

Improving Patient Outcomes with a Mobile Digital Health Platform for Patients Undergoing Transcatheter Aortic Valve Replacement
Abstract
Purpose: ManageMySurgery (MMS) is a digital health application (app) for patients undergoing surgery, including Transcatheter Aortic Valve Replacement (TAVR). Patients using MMS review procedure-specific education, view FAQs, and report patient-reported outcomes. This study assessed the impact of app use on postoperative outcomes.
Methods: Patients who underwent TAVR and invited to use MMS between March 2019 and November 2021 were identified. Patients received standard perioperative care and were defined as App users if they signed into the app at least once and engaged with at least one task or FAQ. Demographics and postoperative outcomes were collected via medical record review. Multivariable logistic regression models were used to determine odds of 90-day readmission, Emergency Room (ER) visits, and complications.
Results: 388 patients met inclusion criteria, of which 238 used the app. The average age at surgery was 76.4±7.7 years for users and 78.1±7.6 for non-users. 63.0% of users and 59.3% of non-users were male. App users had significantly lower 90-day readmission rates, (8.8% vs 16.0%, OR=0.51, p=0.0373), ER visit rates (12.6% vs 27.3%, OR=0.36, p=0.0003), and complication rates (Minor: 12.2% vs 20.7%, OR=0.48, P=0.0126; Major: 8.8% vs. 16%, OR=0.47, P=0.0235).
Conclusions: In this non-randomized, retrospective study, we found significant decreases in 90-day readmissions, ER visits, and complications in TAVR patients using an app compared to traditional care. By engaging patients throughout their interventional journey with structured education and tasks, mobile health platforms may mitigate unnecessary use of emergency and inpatient care, thereby improving patient well-being and lowering the burden on healthcare resources.
Introduction
Aortic stenosis (AS) is estimated to affect up to 10% of the population over the age 80.1 AS was traditionally treated via surgical aortic valve replacement (SAVR) but has increasingly been treated by the less invasive transcatheter aortic valve replacement (TAVR). Multiple clinical trials, including the PARTNER, CoreValve, and NOTION trials,1,2 have shown that TAVR produces similar clinical outcomes to SAVR while resulting in equivalent or lower risk of mortality, as well as allowing for valve replacement in extreme-risk surgical patients.
Given the common diagnosis and elderly population affected by AS, there exists a need to provide easy access to education for patients undergoing aortic valve replacements. In recent years, the ubiquity of smartphones has led to an explosion of digital health technology which aims to engage patients through mobile applications. These apps facilitate patient education, collect patient data, and allow for easier communication between patients and providers. Evidence has shown the efficacy of digital health tools in improving outcomes for chronic conditions such as diabetes and chronic heart disease,3,4 resulting in fewer patient visits and hospitalizations. Mobile applications are feasible for collecting postoperative patient outcomes for prostate surgery, hepatopancreaticobiliary surgery, lung cancer surgery, and C-sections.5-8 Other mobile applications for GI and orthopedic surgery have shown efficacy in postoperative wound monitoring and reducing follow-up visits.9-11 Prior studies have also shown that patient engagement through early postoperative phone calls and telehealth visits reduces postoperative emergency room (ER) visits and hospital readmissions, including in thoracic surgery patients.12,13
Previous studies have shown the feasibility of ManageMySurgery (MMS: Higgs Boson, Inc., Durham, NC), a commercially available patient education and outcomes mobile application, in educating patients prior to surgery, collecting patient-reported outcomes surveys, and assigning perioperative tasks to patients. MMS has been validated for use in TAVR,14 spinal fusion surgery,15 and breast cancer surgery;16 and patients in each study reported ease of use and high satisfaction with the application. Given that digital health platforms have been shown to improve outcomes and that MMS is feasible as a platform for patients undergoing TAVR, we aimed to quantify the effect of its use on outcomes for this population. For patients undergoing TAVR, we hypothesize that the use of structured, procedure-specific digital health tools during the perioperative care period can reduce postoperative ER visits, hospital readmissions, and complications.
Methods
Description of Manage My Surgery (MMS)
MMS is HIPAA-compliant mobile application for patients undergoing interventional procedures. It prepares patients for their procedures by providing in-app educational content through frequently asked questions (FAQs) and informational links specific to their surgery, communication with their care team, and tasks to complete through the application. These tasks include checking into appointments, confirming the completion of preoperative instructions, and completing preoperative and postoperative surveys. MMS is available on Android (Google Inc, Mountain View, CA) and iOS (Apple Inc, Cupertino, CA) devices as well as through a Web Application. Literacy evaluation is performed to ensure that all content is accessible at a 7th-grade reading level.
Patient Cohort
Approval was obtained from the Duke University Institutional Review Board prior to beginning the study (Pro00074329, renewed 5/2/2022). All eligible patients were invited to use MMS by their surgeon at their first preoperative appointment if they were scheduled to undergo TAVR at Duke University Medical Center between March 2019 (the month of MMS implementation) and November 2021. Eligibility criteria included English as their primary language, age at least 18 years old, possession of a compatible device, and ability to consent. Patients who were not able to operate their own device or wanted additional at-home assistance could register and allow a family member or friend to proxy using the in-app caregiver function. Patients were only eligible for the study if they had at least 90 days of follow-up after their procedure, as this was the timeline for the postoperative outcomes being collected. Consent was obtained electronically at the time of study enrollment.
Patients were defined as app users if they (or their proxy caregiver) logged into and engaged with the application by completing at least one task or viewing at least one educational FAQ at any time prior to surgery. Patients who did not meet these criteria were assigned to the non-user cohort.
About 2-4 weeks before surgery, app users logged into the application, received structured pre-operative information, and completed baseline surveys. Patients were sent in-app reminders to complete surveys, check-in to preoperative and postoperative appointments, and complete other tasks assigned by their surgical team. Each patient and their proxies went through a brief, standardized orientation within the app that included instructions on accessing in-app education and tasks.
Data Collection
App usage data was collected from the MMS database and stored securely in Amazon Web Services, including the number of sign-ins, number and type of tasks completed, addition of proxy caregiver(s), device used to access MMS, and FAQs viewed. Patient demographics, including age at the time of surgery, sex, insurance status, preoperative comorbidities, and Society for Thoracic Surgeons (STS) short-term mortality risk score were collected via review of the EHR.17,18 EHR review was also used to collect the 90-day postoperative clinical outcomes for the study, which were unplanned readmissions to any hospital, emergency room (ER) visits at any hospital, reasons for these post-operative ER visits, and postoperative complications.
Complications were assigned a score on the Clavien-Dindo scale, which ranks postoperative complications by severity from 1-5.19,20 On this scale, 1 indicates mild (such as requiring IV fluids or oral pain medication) or no treatment needed. 2 indicates complications, pharmacologic treatments, or blood transfusions. 3 indicates the use of procedural interventions (additional surgery, interventional radiology, or endoscopy). 4 indicates ICU-level treatment or organ failure. 5 indicates patient death. Complications were further classified as minor (Clavien score 1 or 2) or major (requiring procedure intervention or ICU level care, Clavien score 3-5). Common postoperative complications were considered in this study, such as wound infections, postoperative pneumonia, and urinary tract infection, as well as those specific to TAVR, such as hematoma, stroke, conduction blocks, and myocardial infarction/acute coronary syndrome.21-24
Statistical Analysis
Descriptive statistics were performed to summarize patient demographics, app usage, and the reasons for ER visits. Differences in continuous variables between App Users and Non-Users were assessed via Welch’s t-test, while differences in categorical variables were assessed with the Chi-squared test with Yates' continuity correction. The primary outcomes of 90-day readmission rate, 90-day ER visit rate, and 90-day complication rate were calculated with their 95% confidence intervals using binomial distribution. Binomial logistic regression models were used to estimate the odds ratio of readmission and ER visit. A multinomial regression model was used to estimate the odds of minor or major complication. All regression models adjusted for patients’ age (as a continuous variable), sex, insurance status, STS score (percent risk of perioperative mortality), and status of prior valve replacement (yes/Valve-in valve versus no). All statistical tests were two-sided, and the significance was assessed at alpha = 0.05 without accounting for multiple testing. Statistical analyses were performed using R Studio version 2022.07.2 for Mac (RStudio Team (2020). RStudio: Integrated Development for R. RStudio, PBC, Boston, MA).
Results
Patient Characteristics & App Usage
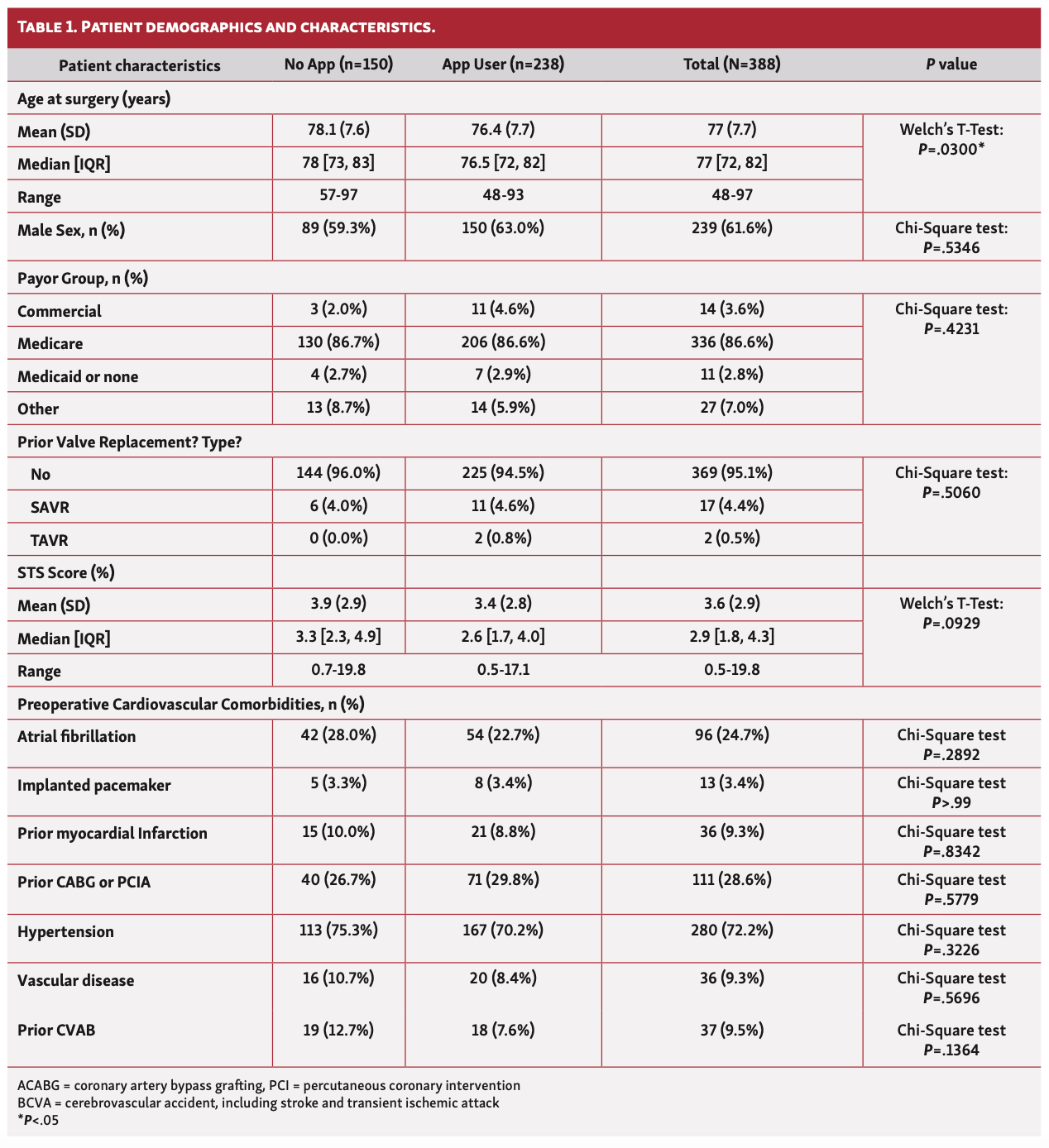
A total of 388 patients undergoing TAVR at Duke University Medical Center between March 2019 and November 2021 were invited to use MMS; of these, 238 patients met the criteria to be counted as App Users. Patient demographics are shown in Table 1. The median age at surgery for app users and non-users was 76.5 years and 78 years, respectively. App users had a higher percentage of male patients (n=150, 63%) as compared to non-users (n=89, 59.3%). The vast majority of patients had Medicare insurance (n=336, 86.6%). 17 patients (4.4%) had previously undergone SAVR, and 2 patients, both in the App User group, had previously undergone TAVR. Common comorbidities in the cohort included hypertension (n=280, 72.2%), previous CABG or PCI (n=111, 28.6%), and atrial fibrillation (n=96, 24.7%). The median STS score was 3.3 and 3.25 percent, respectively, for the app user and non-user groups. The average age was significantly different between the two groups (p=0.03), but none of the other demographics or preoperative comorbidities showed significant differences (Table 1).
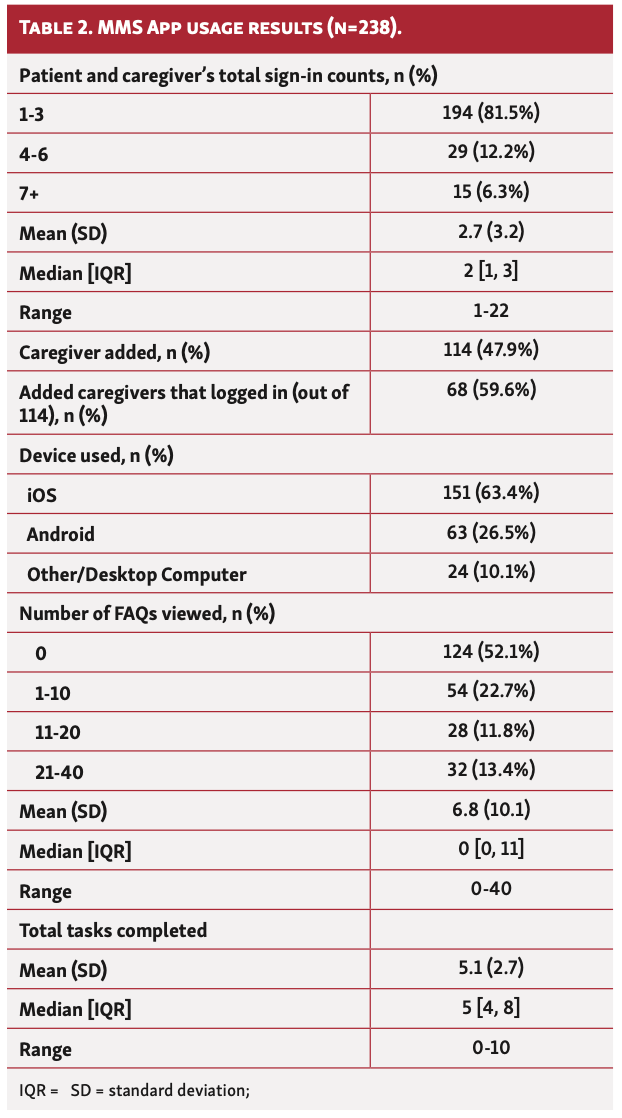
Among the 238 app users, the majority (patients plus caregivers) signed into the app 1-3 times (n=194, 81.5%), 47.9% of the patients had at least one caregiver added (n=114), and 59.6% of them (n=68) had caregivers log in to the app at least once. 151 patients (63.4%) used cell phones with the iOS system and 63 (26.5%) used the Android system. Patients and their caregivers logged onto the application an average of 2.7 times; however, the app can be accessed multiple times if a user is not logged out, thus the actual access number is likely higher. Patients viewed an average of 6.8 FAQs and completed an average of 5.1 tasks. App usage stats are shown in Table 2.
90-Day Clinical Outcomes
90-day ER visit rates, readmission rates, and post-operative complication rates are shown in Table 3. The 90-day readmission rate was lower for app users (8.8% (n=21) vs. 16% (n=24)). The 90-day ER rate for app users was lower than non-users (12.6% (n=30) vs. 27.3% (n=41)). The 90-day complication rate was also lower for app users (21% (n=50) vs. 36.7% (n=55)). The minor complication rate (n=29, 12.2% vs. n=32, 21.3%) and the rate for complications requiring intervention (n=21, 8.8% vs. n=24, 16%) was also lower for app users.
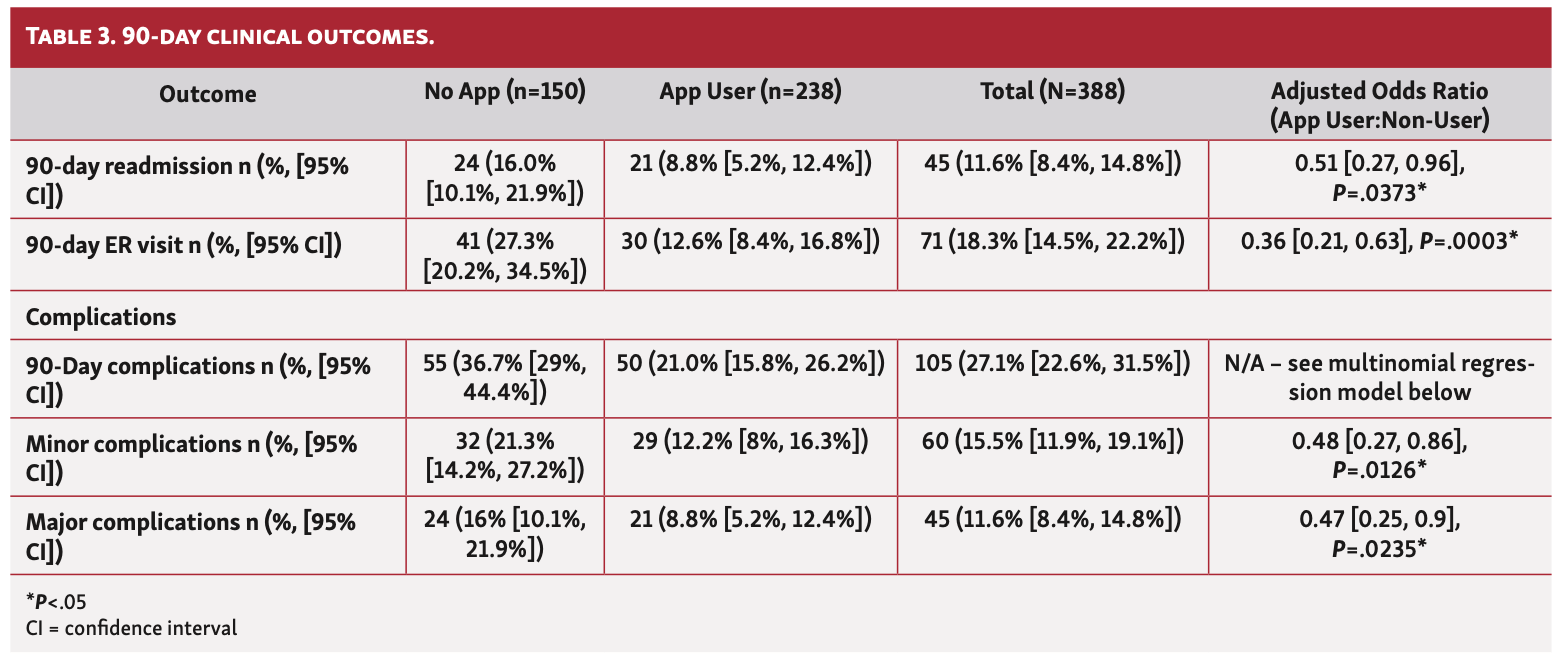
When adjusted for age, sex, insurance status, co-morbid risk (as assessed by the STS Score), and prior valve replacement status using a logistic regression model, the odds of having readmission for app users was 49% lower than in non-users (OR=0.51, p=0.0373) and the odds of having ER visits were 64% lower (OR=0.36, p = 0.0003). The odds of minor complications and major complications (those requiring intervention) for app users compared to non-users were 0.48 (p=0.0126) and 0.47 (p=0.0235), respectively.
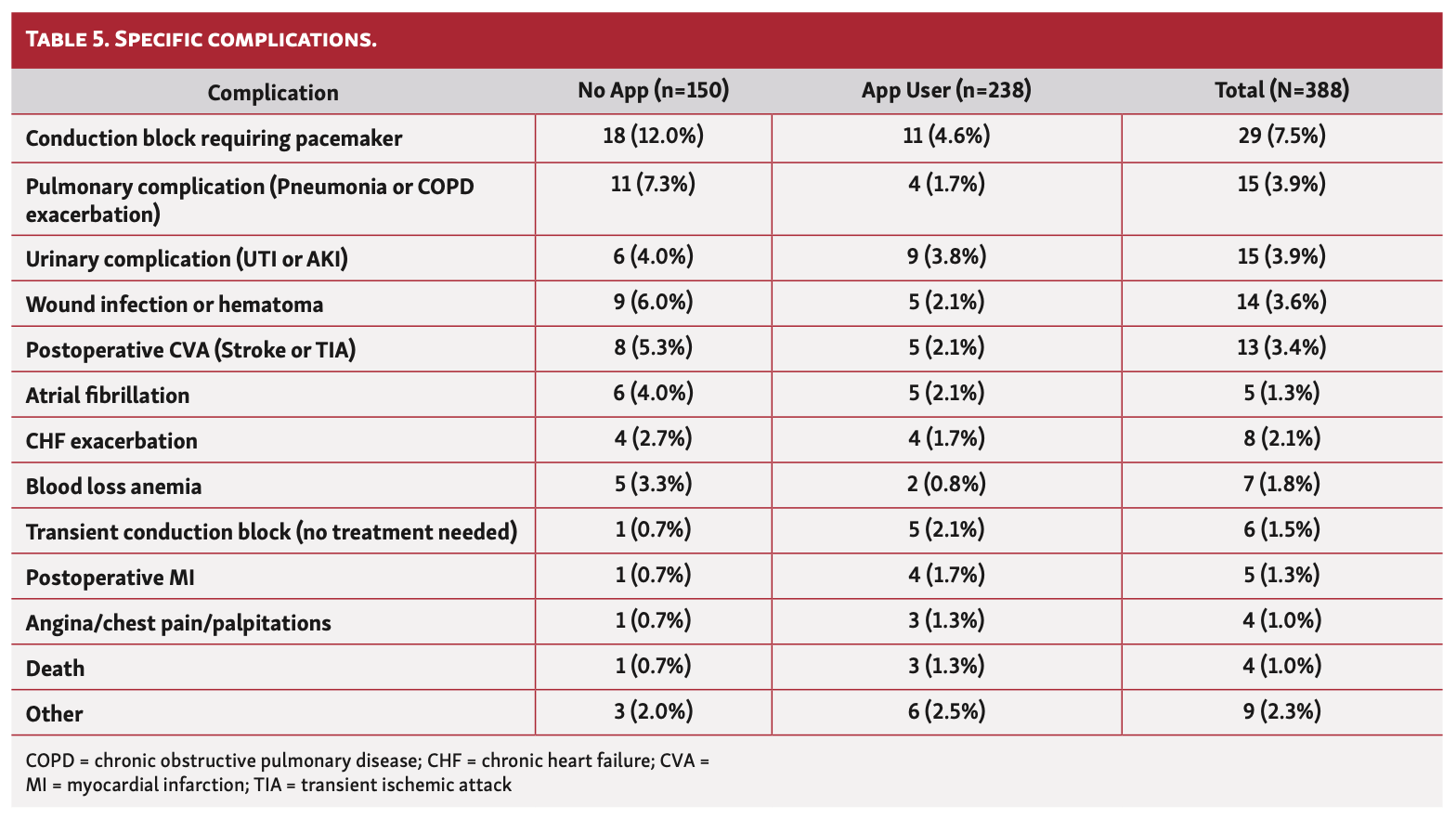
Among the patients who visited the ER in the 90 days after surgery, the most common reasons were heart failure symptoms such as edema, dyspnea, & chest pain (n=18, 4.6%%), neurological symptoms such as weakness & focal neurological deficits, (n=15, 3.9%), and syncope or falls (n=13, 3.4%). The reasons for ER visits are shown in Table 4. Among the patients who experienced postoperative complications, the most common were conduction block requiring placement of a pacemaker (n=29, 7.5%), pulmonary complications such as pneumonia or COPD exacerbation (n=15, 3.9%), and urinary complications such as urinary tract infection or acute kidney injury (n=15, 3.9%). Complications are detailed in Table 5.

Discussion
In our study of TAVR patients, we demonstrate a significant reduction in ER visits, readmissions, and complications associated with the use of a mobile digital health platform. We demonstrated a 7.2% reduction in readmissions, a 14.7% reduction in ER visits, and a 15.7% reduction in total complications among patients using the digital health app. These percentages represent numbers needed to treat (NNT) of 14, 7, and 7, respectively. When adjusted for age, sex, insurance status, STS score, and prior valve replacement status, the odds ratios for all of these outcomes remain statistically significant, suggesting that app use is associated with improved outcomes across demographics and severity of preoperative comorbidities.
This is one of the first digital health application for cardiac surgery reported to improve objective measures of patient outcomes. Although it is not possible to prove direct causality, our results represent a robust analysis, and given the low-risk, low-cost nature of presenting a patient with a smartphone application, implementing digital health tools should be prioritized in procedural settings such as TAVR. The utility of digital health seems to stem from its ability to increase patient engagement, which is a known factor in improving patient outcomes.12,13
Mobile health applications can consistently remind patients of their pre- and postoperative actions, such as stopping and starting medications, taking care of wounds, following up with care providers as appropriate, and looking out for red flags that would necessitate a visit to the ER. This might account for the clinical improvements seen in our study, because patients learn how to better take care of themselves at home and understand what truly constitutes a medical emergency. Digital health also imposes a degree of self-engagement, which might drive long-term change to ensure that a patient stays healthy well after an acute surgical episode.25,26 Further understanding of the mechanism of benefit will require further detailed study.
Our patient demographics suggest that in part, our results might be so stark because of the baseline differences between groups. The app group was significantly younger than the non-app group, and many also had caretakers to help with app nagivation at home. The app group also had a lower STS baseline risk score, which suggests that overall app users were healthier prior to surgery. While this tempers our conclusions, we still believe that app usage and the higher patient education it provides does play some role, especially since the age-difference of 2 years and non-significant STS score differences cannot alone account for adjusted odds differences of over 50%. Additionally, we postulate that if at least some patients are able to self-engage at home through a digital platform, this frees up clinician time to focus on the sicker or more frail patients who require the extra help to prepare for and recover from surgery.
Limitations & Future Directions
Our results are limited by the common biases seen in retrospective cohort studies, such as selection bias. Non-users were initially invited to use MMS but never logged into the app, thus our study excludes patients who were never aware of this technology or who did not own a smartphone and were thus ineligible to participate. While the proportion of older adults with smartphones is increasing, the percentage of those over 65 with a smartphone is about 61%, while over 95% of those under the age of 50 own a smartphone.27 Future studies could compare postsurgical outcomes between people who have a smartphone but never logged into MMS and those without smartphone access to determine if this is a factor.
Other limitations include biases seen in electronic medical record review, including an error in data entry, missing data, and inter-reviewer differences. This study is also limited to patients undergoing TAVR, which while a common procedure, does not represent the wide variety of cardiothoracic procedures a patient can undergo. We plan to develop future modules targeting other procedures such as Coronary Artery Bypass Grafting (CABG) to expand the population that could benefit from a digital health platform. Other future ideas that could improve the experience with a mobile app would be integration with the electronic medical record to automatically transfer data on patient surveys between the two systems or automatically update patient records when medically relevant tasks are completed.
Additionally, while this was a single center study, we believe the results are generalizable to the wider population of patients undergoing TAVR. For example, national database studies have found that the 90-day readmission rate for TAVR patients is around 15-22% 28, 29, which is similar to the non-user readmission rate of 16% in our study. Common reasons for inpatient readmission for TAVR patients include ischemic heart disease, heart failure, arrhythmias, infections, respiratory disorders, and neurological disorders 30, 31, all of which were seen as complications or reasons for ER visits in our study population as listed in Tables 4 and 5.
Conclusions
In summary, we describe the first study demonstrating improvement in patient outcomes after TAVR with a mobile digital health tool used as part of perioperative care. In this non-randomized, retrospective study, we showed significant reductions in 90-day postoperative readmissions, ER visits, and complications among digital app users compared to non-users. By engaging patients throughout their surgical journey with structured education and tasks and making patients aware of a normal postoperative course, digital health tools could prevent unnecessary use of emergency and inpatient care, thus improving individual patient wellbeing, reducing the workload on healthcare providers, and reducing the overall burden on healthcare resources.
Affiliations and Disclosures
From 1Department of Neurosurgery, Duke University Medical Center, Durham, NC, USA; 2Higgs Boson Health, Durham, North Carolina; 3Department of Biostatistics & Bioinformatics, Duke University School of Medicine, Durham, North Carolina; 4Division of Cardiovascular and Thoracic Surgery, Department of Surgery, Duke University Medical Center, Durham, North Carolina; 5Department of Medicine, Duke University Medical Center, Durham, North Carolina; 6Division of Adult Cardiothoracic Surgery, Department of Surgery, UC San Francisco, San Francisco, California.
IRB Approval: Duke University IRB Pro00074329, renewed May 2, 2022
Meeting Presentation: Data from this manuscript was presented as a podium talk at the Society of Thoracic Surgeons 2023 conference.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein. Mr. Venkatraman, Dr. Doberne, and Dr. Nguyen are consultants for Higgs Boson Health, Inc. Dr. Lad, Dr. Gellad, & Mr. Dharmapurikar, as well as Duke University, have equity in Higgs Boson Health. This publication was made possible in part by Grant Number TL1 TR002555 from the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research, given to Mr. Venkatraman. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of NCATS or NIH.
The authors report that patient consent was provided for publication of the images used herein.
Manuscript accepted June 2, 2023
Address for correspondence: Julie Doberne, MD, PhD, Division of Cardiovascular and Thoracic Surgery, Department of Surgery, Box 3443, Duke University Medical Center, Durham, NC 27710. Email: julie.doberne@duke.edu
References
1. Joseph J, Naqvi SY, Giri J, Goldberg S. Aortic Stenosis: Pathophysiology, Diagnosis, and Therapy. Am J Med. Mar 2017;130(3):253-263. doi:10.1016/j.amjmed.2016.10.005
2. Mack MJ, Leon MB, Smith CR, et al. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. Jun 20 2015;385(9986):2477-84. doi:10.1016/S0140-6736(15)60308-7
3. Vegesna A, Tran M, Angelaccio M, Arcona S. Remote Patient Monitoring via Non-Invasive Digital Technologies: A Systematic Review. Telemed J E Health. Jan 2017;23(1):3-17. doi:10.1089/tmj.2016.0051
4. Lunde P, Bye A, Bergland A, Grimsmo J, Jarstad E, Nilsson BB. Long-term follow-up with a smartphone application improves exercise capacity post cardiac rehabilitation: A randomized controlled trial. Eur J Prev Cardiol. Nov 2020;27(16):1782-1792. doi:10.1177/2047487320905717
5. Belarmino A, Walsh R, Alshak M, Patel N, Wu R, Hu JC. Feasibility of a Mobile Health Application To Monitor Recovery and Patient-reported Outcomes after Robot-assisted Radical Prostatectomy. European Urology Oncology. 2019/07/01/ 2019;2(4):425-428. doi:https://doi.org/10.1016/j.euo.2018.08.016
6. Pickens R, Cochran A, Tezber K, et al. Using a Mobile Application for Real-Time Collection of Patient-Reported Outcomes in Hepatopancreatobiliary Surgery within an ERAS® Pathway. The American Surgeon™. 2019;85(8):909-917. doi: 10.1177/000313481908500847
7. Kneuertz PJ, Jagadesh N, Perkins A, et al. Improving patient engagement, adherence, and satisfaction in lung cancer surgery with implementation of a mobile device platform for patient reported outcomes. J Thorac Dis. Nov 2020;12(11):6883-6891. doi:10.21037/jtd.2020.01.23
8. Ke JXC, George RB, Wozney L, Munro A. Perioperative mobile application for mothers undergoing Cesarean delivery: a prospective cohort study on patient engagement. Can J Anaesth. Apr 2021;68(4):505-513. Application mobile perioperatoire destinee aux meres avec un accouchement par cesarienne : une etude de cohorte prospective sur l'interet des patientes. doi:10.1007/s12630-020-01907-x
9. Higgins J, Chang J, Hoit G, Chahal J, Dwyer T, Theodoropoulos J. Conventional Follow-up Versus Mobile Application Home Monitoring for Postoperative Anterior Cruciate Ligament Reconstruction Patients: A Randomized Controlled Trial. Arthroscopy. Jul 2020;36(7):1906-1916. doi:10.1016/j.arthro.2020.02.045
10. Symer MM, Abelson JS, Milsom J, McClure B, Yeo HL. A Mobile Health Application to Track Patients After Gastrointestinal Surgery: Results from a Pilot Study. Journal of Gastrointestinal Surgery. 2017/09/01 2017;21(9):1500-1505. doi:10.1007/s11605-017-3482-2
11. Scheper H, Derogee R, Mahdad R, et al. A mobile app for postoperative wound care after arthroplasty: Ease of use and perceived usefulness. International Journal of Medical Informatics. 2019/09/01/ 2019;129:75-80. doi:https://doi.org/10.1016/j.ijmedinf.2019.05.010
12. Tham E, Nandra K, Whang SE, Evans NR, Cowan SW. Postoperative Telehealth Visits Reduce Emergency Department Visits and 30-Day Readmissions in Elective Thoracic Surgery Patients. J Healthc Qual. Jul-Aug 01 2021;43(4):204-213. doi:10.1097/JHQ.0000000000000299
13. Shah M, Douglas J, Carey R, et al. Reducing ER Visits and Readmissions after Head and Neck Surgery Through a Phone-based Quality Improvement Program. Ann Otol Rhinol Laryngol. Jan 2021;130(1):24-31. doi:10.1177/0003489420937044
14. Venkatraman V, Ponder M, Gellad ZF, et al. Feasibility study of a novel digital health platform for patients undergoing transcatheter aortic valve replacement. J Card Surg. Jul 2022;37(7):2017-2022. doi:10.1111/jocs.16515
15. Ponder M, Ansah-Yeboah AA, Charalambous LT, et al. A Smartphone App With a Digital Care Pathway for Patients Undergoing Spine Surgery: Development and Feasibility Study. JMIR Perioper Med. Oct 16 2020;3(2):e21138. doi:10.2196/21138
16. Ponder M, Venkatraman V, Charalambous L, et al. Mobile Health Application for Patients Undergoing Breast Cancer Surgery: Feasibility Study. JCO Oncol Pract. Sep 2021;17(9):e1344-e1353. doi:10.1200/op.20.01026
17. Shahian DM, Jacobs JP, Badhwar V, et al. The Society of Thoracic Surgeons 2018 Adult Cardiac Surgery Risk Models: Part 1-Background, Design Considerations, and Model Development. Ann Thorac Surg. May 2018;105(5):1411-1418. doi:10.1016/j.athoracsur.2018.03.002
18. O'Brien SM, Feng L, He X, et al. The Society of Thoracic Surgeons 2018 Adult Cardiac Surgery Risk Models: Part 2-Statistical Methods and Results. Ann Thorac Surg. May 2018;105(5):1419-1428. doi:10.1016/j.athoracsur.2018.03.003
19. Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. Aug 2009;250(2):187-96. doi:10.1097/SLA.0b013e3181b13ca2
20. Goitein D, Raziel A, Szold A, Sakran N. Assessment of perioperative complications following primary bariatric surgery according to the Clavien-Dindo classification: comparison of sleeve gastrectomy and Roux-Y gastric bypass. Surg Endosc. Jan 2016;30(1):273-8. doi:10.1007/s00464-015-4205-y
21. Mach M, Okutucu S, Kerbel T, et al. Vascular Complications in TAVR: Incidence, Clinical Impact, and Management. J Clin Med. Oct 28 2021;10(21)doi:10.3390/jcm10215046
22. Rodes-Cabau J, Ellenbogen KA, Krahn AD, et al. Management of Conduction Disturbances Associated With Transcatheter Aortic Valve Replacement: JACC Scientific Expert Panel. J Am Coll Cardiol. Aug 27 2019;74(8):1086-1106. doi:10.1016/j.jacc.2019.07.014
23. Faroux L, Guimaraes L, Wintzer-Wehekind J, et al. Coronary Artery Disease and Transcatheter Aortic Valve Replacement: JACC State-of-the-Art Review. J Am Coll Cardiol. Jul 23 2019;74(3):362-372. doi:10.1016/j.jacc.2019.06.012
24. Mangla A, Gupta S. Vascular complications post-transcatheter aortic valve procedures. Indian Heart J. Sep - Oct 2016;68(5):724-731. doi:10.1016/j.ihj.2015.11.024
25. Graffigna G, Barello S. Patient Health Engagement (PHE) model in enhanced recovery after surgery (ERAS): monitoring patients' engagement and psychological resilience in minimally invasive thoracic surgery. J Thorac Dis. Mar 2018;10(Suppl 4):S517-S528. doi:10.21037/jtd.2017.12.84
26. Miller KL. Patient centered care: A path to better health outcomes through engagement and activation. NeuroRehabilitation. Oct 14 2016;39(4):465-470. doi:10.3233/nre-161378
27. Faviero M. Share of those 65 and older who are tech users has grown in the past decade. Pew Research Center. https://www.pewresearch.org/fact-tank/2022/01/13/share-of-those-65-and-older-who-are-tech-users-has-grown-in-the-past-decade/
28. Pajjuru VS, Thandra A, Guddeti RR, et al. Sex differences in mortality and 90-day readmission rates after transcatheter aortic valve replacement: a nationwide analysis from the USA. Eur Heart J Qual Care Clin Outcomes. Mar 2 2022;8(2):135-142. doi:10.1093/ehjqcco/qcab012
29. Chakraborty S, Patel N, Bandyopadhyay D, et al. Readmission following urgent transcatheter aortic valve implantation versus urgent balloon aortic valvuloplasty in patients with decompensated heart failure or cardiogenic shock. Catheter Cardiovasc Interv. Sep 2021;98(3):607-612. doi:10.1002/ccd.29690
30. Khoury H, Ragalie W, Sanaiha Y, et al. Readmission After Surgical Aortic Valve Replacement in the United States. Ann Thorac Surg. Sep 2020;110(3):849-855. doi:10.1016/j.athoracsur.2019.11.058
31. Senussi MH, Schindler J, Sultan I, et al. Long term mortality and readmissions after transcatheter aortic valve replacement. Cardiovasc Diagn Ther. Aug 2021;11(4):1002-1012. doi:10.21037/cdt-20-916












