


Initial Experiences of Percutaneous Coronary Intervention Using a New-Generation Everolimus-Eluting Stent Platform
Abstract
Background. Outcomes from the new Synergy Megatron drug-eluting stent (DES) platform (Boston Scientific) are not yet reported. This study sought to evaluate periprocedural outcomes in patients undergoing percutaneous coronary intervention (PCI) using this technology. Methods. This was a retrospective study across two United Kingdom centers of 139 patients undergoing PCI of 146 coronary lesions using the Synergy Megatron DES. The primary endpoint was the rate of cardiovascular death. The secondary endpoint was the rate of a composite of non-fatal myocardial infarction, target-vessel revascularization, in-stent restenosis, and probable/definite stent thrombosis. Available intravascular ultrasound (IVUS) imaging was reviewed post hoc and evaluated according to predefined IVUS optimization criteria. Results. Mean follow-up duration was 137.3 ± 38.3 days. The primary endpoint occurred in 0.7% of patients and the secondary endpoint occurred in 0.0% of patients. There were no cases of longitudinal stent deformation (LSD); in patients undergoing an IVUS-guided procedure, our criteria for successful IVUS optimization was achieved in 74.1% of left main stem (LMS) and 83.3% of right coronary artery (RCA) lesions. Mean minimal stent area (MSA) was 14.5 ± 3.4 mm2 in the LMS, 10.0 ± 2.5 mm2 in the left anterior descending coronary artery, 9.8 ± 3.0 mm2 in the left circumflex, and 12.2 ± 4.0 mm2 in the RCA. Conclusion. This study demonstrated very low rates of short-term major adverse cardiovascular events with no cases of LSD or acute/subacute stent thrombosis. It highlights the overexpansion capabilities of the Synergy Megatron DES platform. The technology safely and effectively facilitates IVUS-optimized stent parameters for the treatment of large proximal vessels and bifurcations.
J INVASIVE CARDIOL 2021;33(10):E784-E790.
Key words: device innovations, new-generation drug-eluting stent, new technology
Introduction
The use of intravascular ultrasound (IVUS) to guide percutaneous coronary intervention (PCI) has been associated with an improved prognosis in several studies.1-11 Current European guidelines recommend that IVUS should be considered in patients undergoing PCI (class IIa recommendation).12 In 2020, De La Torre Hernandez et al demonstrated that clinical outcomes can be improved in left main stem (LMS) PCI not only through the use of IVUS, but particularly when applying a detailed IVUS protocol comprising a set of predefined optimization criteria.13
Shand et al demonstrated that the majority of patients with angiographic coronary atheroma have a mean LMS diameter of >4 mm, indicating the requirement for postdilation beyond the nominal diameter of current-generation drug-eluting stent (DES) devices in almost all patients when treating the LMS.14 All modern stent technology is limited by an upper limit to their overexpansion capabilities. Use of postdilation balloons that exceed this upper limit may risk damage to the drug coating integrity, stent fracture, and incomplete stent apposition.15 Incomplete stent apposition has been associated with an increased risk of in-stent restenosis (ISR) and stent thrombosis.16 The treatment of coronary bifurcations and significantly tapered vessels is therefore made challenging by a significant mismatch in proximal and distal reference diameters.
The Synergy Megatron DES platform (Boston Scientific), in comparison with the preceding Synergy DES platform, offers improved overexpansion capabilities as well as superior axial and radial strength for the treatment of tapered proximal vessels and bifurcations. Real-world clinical outcomes in patients undergoing PCI with this technology are yet to be reported. In this study, we present both the periprocedural clinical outcomes and available IVUS parameters following PCI using this DES platform.
Methods
Population. This was a retrospective study conducted across 2 United Kingdom centers offering elective, urgent, and emergency PCI. All patients with previous PCI in these centers using ≥1 Synergy Megatron DES device either in isolation or in addition to other Synergy stent technology were considered eligible. There were no exclusion criteria. IVUS guidance was defined as either use prior to stent deployment for procedural planning or use following stent deployment for optimization.
Data collection and IVUS analysis. All patient demographics, procedural details, and clinical outcome data were collected retrospectively using national electronic healthcare records and procedural logs. Coronary angiograms and IVUS imaging were reviewed post hoc using iReview image viewer software (Boston Scientific). This review was conducted by independent interventional cardiologists/fellows not involved with the indexed procedures. All treatment and clinical decision-making processes were subject to the interventional cardiologists performing the procedures and not affected by this study. Written informed consent was not required as this was a retrospective analysis with no impact on patient management.
For patients with available poststent implantation IVUS imaging, final PCI results were evaluated according to an IVUS optimization protocol adapted from the method published by De La Torre Hernandez et al.13 This optimization criteria had been previously used for LMS interventions only, but relevant IVUS parameters were applied to all coronaries evaluated in the present study.
IVUS optimization criteria.13 There were 4 areas used to define procedural success by IVUS assessment:
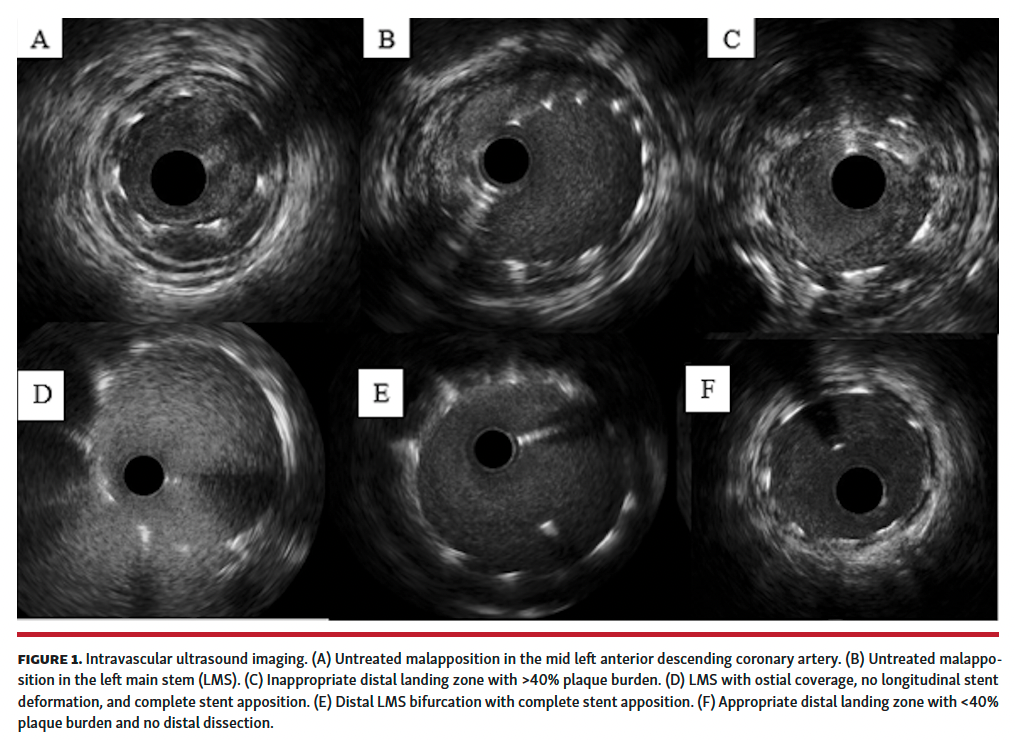
1. Complete stent apposition (Figure 1) was defined as the absence of any IVUS evidence of malapposition. Malapposition was defined as any separation of ≥1 stent strut from the intimal surface of the arterial wall with evidence of blood behind the strut, without involvement of sidebranches. If malapposition was detected and further postdilation was performed with an appropriately sized balloon as per IVUS sizing, but IVUS was not repeated, stent apposition was considered to be complete.
2. Absence of longitudinal stent deformation (LSD). LSD was defined as multiple layers of stent struts seen in any single cross-section within a single stent.
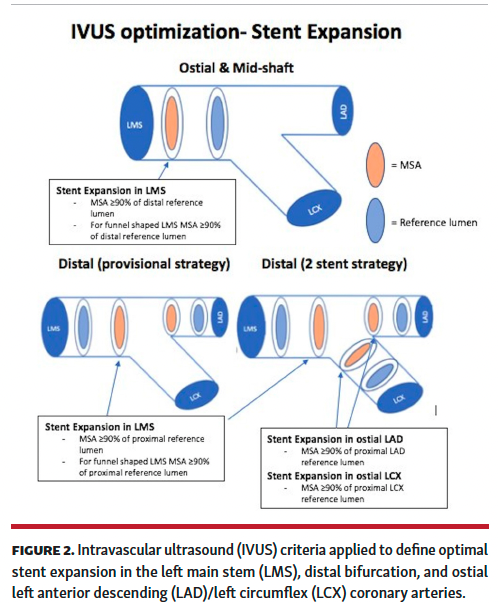
3. Optimal stent expansion (Figure 2). Optimal LMS stent expansion was defined as follows:
(a) Ostial and mid-shaft LMS lesions: expansion >90% of the distal reference lumen in the LMS (>80% if funnel-shaped LMS).
(b) Distal LMS lesions: expansion >90% of the proximal reference lumen in the LMS (>80% if markedly tapered LMS).
(c) In cases showing diffuse LMS disease, the estimated hypothetical reference lumen was equivalent to 90% of the smallest vessel area in the LM. The goal was to attain at least 90% of the expansion according to the selected hypothetical reference lumen.
The morphological shape of the LMS was estimated visually and no quantitative metrics were used to categorize the LMS as funnel shaped, although an angiographic difference >0.5 mm between the proximal and distal LMS was generally the threshold for this visual classification.
Optimal stent expansion at the ostial left anterior descending (LAD) and left circumflex (LCX) coronary arteries were defined as >90% of the reference lumen in the proximal LAD and LCX, respectively. Optimal stent expansion of the right coronary artery (RCA) was defined as >90% of the reference lumen in the distal RCA.
4. Appropriate distal landing zone (Figure 1) was defined as a distal stent edge with residual plaque burden <40% and the absence of dissection or hematoma.
Clinical endpoints and definitions. The primary endpoint was the rate of cardiovascular death. The secondary endpoint was the rate of a composite of non-fatal myocardial infarction (MI), target-vessel revascularization, in-stent restenosis, and definite/probable stent thrombosis. The definition of non-fatal MI was in accordance with the 2018 European Society of Cardiology fourth universal definition of MI.17 Target-vessel revascularization was defined as any unplanned repeat percutaneous or surgical revascularization procedure involving the treated vessel. In-stent restenosis was defined as any repeat coronary angiogram demonstrating >50% stenosis within the previously stented segment or a documented hemodynamically significant area of restenosis by physiological assessment.
Statistical analysis. SPSS for Apple iOS, version 26 was used for all analyses. Continuous variables were described using the mean and standard deviation of the mean for the variable. Categorical variables were described as a number and percentage of the total category number to which the variable belonged.
Results
Between October 2019 and July 2020, a total of 139 patients underwent PCI of 146 coronary lesions using the Synergy Megatron DES platform. Mean follow-up duration was 137.3 ± 38.3 days. There were 0 patients lost to follow-up.
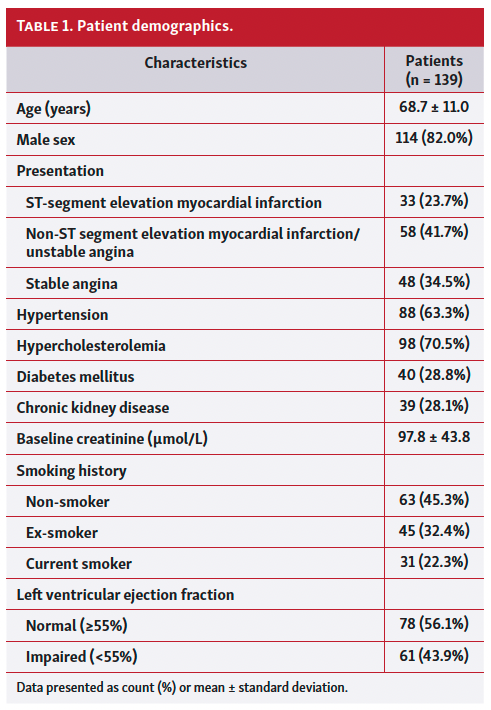
Baseline patient demographics are displayed in Table 1. There were 114 male patients (82.0%). Mean age was 68.7 ± 11.0 years. A total of 48 patients (34.5%) presented with stable angina and 91 (65.5%) presented with an acute coronary syndrome (36.3% ST-segment elevation MI [STEMI] vs 63.7% non-ST segment elevation MI [NSTEMI]/unstable angina). Baseline left ventricular ejection fraction was at least mildly impaired (<55%) in 43.9% and severely impaired (<35%) in 11.5% of patients.
Of the 146 lesions treated, 89 (61.0%) involved the LMS, 18 (12.3%) involved the LAD or LCX arteries in isolation, and 39 (26.7%) involved the RCA. The mean number of Synergy Megatron stents per procedure was 1.3 ± 0.6.
Procedures were IVUS guided in 111 patients (79.9%). The rate of IVUS in these patients was 66.7% prior to stent deployment for procedural planning, 96.4% post stent deployment for optimization, and 63.1% both pre and post stent deployment.
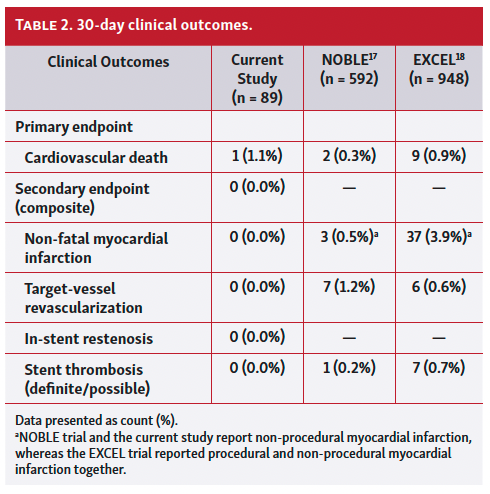
The primary endpoint occurred in 1 patient (0.7%). This periprocedural mortality occurred in the setting of a cardiogenic shock anterior STEMI presentation complicated by severe left ventricular systolic dysfunction. The mortality was due to irrecoverable left ventricular dysfunction and not stent thrombosis. The secondary endpoint occurred in 0 patients (0.0%). Table 2 demonstrates periprocedural clinical outcomes in the LMS cohort of our study within 30 days of the indexed procedure in comparison with the available data from the NOBLE and EXCEL trials.18,19
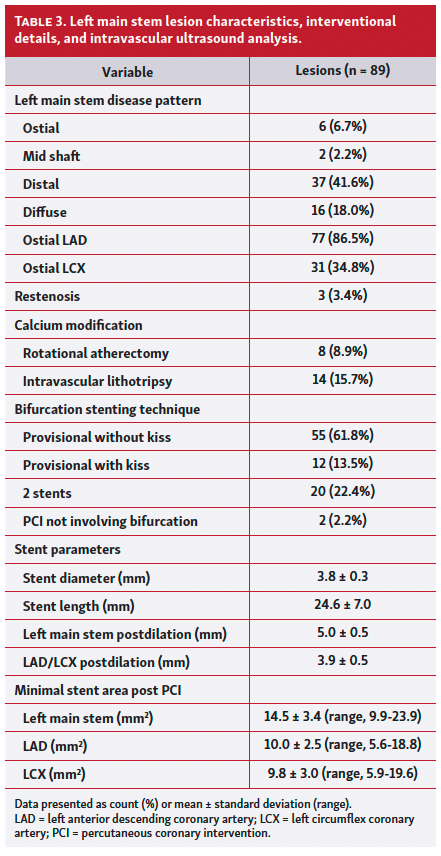
Table 3 demonstrates LMS lesion characteristics, interventional details, and IVUS analysis. The LMS lesions were treated with a provisional strategy in 75.3% of patients and a 2-stent strategy in 22.4% of patients (the remaining 2.2% of PCIs did not involve the distal LMS bifurcation). Advanced calcium-modification techniques were used in 24.7% of patients (15.7% intravascular lithotripsy and 8.9% rotational atherectomy).
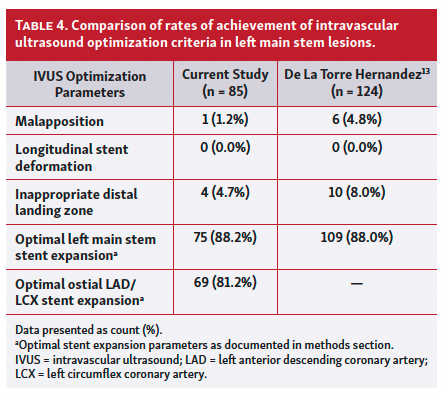
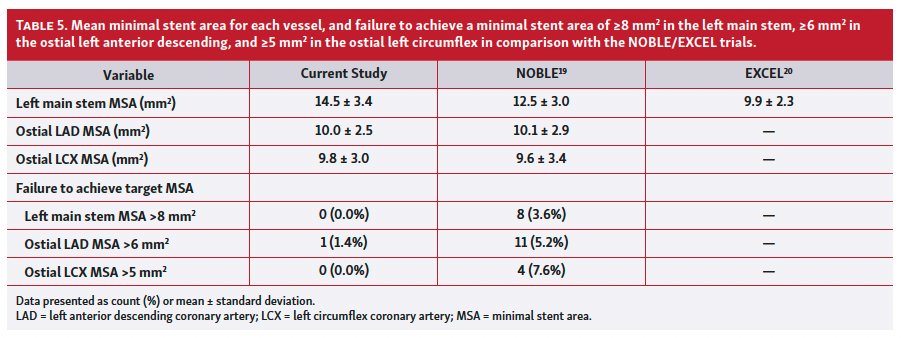
Mean minimal stent area (MSA) was 14.5 ± 3.4 mm2 in the LMS (range, 9.9-23.9 mm2), 10.0 ± 2.5 mm2 in the LAD (range, 5.6-18.8 mm2), and 9.8 ± 3.0 mm2 (range, 5.9-19.6 mm2) in the LCX. Table 4 and Table 5 demonstrate a comparison of IVUS outcomes between data from De La Torre Hernandez et al13 and available data from NOBLE and EXCEL trial substudies.20,21 The IVUS optimization criteria for stent apposition, LSD, stent expansion, and an appropriate distal landing zone were met in 74.1% of IVUS-guided LMS interventions.
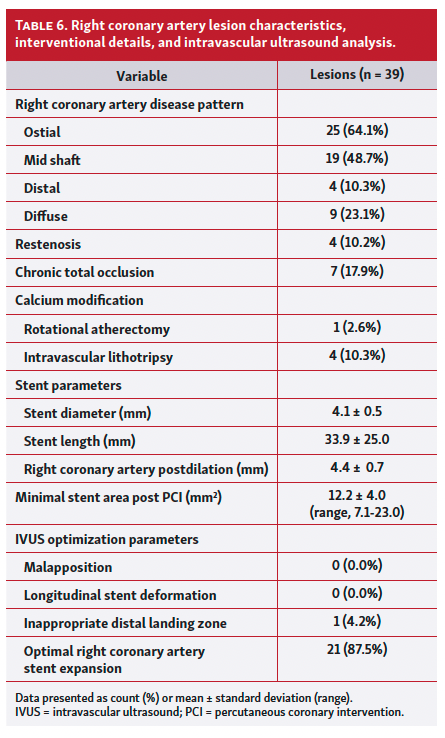
Table 6 demonstrates RCA lesion characteristics, interventional details, and IVUS analysis. Chronic total occlusion procedures accounted for 17.9% of the RCA interventions. Advanced calcium-modification techniques were used in 12.8% of RCA cases (10.3% intravascular lithotripsy and 2.6% rotational atherectomy). Mean MSA was 12.2 ± 4.0 mm2 in the RCA (range, 7.1-23.0 mm2). The IVUS optimization criteria for stent apposition, LSD, stent expansion, and an appropriate distal landing zone were met in 83.3% of IVUS-guided RCA interventions.
Discussion
To the best of our knowledge, this is the first report of periprocedural outcomes using the Synergy Megatron DES platform. We have demonstrated that this technology can achieve high rates of IVUS optimization targets for stent apposition, expansion, appropriateness of landing zones, and absence of LSD even in the absence of such targets being applied in a prospective manner.
Previous studies have demonstrated modest rates of achievement of similar targets for IVUS-optimized procedures. This has been predominantly driven by failure to achieve optimal stent expansion with the aggressive target of an MSA ≥90% of the reference lumen in most studies. In the ULTIMATE trial, the predefined IVUS optimization criteria required the following: MLA in the stented segment >5.0 mm2 or 90% of the MLA at the distal reference segments; plaque burden 5 mm proximal or distal to the stent edge <50%; and no edge dissection involving the media with a length >3 mm. All criteria were achieved in only 53.0% of lesions treated.1 In the AVID trial, only 43.5% of patients met all criteria for IVUS optimization; this was predominantly driven by underexpansion, with only 48.2% of patients achieving the target ≥90% of the cross-sectional area of the distal reference vessel.7 In the IVUS XPL trial, the definition of successful stent expansion was even more strict, aiming for an MSA greater than the distal reference segment, and was achieved in 54.0% of patients.2 In the ILUMIEN III trial, which compared optical coherence tomography (OCT)-guided PCI with both IVUS and angiographic guidance, the rate of ≥90% stent expansion was only 42.0% in the OCT cohort and 37.0% in the IVUS cohort.22
These modest rates of achievement of targets for stent expansion in the above trials do raise the question as to whether a target of 90% stent expansion is either necessary or realistic in highly calcific coronary lesions. It is noteworthy that the application of predefined IVUS optimization stent-expansion criteria led to achievement of these targets in a significantly increased proportion of patients as compared with the use of IVUS alone (88.0% vs 64.5%, respectively; P<.01).13
In 2011, Kang et al published the ability of stent area at the LMS bifurcation to predict the probability of restenosis and adverse cardiac events. This study found the MSA cut-offs that best predicted in-stent restenosis on a segmental basis were 5.0 mm2 in the ostial LCX, 6.3 mm2 in the ostial LAD, 7.2 mm2 within the polygon of confluence, and 8.2 mm2 within the LMS above the polygon of confluence.23 In our study, 98.8% of patients with available IVUS imaging achieved this target using the Synergy Megatron DES platform. However, the NOBLE and EXCEL substudies would suggest that these criteria are inadequate for a Caucasian population.
The NOBLE trial demonstrated that target-lesion revascularization was reduced by both the performance of post-PCI IVUS (5.1% vs 11.6%; P=.01) and the achievement of a large (13.4-25.4 mm2) vs a small (<10.9 mm2) LMS MSA (0.0% vs 12.2%; P<.01).20 In the EXCEL trial, a small final LMS MSA was strongly associated with major adverse cardiovascular events, with the composite endpoint of death, MI, and stroke significantly higher in the smallest vs largest MSA tertiles (19.4% vs 9.6%; P=.01).21
In this smaller study, we have documented the ability of the Synergy Megatron platform to produce a mean LMS MSA that is numerically superior to both the EXCEL and NOBLE trials (14.5 ± 3.4 mm2 vs 12.5 ± 3.0 mm2 vs 9.9 ± 2.3 mm2, respectively). In the NOBLE trial, 8.5% of patients with post-PCI IVUS failed to achieve at least 1 of the MSA targets set out by Kang et al.18 In our study, only 1.2% of patients failed to achieve these targets. A comparison of short-term outcomes in the LMS cohort of this study with both of the EXCEL and NOBLE trials seems to suggest similar if not marginally favorable outcomes in the PCI cohorts of these studies. This is particularly notable given the high rates of acute coronary syndrome presentations in our study (64.9%) in comparison with NOBLE (18.0%) and EXCEL (38.8%).
This platform provides a broad overexpansion range (3.5-6.0 mm) to overcome the issue of significant mismatch between proximal and distal vessel diameters. Most commonly, this difficulty arises during LMS bifurcation intervention and hence there is the potential for dedicated technologies to improve outcomes in a population of patients with a large amount of jeopardized myocardium. The axial and radial strength allow for the successful treatment of heavily calcified, fibrotic, and ostial lesions, with a theoretical reduction in the rate of LSD. Uncorrected LSD in EXCEL was not infrequent, occurring in 6.6% of analyzable final IVUS images. In addition, LSD was associated with adverse outcomes, with a significant increase in the 3-year rate of cardiac death/MI/ischemia-driven target-lesion revascularization (28.3% vs 13.9%; P=.02).24
Study limitations. This study has inherent limitations given the retrospective nature of data analyzed. In addition, there was no control group for comparison with other stent technology. The short follow-up period and relatively small number of patients in this study limit conclusions that can be drawn and mean that it is underpowered to detect events such as stent thrombosis. IVUS analysis of LMS PCI is compared with results from the NOBLE and EXCEL trials. These trials performed core-lab IVUS analysis, which was not possible in this smaller retrospective study.
In this study, patients were included who had PCI using Synergy stents alongside the Synergy Megatron platform. This potentially dilutes the conclusions that can be drawn from this study; however, it reflects real-world practice using this platform. Longer-term follow-up of patients will be required to confirm the conclusions drawn. However, short-term outcomes using this platform appear to be promising and would advocate its use.
Conclusion
This study confirms the overexpansion capabilities of the Synergy Megatron DES platform. This technology safely and effectively facilitates IVUS-optimized stent parameters for the treatment of large proximal vessels and demonstrates acceptable acute performance for the IVUS-optimized treatment of LMS bifurcations.
Affiliations and Disclosures
From the 1Royal Victoria Hospital, Belfast, United Kingdom; and 2St George’s University Hospital, London, United Kingdom.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Cosgrove reports honoraria from Boston Scientific. Dr Spratt and Dr Spence report consulting fees, honoraria, and support for attending meetings and/or travel from Boston Scientific. Dr Walsh reports consulting fees and honoraria from Boston Scientific. The authors report no conflicts of interest regarding the content herein.
Manuscript accepted December 7, 2020.
The authors report patient consent for the images used herein.
Address for correspondence: Jonathan Andrew Mailey, MBChB, FRCP, Cardiology Department, Royal Victoria Hospital, 274 Grosvenor Road, Belfast, BT12 6BA. Email: jonathan.mailey@belfasttrust.hscni.net
References
1. Zhang J, Gao X, Kan J, et al. Intravascular ultrasound versus angiography-guided drug-eluting stent implantation: the ULTIMATE trial. J Am Coll Cardiol. 2018;72:3126-3137.
2. Hong SJ, Kim BK, Shin DH, et al. Effect of intravascular ultrasound-guided vs angiography-guided everolimus-eluting stent implantation: the IVUS-XPL randomized clinical trial. JAMA. 2015;314:2155-2163.
3. Park SJ, Kim YH, Park DW, et al. Impact of intravascular ultrasound guidance on long-term mortality in stenting for unprotected left main coronary artery stenosis. Circ Cardiovasc Interv. 2009;2:167-177.
4. De la Torre Hernandez JM, Baz Alonso JA, Gómez Hospital JA, et al. Clinical impact of intravascular ultrasound guidance in drug-eluting stent implantation for unprotected left main coronary disease pooled analysis at the patient-level of 4 registries. JACC Cardiovasc Interv. 2014;7:244-254.
5. Gao XF, Kan J, Zhang YJ, et al. Comparison of one-year clinical outcomes between intravascular ultrasound guided versus angiography-guided implantation of drug-eluting stents for left main lesions: a single-center analysis of a 1,016-patient cohort. Patient Prefer Adherence. 2014;8:1299-1309.
6. Tan Q, Wang Q, Liu D, et al. Intravascular ultrasound guided unprotected left main coronary artery stenting in the elderly. Saudi Med J. 2015;36:549-553.
7. Russo RJ, Silva PD, Teirstein PS, et al. A randomized controlled trial of angiography versus intravascular ultrasound-directed bare-metal coronary stent placement (the AVID trial). Circ Cardiovasc Interv. 2009;2:113-123.
8. Tian J, Guan C, Wang W, et al. Intravascular ultrasound guidance improves the long-term prognosis in patients with unprotected left main coronary artery disease undergoing percutaneous coronary intervention. Sci Rep. 2017;7:2377.
9. Andell P, Karlsson S, Mohammad MA, et al. Intravascular ultrasound guidance is associated with better outcome in patients undergoing unprotected left main coronary artery stenting compared with angiography guidance alone. Circ Cardiovasc Interv. 2017;10:e004813.
10. Liu XM, Yang ZM, Liu XK, et al. Intravascular ultrasound-guided drug-eluting stent implantation for patients with unprotected left main coronary artery lesions: a single-center randomized trial. Anatol J Cardiol. 2019;21:83-90.
11. Wang Y, Mintz GS, Gu Z, et al. Meta-analysis and systematic review of intravascular ultrasound versus angiography-guided drug eluting stent implantation in left main coronary disease in 4592 patients. BMC Cardiovasc Disord. 2018;18:115.
12. Neumann FJ, Sousa-Uva M, Ahlsson A, et al. ESC Scientific Document Group. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. 2019;40:87-165.
13. De la Torre Hernández JM, García Camarero T, Baz Alonso JA, et al. The application of predefined optimization criteria for intravascular ultrasound guidance of left main stenting improves outcomes. EuroIntervention. 2020;16:210-217.
14. Shand JA, Sharma D, Hanratty C, et al. A prospective intravascular ultrasound investigation of the necessity for and efficacy of postdilation beyond nominal diameter of 3 current generation DES platforms for the percutaneous treatment of the left main coronary artery. Catheter Cardiovasc Interv. 2014;84:351-358. Epub 2013 Nov 9.
15. Ng J, Foin N, Ang HY, et al. Over-expansion capacity and stent design model: an update with contemporary DES platforms. Int J Cardiol. 2016;221:171-179.
16. Noad RL, Hanratty CG, Walsh SJ. Clinical impact of stent design. Interv Cardiol. 2014;9:89-93.
17. Thygesen K, Alpert JS, Jaffe AS, et al. ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Circulation. 2018;138:e618-e651.
18. Mäkikallio T, Holm NR, Lindsay M, et al. Percutaneous coronary angioplasty versus coronary artery bypass grafting in treatment of unprotected left main stenosis (NOBLE): a prospective, randomised, open-label, non-inferiority trial. Lancet. 2016;388:2743-2752.
19. Stone GW, Sabik JF, Serruys PW, et al. Everolimus-eluting stents or bypass surgery for left main coronary artery. N Engl J Med. 2016;375:2223-2235.
20. Ladwiniec A, Walsh SJ, Holm NR, et al. Intravascular ultrasound to guide left main stem intervention: a NOBLE trial substudy. EuroIntervention. 2020;16:201-209.
21. Maehara A, Mintz G, Serruys P, et al. Impact of final minimal stent area by IVUS on 3-year outcome after PCI of left main coronary artery disease: the Excel trial. J Am Coll Cardiol. 2017;69(11 Suppl):963.
22. Ali ZA, Maehara A, Généreux P, et al. Optical coherence tomography compared with intravascular ultrasound and with angiography to guide coronary stent implantation (ILUMIEN III: OPTIMIZE PCI): a randomised controlled trial. Lancet. 2016;388:2618-2628.
23. Kang SJ, Ahn JM, Song H, et al. Comprehensive intravascular ultrasound assessment of stent area and its impact on restenosis and adverse cardiac events in 403 patients with unprotected left main disease. Circ Cardiovasc Interv. 2011;4:562-569.
24. Kim SY, Maehara A, Merkely B, et al. Frequency and impact of acute stent deformation after PCI of left main coronary artery disease: an EXCEL trial intravascular ultrasound substudy. J Am Coll Cardiol. 2017;70(18 Suppl):B19.













