Independent Clinical and Echocardiographic Predictors of Restenosis After Percutaneous Mitral Balloon Commissurotomy in a Large, Consecutive Cohort Followed for 24 Years
Abstract
Objectives. To enlighten preprocedural risk factors of mitral valve restenosis in a large, single-center cohort of patients submitted to percutaneous mitral balloon commissurotomy (PMBC) for the treatment of mitral stenosis (MS) secondary to rheumatic heart disease. Methods. This is a database analysis of a single-center, high-volume tertiary institution involving all consecutive PMBC procedures performed in the mitral valve (MV). Restenosis was diagnosed when MV area was <1.5 cm2 and/or loss of 50% or more of the immediate procedural result aligned with the return/worsened symptoms of heart failure. The primary endpoint was to determine the preprocedural independent predictors of restenosis after PMBC. Results. Among a total of 1921 PMBC procedures, 1794 consecutive patients without previous intervention were treated between 1987 and 2010. Throughout 24 years of follow-up, MV restenosis was observed in 483 cases (26%). Mean age was 36 years and most (87%) were female. Median follow-up duration was 9.03 years (interquartile range, 0.33-23.38). Restenosis population, however, presented a significantly lower age at the procedure time as well as a higher Wilkins-Block score. At multivariate analysis, independent preprocedure predictors of restenosis were left atrium diameter (hazard risk [HR], 1.03; 95% confidence interval [CI], 1.02-1.05; P<.04), preprocedure maximum gradient (HR, 1.02; 95% CI, 1.00-1.03; P=.04), and higher Wilkins-Block score (>8) (HR, 1.38; 95% CI, 1.14-1.67; P<.01). Conclusions. At long-term follow-up, MV restenosis was observed in a quarter of the population undergoing PMBC. Preprocedure echocardiographic findings, including left atrial diameter, maximum MV gradient, and Wilkins-Block score were found to be the only independent predictors.
J INVASIVE CARDIOL 2023;35(3):E113-E121.
Key words: mitral valve stenosis, percutaneous mitral balloon comissurotomy, rheumatic heart disease, restenosis
Development of restenosis after successful percutaneous mitral balloon valvuloplasty (PMBC) is a challenging issue and can occur within the first year after the procedure and thereafter in a growing percentage.1-3 Its incidence varies widely in the literature (from 4% to 39%) according to the differences in populations and follow-up duration.3,4,7-10
Another relevant issue to define the real incidence of mitral restenosis refers to its definition. Since patients with mitral valve area (MVA) >1.5 cm2 are generally considered to have mild stenosis and tend to be relatively asymptomatic, this value has been arbitrarily adopted as the threshold to define procedural success, as well as future recurrence of the stenosis.14
The potential clinical impact of time-dependent MVA reduction during long-term follow-up is not contemplated in this definition, and data on its occurrence are not available in current published registries. Furthermore, little is known on the preprocedural echocardiographic findings and on PMBC acute results in predicting the long-term occurrence of restenosis.4-7,15
We sought to determine the independent preprocedure predictors of restenosis following successful PMBC on patients with mitral stenosis (MS) who have not been previously submitted to any invasive (percutaneous or surgical) valve procedure.
Methods
Study population. A prospective database was created to assemble information from all 1921 consecutive PMBC procedures performed at a single-center, high-volume tertiary institution through patients with severe rheumatic MS submitted to PMBC between 1987 and 2010. For the purpose of the present study, 116 procedures were excluded from the analysis due to a prior surgical mitral valve intervention and another 11 patients were excluded due to missing data crucial to the implementation of the analysis.
All procedures were executed by the same team of interventional cardiologists and were guided by transesophageal echocardiography. Patient clinical status was determined according to the New York Heart Association (NYHA) classification.
Indications for PMBC were in compliance with national and international guidelines of cardiac valve diseases at the time of the procedure, as follows: (1) symptomatic patients with moderate or severe MS with favorable valve morphology, based on echocardiographic evaluation, including Wilkins score ≤8;20 (2) asymptomatic patients with moderate to severe MS and pulmonary hypertension (systolic pulmonary artery pressure >50 mm Hg at rest) with favorable valve morphology; and (3) symptomatic patients with moderate or severe MS, with unfavorable valve morphology, but not eligible for surgery. Contraindications to PMBC were detailed previously and correspond to guidelines, including patients with moderate or greater MR or left atrial appendage thrombus.21-23
The study protocol and related materials were approved by the institutional review board and ethical committee of our center and followed the principles of the 1975 Declaration of Helsinki. Patients were enrolled after signing the informed consent.
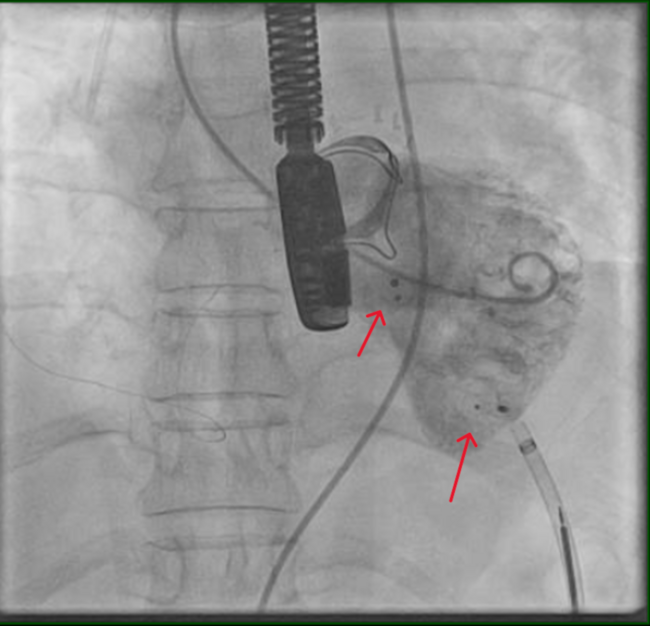
Percutaneous mitral balloon commissurotomy and imaging study. PMBC was performed by an antegrade transseptal approach using the Inoue technique,24 multitrack,25 double-balloon,24 or metallic commissurotomy.26 Balloon size was chosen according to the mitral annulus size or to obtain an effective balloon dilation area/body surface area of approximately 4 cm2/m2,5 and 1-step dilation was performed. Maximum balloon size was determined by the following formula: (patient height [cm]/10) + 10.27 The decision to perform additional inflations was left at the operator’s discretion and based on immediate hemodynamic and echocardiographic findings.
Doppler echocardiographic evaluation was performed before and during the procedure and 24 hours after PMBC, and included the assessment of MVA using 2-dimensional echocardiography or, when the planimetry was not viable, the pressure half-time method. Estimation of mitral regurgitation (MR) was performed by the semiquantitative color Doppler method28 and classified as absent (0), mild (1+), moderate (2+), moderately severe (3+), or severe (4+).
In addition, MV morphological assessment was performed based on the semiquantitative valve analysis, including the degree of leaflet mobility (ranging from 1-4), valve calcification, as well as valvar and subvalvar apparatus thickening. The sum of these characteristics resulted in the echocardiographic score proposed by Wilkins and Block et al.20 Patients were categorized according to the score obtained into score ≤8 or score >8 groups.
The success of the procedure was defined as the achievement of postprocedure MVA ≥1.5 cm2 or a gain of at least 50% of the preprocedure MVA, without angiographic MR <3+ (by the Sellers classification), and in the absence of in-hospital major adverse cardiac and cerebrovascular events, including any death, stroke, mitral valve surgery, and cardiac tamponade.
Follow-up and restenosis. Clinical and echocardiographic evaluations were performed immediately after the procedure and annually after PMBC for up to 24 years. Clinical evaluation was performed by direct interview (history and physical examination) of the patient at outpatient visits. Adverse events were monitored throughout the study period. If a patient was lost to follow-up, family, physician, or personal cardiologist was contacted.
Restenosis was defined as the worsening of symptoms of heart failure combined with echocardiographic findings supporting such clinical findings, or when a follow-up echocardiography was performed and revealed the degeneration of MS, defined as MVA (obtained through either planimetry or half pressure time) <1.5 cm2 and/or loss of 50% or more of the postprocedural immediate result, in an otherwise asymptomatic patient.
Statistical analysis. Continuous variables were reported as mean ± standard deviation and were compared using Student’s t test or the Wilcoxon test, as appropriate. Categorical variables were reported as percentages and compared using Chi-square or Fisher’s exact test.
Significant variables in the univariate analysis and/or clinically relevant variables were included in the logistic regression analyzes for predictors of immediate success after PMBC. Stepwise-backward method was used to access the reduced model.
Long-term restenosis-free survival was calculated using the Kaplan-Meier method. Univariate analysis was used to test the relationship between clinical and treatment variables and the occurrence of restenosis in the follow-up, by Cox regression for the quantitative variables and by the log-rank test for the qualitative variables. At the multivariate analysis, multiple stepwise Cox regression methodology was applied to the covariables found significant at the univariate analysis.
The population was divided according to the occurrence of MV restenosis and a total of 16 variables were analyzed, 4 clinical (age, gender, NYHA classification, and baseline electrocardiographic rhythm) and 12 echocardiographic parameters: pressure half-time valve area (PHVA), planimetry valve area (PLVA), maximum mitral gradient (MaxMG), medium mitral gradient (MedMG), left ventricular ejection fraction (LVEF), left atrium diameter, Wilkins score, mitral leaflet mobility, MV thickness, subvalvular thickening, MV calcification, and MR).
For all analyses, P-value was considered significant when <.05. The data were analyzed using the statistical software package IBM SPSS (Statistical Package for the Social Sciences), version 20.0, and R Core Team 2017 (The R Foundation for Statistical Computing) programs.
Results
Between 1987 and 2011, a total of 1921 consecutive PMBC procedures were performed in our center. Among the total population, 1805 procedures (93.9%) were performed on MV without previous interventions. For the final analysis, 11 procedures were excluded due to insufficient data. Restenosis was observed in 483 patients (26%).
Baseline clinical, electrocardiographic and echocardiographic variables are shown in Table 1 and Table 2, respectively. Mean population age was 36.5 ± 12.8 years and most (86.1%) were female. Interestingly, pulmonary artery hypertension was the single clinical variable to differ between groups (34.8% vs 21.7%; P<.01), being significantly more present in restenosis group. Regarding echocardiography variables, only Wilkins score variables differ significantly (8.76 ± 1.27 [IQR, 6-14] vs 8.62 ± 1.17 [IQR, 6-14]; P=.05). MV thickness and express calcification were both significantly more observed in the restenosis population. Although not as statistically significant, the subvalvular apparatus was more compromised in the group without restenosis.
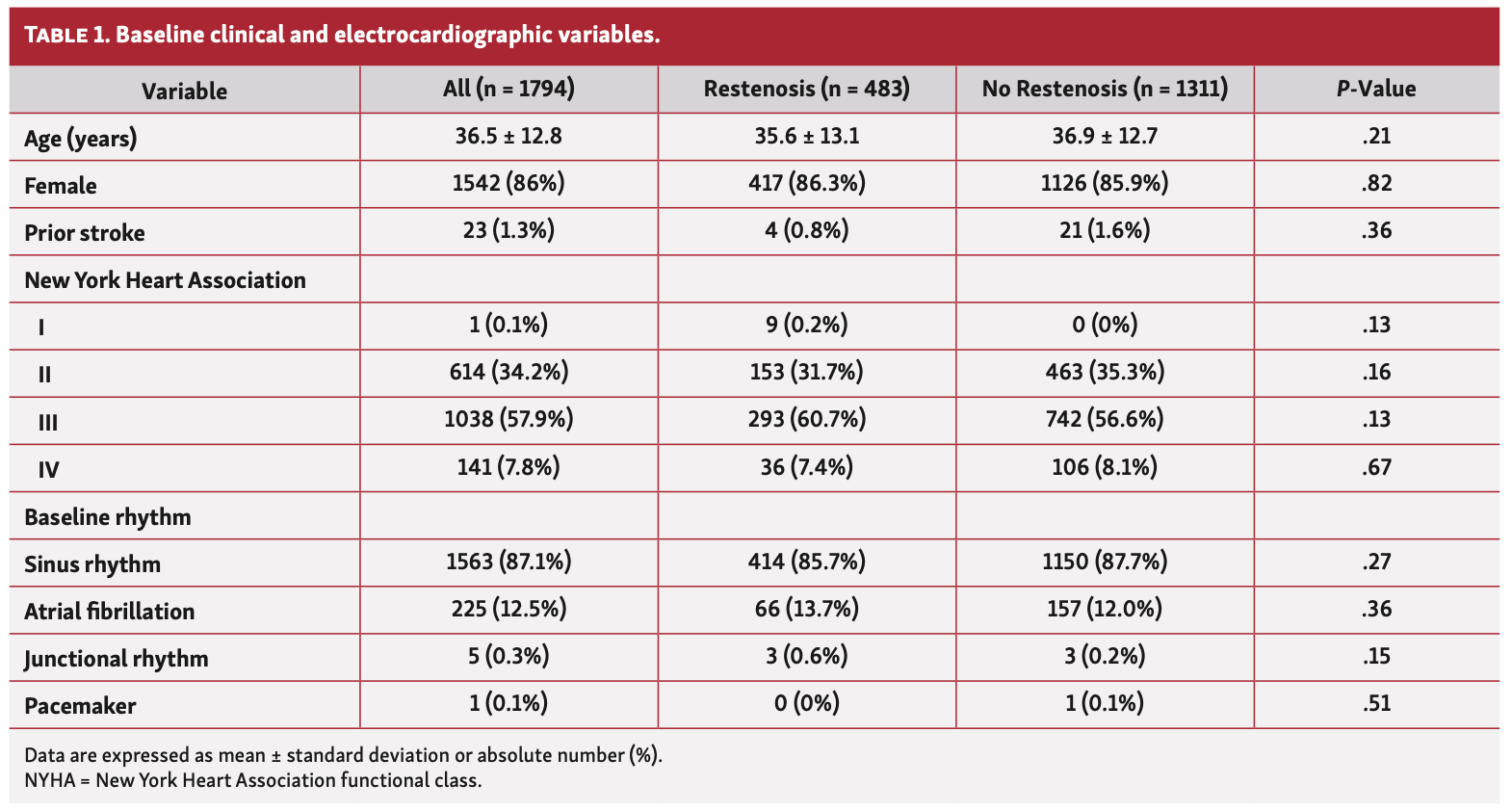
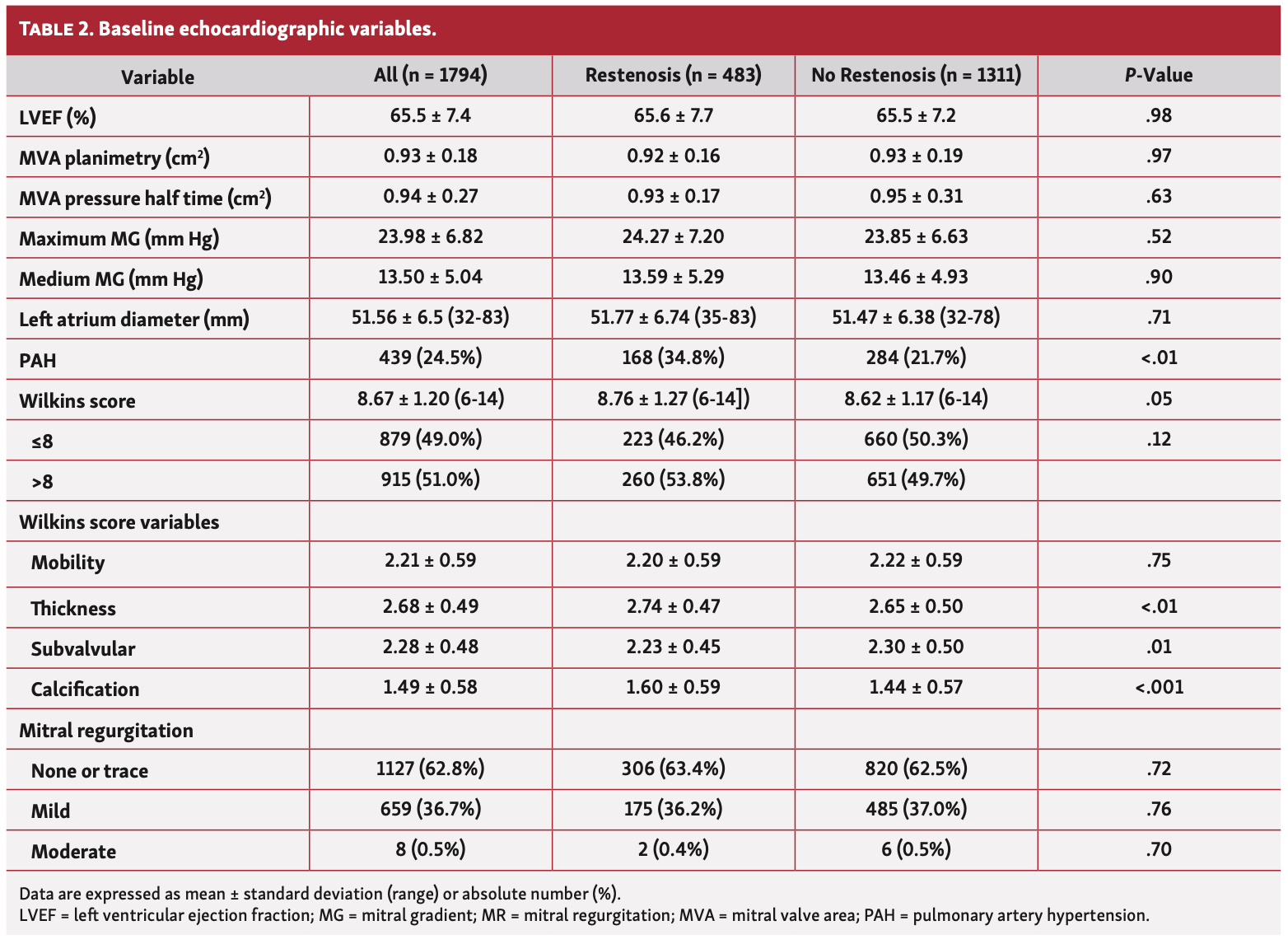
Figure 1 shows Kaplan-Meier overall cumulative incidence of restenosis after PMBC due to rheumatic mitral stenosis. The median follow-up time for the study population was 9.03 years, ranging from 0.33 up to 23.38 years.
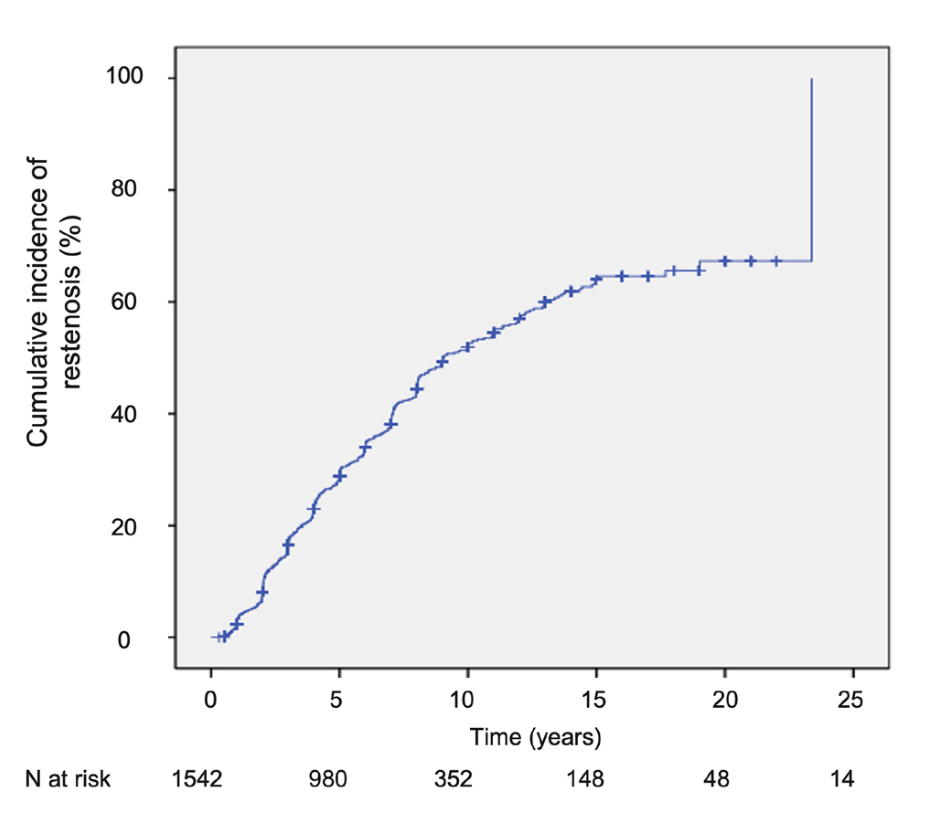
Figure 2 shows grading of MV characteristics (Wilkins score) distribution among patients submitted to PMBC with and without restenosis throughout 24 years of follow-up.
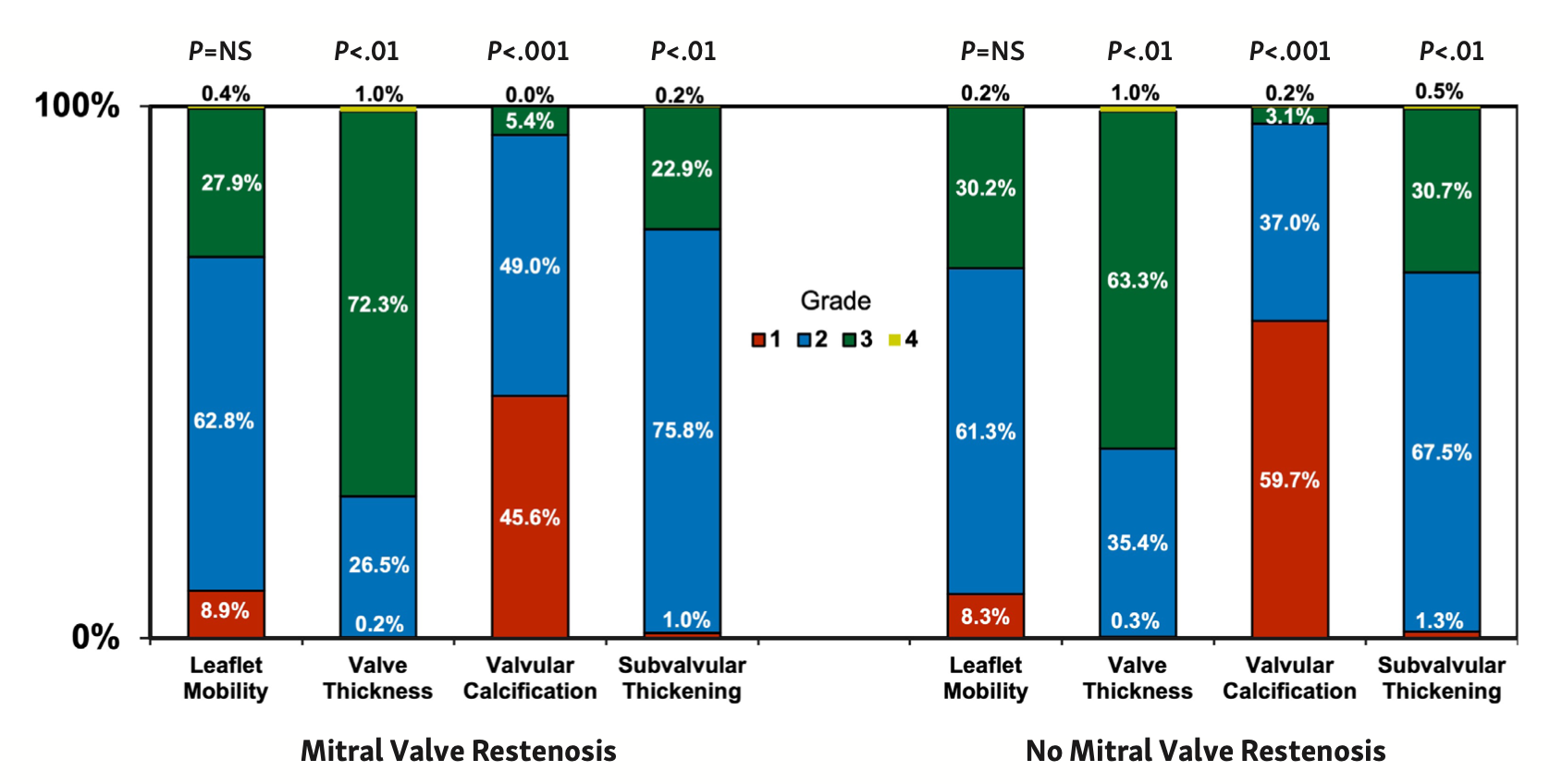
The different echocardiographic parameters evaluated in the Wilkins score play different roles in the occurrence of restenosis, with the most impactful being the leaflet mobility (Figure 3A) (log-rank P<.01), valvular calcification (Figure 3C) (log-rank P<.01), and valve thickness (Figure 3D) (log-rank P=.02). In the present analysis, subvalvular thickening was less relevant (Figure 3B) (log-rank P=.51). Of note, unfavorable Wilkins score (>8) was associated with a higher occurrence of restenosis, as showed in Kaplan-Meier restenosis-free survival curves after PMBC (Figure 4).
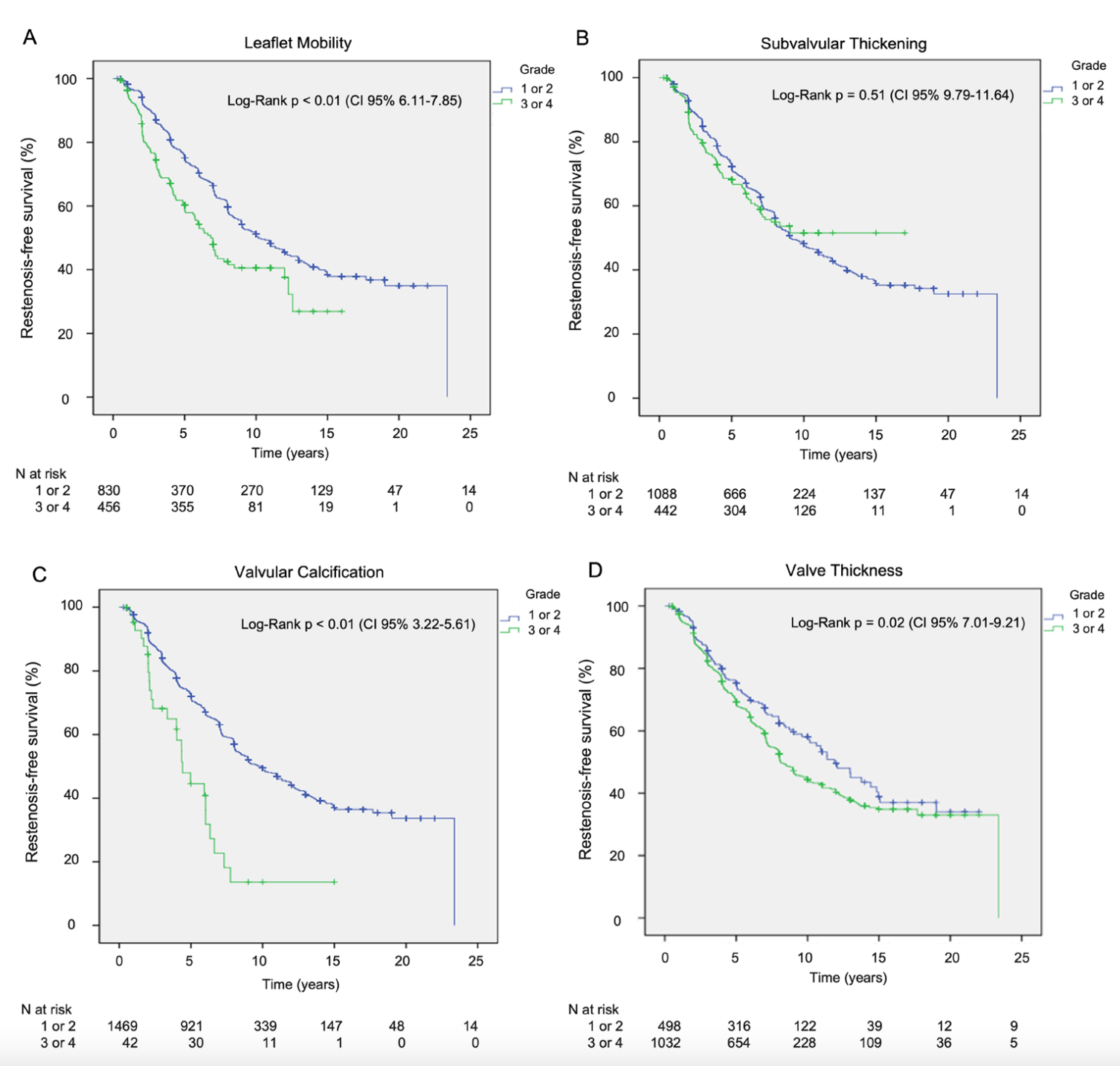
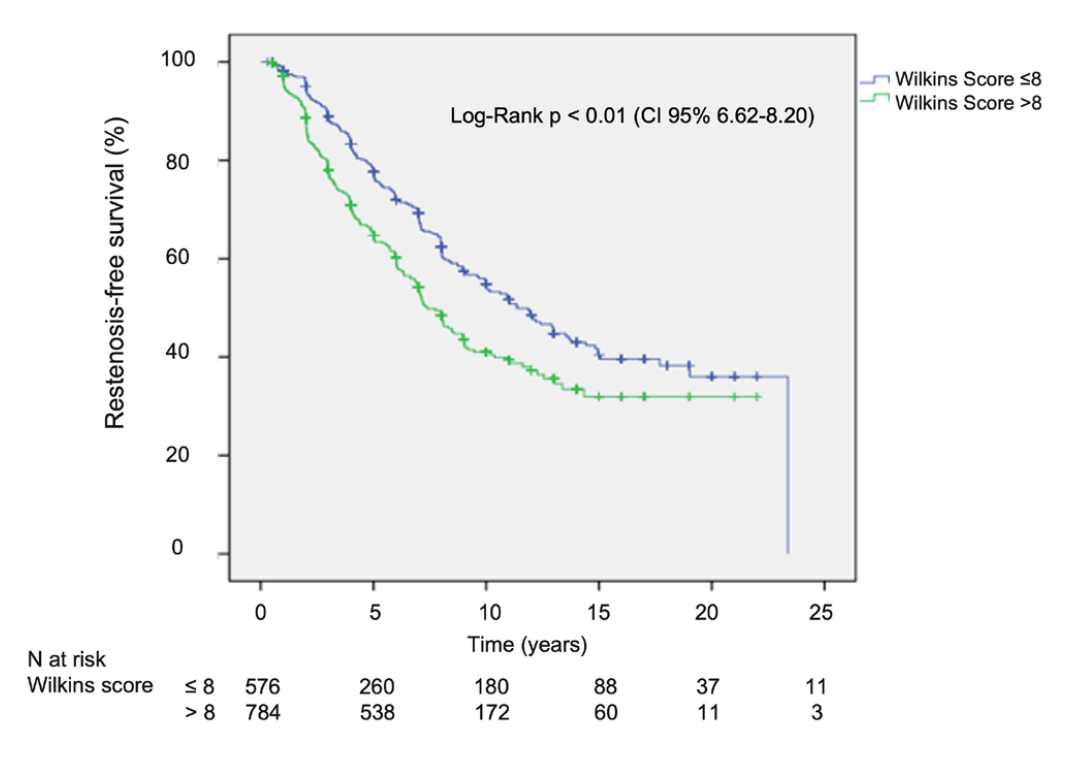
Table 3 displays the results of the univariate analysis. Lack of atrial fibrillation at the time of PMBC was the single clinical variable that correlated to restenosis-free survival in the univariate model, regardless of how the analysis was made (grouped [P=.36] or ungrouped [P<.01]; hazard risk [HR], 1.16; 95% confidence interval [CI], 0.84-1.59) (Table 3). Figure 5 illustrates the Kaplan-Meier curves for the comparison between patients with and without atrial fibrillation. Conversely, echocardiographic measurements, such as maximum and medium MV gradients, pressure-half time MVA, and left atrium diameter were all correlated to the development of restenosis. Regarding Wilkins score variables, leaflet mobility (P<.001), valve thickness (P=.047), and calcification (P<.001) were found to be significantly related to the development of restenosis. Interestingly, subvalvular apparatus thickening did not show the same correlation (P=.93). When these variables were combined in the Wilkins score and grouped as favorable (≤8) or unfavorable (>8), the latest one was strongly correlated to poor clinical outcomes.
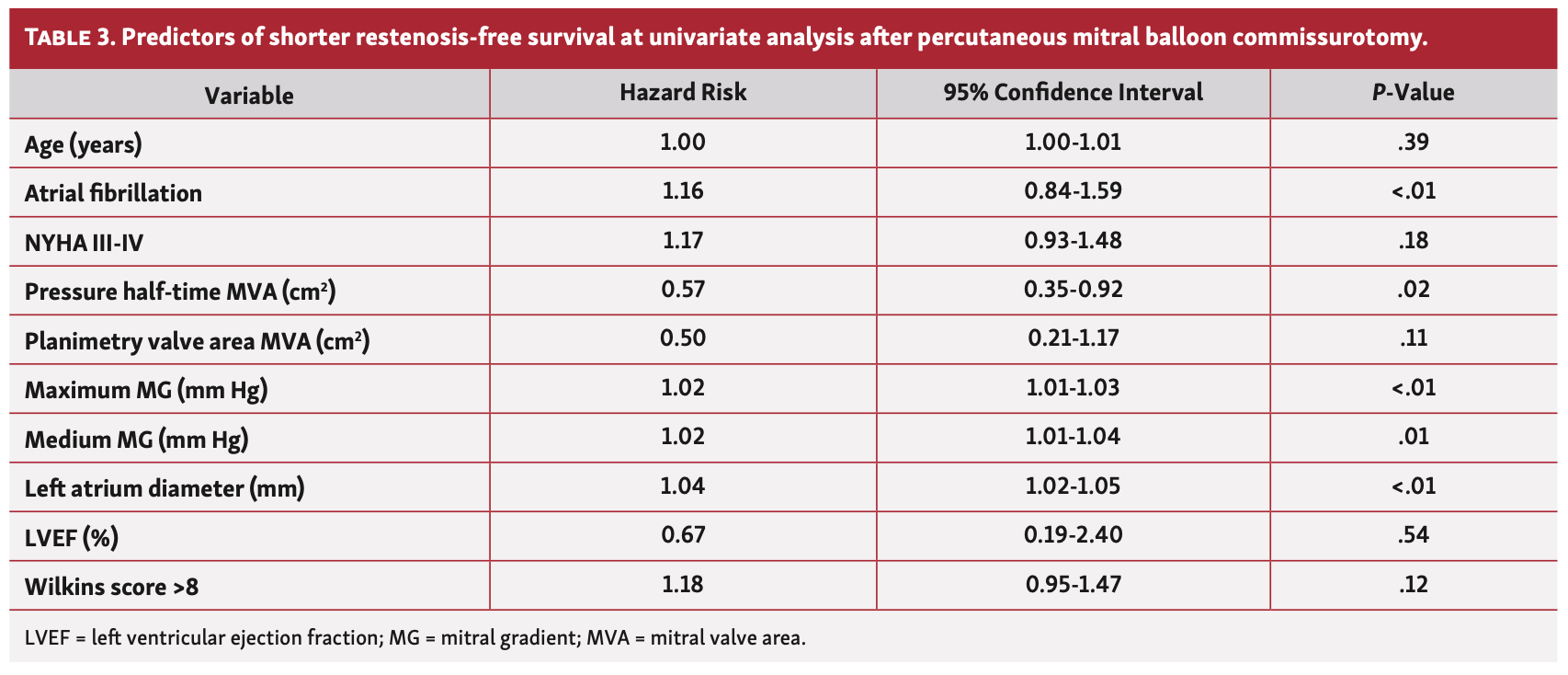
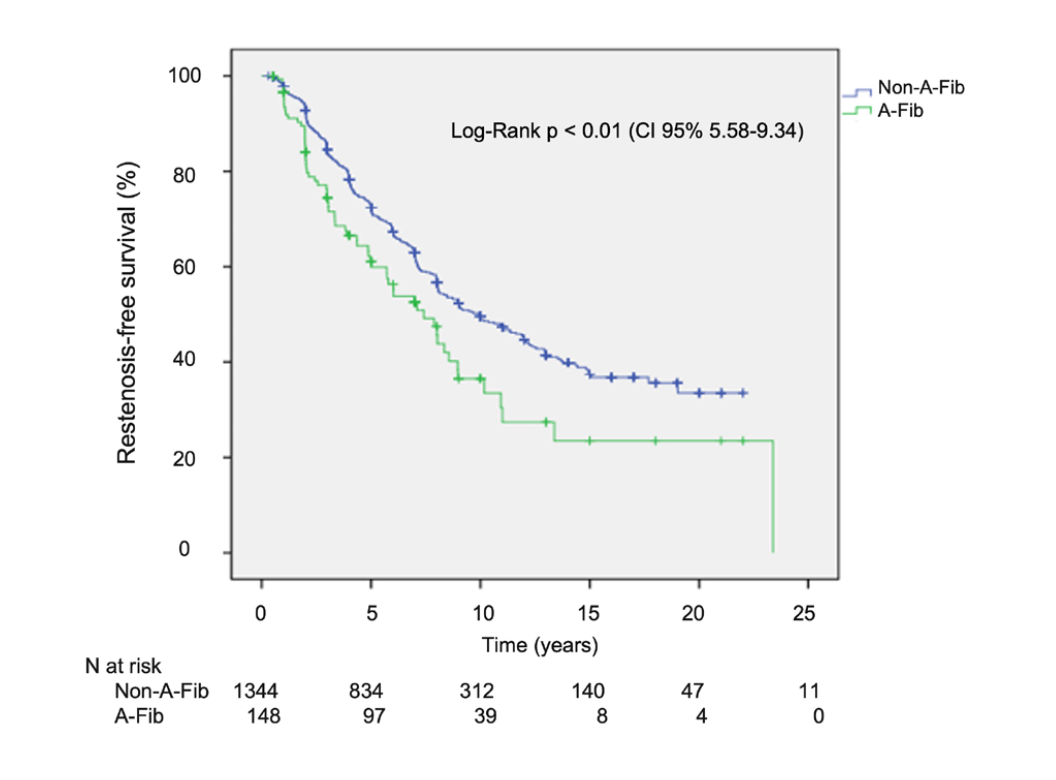
Table 4 displays the multivariate analysis. Only echocardiographic variables were associated with the occurrence of restenosis, ie, left atrium diameter (HR, 1.03; 95% CI, 1.02-1.05; P<.04), preprocedure maximum gradient (HR, 1.02; 95% CI, 1.00-1.03; P=.04), and higher Wilkins score (>8) (HR, 1.38; 95% CI, 1.14-1.67; P<.01).

At a median of 9.03 years (IQR, 0.33-23.38) of clinical follow-up, mortality was similar between both groups (1% for patients without restenosis vs 0.94% for those with restenosis; P=.89). However, patients with restenosis required significantly more percutaneous redilation (31.2% vs 0.11%; P<.01) and/or surgical MV replacement (19.66% vs 8.43%; P<.01).
Discussion
Using data from our local registry, we have identified that development of restenosis after successful PMBC was time dependent, and that preprocedure echocardiographic findings of left atrial diameter, maximum MV gradient, and higher Wilkins-Block score were found to be independent predictors of this deleterious event throughout time (up to 24 years).
In the 40 years since its first performance, PMBC has revolutionized the evolution of MS patients in developing countries and remains an important option for suitable patients in industrialized nations. Mitral valve restenosis is expected at some point during follow-up due to the persistence of underlying rheumatic pathology. However, the timing of its appearance and incidence rates have been shown to be multifactorial; most studies correlate restenosis with age and anatomy, and time to restenosis correlates with the initial improvement in MVA.29,30
In a study from Saudi Arabia, patients with a mean age of 31 years had freedom from restenosis in 85%, 70%, and 44% at 5, 10, and 15 years, respectively.31 Baseline echocardiographic score, which represents MV morphology, has been found to be the most important preprocedural factor determining procedural success, as well as being an independent factor determining event-free survival.7,15,16,18,19 These findings have been very useful in selecting appropriate candidates for PMBC, with a standard guideline of echocardiographic score ≤8. However, a number of alternative scoring systems have been proposed because of multiple limitations of this score.
The analysis of a homogeneous mechanism of MV deterioration, ie, mitral restenosis, is more appropriate to ensure a reliable identification of predictive factors of good late functional results.32 Late outcome is highly dependent on the immediate results of PMBC and poor immediate results are related to insufficient valve opening or severe traumatic MR, leading to early surgery or death in most patients.32 Conversely, after good immediate results, late functional deterioration is progressive and occurs at a constant rate over time, as shown by the linear decrease of the curve in the present series. Restenosis has been shown to be the main cause of late deterioration after successful PMBC, and therefore, must be monitored.4,6,16,33
Controversial reports are available for the relationship between restenosis and long-term clinical outcomes.6,16 The absence of regular echocardiographic follow-up data and relatively short follow-up duration of the previous reports might have contributed as serious confounding factors. Considering the gradual deterioration of functional class and a continued risk of MV surgery after PMBC17-19 with relatively sharp deterioration of functional status 5 years after successful PMBC,18,19 longer clinical observation was required to accurately assess the procedural success of PMBC.
Regarding the echocardiography variables in the present study, only Wilkins score variables differed significantly (8.76 ± 1.27 [IQR, 6-14] vs 8.62 ± 1.17 [IQR, 6-14]; P=.05) between groups. Specifically, the variables of leaflet mobility (P<.001), valve thickness (P=.047), and calcification (P<.001) were found to be significantly related to the development of restenosis. This has not been demonstrated previously, and only leaflet calcification and subvalvular thickening were independently predictive of outcomes; leaflet mobility and leaflet thickening, the other 2 elements of the scoring system, were not.21,22
In another study, baseline echocardiographic score was not an independent predictor of procedural success and development of restenosis or clinical events, probably due to selection bias. In contrast to our study, the mean echocardiographic score was 7.3 ± 1.3 and the proportion of patients with echocardiographic score >8 was significantly lower (around 30%), while the population was older. Thus, the prognostic power of echocardiographic score might be underestimated.33
After a good immediate result with PMBC, 1 out of 3 patients remains free from surgery, and 1 out of 5 have a good functional result at 20 years. Percutaneous mitral balloon commissurotomy can also be used to treat restenosis, but only a few series have reported mid-term results, with the longest follow-up reported to 10 years. A series of 163 consecutive patients with previous commissurotomy (surgical commissurotomy in the majority) reported overall survival of 68% at 20 years after PMBC and a large majority of patients had a reintervention on the MV, since only 16% of patients were free from any reintervention.34
Patients with restenosis after PMBC or closed surgical separation can be treated by repeat PMBC, which has similar curative effect with primary PMBC and better improvement of symptoms with long-term follow-up.35
The presence of AF is definitely associated with worse outcomes in patients with rheumatic MS and with suboptimal results after PMBC, as demonstrated previously36 and in the present study, and could represent ongoing inflammation. Atrial fibrillation may be the equivalent of symptom onset, signifying that rheumatic MS is resulting in progressive left atrial damage and also may contribute to persistent atrial fibrillation and restenosis after PMBC. Commissurotomy does not appear to prevent the occurrence of atrial fibrillation, but should be considered the first-line therapy in MS when atrial fibrillation is associated with severe symptomatic MS, or even asymptomatic patient with a favorable valve morphology for several reasons.21
In this study, we reported patients with restenosis after PMBC, which has shown to be effective and to provide satisfactory immediate results irrespective of the type of past commissurotomy procedures done. Restenosis with persistent commissural opening is due to valve rigidity and PMBC should not be attempted in these cases.
Follow-up of patients after successful PMBC is similar to that of asymptomatic patients and should be more frequent if asymptomatic restenosis occurs.22 Restenosis is the first indication to consider reintervention. When symptomatic restenosis occurs after surgical commissurotomy or PMBC, reintervention in most cases requires valve replacement, but PMBC can be proposed in selected candidates with favorable characteristics if the predominant mechanism is commissural refusion.37 The success of reintervention largely correlates with elements of the echocardiographic scores, and in particular, with whether or not the commissures have re-fused and look amenable to splitting. Unknown issues include the lack of consideration of the types and extent of commissural fusion, as well as MV calcification, which could directly influence restenosis.
Study limitations. Despite being one of the largest and longest available databases on this subject, this is a retrospective analysis that carries some limitations inherent to this kind of study. In addition, this is a single-center report from a tertiary institution with interventional cardiologists with extensive experience with the procedure; thus, the results obtained may not reflect the practices in other populations worldwide.
Conclusion
Over a very long-term follow-up period, MV restenosis was observed in a quarter of the population submitted to PMBC due to rheumatic mitral stenosis. Preprocedure echocardiographic findings, including left atrial diameter, maximum MV gradient, and higher Wilkins-Block score, were found to be independent predictors of this deleterious event throughout time.
Affiliations and Disclosures
From the 1Department of Interventional Cardiology, Instituto Dante Pazzanese de Cardiologia, Sao Paulo, Brazil; 2Department of Medicine, Universidade Federal de Sergipe, Lagarto, Brazil; 3Centro de Ensino e Pesquisa da Rede Primavera, Aracaju, Brazil; 4Department of Structural Heart Disease, Instituto Dante Pazzanese de Cardiologia, Sao Paulo, Brazil; 5Department of Echocardiography, Instituto Dante Pazzanese de Cardiologia, Sao Paulo, Brazil; 6Interventional Cardiology, Rede D’Or, Sao Paulo, Brazil; and 7Hospital Sao Domingos–Rede DASA, São Luis, Brazil.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript accepted November 18, 2022.
Address for correspondence: J. Ribamar Costa, Jr, MD, PhD, Av. Dante Pazzanese, n. 500, 04012-909, Sao Paulo, Brazil. Email: rmvcosta@uol.com.br
References
1. Inoue K, Owaki T, Nakamura T, Kitamura F, Miyamoto N. Clinical application of transvenous mitral commissurotomy by a new balloon catheter. J Thorac Cardiovasc Surg. 1984;87(3):394-402.
2. Badheka AO, Shah N, Ghatak A, et al. Balloon mitral valvuloplasty in the United States: a 13-year perspective. Am J Med. 2014;127(11):1126.e1-1126.e12. doi:10.1016/j.amjmed.2014.05.015
3. Palacios IF, Block PC, Wilkins GT, Weyman AE. Follow-up of patients undergoing percutaneous mitral balloon valvotomy. Analysis of factors determining restenosis. Circulation. 1989;79(3):573-579. doi:10.1161/01.cir.79.3.573
4. Hernandez R, Banuelos C, Alfonso F, et al. Long-term clinical and echocardiographic follow-up after percutaneous mitral valvuloplasty with the Inoue balloon. Circulation. 1999;99(12):1580-1586. doi:10.1161/01.cir.99.12.1580
5. Kang DH, Park SW, Song JK, et al. Long-term clinical and echocardiographic outcome of percutaneous mitral valvuloplasty: randomized comparison of Inoue and double-balloon techniques. J Am Coll Cardiol. 2000;35(1):169-175. doi:10.1016/s0735-1097(99)00502-1
6. Wang A, Krasuski RA, Warner JJ, et al. Serial echocardiographic evaluation of restenosis after successful percutaneous mitral commissurotomy. J Am Coll Cardiol. 2002;39(2):328-334. doi:10.1016/s0735-1097(01)01726-0
7. Ben-Farhat M, Betbout F, Gamra H, et al. Predictors of long-term event-free survival and of freedom from restenosis after percutaneous balloon mitral commissurotomy. Am Heart J. 2001;142(6):1072-1079. doi:10.1067/mhj.2001.118470
8. Desideri A, Vanderperren O, Serra A, et al. Long-term (9 to 33 months) echocardiographic follow-up after successful percutaneous mitral commissurotomy. Am J Cardiol. 1992;69(19):1602-1606. doi:10.1016/0002-9149(92)90711-7
9. Lau KW, Ding ZP, Quek S, Kwok V, Hung JS. Long-term (36-63 months) clinical and echocardiographic follow-up after Inoue balloon mitral commissurotomy. Cathet Cardiovasc Diagn. 1998;43(1):33-38. doi:10.1002/(sici)1097-0304(199801)43:1<33::aid-ccd9>3.0.co;2-9
10. Vahanian A, Michel PL, Cormier B, et al. Results of percutaneous mitral commissurotomy in 200 patients. Am J Cardiol. 1989;63(12):847-852. doi:10.1016/0002-9149(89)90055-6
11. Chen CR, Cheng TO, Chen JY, Zhou YL, Mei J, Ma TZ. Long-term results of percutaneous mitral valvuloplasty with the Inoue balloon catheter. Am J Cardiol. 1992;70(18):1445-1448. doi:10.1016/0002-9149(92)90297-c
12. Gordon SP, Douglas PS, Come PC, Manning WJ. Two-dimensional and Doppler echocardiographic determinants of natural history of mitral valve narrowing in patients with rheumatic mitral stenosis: implications for follow-up. J Am Coll Cardiol. 1992;19(5):968-973. doi:10.1016/0735-1097(92)90280-z
13. Sagie A, Freitas N, Padial LR, et al. Doppler echocardiographic assessment of long-term progression of mitral stenosis in 103 patients: valve area and right heart disease. J Am Coll Cardiol. 1996;28(2):472-479. doi:10.1016/0735-1097(96)00153-2
14. Abascal VM, Wilkins GT, O'Shea JP, et al. Prediction of successful outcome in 130 patients undergoing percutaneous balloon mitral valvotomy. Circulation. 1990;82(2):448-456. doi:10.1161/01.cir.82.2.448
15. Fawzy ME, Hegazy H, Shoukri M, El Shaer F, ElDali A, Al-Amri M. Long-term clinical and echocardiographic results after successful mitral balloon valvotomy and predictors of long-term outcome. Eur Heart J. 2005;26(16):1647-1652. doi:10.1093/eurheartj/ehi226
16. Iung B, Garbarz E, Michaud P, et al. Late results of percutaneous mitral commissurotomy in a series of 1024 patients. Analysis of late clinical deterioration: frequency, anatomic findings, and predictive factors. Circulation. 1999;99(25):3272-3278. doi:10.1161/01.cir.99.25.3272
17. Dean LS, Mickel M, Bonan R, et al. Four-year follow-up of patients undergoing percutaneous balloon mitral commissurotomy. A report from the National Heart, Lung, and Blood Institute Balloon Valvuloplasty Registry. J Am Coll Cardiol. 1996;28(6):1452-1457. doi:10.1016/s0735-1097(96)00350-6
18. Meneveau N, Schiele F, Seronde MF, et al. Predictors of event-free survival after percutaneous mitral commissurotomy. Heart. 1998;80(4):359-364. doi:10.1136/hrt.80.4.359
19. Palacios IF, Sanchez PL, Harrell LC, Weyman AE, Block PC. Which patients benefit from percutaneous mitral balloon valvuloplasty? Prevalvuloplasty and postvalvuloplasty variables that predict long-term outcome. Circulation. 2002;105(12):1465-1471. doi:10.1161/01.cir.0000012143.27196.f4
20. Wilkins GT, Weyman AE, Abascal VM, Block PC, Palacios IF. Percutaneous balloon dilatation of the mitral valve: an analysis of echocardiographic variables related to outcome and the mechanism of dilatation. Br Heart J. 1988;60(4):299-308. doi:10.1136/hrt.60.4.299
21. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143(5):e35-e71. doi:10.1161/CIR.0000000000000932
22. Vahanian A, Beyersdorf F, Praz F, et al; ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43(7):561-632. doi:10.1093/eurheartj/ehab395
23. Iung B, Cormier B, Ducimetiere P, et al. Immediate results of percutaneous mitral commissurotomy. A predictive model on a series of 1514 patients. Circulation. 1996;94(9):2124-2130. doi:10.1161/01.cir.94.9.2124
24. Feldman T, Herrmann HC, Inoue K. Technique of percutaneous transvenous mitral commissurotomy using the Inoue balloon catheter. Cathet Cardiovasc Diagn. 1994;Suppl 2:26-34.
25. Bonhoeffer P, Piechaud JF, Sidi D, et al. Mitral dilatation with the Multi-Track system: an alternative approach. Cathet Cardiovasc Diagn. 1995;36(2):189-193. doi:10.1002/ccd.1810360224
26. Cribier A, Eltchaninoff H, Carlot R, et al. Percutaneous mechanical mitral commissurotomy with the metallic valvulotome: detailed technical aspects and overview of the results of the multicenter registry on 882 patients. J Interv Cardiol. 2000;13(4):255-262. doi:10.1111/j.1540-8183.2000.tb00300.x
27. Palacios IF. Percutaneous mitral balloon valvuloplasty. In: Sievert H, ed. Percutaneous Interventions for Congenital Heart Disease. London: Informa Healthcare, 2007:177-184.
28. Helmcke F, Nanda NC, Hsiung MC, et al. Color Doppler assessment of mitral regurgitation with orthogonal planes. Circulation. 1987;75(1):175-183. doi:10.1161/01.cir.75.1.175
29. Wang A, Krasuski RA, Warner JJ, Pieper K, Kisslo KB, Bashore TM. Serial echocardiographic evaluation of restenosis after successful percutaneous mitral commissurotomy. J Am Coll Cardiol. 2002;39(2):328-334. doi:10.1016/s0735-1097(01)01726-0
30. Murthy Jayanthi Sriram SN, Venkata BJ, Sadagopan T, Ramamurthy MT. Immediate, intermediate and long term clinical outcomes of percutaneous transvenous mitral commissurotomy. Int J Cardiol Heart Vasc. 2015;6:66-70. doi:10.1016/j.ijcha.2015.01.006
31. Fawzy ME, Fadel B, Al-Sergani H, et al. Long-term results (up to 16.5 years) of mitral balloon valvuloplasty in a series of 518 patients and predictors of long-term outcome. J Interv Cardiol. 2007;20(1):66-72. doi:10.1111/j.1540-8183.2007.00212.x
32. Bouleti C, Iung B, Laouenan C, et al. Late results of percutaneous mitral commissurotomy up to 20 years: development and validation of a risk score predicting late functional results from a series of 912 patients. Circulation. 2012;125:2119-2127. doi:10.1161/CIRCULATIONAHA.111.055905
33. Song JK, Song JM, Kang DH, et al. Restenosis and adverse clinical events after successful percutaneous mitral valvuloplasty: immediate post-procedural mitral valve area as an important prognosticator. Eur Heart J. 2009;30(10):1254-1262. doi:10.1093/eurheartj/ehp096
34. Bouleti C, Iung B, Himbert D, et al. Long-term efficacy of percutaneous mitral commissurotomy for restenosis after previous mitral commissurotomy. Heart. 2013;99(18):1336-1341. doi:10.1136/heartjnl-2013-303944
35. Hildick-Smith DJ, Taylor GJ, Shapiro LM. Inoue balloon mitral valvuloplasty: long-term clinical and echocardiographic follow-up of a predominantly unfavourable population. Eur Heart J. 2000;21(20):1690-1697. doi:10.1053/euhj.2000.2241
36. Iung B, Leenhardt A, Extramiana F. Management of atrial fibrillation in patients with rheumatic mitral stenosis. Heart. 2018;104(13):1062-1068. doi:10.1136/heartjnl-2017-311425
37. Bouleti C, Iung B, Himbert D, et al. Reinterventions after percutaneous mitral commissurotomy during long-term follow-up, up to 20 years: the role of repeat percutaneous mitral commissurotomy. Eur Heart J. 2013;34(25):1923-1930. Epub 2013 Mar 20. doi:10.1093/eurheartj/eht097