


Outcomes Following Coronary Chronic Total Occlusion Revascularization With Drug-Coated Balloons
Abstract
Objectives. Despite the introduction of improved drug eluting stents (DES), the rate of repeat revascularization procedures following percutaneous coronary interventions (PCI) in coronary chronic total occlusions (CTO) remains high. By leaving vessels uncaged and limiting length of stented segments, drug-coated balloons (DCB) represent an appealing alternative to DES for CTO-PCI. Since data supporting the use of DCBs in CTO-PCI is scarce, we compared the outcomes of patients undergoing CTO-PCI involving DCBs vs DES only.
Methods. From 2 prospective registries, outcomes of patients undergoing CTO-PCI involving DCBs and those undergoing PCI with DES only were compared. Outcomes included major adverse cardiac and cerebrovascular events (MACCE) and cardiovascular death (CV-death).
Results. Overall, 157 patients were studied; 112 (71%) underwent CTO-PCI involving DCBs and 45 (29%) were treated with DES only. Mean J-CTO score was 1.84 ± 0.7. Most CTO-lesions involved the right coronary artery, 88 (56%), and 26 (17%) cases were in-stent occlusions. In the DCB group, 46 (41%) lesions were treated with DCBs alone. Mean lengths of the stented segments in the DCB vs DES cohorts were 59 ± 28 mm vs 87 ± 37 mm (P<.001), respectively. After 12 months, the MACCE rate was higher in the DES only vs DCB group (26% vs 11%, P=.03). Length of the stented segment was an independent predictor for MACCE (HR 1.15 [95% CI, 1.05-1.26] per 10-mm stent length).
Conclusions. Revascularization of CTO lesions involving DCBs appears safe and potentially lowers MACCE rates compared to treatment with DES alone. Importantly, using DCBs for CTO treatment may reduce total stent length, which determines PCI outcomes.
Introduction
Despite improved chronic total occlusion (CTO)-percutaneous coronary intervention (PCI) techniques and use of modern stent platforms, the rate of target lesion failure (TLF) and repeat revascularization procedures due to target vessel revascularization (TVR) among patients with CTO lesions remains high.1 In-stent restenosis (ISR) and TVR rates between 5% and 30% after 12 months have been reported in recent studies.2-4
The factors leading to the high ISR and TVR rates following CTO-PCI appear multifaceted. Aside from patient factors (eg, higher diabetes prevalence), several histopathological features commonly encountered in coronary CTOs contribute to the higher rates of stent failure. These features include the presence of extensive calcifications and long-diseased segments, among others.5,6 Moreover, following CTO-PCI, vessels tend to undergo positive remodeling, which can lead to stent under expansion and malposition following stent implantation.6-8 Erroneously, presuming that the vascular healing, and thus clinical outcomes, following stent implantation in CTO and non-CTO lesions are similar, interventional cardiologists tend to apply uniform stenting approaches for both lesion types and may neglect the afore-mentioned issues, which contributes to the elevated risk for adverse events following CTO-PCI.4
Following the encouraging results of randomized trials supporting the use of drug-coated balloons (DCB) in the treatment of ISR and native coronary lesions (up to 3 mm), there has been some interest to test DCBs in CTO lesions as well.9-12 However, studies comparing CTO treatment strategies involving DCBs to those with DES only remain scarce.12 Hypothetically, DCBs have the potential to overcome some of the limitations seen with use of contemporary drug-eluting stents (DES) in CTO-PCI since they leave the vessel uncaged (implant-free), allowing it to positively remodel over time.13
With this background, our study aimed to describe the safety and long-term outcomes of patients with coronary CTOs undergoing PCI with the latest generation of DCBs vs novel DES.
Methods
Study population. We analyzed consecutive patients undergoing successful CTO-PCI involving DCBs who were enrolled in the prospective SIROOP (Prospective Registry Study to Evaluate the Outcomes of Coronary Artery Disease Patients Treated With SIROlimus Or Paclitaxel Eluting Balloon Catheters) Registry (NCT04988685).14 For comparison, we included CTO patients who had undergone successful CTO-PCI with DES only and were enrolled in the COMPLEX (A Prospective Cohort Study to Describe the Management and Outcomes of Patients Presenting with Complex calcified coronary lesions) Registry (NCT06075602). Both studies complied with the Declaration of Helsinki and were approved by the regional ethics committee (BASEC IDs 2021-00615 and 2021-01290, respectively).
In brief, the SIROOP Registry was designed to describe the management and outcomes of patients undergoing PCI with contemporary DCBs, whereas the aim of the COMPLEX Registry was to assess the practice and outcomes of patients presenting with complex and calcified coronary artery lesions (eg, CTO and heavily calcified coronary lesions).14 All patients were enrolled at the Heart Center of the Luzerner Kantonsspital (Lucerne, Switzerland), which represents the tertiary cardiology facility for the central part of Switzerland (annual CTO-PCI volume: approximately 200 dedicated CTO-PCI cases).
Data collection and follow-up. From every study participant, demographic and procedural data were entered in a dedicated database (REDCap, Version 10.6.28;Vanderbilt University) Of note, patients with unsuccessful percutaneous CTO revascularization were excluded from this study. Clinical follow-up information was obtained from the studied subjects by clinic visits or telephone interviews at 30 days, 6 months, 1 year, and 2 years after the index procedure.
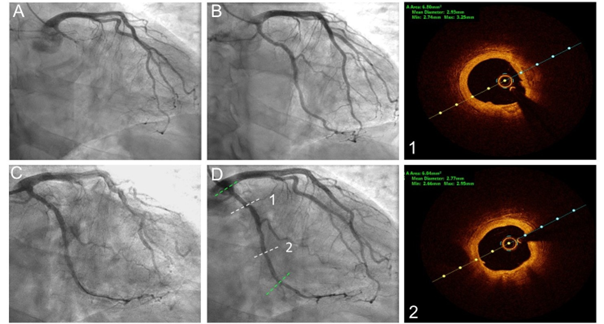
PCI procedures. For PCI procedures at our institution, we follow the international guideline recommendations.15-17 For CTO-PCIs, we apply commonly recommended crossing techniques (eg, wire escalation, parallel wire techniques, controlled antegrade and retrograde subintimal tracking [CART] technique) using an antegrade or bi-directional approach, as needed.18 To achieve optimal visualization of the distal target, we use bilateral injections in almost all CTO interventions. Following successful CTO crossing, our internal practice recommendations encourage liberal use of intravascular imaging (intravascular ultrasound [IVUS] or optical coherence tomography [OCT]) to plan lesion preparation and treatment. We almost routinely use cutting balloons and/or non-compliant (NC) balloons for lesion preparation, especially in coronary cases involving DCBs.14 This practice is in line with the third DCB consensus paper.19
Patients enrolled in the SIROOP registry had their CTO lesions treated with the latest generation DCBs — and DES if needed — following successful lesion preparation and in the absence of major complications (eg, > 30% residual stenosis, flow limiting dissections, or menacing abrupt vessel closure).14 We used the following DCB devices: Selution SLR (MedAlliance), SeQuent Please NEO and SeQuent SCB (B.Braun), MagicTouch (Concept Medical), and Prevail (Medtronic). The devices were used according to each manufacturer’s instructions for use. Whenever possible, we attempted to inflate the DCB for at least 45 seconds (optimally ≥ 90-120 seconds) to achieve optimal drug transmission to the treated vessel segments. In DCB cases, bailout stenting was defined as a requirement to implant a DES to ensure vessel patency and/or restore flow (eg, > 30% residual stenosis, flow limiting dissections, or menacing abrupt vessel closure) following treatment with at least one of the afore-mentioned DCB devices. A hybrid approach was defined as lesions that required direct implantation of DES following predilatation (eg, due to recoil or deep dissections) while the rest of the vessel was treated with DCBs.
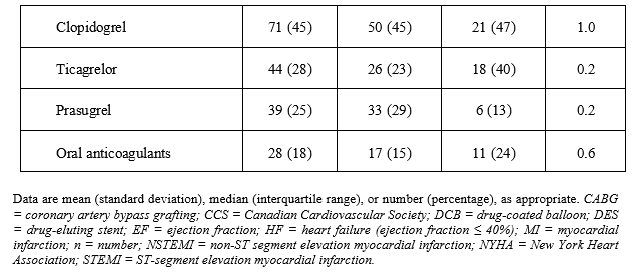
Antithrombotic treatment. Regarding the applied antithrombotic regimens, we followed the current guidelines.15,16,19 We ensured that all patients were pretreated with aspirin prior to PCI, if tolerated. At the discretion of the treating physician, the patients were loaded with clopidogrel, ticagrelor, or prasugrel during or following PCI. PCI was performed using heparin (70-100 units/kg body weight, target activated clotting time [ACT] >230-250 seconds during PCI). In case of DCB-only treatment, the duration of dual antiplatelet therapy (DAPT) varied between 1 and 3 months, which was determined by the Third Report of the International DCB Consensus Group and the patient’s bleeding and thrombotic risk.19 Otherwise, in case of stent implantation the duration of DAPT was generally between 6 and 12 months, according to the latest guidelines.15 In patients who required anticoagulation, we recommended the use of a novel oral anticoagulant in combination with aspirin for 1 week, as well as clopidogrel.
Angiographic analyses and event adjudication. All angiograms were reviewed by 2 independent reviewers (VG and EG). CTOs were defined as completely occluded coronary arteries without antegrade coronary flow with a duration of more than 3 months.20 Occlusions located within a previously implanted stent or up to 5 mm from the edge of the stent were defined as in-stent-CTO.21 CTO complexity was classified according to the Japanese (J)-CTO score.22 Dissections were classified according to the National Heart, Lung and Blood Institute classification system for intimal tears, consisting of Types A through F.23
Study outcomes. For this study, we defined major adverse cardiac and cerebrovascular events (MACCE) as a composite of cardiovascular death, target lesion revascularization (TLR), target vessel myocardial infarction (TV-MI), and stroke. Other outcomes of interest included target lesion target vessel revascularization (TVR), new myocardial infarction (MI), stent thrombosis (ST), and all-cause death. For definitions, we followed the criteria of the Academic Research Consortium (ARC).24 Heart failure (HF) was defined as having a left ventricular ejection fraction (LVEF) of less than 40%. Also, we collected detailed information on any periprocedural complications (eg, coronary perforations, urgent coronary artery bypass grafting [CABG], bleedings, and strokes). Procedural success was defined as a residual stenosis of less than 30% remaining after PCI with a Thrombolysis in Myocardial Infarction (TIMI) flow grade 3 at the end of the procedure, and freedom from any major procedure-related complication. All outcomes were independently adjudicated by 2 experienced physicians who were not involved in the procedures (MM and GMC).
Statistical method. Categorical variables are displayed as frequencies and percentages, while continuous variables are presented as mean (± SD) or median (Interquartile range, IQR), as appropriate. P-values were calculated using Pearson’s chi-square test or Fisher exact test for categorical variables and Student’s t-test or Wilcoxon rank-sum test for continuous variables, as applicable, and adjusted using the Benjamini and Hochberg method. Gray's test was used to compare cumulative rates of outcomes, while factor associations with outcomes were evaluated using Cox proportional hazards regression model. A 2-tailed P-value of less than .05 was considered statistically significant. The analyses were conducted using R version 4.2.2 (R Core Team, 2022).
Results
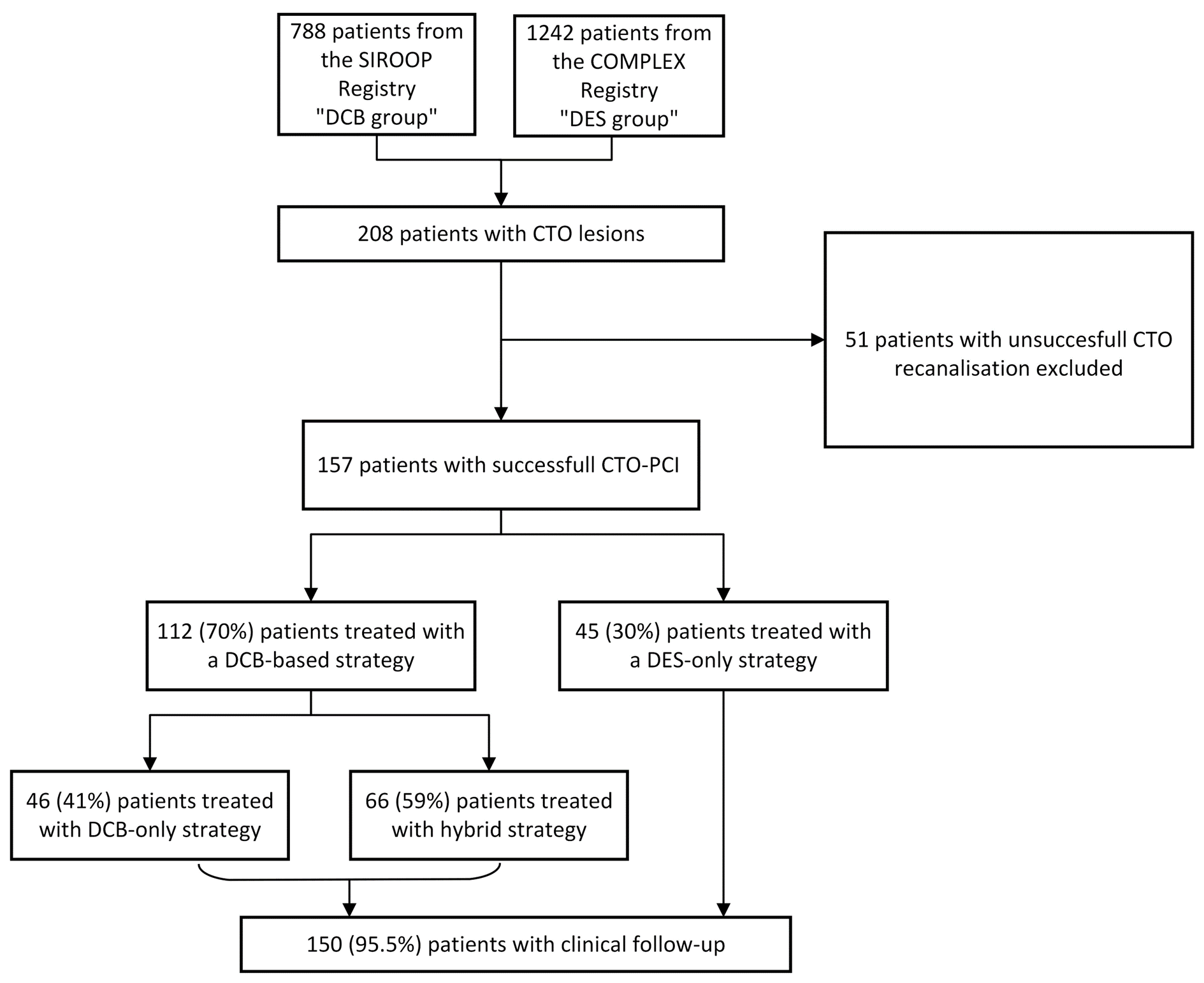
Between February 2021 and February 2023, we enrolled a total of 157 patients who underwent a successful CTO-PCI procedures at our institution. Of these, 112 (71%) patients underwent CTO treatment involving DCBs (“DCB group”), whereas 46 (29%) matching patients were treated with DES only (“DES group”), as highlighted in the study flow chart (Figure 1).
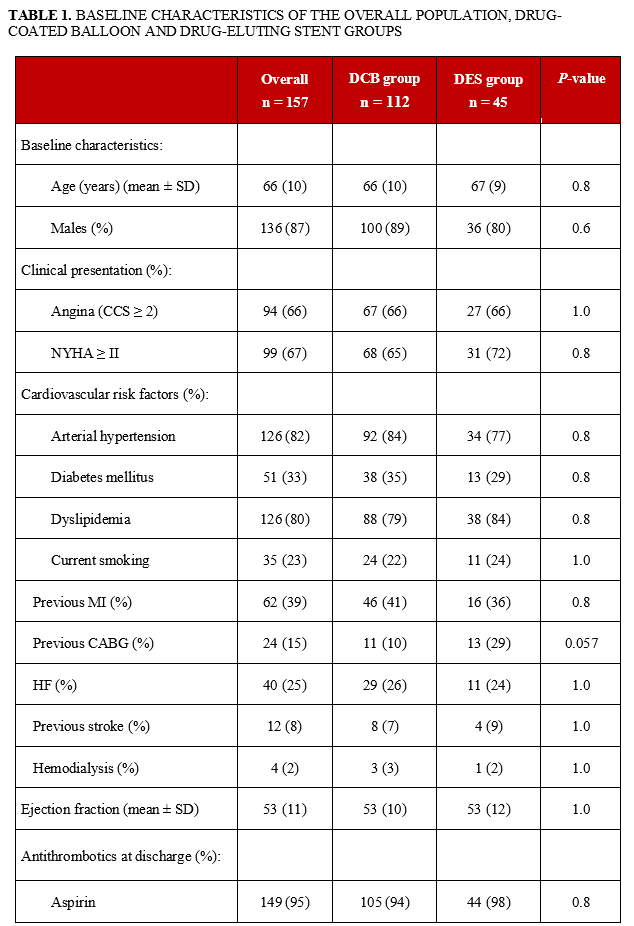
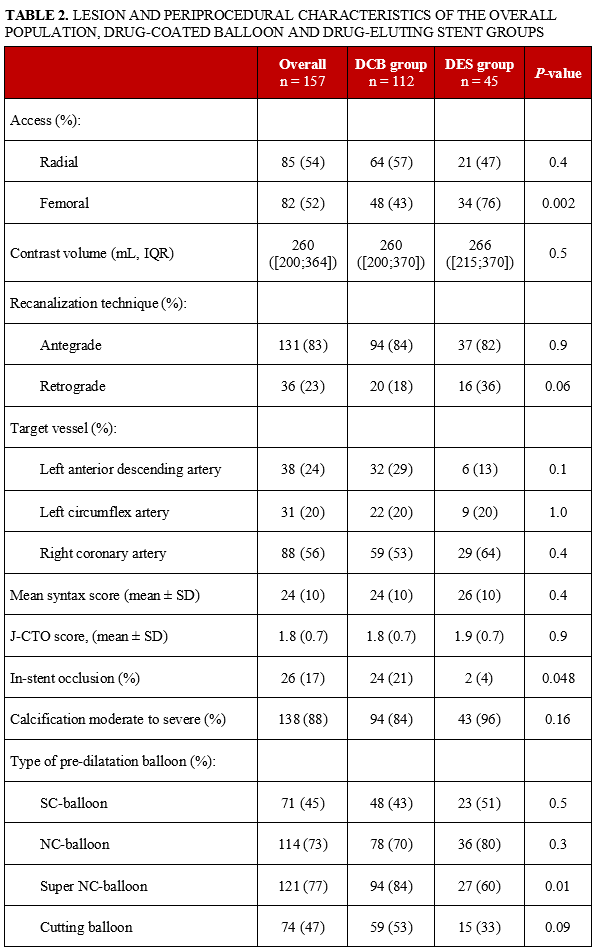
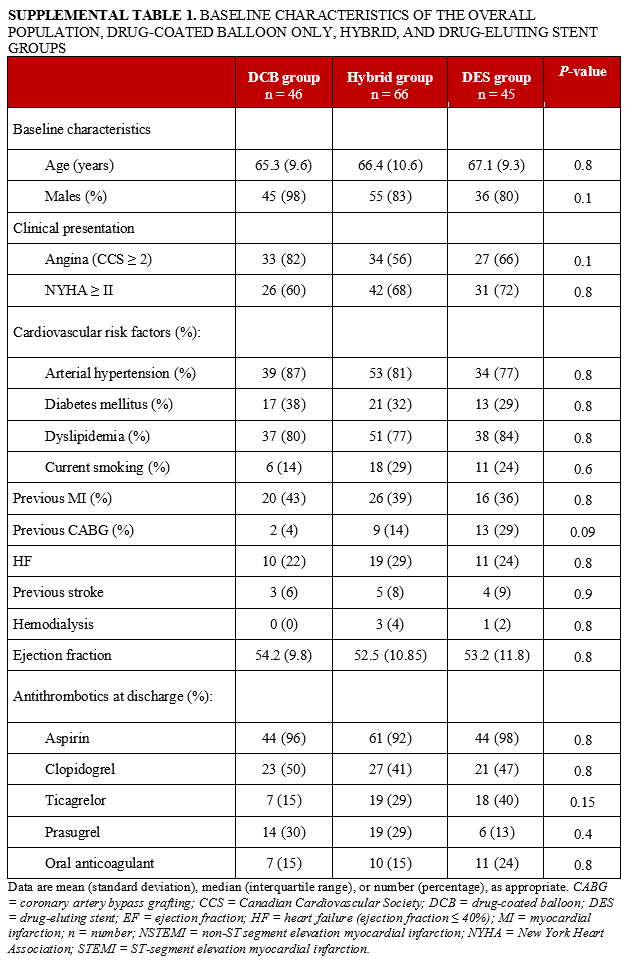
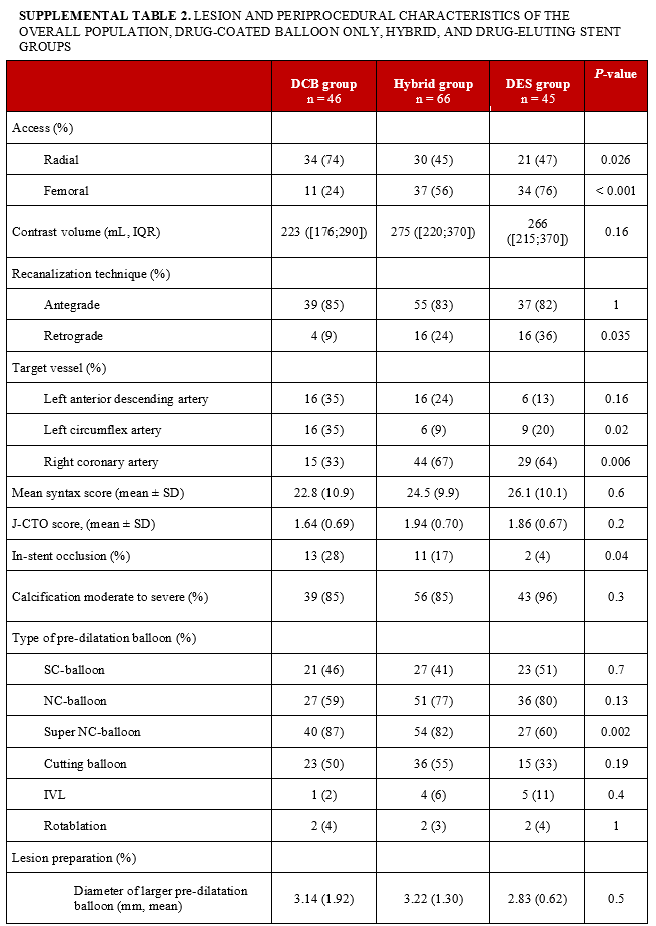
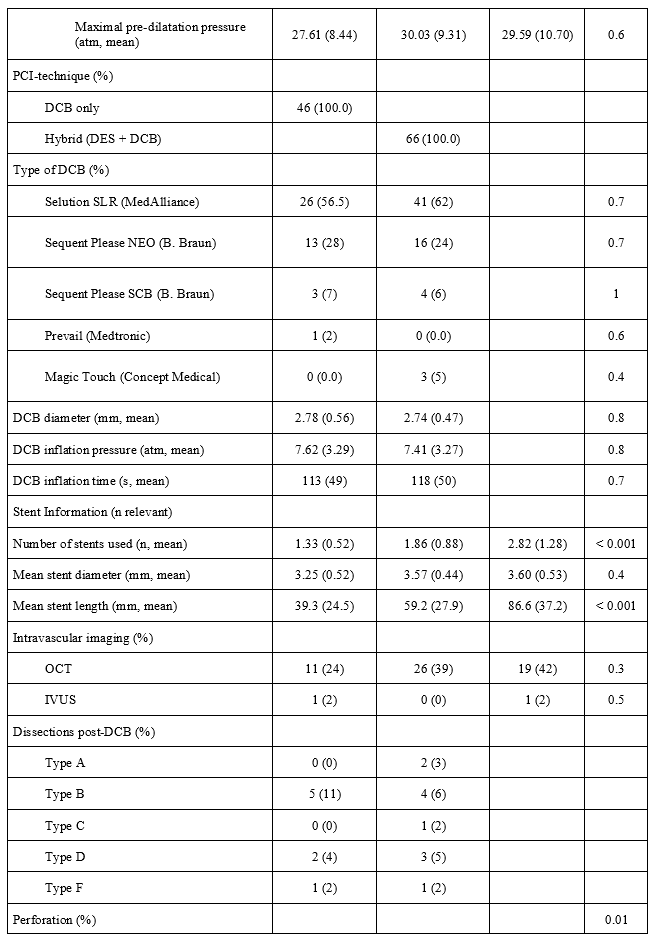
Baseline and procedural demographics. The baseline characteristics of the included patients are displayed in Table 1. The mean age of the population was 66 ± 10 years, most patients were males (87%), and approximately one-third had diabetes. The angiographic and procedural characteristics are summarized in Table 2. Most CTO lesions involved the right coronary artery (RCA), the mean J-CTO score was 1.8 ± 0.7, and the cohort´s mean SYNTAX score was 24 ± 10. In the DCB group, 66 (59%) of the patients had hybrid treatment of their target vessels involving the CTO lesions. Regarding lesion pre-treatment, the use of both NC and cutting balloons was significantly higher in the DCB group compared to the DES group. Regarding DCB and DES sizing, the mean DCB and DES diameters were 2.8 ± 0.5 mm and 3.5 ± 0.5 mm, respectively. The majority of DCB cases were managed with sirolimus-coated balloons (74, 66%). Of note, 56 (36%) of the procedures involved the use of intravascular imaging with OCT.
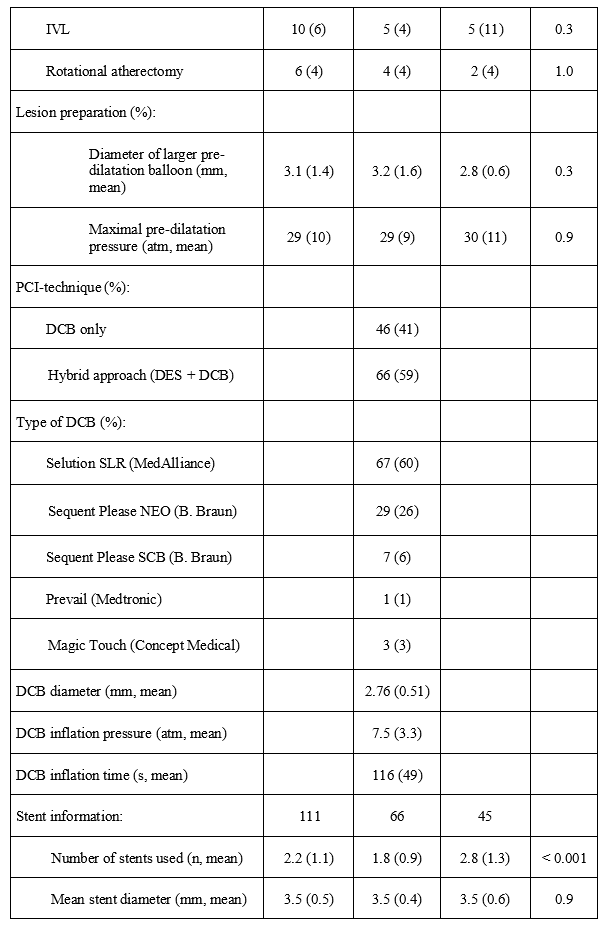
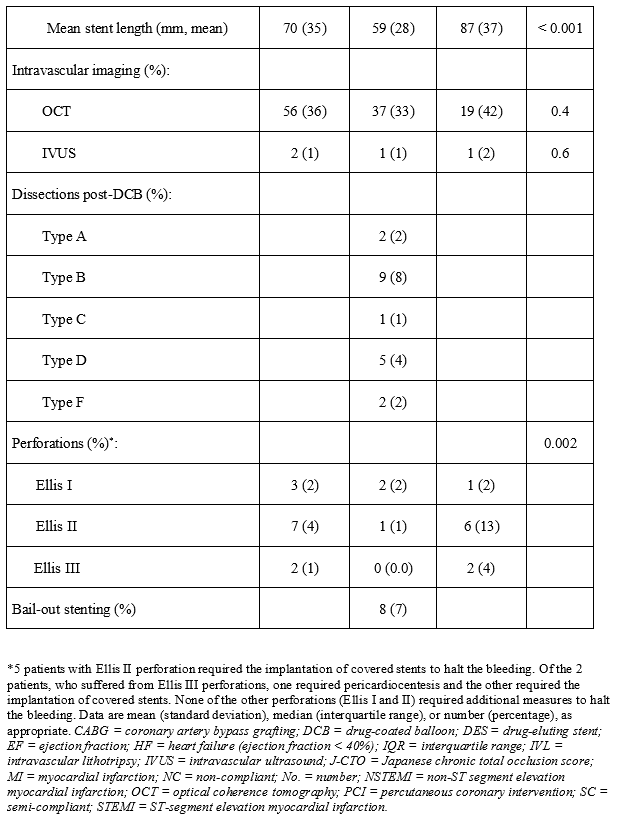
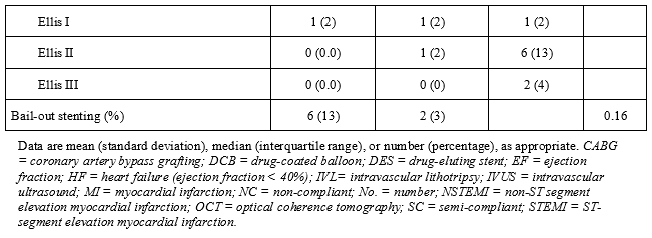
In the DCB group, bailout stenting was carried out in 8 (7%) patients, whereas 7 cases involved flow-limiting dissections and 1 lesion showed relevant recoil. With respect to periprocedural complications, we observed more perforation, predominantly Ellis II, in the DES group compared to the DCB group (13% vs 1%, P=.002). No acute vessel closure was observed in either group.
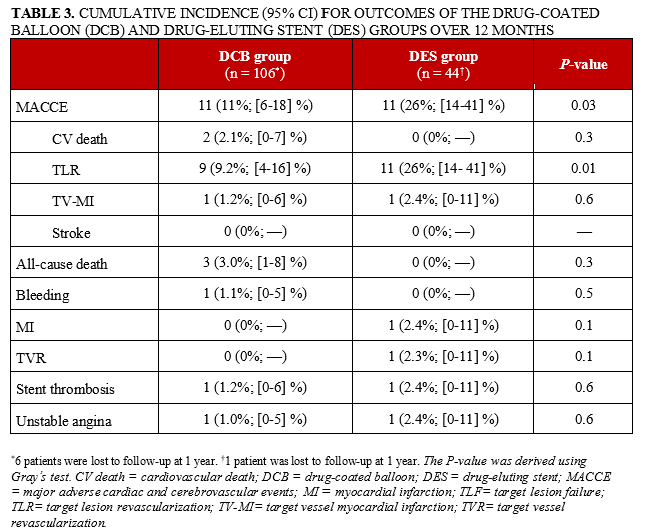
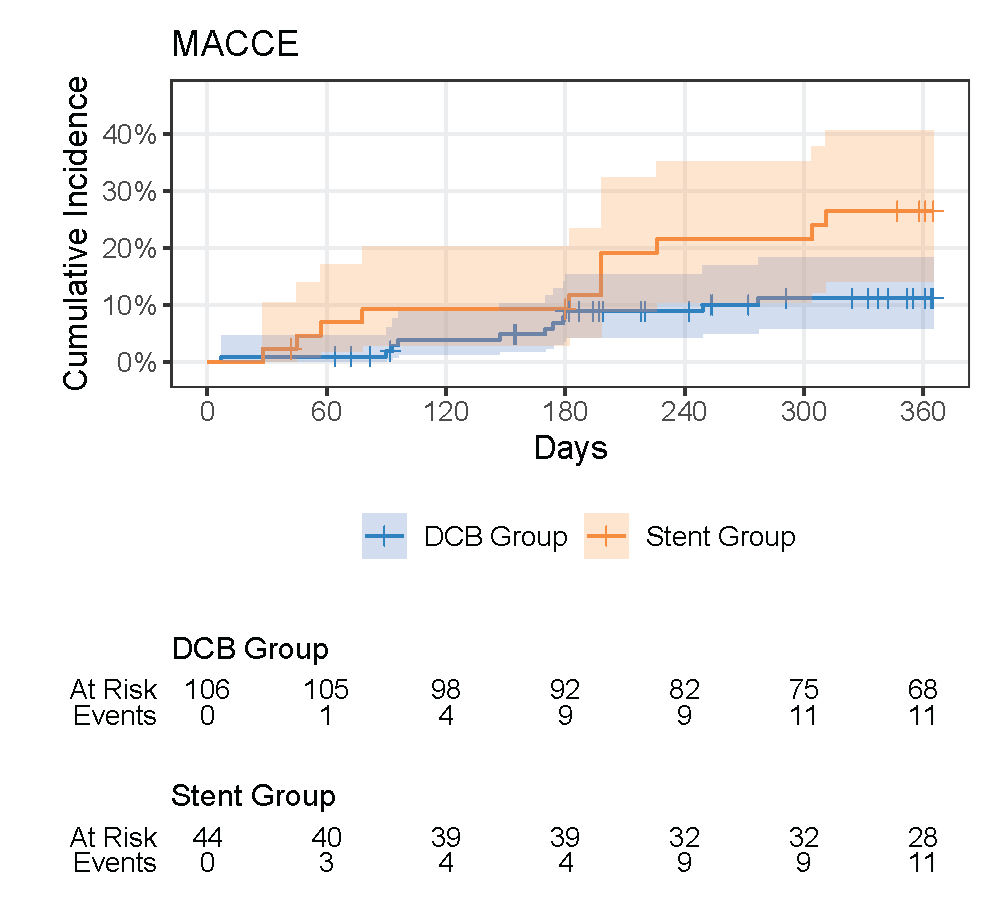
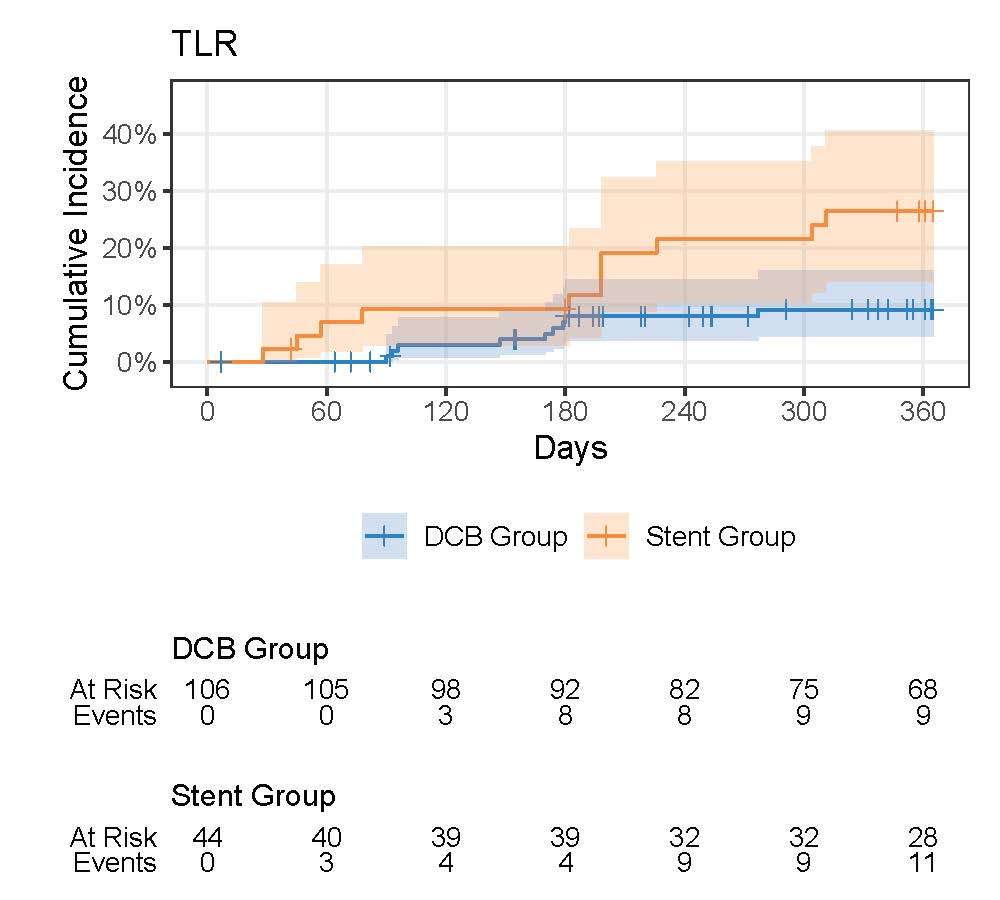
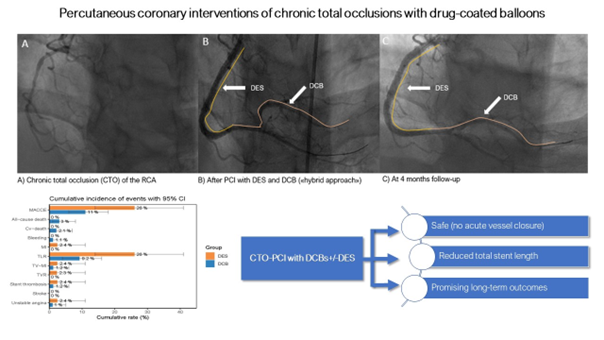
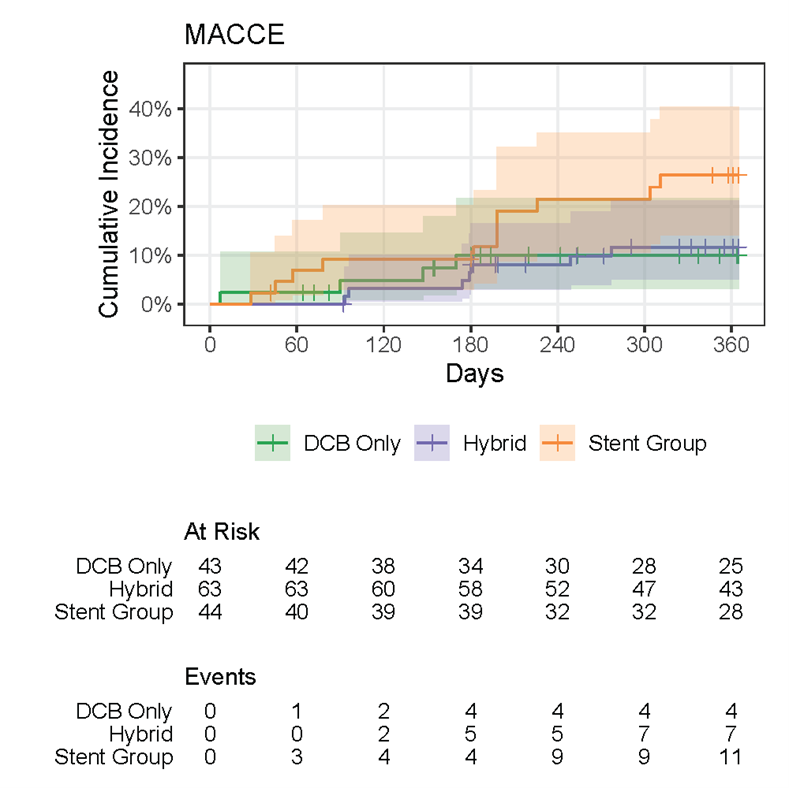
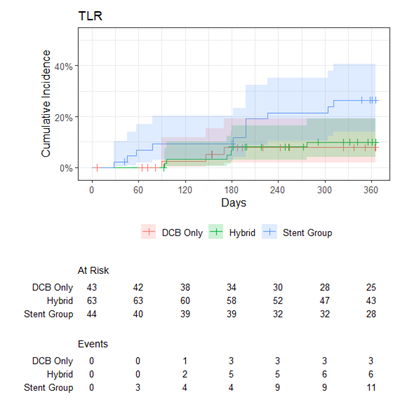
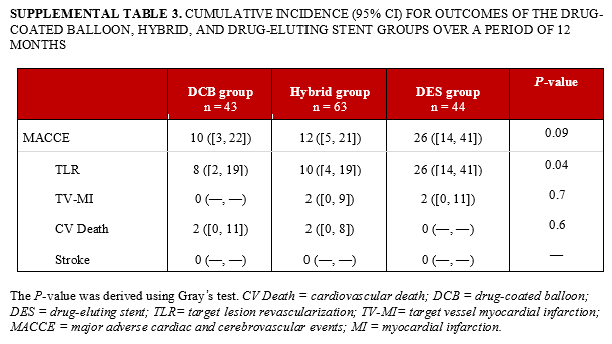
Follow-up. The median follow-up duration was 20 (IQR 12; 20.5) months. After 12 months, we observed a MACCE rate of 26% in the DES group vs 11% in the DCB group (P=.031). Of note, we did not observe a single case with acute vessel closure. Stent thrombosis rate was 2% in the DES group vs 1% in the DCB group. The detailed description of the clinical outcomes is reported in Table 3. The cumulative incidence curves in Figures 2 and 3 illustrate the lower MACCE and TLR rate following CTO-PCI involving DCBs compared to the DES-only group. The most common presentation for MACCE was TLR. Figure 4 reports an illustrative case of a patient with CTO treated in a DCB-only approach. In a subgroup analysis, DCB-only PCI was associated with better long-term outcomes compared to the DES-only and hybrid groups (TLR rates were 8% vs 26% and 10%, respectively, P=.04). However, CTO lesions managed with only DCBs appeared less complex compared to the lesions requiring treatment with DES. Figure 5 (central illustration) summarizes the most salient findings of this study. This is highlighted in Supplemental Tables 1-3 as well as Supplemental Figures 1 and 2.
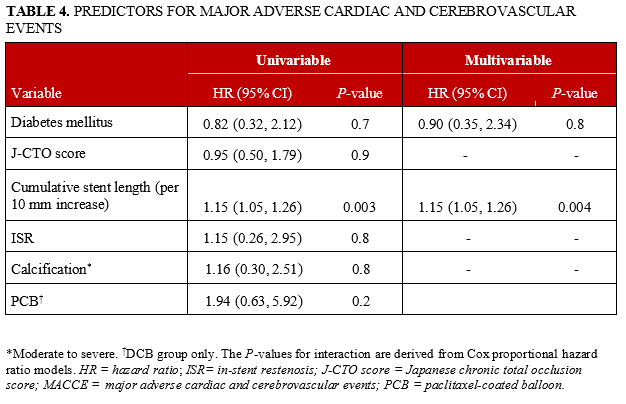
Predictors for MACCE. When assessing potential predictors for MACCE following CTO-PCI, we found that cumulative stent length was the strongest predictor (HR 1.15 [1.05, 1.26] per 10 mm), as highlighted in Table 4.
Discussion
More than 20% of patients referred for evaluation of coronary artery disease have at least 1 CTO lesion, and the prevalence of CTOs is expected to increase with the aging of societies and the growing prevalence of cardiovascular risk factors.1,25 Over the last decade, there has been a global dissemination in advanced CTO-PCI techniques and experienced centers consistently achieve CTO-PCI success rates of more than 80%.1,25-27 But irrespective of those achievements, the TVR rate following successful CTO-PCI with stent implantation remains high and warrants further improvements.2-4,11, 28, 29
In this context, our study may provide several important insights since it represents one of the first to evaluate CTO revascularization with DCBs vs only DES. Our analysis not only highlights the safety of CTO-PCI involving DCBs, but also that integrating DCBs into CTO-PCI treatment appears to result in good clinical outcomes.
Vascular healing following PCI with stent implantation in CTO lesions differs from other coronary lesions. In fact, CTO lesions often involve long segments and tend to negatively remodel beyond the occlusion site. Those factors can complicate the selection of the appropriate stent length and sizes. There is often vessel growth following CTO reperfusion, which can leave previously implanted stents undersized and malposed, directly increasing the risk for adverse outcomes (eg, ST and ISR).6-8 Furthermore, following application of dissection re-entry techniques during CTO-PCI, extraluminal stent placement might occur, which can potentially hinder adequate stent sizing and healing.
Therefore, DCBs hypothetically represent an appealing alternative to DES. Treating CTO vessels with DCBs, at least partially, not only reduces the total stent burden and the associated complications, but also enables growth and restoration of vasomotion.11, 30. In fact, extensive stenting has been associated with adverse clinical outcomes, as highlighted in earlier studies.31, 32
In our study, the mean number of stents and the total stent length were reduced by more than 30% in the DCB compared to the DES group (2.8 ± 1.3 vs. 1.8 ± 0.9, P < .001 and 87 ± 37 mm vs 58 ± 28 mm, P <. 001). This appears important, since our data also imply that cumulative stent length in CTO-PCI is a significant predictor for MACCE. Additionally, we observed that the rate of coronary perforations, particularly of those requiring interventions (Ellis II and III), was lower in the CTO cohort managed with DCBs. Of note, 3 of the Ellis II and III perforations occurred following stent post-dilatation. Although no firm inferences can be drawn from this observation, it may nonetheless represent an important safety signal, reminding physicians to be mindful of aggressive stent optimization after CTO-PCI with DES implantation and prompting them to opt for CTO-PCI involving DCBs, if feasible.
So far, data describing the safety and outcomes following treatment of CTO lesions with DCBs remain limited and comparative studies are scarce. Only case series and retrospective studies reporting outcomes following CTO-PCI involving DCBs have been published.9-12, 33 Whereas an early study reported TLF rates of approximately 18%,10 a more recent study by Jun et al reported a MACCE rate of 8.3% at 12-month follow-up after treatment of de novo CTO lesions with DCB only.11 However, one needs to consider that those studies included less complex CTO cases in comparison to ours (eg, mean J-CTO score 1.4 score vs 1.8).9-12, 33
Interestingly, we found that CTO cases treated with DCBs only had the lowest rates of adverse outcomes, especially TLR. While this data should be interpreted cautiously, it appears intriguing and, moreover, expands upon data from recent retrospective studies.10, 11
When interpreting our results, physicians should be aware that our site generally aims for meticulous lesion preparation in CTO-PCI involving a high percentage of cutting and NC balloons.14, 34, 35 In PCI with DCBs, lesion preparation is of paramount importance in order to achieve optimal lumen gain, not just acutely but also over time.19 In our experience, the combined use of cutting and NC balloons (“cut and crack approach”) mitigates the risk of flow-limiting dissections, and increases the luminal gain in the majority of cases. This is also highlighted by our results, which show a low rate of flow-limiting dissections and requirement of bail-out stenting. Additionally, cutting balloons may provide a more controlled disruption of the atherosclerotic plaque and facilitate tissue penetration of the cytotoxic drug.19 In this context, the use of OCT allows the selection of adequately sized balloons and evaluation of dissection.
Another important factor that could have influenced our results is the type of DCBs used. To date, the majority of studies that have been published on DCBs involve paclitaxel-coated balloons.10,19 Contrastingly, in our CTO population, more than two-thirds of all patients were treated with novel sirolimus-coated balloons, which were introduced just recently.14,36 Those novel DCB devices not only have a limus-based coating, which executes different cytostatic actions on smooth muscle cells, but their enhanced catheter design and refined drug coating (eg, using microreservoirs or phospholipids) may permit delivery of higher drug concentrations than earlier generation paclitaxel-coated balloons with either iopromide, shellac, or citrate-based coating, which tend to dissolve very rapidly in the blood stream.19, 37 Recently published outcomes of all-comers treated with some of these novel sirolimus-coated balloons found adverse cardiovascular event rates as low as 7%.14, 36
We are aware of several limitations that apply to our study. First, this is an observational single-center study, which may limit its generalizability and does not allow firm inferences to be drawn. Thus, the data should be considered as hypothesis-generating. Second, the study´s sample size was relatively small, which limits statistical power. Also, at the timepoint of this analysis, we had a smaller number of patients enrolled in the COMPLEX registry than in the SIROOP registry. Third, although the compared CTO cohorts showed no relevant imbalances with respect to baseline and procedural characteristics, some confounding cannot be ruled out. Nonetheless, the CTO operators were the same in both cohort studies, which should at least somewhat mitigate the risk for relevant selection as well as information bias. Fourth, we did not routinely collect quantitative coronary angiography (QCA) data, which could have provided important information on differences in vessel diameter and residual stenosis following treatment with either strategy. Finally, we also did not routinely perform angiographic follow-up examinations in our cohort.
Conclusions
Compared to treatment with DES only, treatment of CTO lesions with DCBs appears to be safe and associated with improved overall long-term outcomes, including lower MACCE rates at 12-month follow-up. CTO treatment with DCBs also reduces total stent length, which appears to be an important predictor for adverse outcomes. The intriguing data derived from our study expands upon existing research that supports the utility of DCB in the treatment of coronary artery disease.
Affiliations and Disclosures
From the 1Cardiology Division, Heart Center, Luzerner Kantonsspital, Lucerne, Switzerland; 2Department of Health Sciences and Medicine, University of Lucerne, Lucerne, Switzerland; 3McMaster University, Hamilton, Ontario, Canada; Hamilton Health Sciences, Hamilton, Canada; 4Istituto Cardiocentro Ticino, Ente Ospedaliero Cantonale, Lugano, Switzerland; 5Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico di Milano, University of Milan, Milan, Italy; 6Faculty of Medicine, University of Zurich, Zurich, Switzerland.
Drs Madanchi and Bossard contributed equally and should be considered as shared first authors. Dr Attinger-Toller and Cuculi should be considered as shared last authors.
Disclosures: Dr Attinger-Toller has received consulting and speaker fees from SIS Medical. Dr Bossard has received consulting and speaker fees from Abbott Vascular, Abiomed, Amarin, Amgen, Astra Zeneca, Bayer, Boehringer Ingelheim, Daichii, MedAlliance, Mundipharma, Novartis, Ompharma and SIS Medical. Dr Cuculi has received consulting and speaker fees from Abbott Vascular, Abiomed, Boston Scientific and SIS Medical. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Florim Cuculi, MD, Cardiology Division, Heart Center – Luzerner Kantonsspital, Luzern, Switzerland. Email: florim.cuculi@luks.ch
Supplemental Material
References
- Brilakis ES, Banerjee S, Karmpaliotis D, et al. Procedural outcomes of chronic total occlusion percutaneous coronary intervention: A report from the NCDR (National Cardiovascular Data Registry). JACC Cardiovasc Interv. 2015;8(2):245-253. doi:10.1016/j.jcin.2014.08.014
- Azzalini L, Carlino M, Bellini B, et al. Long-term outcomes of chronic total occlusion recanalization versus percutaneous coronary intervention for complex non-occlusive coronary artery disease. Am J Cardiol. 2020;125(2):182-188. doi:10.1016/j.amjcard.2019.10.034
- Guan C, Yang W, Song L, et al. Association of acute procedural results with long-term outcomes after CTO PCI. JACC Cardiovasc Interv. 2021;14(3):278-288. doi:10.1016/j.jcin.2020.10.003
- Kandzari DE, Kini AS, Karmpaliotis D, et al. Safety and effectiveness of everolimus-eluting stents in chronic total coronary occlusion revascularization: Results from the EXPERT CTO Multicenter Trial (evaluation of the XIENCE coronary stent, performance, and technique in chronic total occlusions). JACC Cardiovasc Interv. 2015;8(6):761-769. doi:10.1016/j.jcin.2014.12.238
- Sakakura K, Nakano M, Otsuka F, et al. Comparison of pathology of chronic total occlusion with and without coronary artery bypass graft. Eur Heart J. 2014;35(25):1683-1693. doi:10.1093/eurheartj/eht422
- Mahadevan K, Cosgrove C, Strange JW. Factors Influencing stent failure in chronic total occlusion coronary intervention. Interv Cardiol. 2021;16:e27. doi:10.15420/icr.2021.03
- Galassi AR, Tomasello SD, Crea F, et al. Transient impairment of vasomotion function after successful chronic total occlusion recanalization. J Am Coll Cardiol. 2012;59(8):711-718. doi:10.1016/j.jacc.2011.10.894
- Nguyen-Trong PKJ, Rangan BV, Karatasakis A, et al. Predictors and outcomes of side-branch occlusion in coronary chronic total occlusion interventions. J Invasive Cardiol. 2016;28(4):168-173.
- Cortese B, Buccheri D, Piraino D, Silva-Orrego P. Drug-coated balloon angioplasty for coronary chronic total occlusions. An OCT analysis for a "new" intriguing strategy. Int J Cardiol. 2015;189:257-258. doi:10.1016/j.ijcard.2015.04.102
- Köln PJ, Scheller B, Liew HB, et al. Treatment of chronic total occlusions in native coronary arteries by drug-coated balloons without stenting - A feasibility and safety study. Int J Cardiol. 2016;225:262-267. doi:10.1016/j.ijcard.2016.09.105
- Jun EJ, Shin ES, Teoh EV, et al. Clinical outcomes of drug-coated balloon treatment after successful revascularization of de novo chronic total occlusions. Front Cardiovasc Med. 2022;9:821380. doi:10.3389/fcvm.2022.821380
- Wang X, Yang X, Lu W, et al. Long-term outcomes of less drug-eluting stents by the use of drug-coated balloons in de novo coronary chronic total occlusion intervention: A multicenter observational study. Front Cardiovasc Med. 2023;10:1045859. doi:10.3389/fcvm.2023.1045859
- Picard F, Doucet S, Asgar AW. Contemporary use of drug-coated balloons in coronary artery disease: Where are we now? Arch Cardiovasc Dis. 2017;110(4):259-272. doi:10.1016/j.acvd.2017.01.005
- Madanchi M, Cioffi GM, Attinger-Toller A, et al. Metal free percutaneous coronary interventions in all-comers: First experience with a novel sirolimus-coated balloon. Cardiol J. 2022;29(6):906-916. doi:10.5603/CJ.a2022.0106
- Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87-165. doi:10.1093/eurheartj/ehy394
- Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41(3):407-477. doi:10.1093/eurheartj/ehz425
- Virani SS, Newby LK, Arnold SV, et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients With Chronic Coronary Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2023;148(9):e9-e119. doi:10.1161/CIR.0000000000001168
- Galassi AR, Werner GS, Boukhris M, et al. Percutaneous recanalisation of chronic total occlusions: 2019 consensus document from the EuroCTO Club. EuroIntervention. 2019;15(2):198-208. doi:10.4244/EIJ-D-18-00826
- Jeger RV, Eccleshall S, Wan Ahmad WA, et al. Drug-coated balloons for coronary artery disease: Third report of the International DCB Consensus Group. JACC Cardiovasc Interv. 2020;13(12):1391-1402. doi:10.1016/j.jcin.2020.02.043
- Tajti P, Burke MN, Karmpaliotis D, et al. Update in the percutaneous management of coronary chronic total occlusions. JACC Cardiovasc Interv. 2018;11(7):615-625. doi:10.1016/j.jcin.2017.10.052
- Christopoulos G, Karmpaliotis D, Alaswad K, et al. The efficacy of "hybrid" percutaneous coronary intervention in chronic total occlusions caused by in-stent restenosis: insights from a US multicenter registry. Catheter Cardiovasc Interv. 2014;84(4):646-651. doi:10.1002/ccd.25465
- Morino Y, Kimura T, Hayashi Y, et al. In-hospital outcomes of contemporary percutaneous coronary intervention in patients with chronic total occlusion insights from the J-CTO Registry (Multicenter CTO Registry in Japan). JACC Cardiovasc Interv. 2010;3(2):143-151. doi:10.1016/j.jcin.2009.10.029
- Huber MS, Mooney JF, Madison J, Mooney MR. Use of a morphologic classification to predict clinical outcome after dissection from coronary angioplasty. Am J Cardiol. 1991;68(5):467-471. doi:10.1016/0002-9149(91)90780-o
- Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation. 2007;115(17):2344-2351. doi:10.1161/CIRCULATIONAHA.106.685313
- Konstantinidis NV, Werner GS, Deftereos S, et al. Temporal trends in chronic total occlusion interventions in Europe. Circ Cardiovasc Interv. 2018;11(10):e006229. doi:10.1161/CIRCINTERVENTIONS.117.006229
- Habara M, Tsuchikane E, Muramatsu T, et al. Comparison of percutaneous coronary intervention for chronic total occlusion outcome according to operator experience from the Japanese retrograde summit registry. Catheter Cardiovasc Interv. 2016;87(6):1027-1035. doi:10.1002/ccd.26354
- Azzalini L, Jolicoeur EM, Pighi M, et al. Epidemiology, management strategies, and outcomes of patients with chronic total coronary occlusion. Am J Cardiol. 2016;118(8):1128-1135. doi:10.1016/j.amjcard.2016.07.023
- Kotsia A, Navara R, Michael TT, et al. The angiographic evaluation of the everolimus-eluting stent in chronic total occlusion (ACE-CTO) study. J Invasive Cardiol. 2015;27(9):393-400.
- Walsh SJ, Hanratty CG, McEntegart M, et al. Intravascular Healing is not affected by approaches in contemporary CTO PCI: The CONSISTENT CTO Study. JACC Cardiovasc Interv. 2020;13(12):1448-1457. doi:10.1016/j.jcin.2020.03.032
- Kleber FX, Schulz A, Waliszewski M, et al. Local paclitaxel induces late lumen enlargement in coronary arteries after balloon angioplasty. Clin Res Cardiol. 2015;104(3):217-225. doi:10.1007/s00392-014-0775-2
- Hara H, Ono M, Kawashima H, et al. Impact of stent length and diameter on 10-year mortality in the SYNTAXES trial. Catheter Cardiovasc Interv. 2021;98(3):E379-E387. doi:10.1002/ccd.29721
- Mauri L, O'Malley AJ, Cutlip DE, et al. Effects of stent length and lesion length on coronary restenosis. Am J Cardiol. 2004;93(11):1340-1346, A5. doi:10.1016/j.amjcard.2004.02.027
- Onishi T, Onishi Y, Kobayashi I, Umezawa S, Niwa A. Drug-coated balloon angioplasty for de novo small vessel disease including chronic total occlusion and bifurcation in real-world clinical practice. Cardiovasc Interv Ther. 2019;34(2):139-148. doi:10.1007/s12928-018-0534-9
- Seiler T, Attinger-Toller A, Cioffi GM, et al. Treatment of in-stent restenosis using a dedicated super high-pressure balloon. Cardiovasc Revasc Med. 2023;46:29-35. doi:10.1016/j.carrev.2022.08.018
- Pinilla-Echeverri N, Bossard M, Hillani A, et al. Treatment of calcified lesions using a dedicated super-high pressure balloon. Multicenter optical coherence tomography registry. Cardiovasc Revasc Med. 2023;52:49-58. doi:10.1016/j.carrev.2023.02.020
- Cortese B, Testa L, Di Palma G, et al. Clinical performance of a novel sirolimus-coated balloon in coronary artery disease: EASTBOURNE registry. J Cardiovasc Med (Hagerstown). 2021;22(2):94-100. doi:10.2459/JCM.0000000000001070
- Chen Y, Zeng Y, Zhu X, et al. Significant difference between sirolimus and paclitaxel nanoparticles in anti-proliferation effect in normoxia and hypoxia: The basis of better selection of atherosclerosis treatment. Bioact Mater. 2021;6(3):880-889. doi:10.1016/j.bioactmat.2020.09.005











