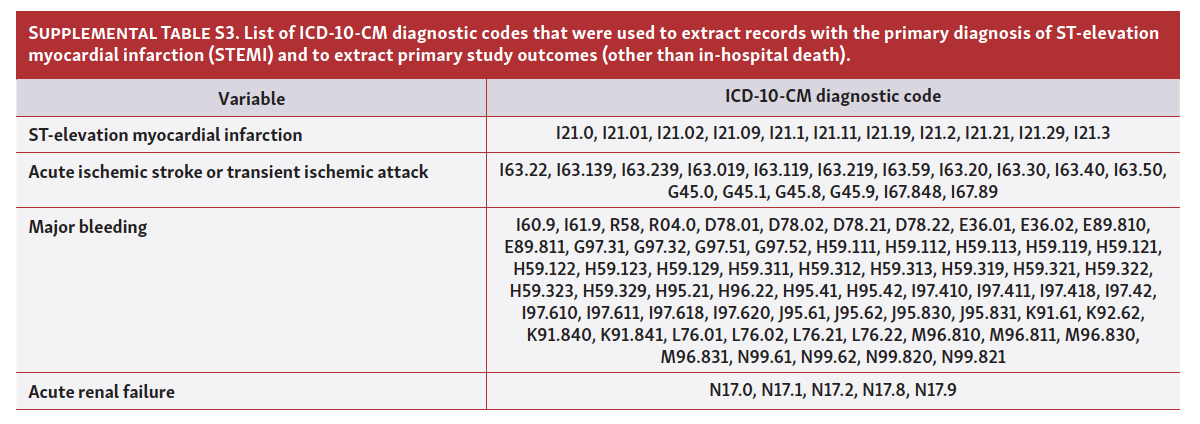
The primary diagnosis of STEMI was defined as the acute myocardial infarction encompassing ICD-10-CM diagnostic codes shown in Supplemental Table S3.
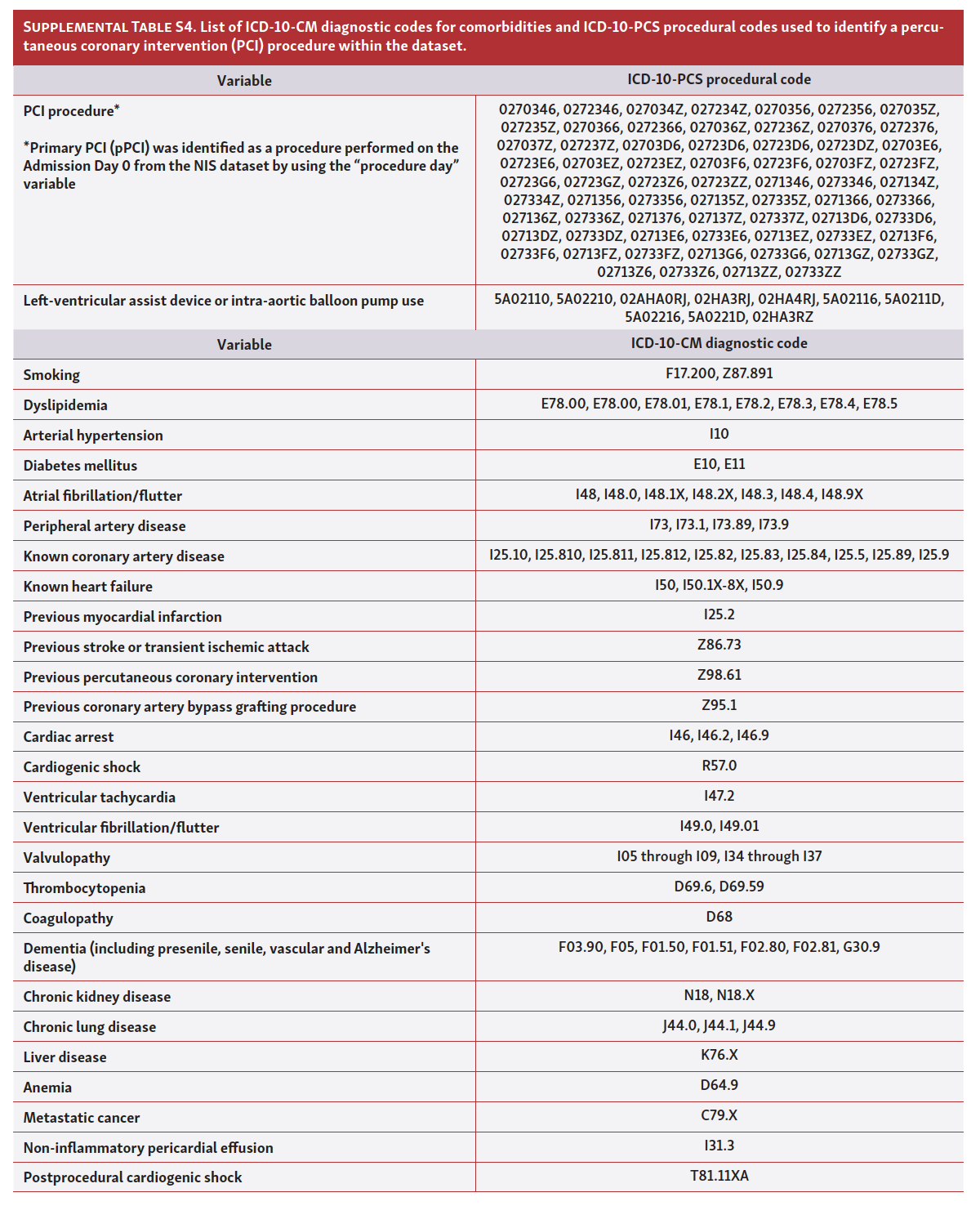
The principal aim of the study was to analyze the treatment effect of pPCI compared with MT across different frailty groups in STEMI patients. For this purpose, the MT group was comprised of patients that (a) did not undergo diagnostic cardiac catheterization and (b) did not receive any form of revascularization. However, patients that underwent diagnostic coronary angiography but without pPCI performed (cath+ / PCI-) were included in sensitivity analyses to determine if the main outcome results would significantly differ if these patients were included in the MT group. Accordingly, pPCI procedure was defined as the PCI procedure performed on admission day 0 by using information from the “procedure day” variables. For the identification of PCI procedures within the dataset, we used International Classification of Diseases 10th Revision Procedure Coding System (ICD-10-PCS) codes while patients’ comorbidities were identified by using ICD-10-CM diagnostic codes (Supplemental Table S4). Data were also collected on patients’ sociodemographic status including age, sex, race, primary expected payer, quartile of household income based on the ZIP code, weekend admission, hospital bed size, teaching status of the hospital, hospital ownership, mean HFRS, LoS, and mean hospitalization cost (US$). Multivessel disease in this study was defined as a disease on ≥2 epicardial coronary vessels.
Outcomes. The primary outcome of treatment effect was all-cause in-hospital death. The secondary outcomes of interest were in-hospital events consisting of acute stroke or transient ischemic attack (TIA), acute renal failure, and major bleeding (ICD-10-CM extraction codes used to capture these outcomes are provided in Supplemental Table S3).
Statistical analysis. All analyses were carried out using SPSS for Windows, version 26 (IBM) and Stata, version 14 (StataCorp). Data were presented as mean ± standard deviation (SD) for continuous variables and counts (N) or proportions (%) for categorical variables. For continuous variables, frailty group means were compared using t-tests of independent samples for two groups, or with one-way ANOVAs for three groups. The Chi-square (χ2) test was used for categorical variables. Separate multivariable logistic regression models were performed to evaluate the association of different frailty risk categories with the primary outcome. In these analyses, a low frailty risk category was set as the reference to which intermediate and high frailty risk categories were compared. All regression models were adjusted for age, sex, race, weekend admission, elective procedure, LoS, admission year, primary expected payer, quartile of income, arterial hypertension, dyslipidemia, diabetes mellitus, peripheral artery disease, known CAD, previous MI, known HF, previous PCI, previous CABG, previous stroke or TIA, atrial fibrillation/flutter, valvulopathy, chronic lung disease, chronic renal failure, liver disease, anemia, metastatic cancer, coagulopathy, thrombocytopenia, hospital bed size, hospital teaching status, hospital geographic region, cardiogenic shock, in-hospital treatment type, and multivessel disease. For these analyses, adjusted odds ratios (ORs), 95% confidence intervals (95% CIs), and P-values were reported.
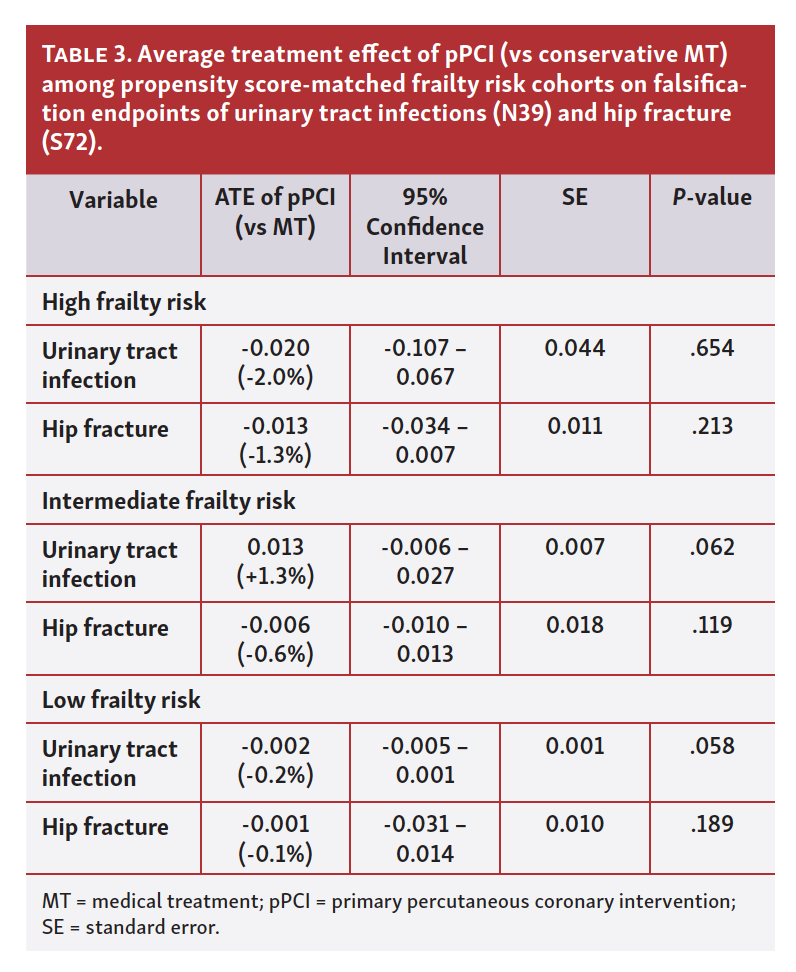
Each frailty risk subgroup was separately propensity score-matched (PSM) with respect to treatment type (pPCI vs MT) in order to estimate the average treatment effect (ATE) of pPCI versus conservative treatment on the outcome of in-hospital death. The ATE is defined as the average difference in the designated outcome with and without treatment and is expressed as the coefficient with the corresponding 95% CIs, z- and P-values. Therefore, the risk of death associated with pPCI is increased if the coefficient is positive while is reduced if the coefficient is negative. When multiplied by 100 this coefficient can also be expressed as the percentage (%) point. Obtained ATE coefficients for each frailty subgroup were compared to see if they significantly differ from each other by using the suest command in Stata. Additional PSM analysis was performed by including cath+ / PCI- patients in the OMT group for sensitivity analysis. Details of PSM and ATE analysis are provided in the Appendix 1. To further assess for selection biases / unmeasured confounders when studying pPCI treatment with respect to mortality across frailty risk subgroups, we performed negative control analysis in which urinary tract infection (N39) and hip fracture (S72) were tested as falsification endpoints. These endpoints were incorporated as outcome measures in the ATE analysis in which each frailty risk subgroup was PS-matched with respect to treatment type. A two-tailed P-value <.05 was considered statistically significant in all analyses.
Results
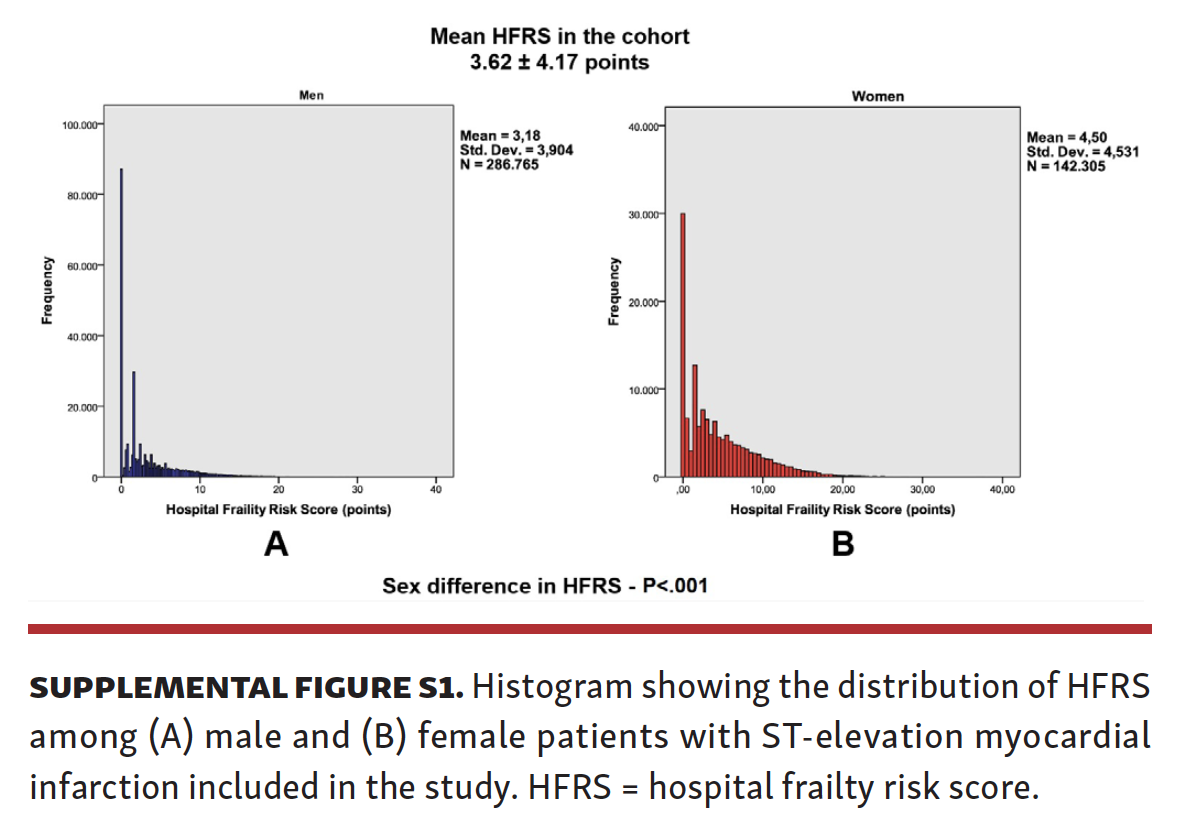
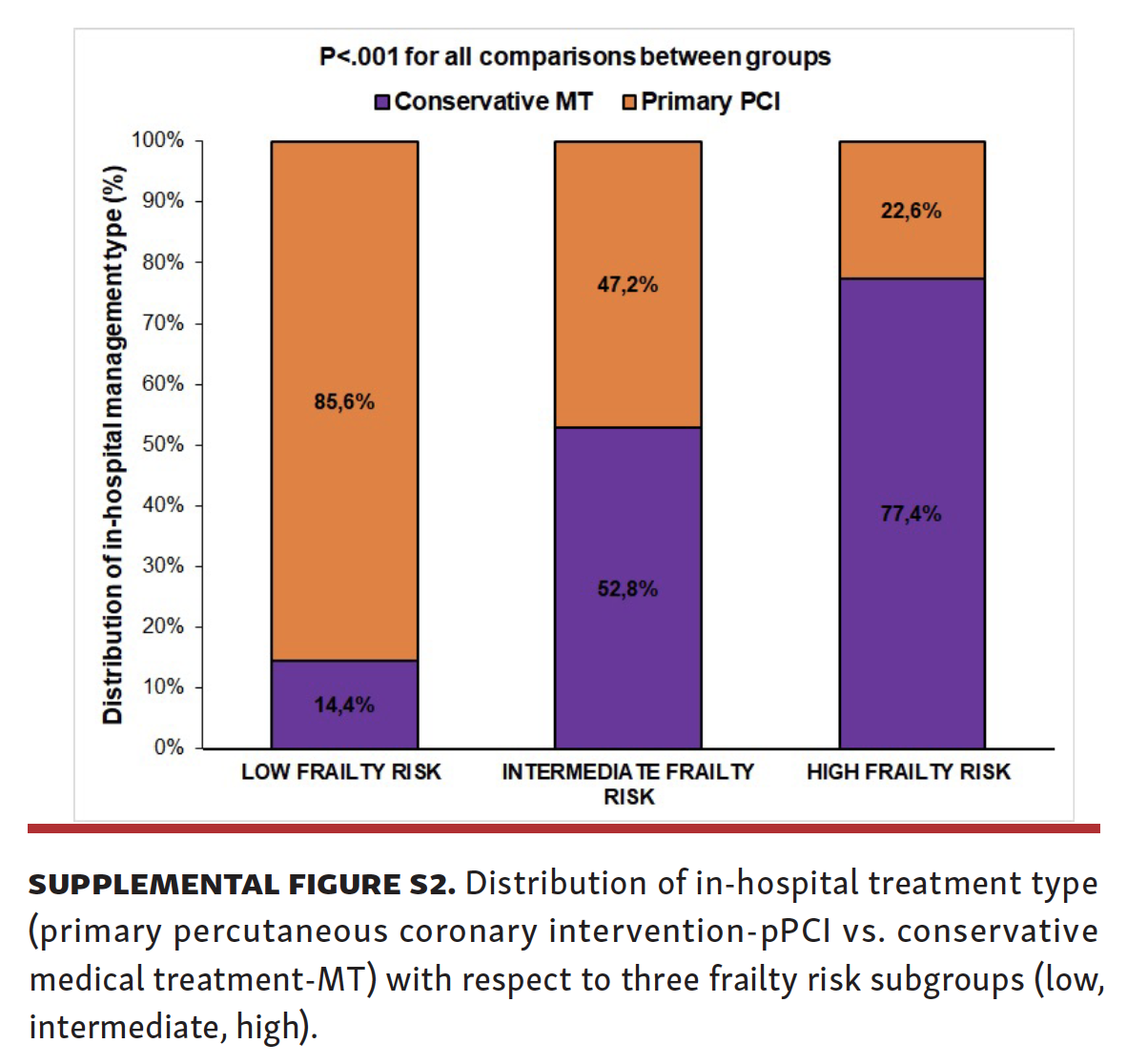
Baseline data of the whole patient cohort. A total of 500,225 weighted records were identified in the dataset and after applying exclusion criteria, a total of 429,070 patients with a primary in-hospital diagnosis of STEMI between 2015-2017 were included in the analysis. Missing records (weighted) comprised 0.12% of the full dataset while the total of 14.3% cases (weighted records) of initial dataset were not included in the final analysis due to exclusion criteria (Figure 1). The mean age of the STEMI cohort was 64.6 ± 13.7 years, about two-thirds (n = 286,765; 66.8%) were male, and the majority were White. Nearly three-quarters (74.2%) of patients received pPCI whereas 25.8% of the cohort were managed with conservative medical treatment. As shown in Supplemental Figure S1, the mean HFRS in the entire cohort was 3.6 ± 4.2 points with women having a significantly higher HFRS than men (4.5 ± 4.5 vs 3.2 ± 3.9 points, P<.001, respectively). The vast majority of patients (71.6%) were classified as low frailty risk (HFRS <5 points), 113,050 (26.3%) were designated as having an intermediate frailty risk (HFRS 5-15 points) while only 2.1% of patients (N=8,995) were at a high risk of frailty (HFRS >15 points). The rates of pPCI utilization significantly decreased with increasing frailty risk whereas the rates of conservative MT were significantly higher in patients with increased frailty risk (52.8% and 77.4% in the intermediate and high frailty risk groups vs 14.4% in the low frailty risk group, P<.001; Supplemental Figure S2).
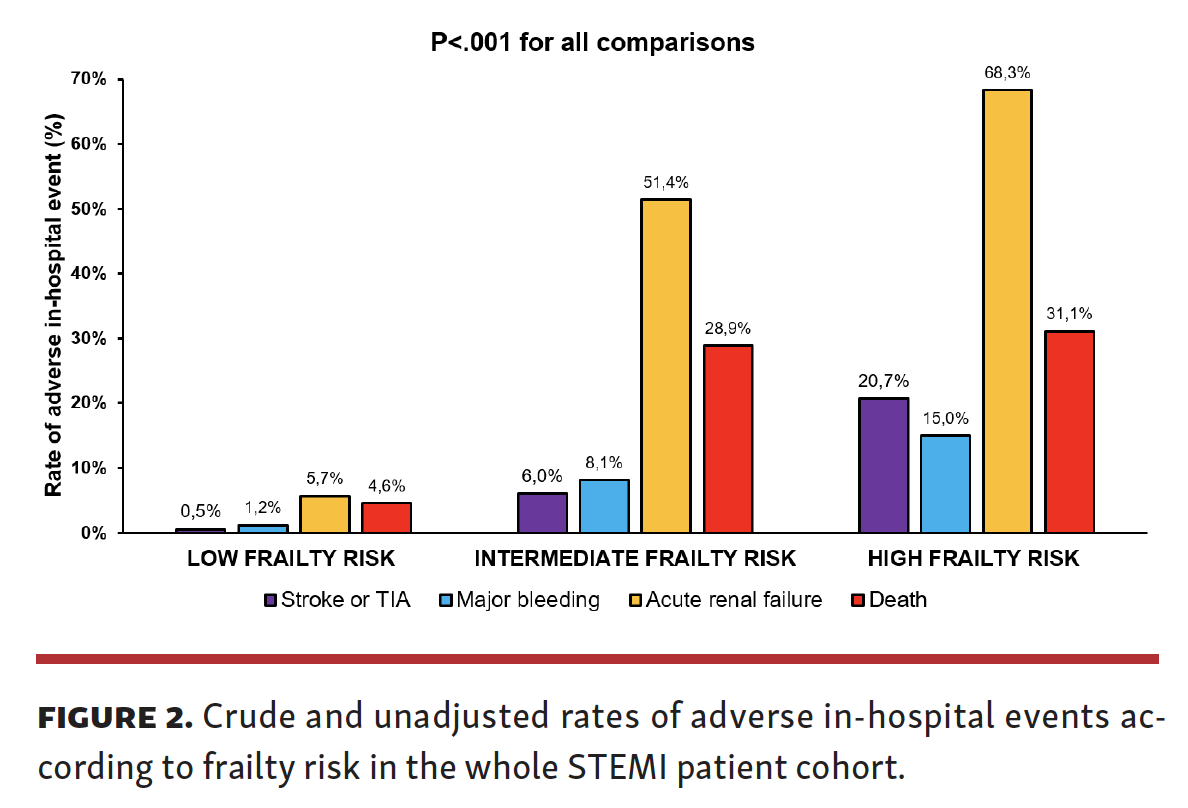
Crude (unadjusted) rates of adverse in-hospital outcomes consisting of acute stroke/TIA, major bleeding, acute renal failure, and all-cause death were significantly more prevalent among STEMI patients with an increased frailty risk compared with those with a low risk of frailty. Of note, rates of acute stroke/TIA were 0.5%, 6.0%, and 20.7% among patients with low, intermediate, and high frailty risk, respectively. Similar trends were observed with respect to outcomes of major bleeding (1.2%, 8.1%, and 15.0%), acute renal failure (5.7%, 51.4%, 68.3%), and in-hospital death (4.6%, 28.9%, and 31.1%) among low, intermediate, and high frailty risk respectively. All outcome comparisons across three frailty risk groups were significant at P<.001 (Figure 2).
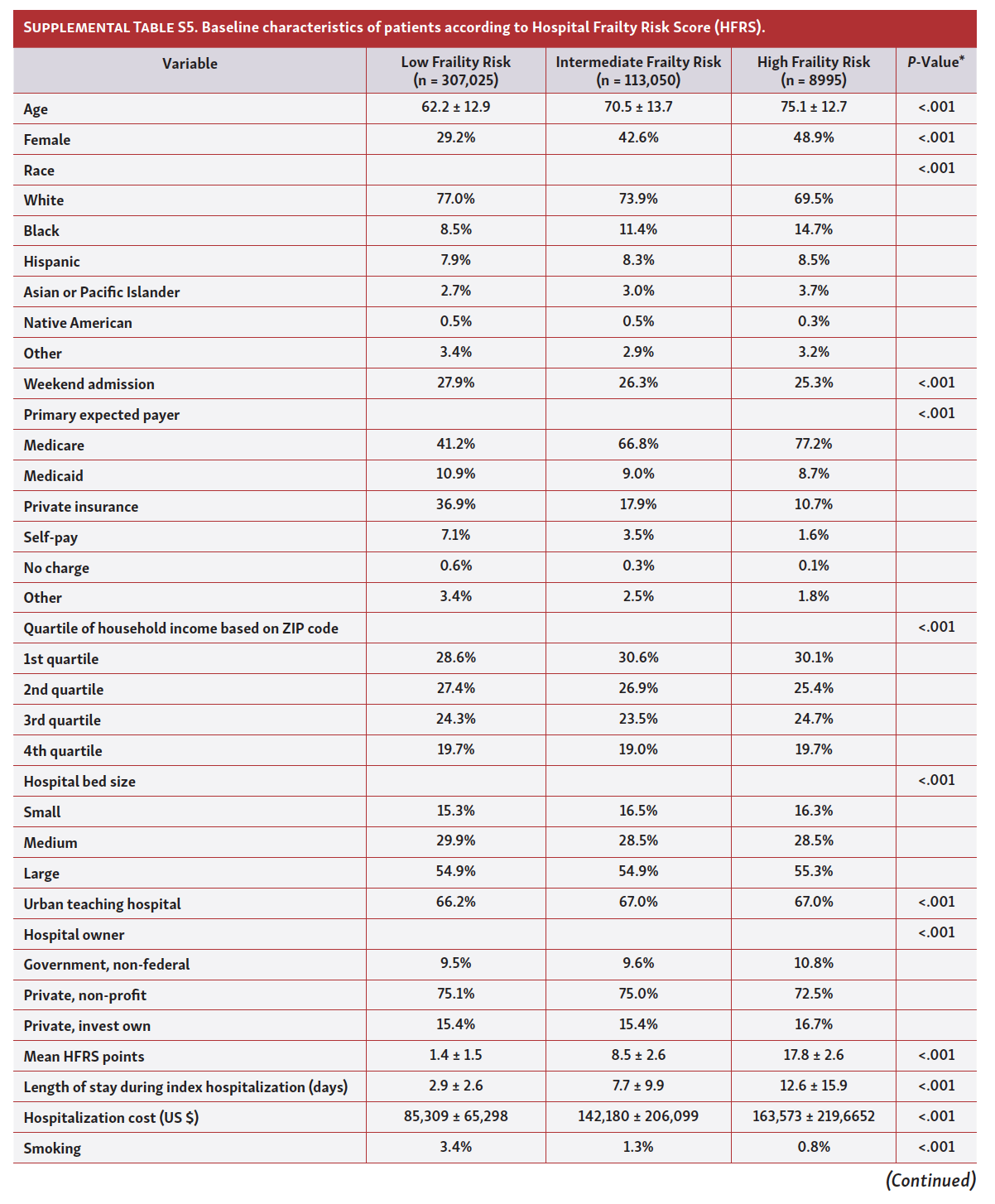
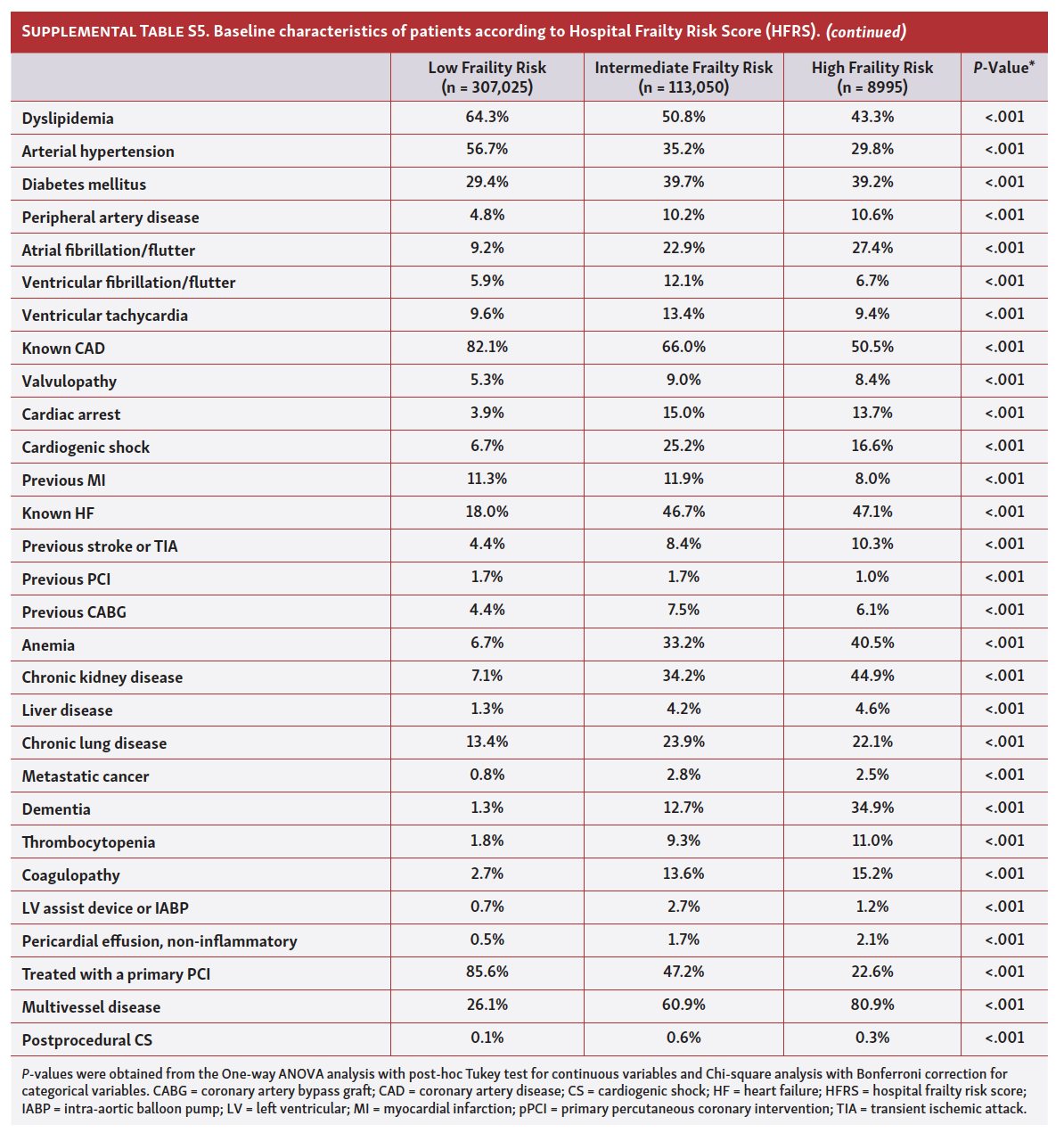
Furthermore, as shown in Supplemental Table S5 (Part 1, Part 2), patients with STEMI at increased risk of frailty (ie, belonging to intermediate and high frailty risk subgroups) tended to be older, women, and less likely to be admitted on weekends. Similarly, these patients were more likely to experience a significantly longer LoS and higher hospitalization costs during their index hospitalization. In terms of comorbidities, patients at an increased frailty risk were less likely to smoke, had a lower prevalence of arterial hypertension, dyslipidemia, and known CAD, however, were more likely to have diabetes mellitus, peripheral artery disease, atrial fibrillation, anemia, chronic renal failure, and valvular heart disease. Finally, STEMI patients with an increased frailty risk were more likely to have a multivessel disease and to experience cardiogenic shock and cardiac arrest during the index hospitalization.
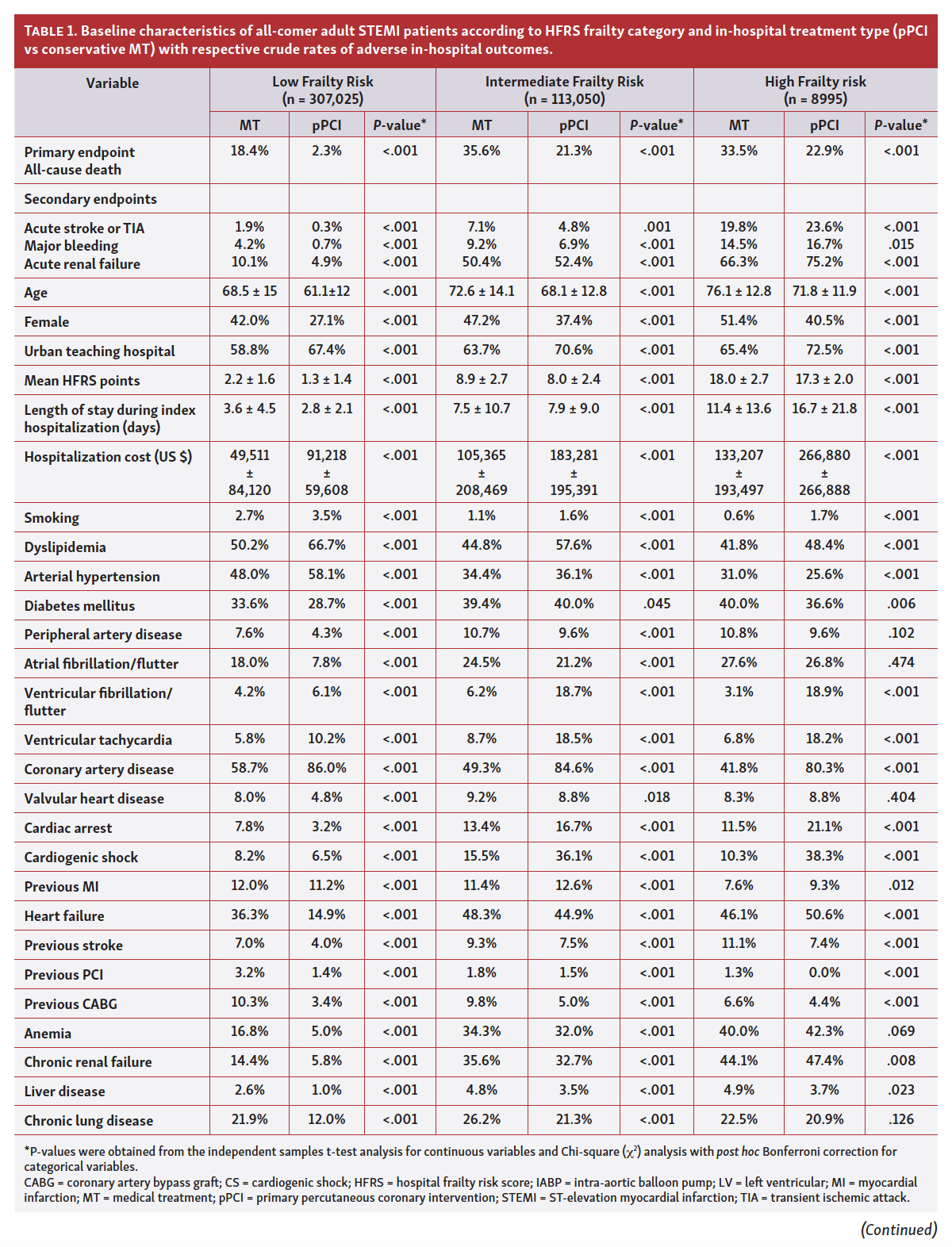
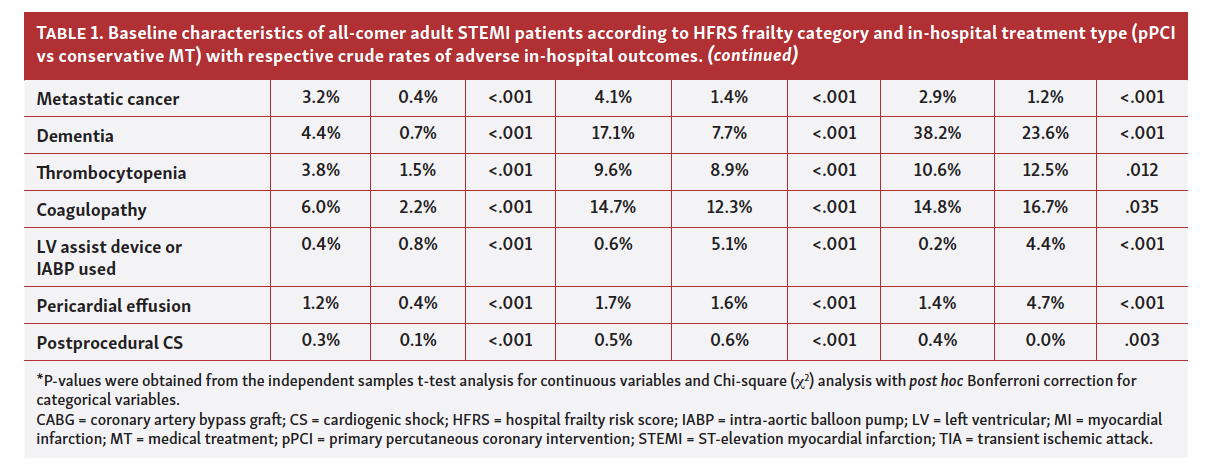
Patient characteristics and crude rates of adverse in-hospital outcomes with respect to treatment type. The crude rates of adverse in hospital-outcomes and baseline characteristics with respect to treatment type (pPCI vs MT) across frailty risk subgroups are shown in Table 1 (Part 1, Part 2). Generally, patients that received pPCI in each frailty subgroup were younger, more commonly men and smokers with lower prevalence of comorbidities such as diabetes mellitus, atrial fibrillation, and peripheral artery disease. However, patients that underwent pPCI were more likely to have dyslipidemia, arterial hypertension, and previously known CAD. Furthermore, the crude rates of adverse in hospital-outcomes consisting of all-cause death, acute stroke or TIA, and major bleeding were significantly lower among STEMI patients treated with pPCI compared with MT in the low and intermediate frailty risk groups. More specifically, in the high frailty risk subgroup, patients treated with pPCI experienced significantly less in-hospital death compared with patients receiving MT (22.9% vs 33.5%) while there was a higher prevalence of acute stroke/TIA and major bleeding in the pPCI group compared with patients managed with MT (23.6% vs 19.8% and 16.7% vs 14.5%, respectively). In terms of acute renal failure events, patients with low frailty risk experienced significantly fewer of these events when treated with pPCI compared to MT (4.9% vs 10.1%), however, in intermediate and high frailty risk groups, patients treated with pPCI experienced significantly more acute renal failure events.
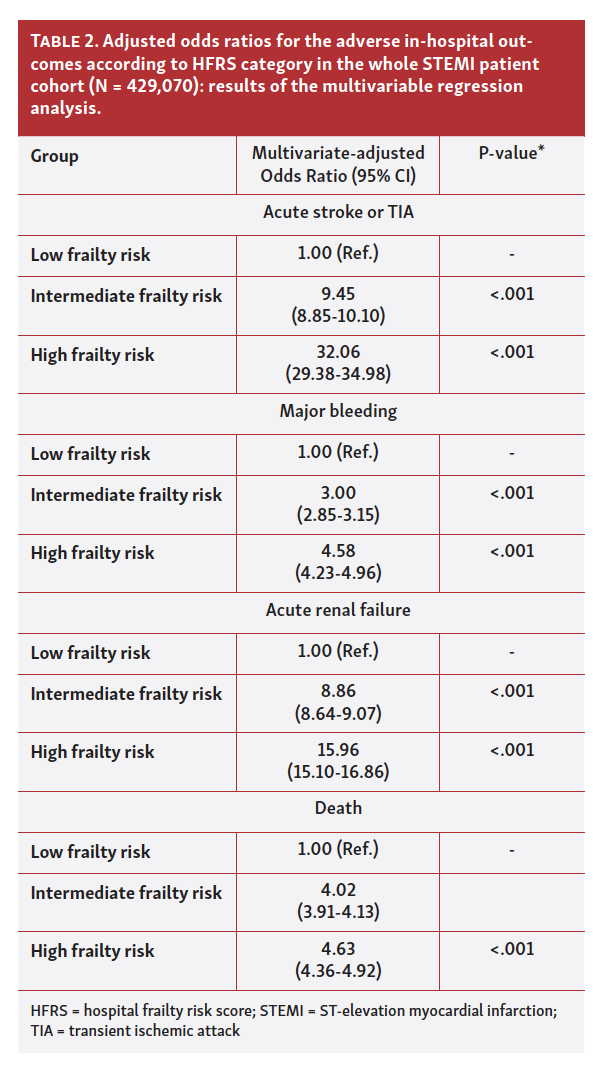
Frailty risk categories and odds of adverse in-hospital outcomes. A multivariable logistic regression analysis adjusted for a number of relevant covariates and in-hospital treatment types in the model, showed that STEMI patients in the intermediate and high frailty risk categories had a significantly higher likelihood of sustaining an adverse in-hospital event, compared with patients with low frailty risk (Table 2). Specifically, compared with low frailty risk category, patients at intermediate and high frailty risk had more than 4-fold increases in the odds of in-hospital death (OR 4.02, 95% CI 3.91-4.13 and OR 4.63, 95% CI 4.36-4.92), with observations recorded for acute stroke or TIA (OR 9.45, 95% CI 8.85-10.10 and OR 32.06, 95% CI 29.38-34.98), major bleeding (OR 3.00, 95% CI 2.85-3.15 and OR 4.58, 95% CI 4.23-4.96), and acute renal failure (OR 8.86, 95% CI 8.64-9.07 and OR 15.96, 95% CI 15.01-17.32).
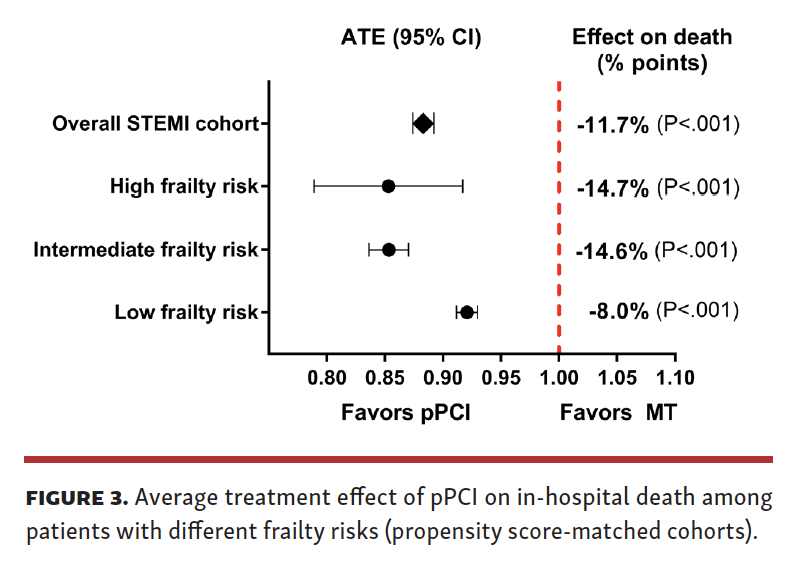
Average treatment effects of pPCI on in-hospital death and rates of adverse in-hospital events across propensity-score matched frailty subgroups. The propensity score matched ATE analysis showed that pPCI was associated with a significant and consistent reduction of in-hospital all-cause death across all frailty subgroups in the setting of STEMI, compared with MT (P<.001 for all comparisons). Of note, across the whole STEMI cohort, pPCI provided ATE of -0.117 (95% CI -0.126 to -0.108, z= -25.59) compared to MT. Among patients with low frailty risk ATE of pPCI was -0.080 (95% CI -0.088 to 0.070, z= -17.52) while among those with intermediate frailty risk ATE of pPCI was -0.146 (95% CI -0.164 to -0.130, z= -16.67). Finally, in STEMI patients with high frailty risk, pPCI was associated with ATE of -0.147 (95% CI -0.211 to -0.083, z= -4.52).
As shown in Figure 3, benefit of pPCI in reduction of in-hospital all-cause death was higher among STEMI patients at increased risk of frailty (intermediate and high-risk groups) compared with low frailty risk group. There was no significant difference in estimated ATE coefficients for pPCI between three frailty risk subgroups (P=.121) showing that the effect of pPCI in high frailty STEMI patients was at least equal to the effect of pPCI in STEMI patients at low frailty risk. More specifically, low frailty risk ATE of pPCI did not significantly differ compared to ATE of pPCI in the intermediate frailty risk subgroup (P=.162) and this was also true when a comparison was made between low and high frailty risk subgroups (P=.160). Likewise, ATE values for pPCI between intermediate and high frailty risk subgroups did not differ significantly (P=.997).
The ATE analysis incorporating hip fracture and urinary tract infection as falsification endpoints among PS-matched frailty risk subgroups showed that there was no significant difference between pPCI and MT with respect to average treatment effect concerning both endpoints (Table 3).
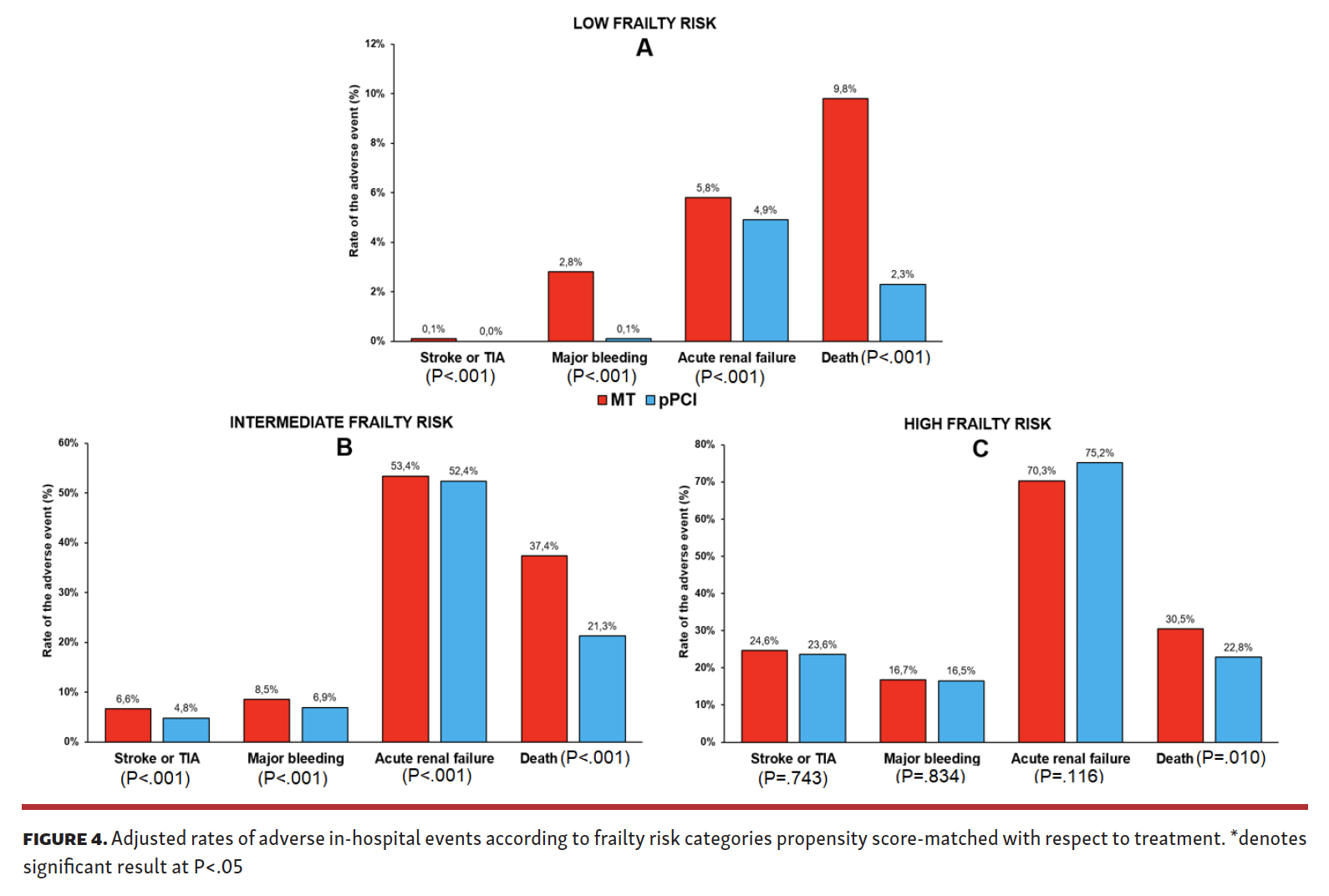
Furthermore, after propensity score matching, patients in the pPCI group had significantly lower rates of stroke or TIA, major bleeding, acute renal failure, and all-cause death, compared to MT, among patients with low frailty risk (Figure 4A; P<.001 for all comparisons). Similarly, pPCI was associated with significantly lower rates of stroke or TIA, major bleeding, and all-cause death, compared to MT, among patients with intermediate frailty risk (P<.001 for those comparisons), while there was no significant difference between two treatment types in terms of acute renal failure events (Figure 4B). Among patients with high frailty risk, pPCI was associated with significantly lower rates of all-cause death compared to MT (22.8% vs 30.5%, P=.010) while no significant differences were observed between two treatment types with respect to stroke or TIA, major bleeding, and acute renal failure (Figure 4C).
Discussion
To our best knowledge, this is the first large nationwide registry analysis that examined the treatment effect of pPCI in a contemporary cohort of STEMI patients across the continuum of frailty risk.
This study reports several important findings. First, the intermediate and high frailty risk patients presenting with STEMI are less likely to receive pPCI than patients deemed to have a low frailty risk. Secondly, patients with increased frailty risk have significantly higher rates of adverse in-hospital events including all-cause death, acute stroke/TIA, acute renal failure, and major bleeding. Finally, pPCI was consistently associated with significantly lower rates of death in all crude (unadjusted) and PSM-adjusted analyses, regardless of the frailty risk. Importantly, the treatment effect of pPCI was not significantly different amongst the different frailty groups. Taken together, our results suggest a substantial survival benefit associated with invasive rather than conservative medical management in frail STEMI patients, however, this is based on observational data and further studies are required to evaluate the long-term efficacy and safety of such approach in these delicate patients.
There are limited data in the literature regarding the optimal treatment approach of patients with STEMI who are frail and present with significant multimorbidites. This is a particularly challenging patient population that is prone to poor clinical outcomes when presenting with ACS,15,16 and are largely excluded from large randomized clinical trials informing our daily practice. Consequently, such data may contribute to biases towards these patients, who are often not referred for invasive management and are treated conservatively instead. A previous study examining a national cohort of US patients showed that the prevalence of frail patients among those undergoing PCI significantly increased over the 10 years while high frailty risk was associated with prolonged hospital stay and increased likelihood of mortality, bleeding, and vascular injury.17 Similar studies conducted among patients with ACS showed that the proportion of patients treated with PCI was lowest among patients with the highest frailty risk while frail patients were significantly less likely to receive guideline-directed care for ACS despite having significantly worse outcomes while in hospital.7,16
Current European Society of Cardiology (ESC) and American College of Cardiology Foundation (ACCF) / American Heart Association (AHA) guidelines for STEMI management advocate pPCI in patients with ischemia of ≤12 hours duration and persistent ST-segment elevation as a class I recommendation, level of evidence A.18-20 In current ESC and US STEMI guidelines [including focused ACC/AHA/ Society of Coronary Angiography and Intervention (SCAI) update], frailty is mentioned only once, with the recommendation that elderly patients should be treated as recommended (meaning pPCI), emphasizing bleeding risk-reducing strategies such as radial access use, proper dosing of antithrombotic regimens, and taking renal function, frailty and comorbidities into account.18 It is important to acknowledge that while frailty and aging are closely related, they should not be conflated since younger patients with chronic diseases such as cancer, liver failure, or renal failure can be frail as well and these phenomena are often poorly distinguished in the literature.
It is unclear why frail and old patients tend to have pPCI underutilized in the setting of STEMI especially if withholding this highly recommended mode of revascularization would likely precipitate poorer clinical outcomes. Earlier data from the Tratamiento del Infarto Agudo de miocardio eN Ancianos (TRIANA) trial and pooled analysis of previous studies showed that there should be no upper age limit regarding the reperfusion with pPCI in the setting of STEMI.21 Data from the National Cardiovascular Data Registry (NCDR) in the US showed that it was the oldest age group (≥80 years) that gained the largest absolute reduction for in-hospital mortality among patients that received PCI.22 However, it should be noted that this study enrolled only 13.4% of patients with STEMI, while the majority of patients had other types of ACS or were referred to angiography for other causes such as decompensated HF and cardiogenic shock. This notion is in line with earlier studies demonstrating the greatest benefit with surgical or percutaneous revascularization among elderly patients with CAD, compared with medical treatment alone and younger age groups.9,10 On the other hand, analysis from the BLITZ survey included an unselected pool of patients older than 75 years presenting with STEMI and evaluated the 30-day rates of major adverse cardiovascular events (MACE) relative to different treatment strategies.11 This analysis showed that 57.1% of these patients did not receive any early reperfusion therapy and these patients presented with a higher incidence of MACE at 30 days. More recent observations from the Cooperative National Registry of Acute Coronary care, Guideline Adherence, and Clinical Events (CONCORDANCE) registry confirmed that frail STEMI patients received 30% less reperfusion and 22% less revascularization during index hospitalizations compared to non-frail patients.23 In this analysis, frailty was associated with increased post-discharge all-cause but not cardiac-specific mortality thus stressing the need to address competing risks for mortality in this group of patients.
Elderly and frail patients often have advanced CAD characterized by high risk plaque morphology (increased incidence of thin-cap fibroatheroma), highly calcified, tortuous, ostial or bifurcation lesions, multivessel disease, and left main stenosis.24-26 These patients are often comorbid,27 cachectic,28 prone to bleeding complications,29 and more susceptible to adverse drug-drug interactions due to polypharmacy.30 In such a population, several non-cardiac comorbidities compete with CV disease for all-cause mortality. This may explain why despite having a high-risk CV disease profile, these patients tend to be treated less aggressively thereby creating a significant gap between clinical practice and interventional guidelines, thus contributing to a “treatment-risk” paradox.16,31 Furthermore, patients' or their legal guardians' personal wishes are an important component of shared decision-making in “real world” practice and it is possible that some patients might have declined an invasive procedure, some might have been discharged with palliative care at home or consented to other goals of care, while some of the interventions might have not been performed at the operator's discretion due to physician’s selection bias. Likely, such factors and other unmeasured parameters that are not captured by the hospital administrative and coding system might significantly impact the utilization of pPCI thus prompting other treatment choices in this patient population.
Study limitations. There are several limitations to this study. Due to the retrospective and non-randomized design of the study, it is impossible to ascertain direct causality between pPCI and outcomes of interest. As with any large-scale nationwide database, there is an inherent possibility of underreporting bias and coding errors within the NIS dataset, and it should be noted that in this analysis we did not account for hospital-level clustering effects. NIS does not provide data on periprocedural medications and in-hospital pharmacotherapy as well as data on continuous variables such as body mass index or laboratory values that might aid in prediction of bleeding and ischemic risks. Importantly, one of the main weaknesses of our analysis is the inability to account for goals of care and palliative care intentions as well as to account for unmeasured parameters in our PSM analysis that might drive clinical judgment (physician selection bias) when it comes to a decision to perform pPCI among STEMI patients at increased risk of frailty. We have attempted to assess for the significant presence of unmeasured confounders or selection bias through the inclusion of falsification endpoints of UTI and hip fracture, in which PPCI would not be expected to have an impact. Our analysis shows that receipt of PPCI was associated with improved mortality outcomes across all strata of frailty, but had no impact on the falsification endpoints, suggesting that it was unlikely that unmeasured confounders/selection biases were driving the mortality endpoint results, although we cannot rule this out fully.
Another important limitation of the study was around the definition of frailty that was based on the administrative hospital health record score that might not fully correlate with clinical frailty. However, the HFRS has been robustly validated for frailty risk assessment and prognosis. Finally, it is important to note that this study focused on the impact of pPCI on in-hospital outcomes, although it is not clear if this benefit would extend during the later period since the relationship of frailty and mortality appears to be strongly modified by competing non-CV risks.
Conclusion
Our study showed that STEMI patients at an increased frailty risk have a high-risk CV profile but are significantly undertreated with invasive management. pPCI provided consistent mortality benefit in frail STEMI patients to a similar degree as in patients at low risk of frailty. Whether these group level outcomes reflect treatment benefit or clinical judgement or both in real-life clinical practice remains uncertain. The presented findings based on observational data suggest that pPCI should be implemented by careful examination of patients’ comorbidities, precision balancing of bleeding/ischemic risk, and patient’s personal or caregiver’s wishes in the concept of shared decision-making. Furthermore, it is likely that the innovations in antithrombotic drugs, the use of the latest DES platforms and radial access would make pPCI in this population even safer than what historic data show. Due to the evidence gap in this setting, further prospective trials are required to ascertain the long-term efficacy and safety of invasive versus conservative medical management in the setting of STEMI for frail patients or those at increased risk of frailty.
Affiliations and Disclosures
From the 1Keele Cardiovascular Research Group, Centre for Prognosis Research, Institutes of Applied Clinical Science and Primary Care and Health Sciences, Keele University, Stoke-on-Trent, United Kingdom; 2Department of Pathophysiology, University of Split School of Medicine, Split, Croatia; 3Clinic for Cardiovascular Diseases, University Hospital of Split, Split, Croatia; 4Department of Health Studies, University of Split, Split, Croatia; 5Division of Informatics, Imaging and Data Sciences, University of Manchester, Manchester, United Kingdom; 6Department of Cardiology, Mayo Clinic, Rochester, Minnesota; 7Cardiology Department, Wayne State University, Detroit Medical Center, Detroit Heart Hospital, Detroit, Michigan; 8Division of Cardiology, University of Washington, Seattle, Washington; 9Division of Cardiology, Weill Cornell Medicine-Qatar, Doha, Qatar; 10Division of Cardiology, University of Nebraska Medical Center, Omaha, Nebraska; 11Division of Cardiovascular Medicine, East Tennessee State University, Johnson City, Tennessee; and 12Division of Cardiology, Department of Medicine, Population Health Research Institute, ICES, McMaster University, Hamilton, Ontario, Canada.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no financial relationships or conflicts of interest regarding the content herein.
Manuscript accepted March 22, 2021.
Address for correspondence: Mamas A. Mamas, BMBCh, DPhil, MRCP, Professor of Cardiology, Keele Cardiovascular Research Group, Centre for Prognosis Research, Institute for Primary Care and Health Sciences, Keele University, United Kingdom. Email: mamasmamas1@yahoo.co.uk
Appendices 1-3
Frailty among patients with acute ST-elevation myocardial infarction in the United States: the impact of a primary percutaneous coronary intervention on in-hospital outcomes.
Propensity score matching methodology and balance diagnostics
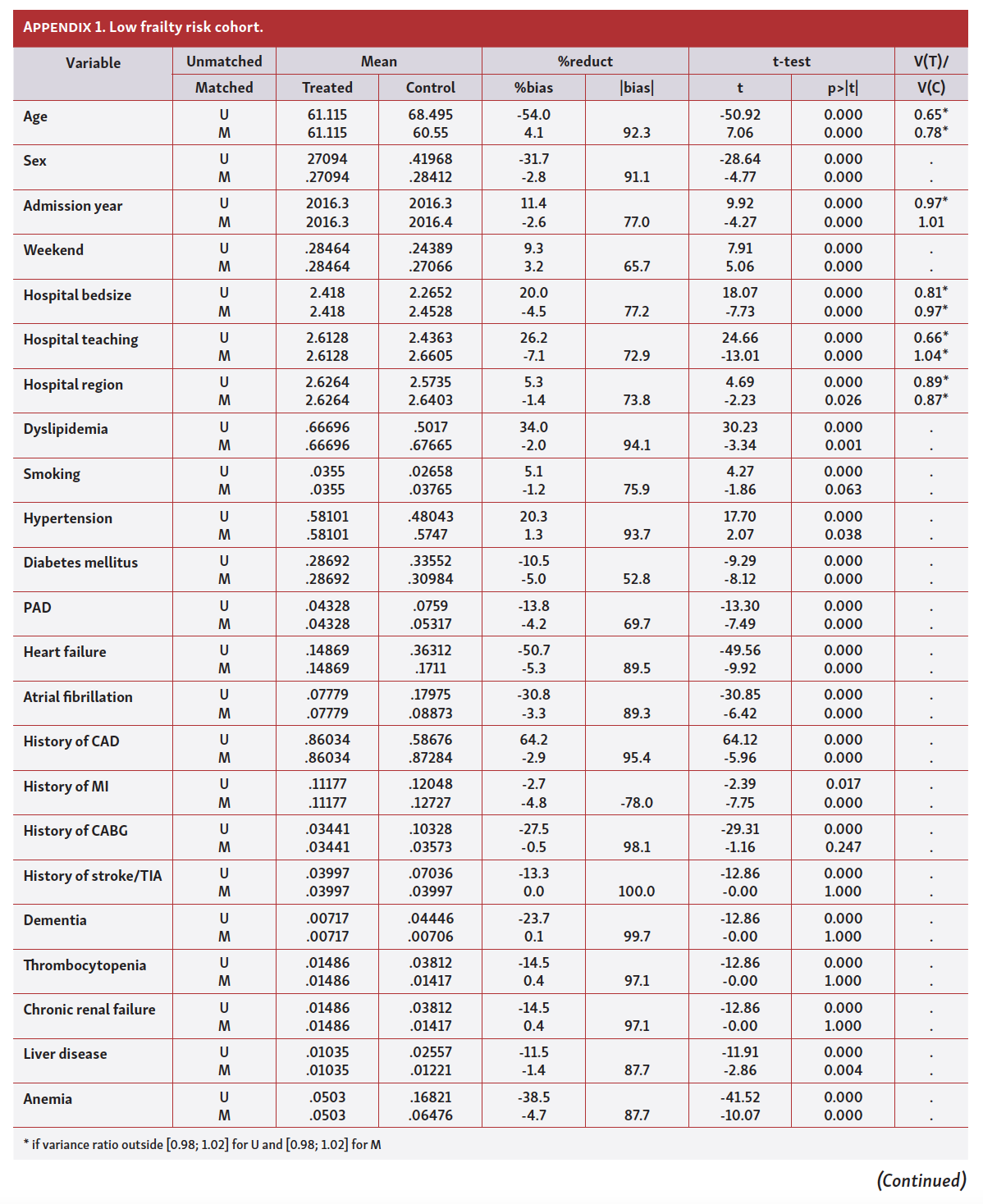
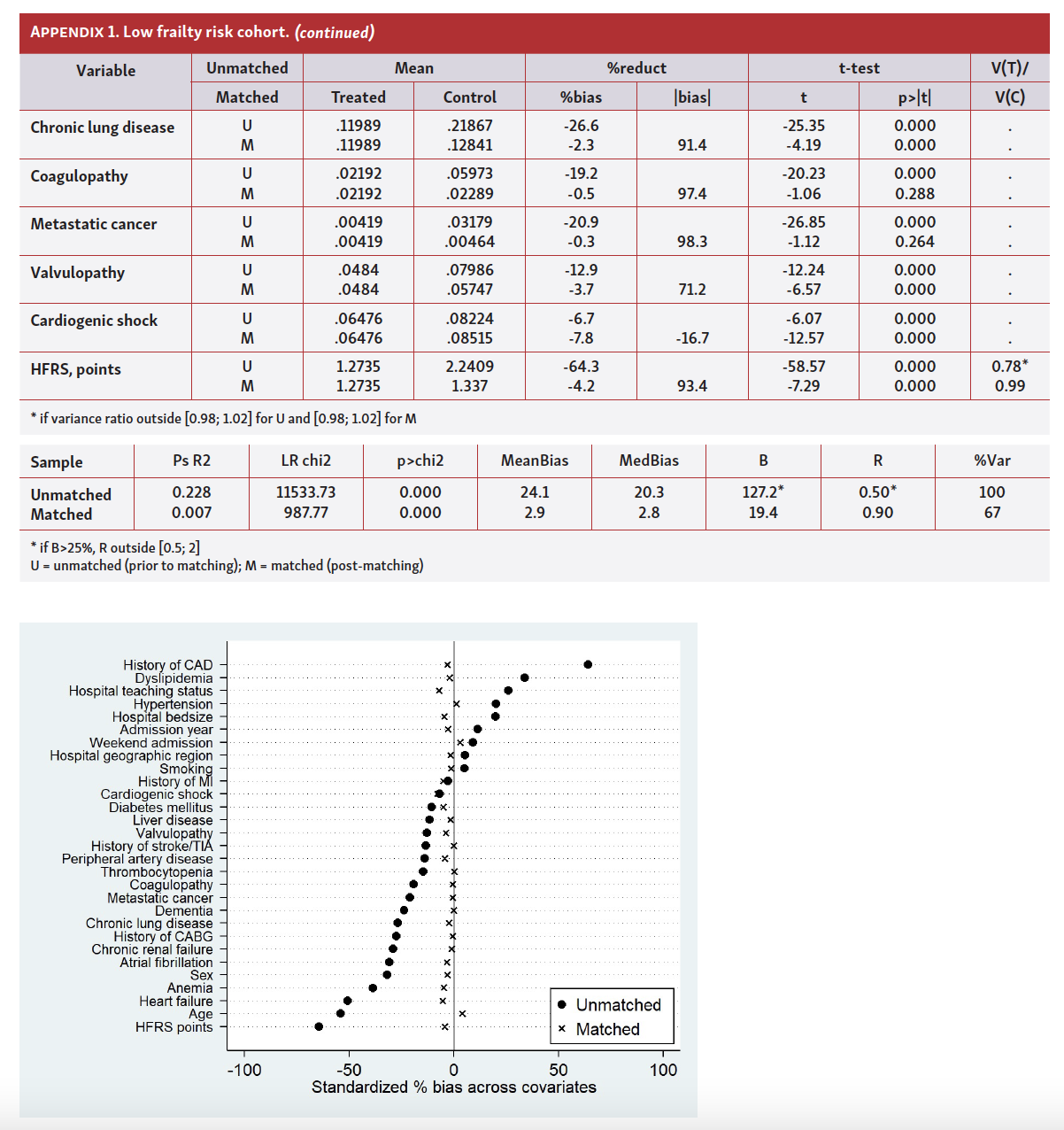
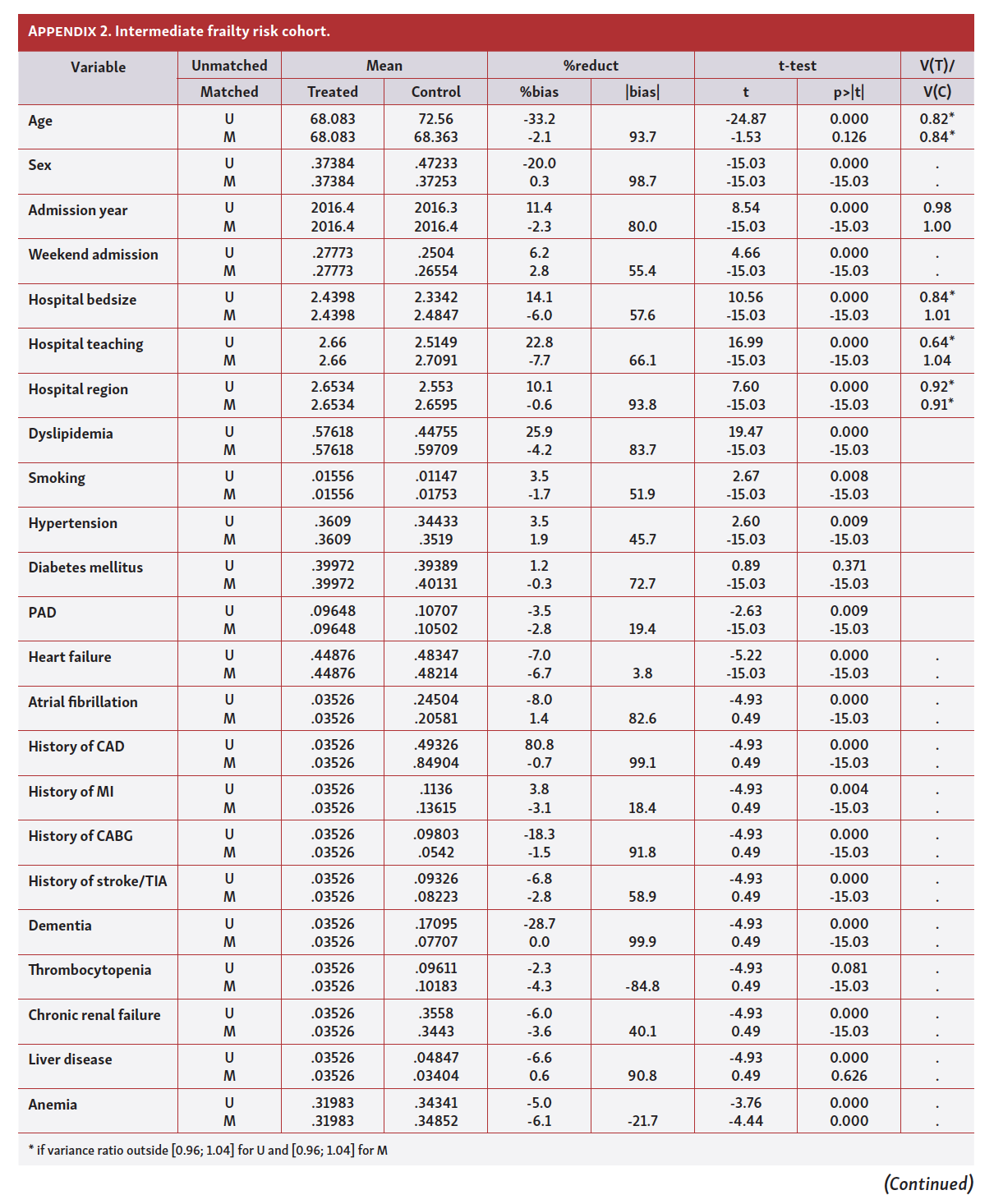
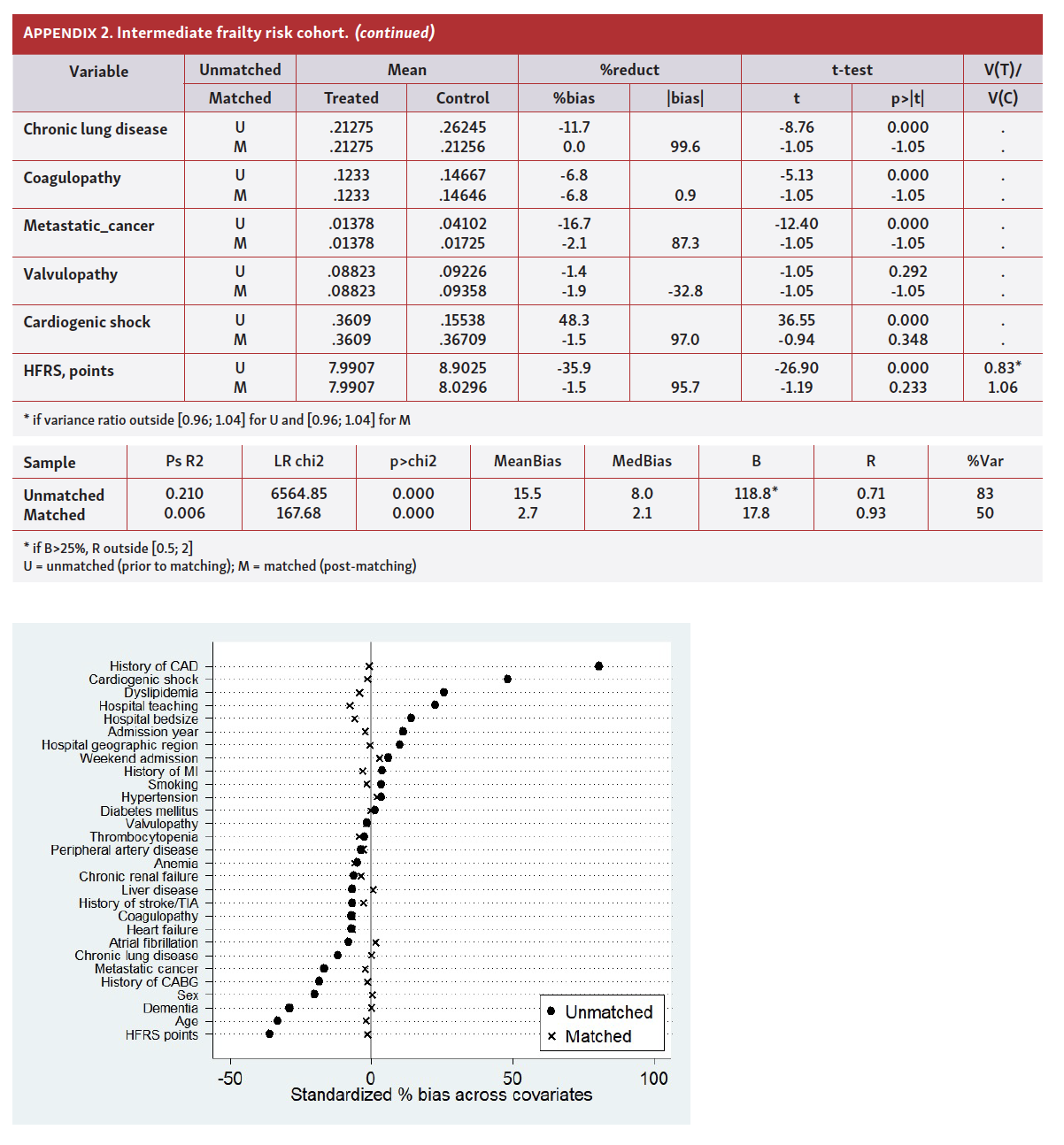
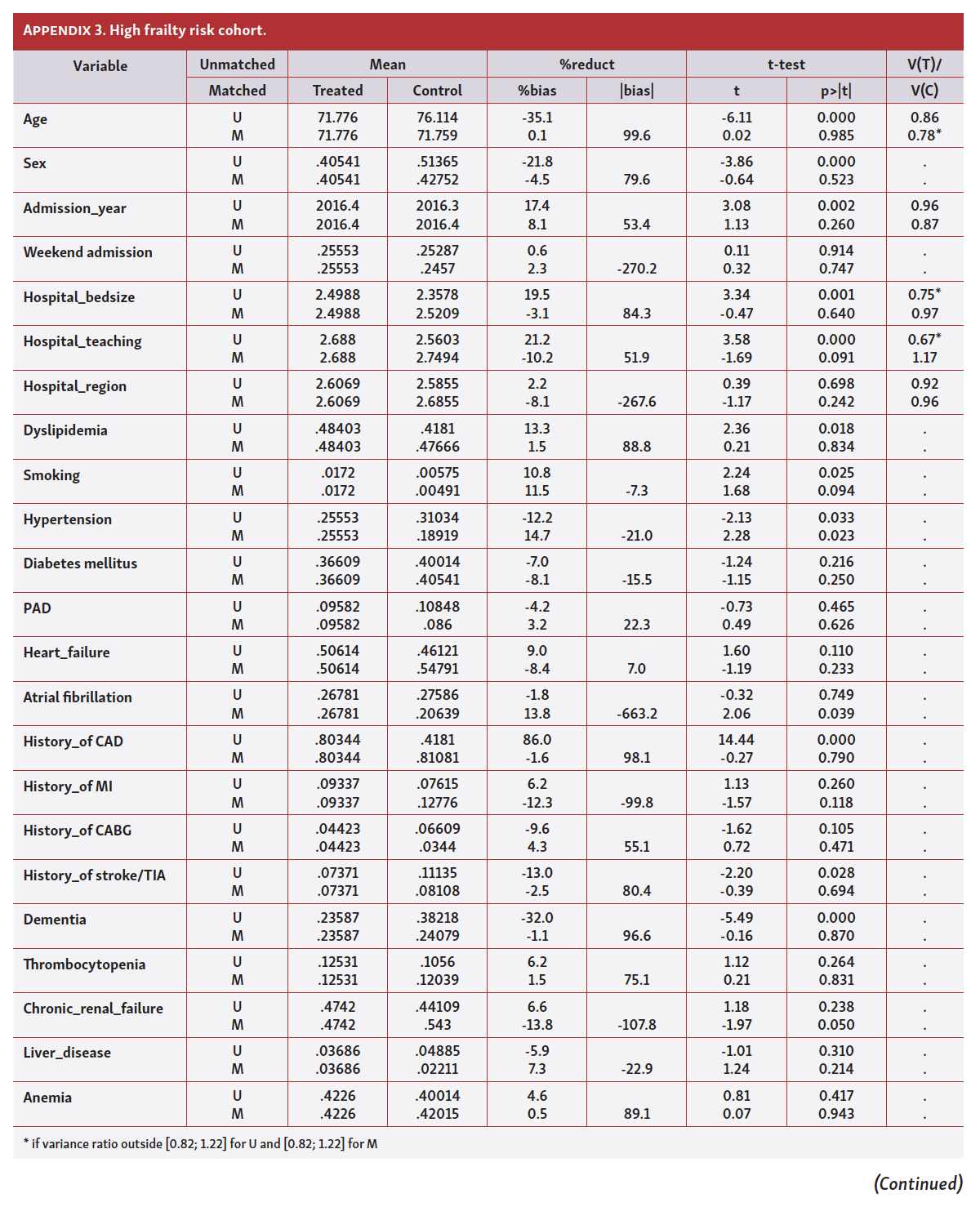
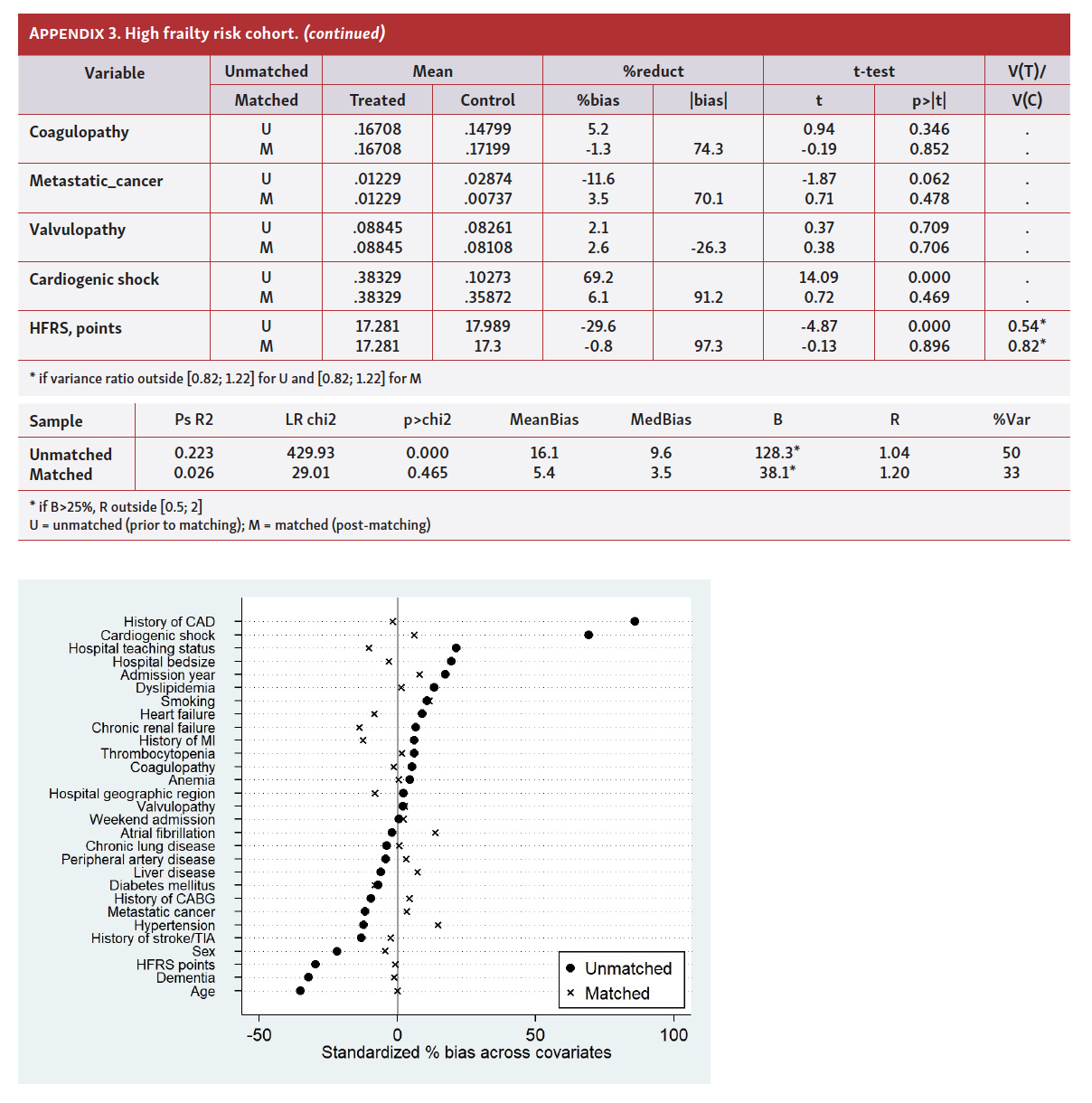
For the average treatment effects (ATE) analysis of pPCI on the outcome of in-hospital all-cause death teffects psmatch command in the Stata was used. In order to balance treatment groups (pPCI vs MT) for baseline clinical and sociodemographic covariates, the nearest neighbor logit matching algorithm was used. In each frailty risk category (low, intermediate, high), both treatment groups were PSM-balanced for the covariates that were selected a priori and included: age, sex, calendar year, weekend admission, hospital bedsize (small, medium, large), hospital teaching status (rural, urban/teaching, urban/non-teaching), hospital geographic region (Northeast, Midwest or North Central, South, West), dyslipidemia, smoking, arterial hypertension, diabetes mellitus, peripheral artery disease, heart failure, history of coronary artery disease, atrial fibrillation, history of myocardial infarction, history of coronary artery bypass grafting, history of stroke/transient ischemic attack, dementia, thrombocytopenia, chronic renal failure, liver disease, anemia, chronic lung disease, coagulopathy, metastatic cancer, valvulopathy, cardiogenic shock, and HFRS points.
Quality of matching was assessed through balance diagnostics executed with pstest command showing the standardized mean difference between two treatment groups, percent (%) bias showing the difference between treatment and comparison group propensity scores while percent (%) bias reduction (PBR) was calculated by using equation PBR = [(biasbefore matching – biasafter matching)/biasbefore matching] x 100. Furthermore, t-test for the equality of means and variance ratios indicating variances of propensity scores between two treatment groups were also shown. Ideally, the variance ratio should be close to 1 meaning that variances of the propensity scores between the two groups are near equal. Tables showing covariate balances and graphs showing standardized % bias across covariates, prior to matching (unmatched-U) and post-matching (matched-M), are further shown in this document.
References
1. Singh M, Stewart R, White H. Importance of frailty in patients with cardiovascular disease. Eur Heart J. 2014;35:1726-1731.
2. Afilalo J, Karunananthan S, Eisenberg MJ, et al. Role of frailty in patients with cardiovascular disease. Am J Cardiol. 2009;103:1616-1621.
3. Lee DH, Buth KJ, Martin BJ, et al. Frail patients are at increased risk for mortality and prolonged institutional care after cardiac surgery. Circulation. 2010;121:973-978.
4. McNallan SM, Singh M, Chamberlain AM, et al. Frailty and healthcare utilization among patients with heart failure in the community. JACC Heart Fail. 2013;1:135-141.
5. Zhang Y, Yuan M, Gong M, et al. Frailty and clinical outcomes in heart failure: a systematic review and meta-analysis. J Am Med Dir Assoc. 2018;19:1003-1008.e1.
6. Murali-Krishnan R, Iqbal J, Rowe R, et al. Impact of frailty on outcomes after percutaneous coronary intervention: a prospective cohort study. Open Heart. 2015;2:e000294.
7. Kwok CS, Lundberg G, Al-Faleh H, et al. Relation of frailty to outcomes in patients with acute coronary syndromes. Am J Cardiol. 2019;124:1002-1011.
8. Damluji AA, Huang J, Bandeen-Roche K, et al. Frailty among older adults with acute myocardial infarction and outcomes from percutaneous coronary interventions. J Am Heart Assoc. 2019;8:e013686.
9. Graham MM, Ghali WA, Faris PD, et al. Survival after coronary revascularization in the elderly. Circulation. 2002;105:2378-2384.
10. TIME Investigators. Trial of invasive versus medical therapy in elderly patients with chronic symptomatic coronary-artery disease (TIME): a randomised trial. Lancet. 2001;358:951-957.
11. De Luca L, Bolognese L, Casella G, et al. Modalities of treatment and 30-day outcomes of unselected patients older than 75 years with acute ST-elevation myocardial infarction: data from the BLITZ study. J Cardiovasc Med (Hagerstown). 2008;9:1045-1051.
12. Khera R, Krumholz HM. With great power comes great responsibility: big data research from the national inpatient sample. Circ Cardiovasc Qual Outcomes. 2017;10:e003846.
13. Gilbert T, Neuburger J, Kraindler J, et al. Development and validation of a hospital frailty risk score focusing on older people in acute care settings using electronic hospital records: an observational study. Lancet. 2018;391:1775-1782.
14. Eckart A, Hauser SI, Haubitz S, et al. Validation of the hospital frailty risk score in a tertiary care hospital in Switzerland: results of a prospective, observational study. BMJ Open. 2019;9:e026923.
15. Dou Q, Wang W, Wang H, et al. Prognostic value of frailty in elderly patients with acute coronary syndrome: a systematic review and meta-analysis. BMC Geriatr. 2019;19:222.
16. Bebb O, Smith FG, Clegg A, et al. Frailty and acute coronary syndrome: a structured literature review. Eur Heart J Acute Cardiovasc Care. 2018;7:166-175.
17. Kwok CS, Achenbach S, Curzen N, et al. Relation of frailty to outcomes in percutaneous coronary intervention. Cardiovasc Revasc Med. 2020;21:811-818.
18. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39:119-177.
19. O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61:485-510.
20. Levine GN, Bates ER, Blankenship JC, et al. 2015 ACC/AHA/SCAI focused update on primary percutaneous coronary intervention for patients with ST-elevation myocardial infarction: an update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention and the 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction. J Am Coll Cardiol. 2016;67:1235-1250.
21. Bueno H, Betriu A, Heras M, et al. Primary angioplasty vs fibrinolysis in very old patients with acute myocardial infarction: TRIANA (TRatamiento del Infarto Agudo de miocardio eN Ancianos) randomized trial and pooled analysis with previous studies. Eur Heart J. 2011;32:51-60.
22. Singh M, Peterson ED, Roe MT, et al. Trends in the association between age and in-hospital mortality after percutaneous coronary intervention: national cardiovascular data registry experience. Circ Cardiovasc Interv. 2009;2:20-26.
23. Patel A, Goodman SG, Yan AT, et al. Frailty and outcomes after myocardial infarction: insights from the CONCORDANCE registry. J Am Heart Assoc. 2018;7:e009859.
24. Endo A, Kawamura A, Miyata H, et al. Angiographic lesion complexity score and in-hospital outcomes after percutaneous coronary intervention. PloS One. 2015;10:e0127217.
25. Mohamed MO, Polad J, Hildick-Smith D, et al. Impact of coronary lesion complexity in percutaneous coronary intervention: one-year outcomes from the large, multicentre e-Ultimaster registry. EuroIntervention. 2020;16:603-612.
26. Gu SZ, Qiu W, Batty JA, et al. Coronary artery lesion phenotype in frail older patients with non-ST-elevation acute coronary syndrome undergoing invasive care. EuroIntervention. 2019;15:e261-e268.
27. Al-Khadra Y, Kajy M, Idris A, et al. Comparison of outcomes after percutaneous coronary interventions in patients of eighty years and above compared with those less than 80 years. Am J Cardiol. 2019;124:1372-1379.
28. Bielecka-Dabrowa A, Ebner N, Dos Santos MR, et al. Cachexia, muscle wasting, and frailty in cardiovascular disease. Eur J Heart Fail. 2020;22:2314-2326.
29. Bainey KR, Welsh RC. Bleeding in STEMI with staged multivessel PCI: is it truly benign? EuroIntervention. 2016;12:1203-1205.
30. Serbin MA, Guzauskas GF, Veenstra DL. Clopidogrel-proton pump inhibitor drug-drug interaction and risk of adverse clinical outcomes among PCI-treated ACS patients: a meta-analysis. J Manag Care Spec Pharm. 2016;22:939-947.
31. Shanmugasundaram M. Percutaneous coronary intervention in elderly patients: is it beneficial? Tex Heart Inst J. 2011;38:398-403.










