


Paclitaxel Drug-Coated Balloon for the Treatment of De Novo Small-Vessel and Restenotic Coronary Artery Lesions: 12-Month Results of the Prospective, Multicenter, Single-Arm PREVAIL Study
Abstract
Objectives. The PREVAIL study evaluated the safety and effectiveness of a paclitaxel-coated percutaneous transluminal coronary angioplasty balloon catheter for the treatment of coronary de novo and in-stent restenosis (ISR) lesions in patients with symptomatic ischemic heart disease. Methods. PREVAIL was a prospective, multicenter, single-arm study that enrolled patients with clinical evidence of ischemia who had coronary lesions (de novo or first ISR) amenable to treatment with a drug-coated balloon (DCB). The study included 50 subjects (53 target lesions) who were treated with a Prevail DCB (Medtronic) during the index procedure and followed for 12 months. Mean lesion length was 14.5 ± 7.6 mm. The primary endpoint was in-stent (in-balloon) late lumen loss (LLL) by quantitative coronary angiography at 6 months post procedure. If the mean in-stent (in-balloon) LLL was less than the maximum acceptance rate of 0.50 mm at 6 months, then the study was considered successful. Results. Mean in-stent (in-balloon) LLL was 0.05 ± 0.44 mm at 6 months post procedure. There were no deaths, myocardial infarctions, or stent (lesion) thrombosis events within 12 months. The incidence of clinically driven target-lesion revascularization was 6.0% at 12 months and clinically driven target-vessel revascularization was 10.0%. Conclusions. Paclitaxel DCB treatment of coronary de novo and first ISR lesions led to low LLL at 6 months and low rates of revascularization and safety events through 12 months.
J INVASIVE CARDIOL 2021;33(11):E863-E869. Epub 2021 August 19.
Key words: DCB, drug-coated balloon, in-stent restenosis, ischemia, revascularization
Introduction
As an alternative to drug-eluting stent (DES) options, drug-coated balloons (DCBs) provide targeted delivery of an antirestenotic agent during percutaneous coronary intervention (PCI) without leaving a permanent implant behind. Clinical investigations have evaluated the role of coronary DCBs in the treatment of in-stent restenosis (ISR) and small-vessel lesions, with prospective single-arm trials, retrospective and observational cohort studies, and registries showing that paclitaxel DCBs can safely and effectively treat these lesion types.1-6 While randomized controlled trials have demonstrated that paclitaxel DCBs are superior to angioplasty with an uncoated balloon and non-inferior to DESs for the treatment of coronary ISR,7-14 findings have been mixed in patients with small-vessel disease, highlighting that this technology does not have a class effect and not all DCBs are created equally.15-17
The aim of the present study was to evaluate the clinical safety and effectiveness of a next-generation paclitaxel-coated percutaneous transluminal coronary angioplasty (PTCA) balloon for the treatment of patients with de novo or ISR lesions. Herein, we report 6-month angiographic and 12-month clinical and safety outcomes.
Methods
Study design. PREVAIL was a prospective, multicenter, single-arm premarket study that evaluated the clinical safety and effectiveness of the Prevail paclitaxel-coated PTCA balloon catheter (Medtronic) for the treatment of coronary de novo lesions, ISR, and small-vessel disease in patients with symptomatic ischemic heart disease. Patients were treated with the DCB during the index procedure and clinical follow-up was performed at 30 days, 6 months, and 12 months post procedure; quantitative coronary angiography (QCA) was performed before and after the procedure, and at 6-month follow-up. All patients provided informed consent.
A clinical events committee reviewed and adjudicated all clinical endpoints (Baim Institute for Clinical Research). A data monitoring committee evaluated safety data over the course of the study (Baim Institute for Clinical Research). An angiography core laboratory analyzed procedural and follow-up images (Beth Israel Deaconess Medical Center).
The study was conducted in accordance with the Declaration of Helsinki, Good Clinical Practice principles outlined in ISO 14155:2011, and applicable laws as specified by all relevant governmental authorities. The protocol was reviewed and approved by all ethics committees and institutional review boards. All patients provided written informed consent prior to enrollment. The study is registered at clinicaltrials.gov (NCT03260517).
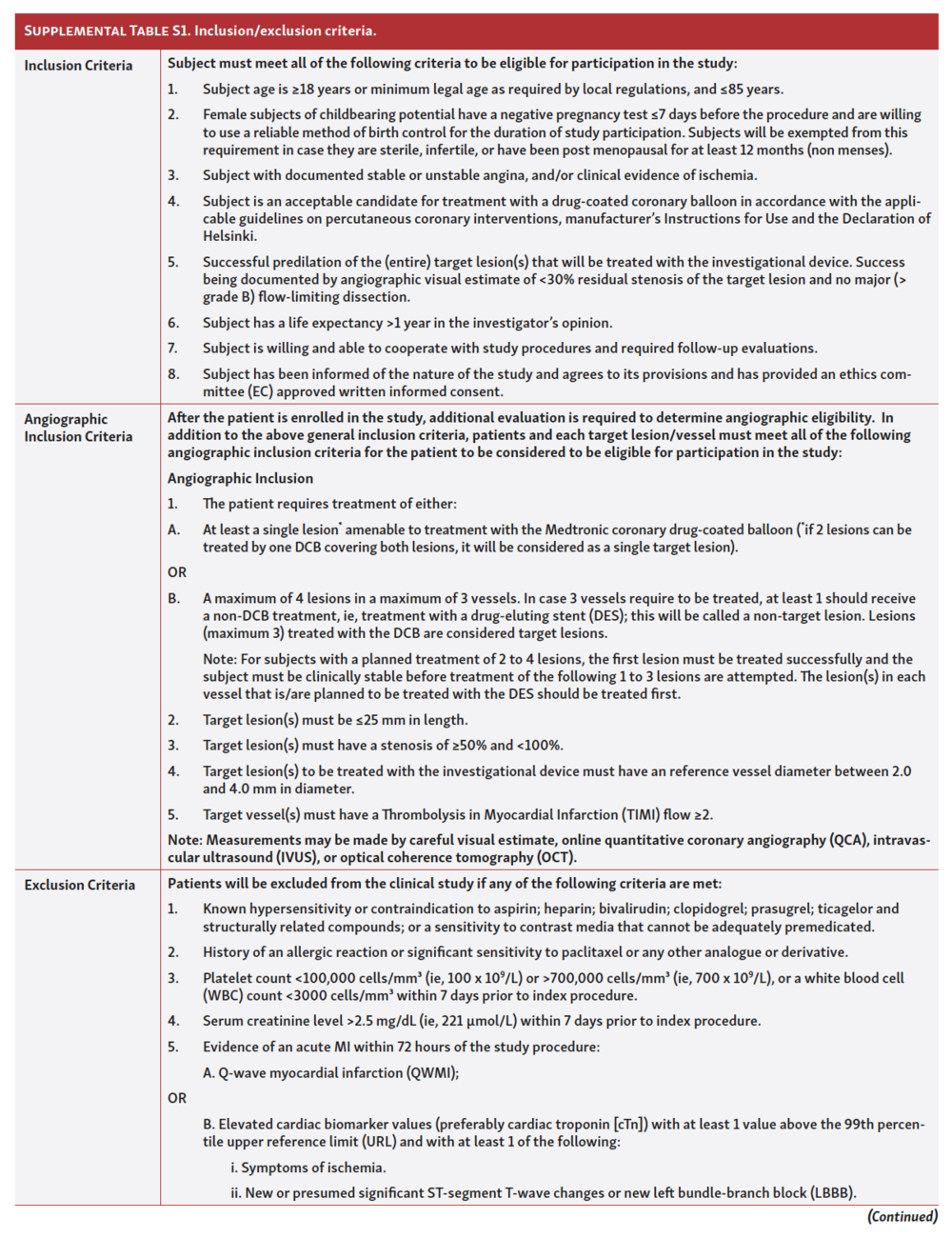
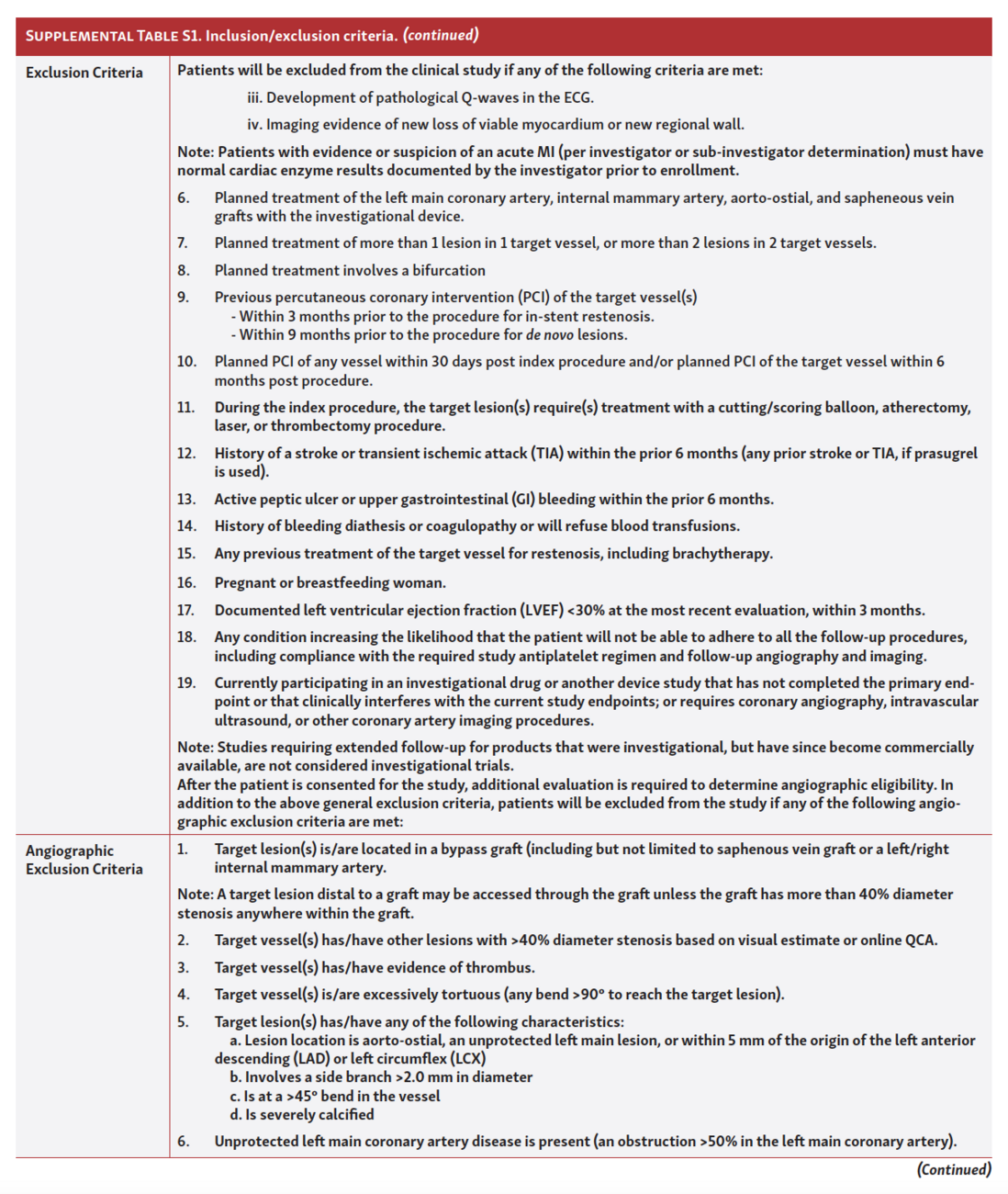
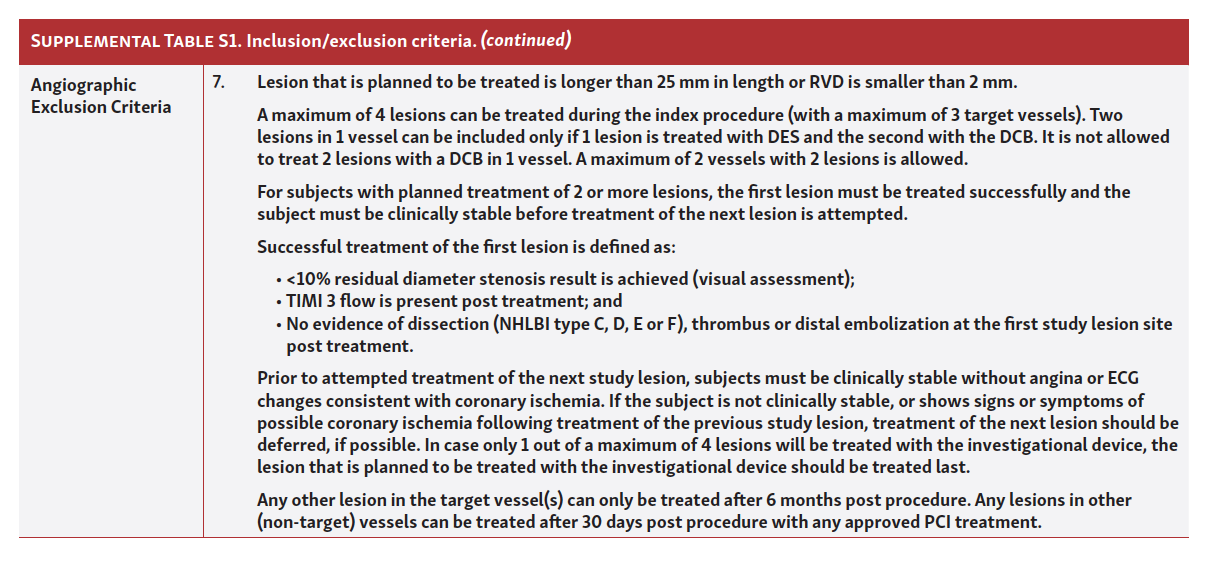
Patient population. Patients enrolled had documented stable or unstable angina and/or clinical evidence of ischemia and were deemed acceptable candidates for treatment with a DCB. Major exclusion criteria included previous PCI of the target vessel (<9 months before the index procedure for de novo lesions, <3 months for ISR), a stroke/transient ischemic attack <6 months or a myocardial infarction (MI) event <72 hours before the index procedure. Complete inclusion/exclusion criteria are listed in Supplemental Table S1 (Part 1 of 3) / (Part 2 of 3) / (Part 3 of 3). All enrolled patients had angiography to confirm additional angiographic inclusion/exclusion criteria as listed in Supplemental Table S1 (Part 1 of 3) / (Part 2 of 3) / (Part 3 of 3). Of note, target lesions must have been ≤25 mm in length with a reference vessel diameter of 2-4 mm and diameter stenosis ≥50% but <100%.
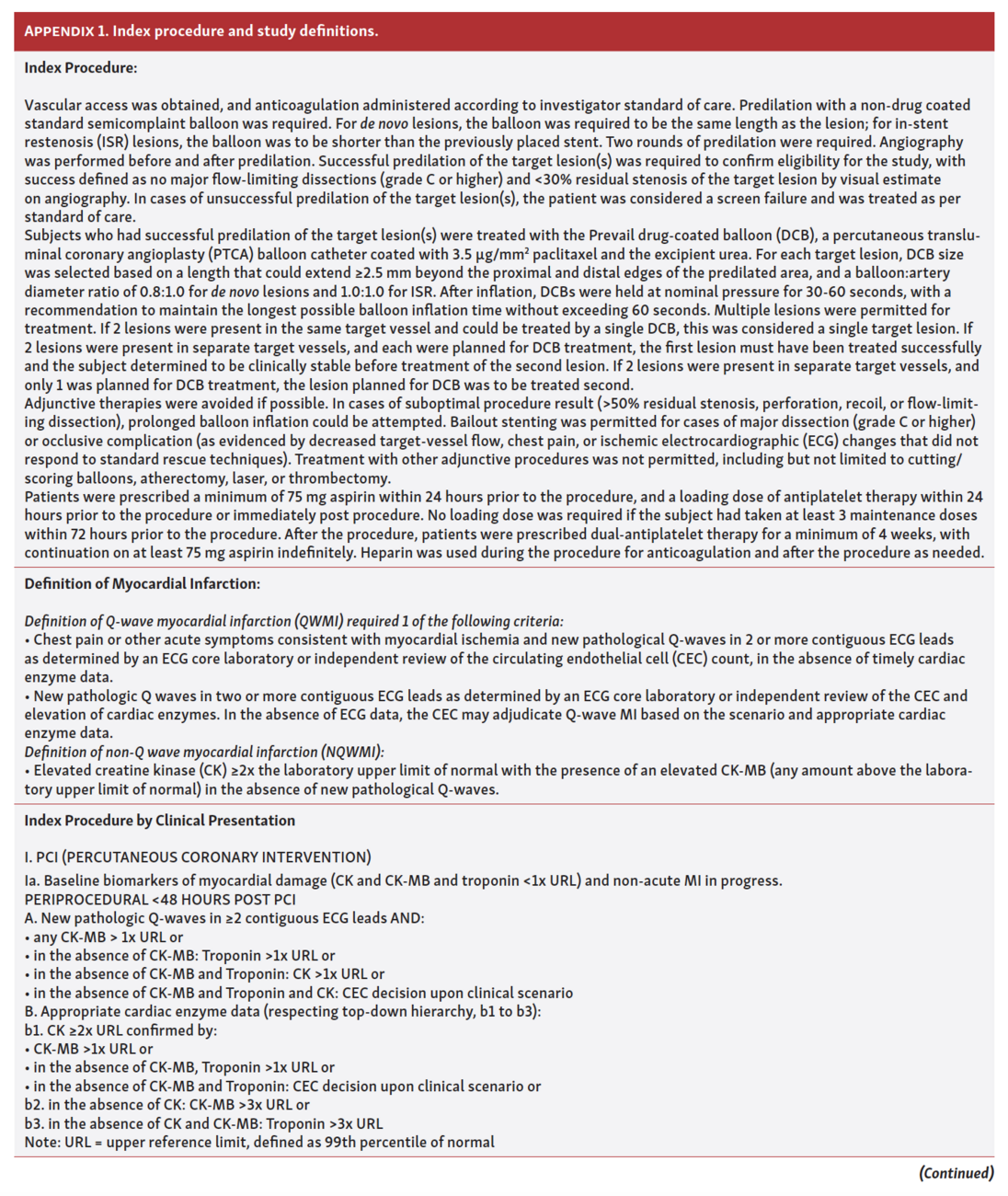
Index procedure. Successful predilation with semi- and/or non-compliant balloons was required (success being documented by angiographic visual estimation of <30% residual stenosis of the target lesion and no major [> grade B] flow-limiting dissection). Angiography was performed before and after predilation. Adjunctive procedures for lesion preparation, such as cutting/scoring balloons, atherectomy, laser, or thrombectomy, were not permitted. Although 23.4% of lesions had moderate or severe calcification, the study excluded lesions that could not be optimally prepared for DCB with non-compliant balloons, as these are lesions that would be more complex and there are minimal data to support the efficacy of DCB over DES in these lesion types. Since this was the first clinical evaluation of this device, it was important to evaluate the DCB in lesions of moderate complexity where the efficacy and safety would be comparable to studies of other devices. Subjects with successful predilation of the target lesion(s) were treated with the Prevail DCB, a PTCA balloon catheter coated with a target dose of 3.5 µg/mm2 paclitaxel and the excipient urea. Multiple lesions that individually met the inclusion and exclusion criteria could be treated with a study device. Lesions treated with the DCB were defined as target lesions. A maximum of 4 lesions could be treated during the index procedure (maximum of 3 target vessels). Two lesions in 1 vessel could not be treated with a DCB. A maximum of 2 vessels with 2 lesions was allowed. A unique DCB was to be used for each lesion.
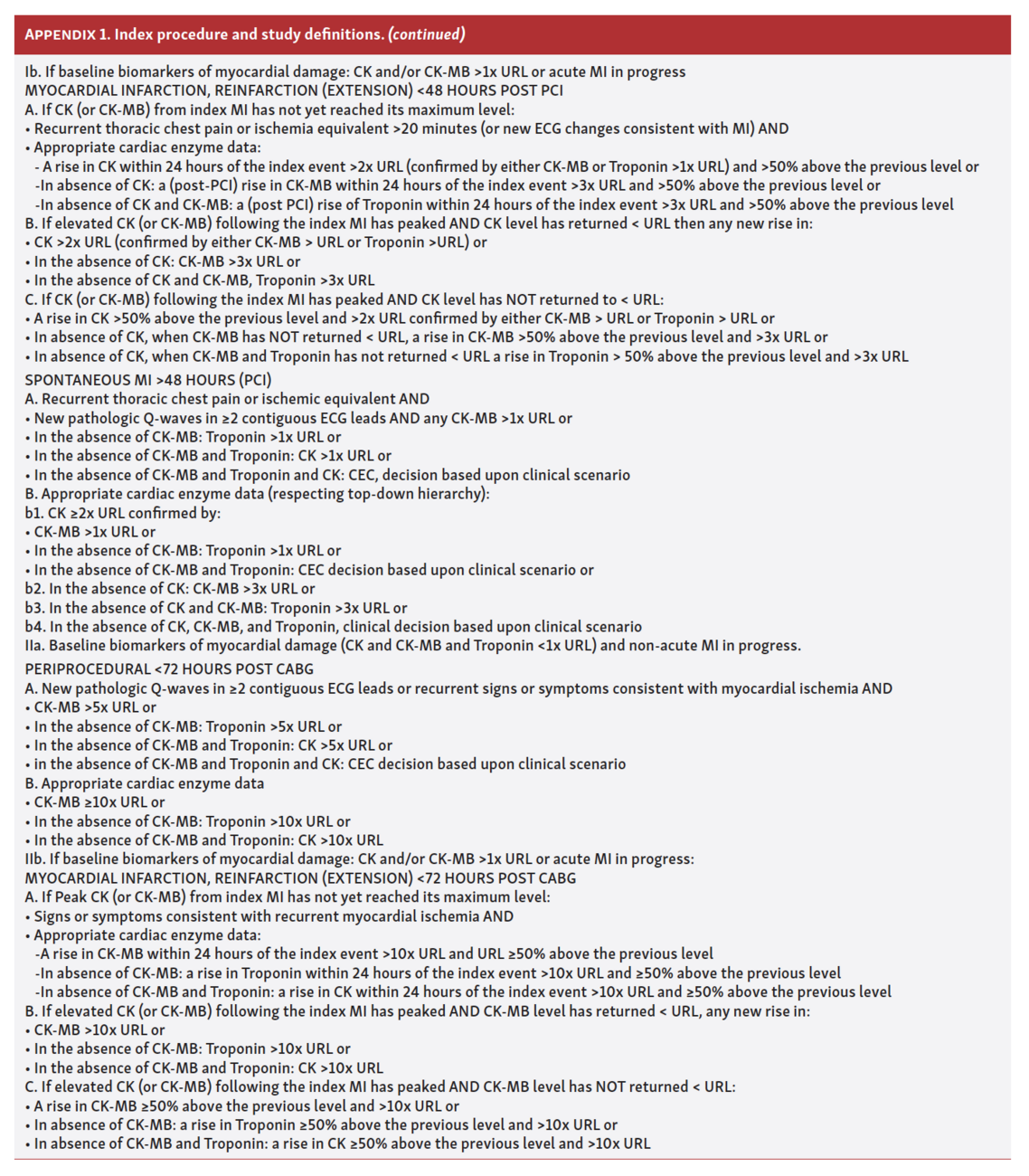
Bailout stenting was permitted for cases of major and/or flow-limiting dissection (grade C or higher) or occlusive complications. Details of the index procedure are provided in Appendix 1 (Part 1) and Appendix 1 (Part 2).
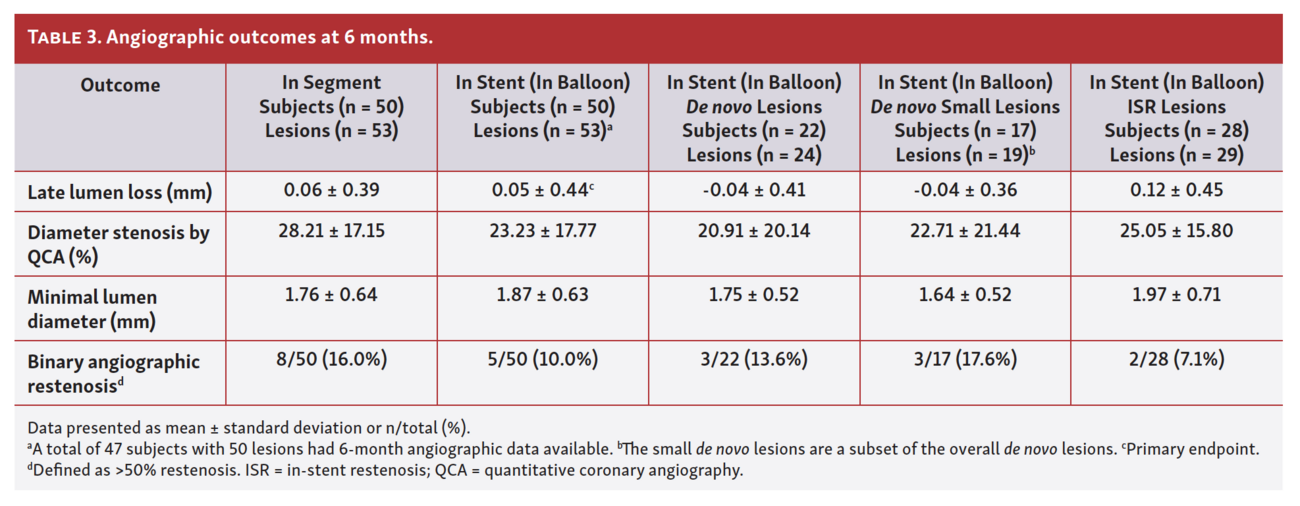
Study endpoints. The primary endpoint was in-stent (in-balloon) late lumen loss (LLL) by quantitative coronary angiography (QCA) at 6 months post procedure. If the mean in-stent (in-balloon) LLL was less than the maximum acceptance rate of 0.50 mm at 6 months, then the study was considered successful. Secondary angiographic endpoints were also measured by QCA at 6 months post procedure and included in-segment LLL, percent diameter stenosis, minimal lumen diameter (MLD), and binary angiographic restenosis (defined as ≥50% diameter stenosis). Besides LLL, all secondary angiographic endpoints were assessed in segment and in stent (in balloon).
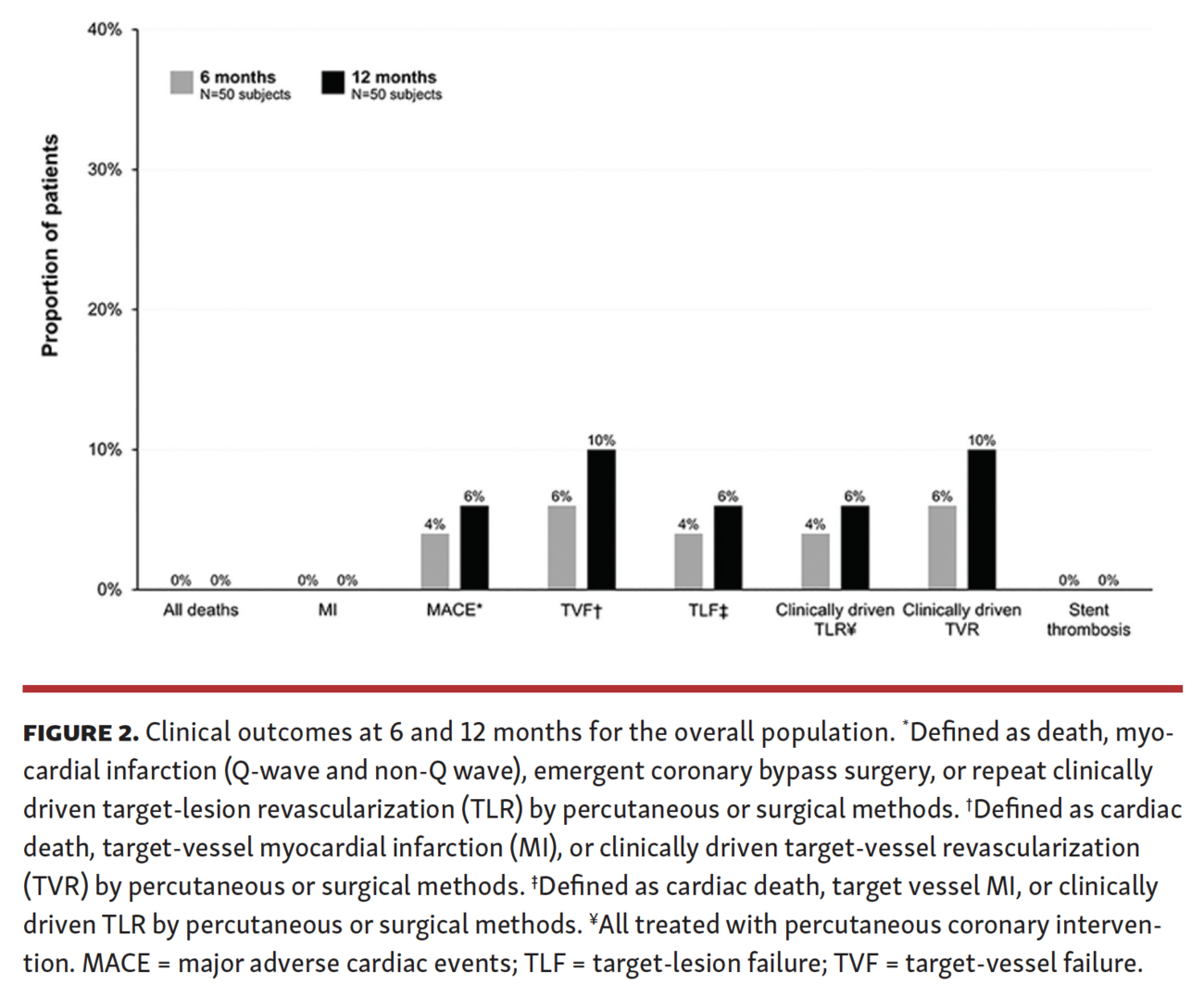
Secondary clinical outcomes were assessed at 30 days, 6 months, and 12 months post procedure for the overall population and by lesion type (de novo and ISR). Clinical endpoints included: all deaths; target-vessel MI; major adverse cardiac event (MACE), defined as a composite of death, MI (Q-wave and non-Q wave), emergent coronary artery bypass graft surgery, or repeat clinically driven target-lesion revascularization (TLR) by percutaneous or surgical methods; target-vessel failure (TVF), defined as cardiac death, target-vessel MI, or clinically driven target-vessel revascularization (TVR) by percutaneous or surgical methods; target-lesion failure (TLF), defined as cardiac death, target-vessel MI, or clinically driven TLR by percutaneous or surgical methods; and stent (lesion) thrombosis, defined according to the Academic Research Consortium.18 MI is defined in detail in Appendix 1 (Part 1) and Appendix 1 (Part 2).
The following procedural outcomes were assessed: device success (attainment of <50% residual stenosis of the target lesion using only the study device); lesion success (attainment of <50% residual stenosis of the target lesion using any percutaneous method); and procedural success (attainment of <50% residual stenosis of the target lesion and no in-hospital MACE).
Statistical analysis. Categorical variables were reported as percentages and counts, and continuous variables were reported as means ± standard deviations. Statistical analyses were performed with SAS, version 9.1 or higher (SAS Institute).
Results
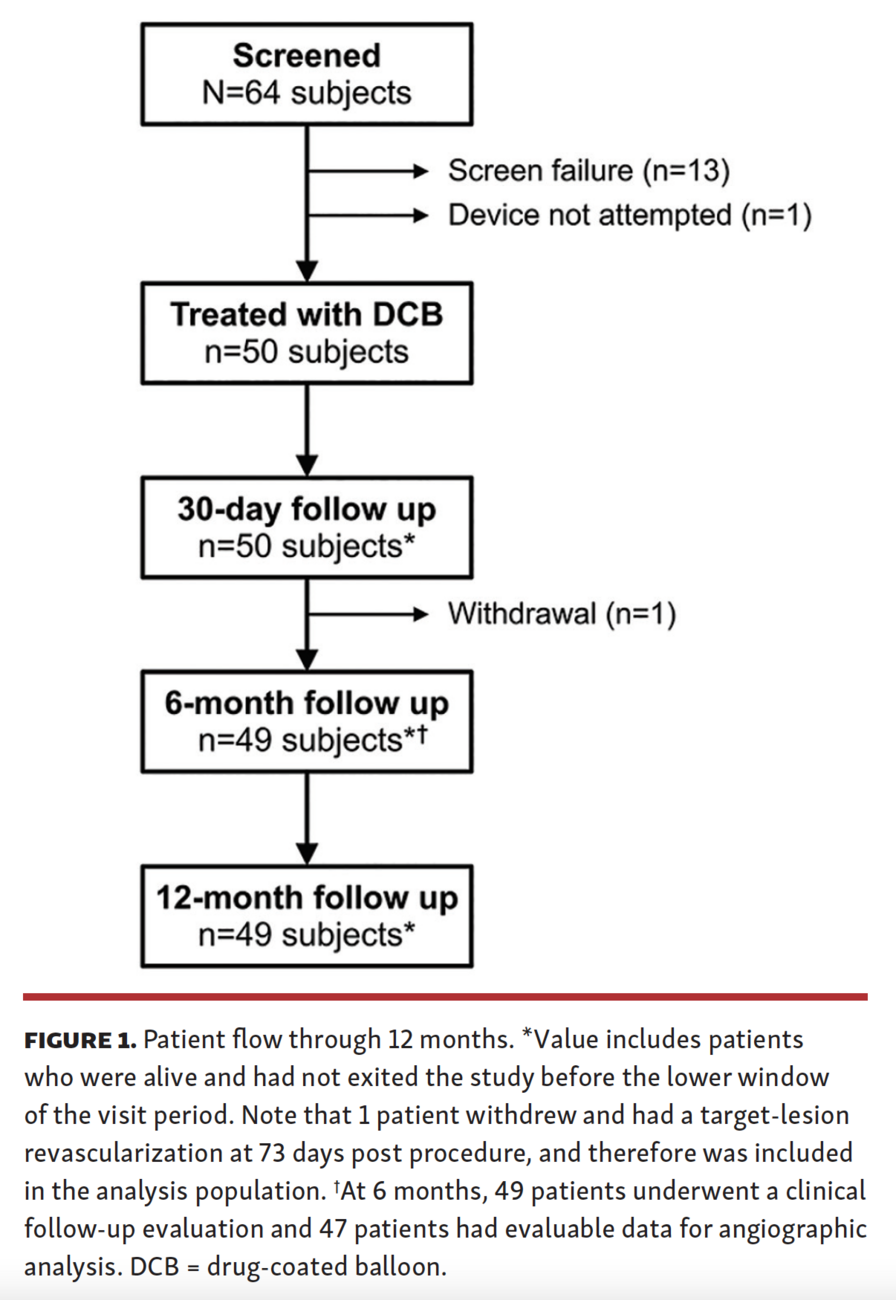
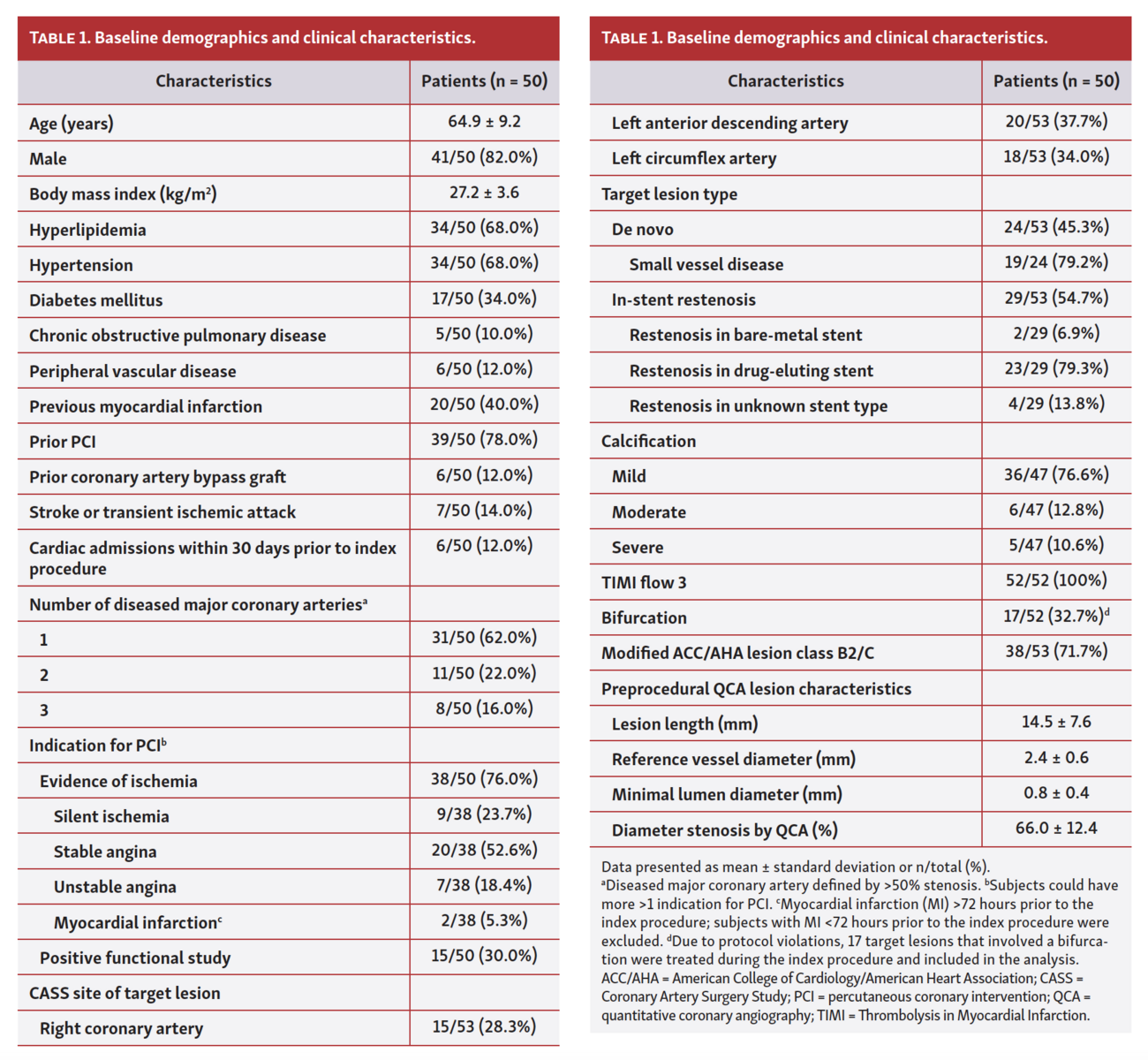
Baseline demographics and clinical characteristics. The study flow chart is depicted in Figure 1. The intent-to-treat population included 50 patients with 53 target lesions. Baseline demographic, clinical, and lesion characteristics are reported in Table 1. The mean age was 64.9 ± 9.2 years and 82.0% were men. Comorbidities were prevalent, including hyperlipidemia (68.0%), hypertension (68.0%), and diabetes (34.0%). Most patients (38/50; 76.0%) had evidence of ischemia, with stable angina being the most prevalent indication for PCI (20/38; 52.6%). The mean lesion length was 14.5 ± 7.6 mm, 45.3% were de novo lesions (of which 79.2% were in small vessels) and the remaining (54.7%) were ISR lesions.
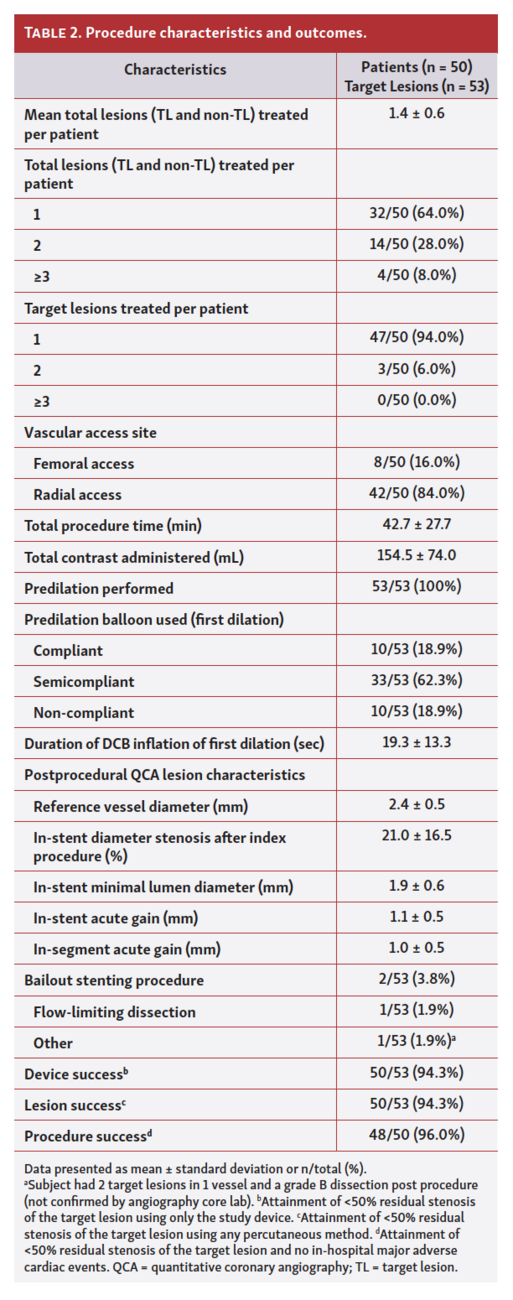
Procedural characteristics and outcomes. Procedural characteristics and outcomes are reported in Table 2. Most patients (94.0%) had 1 target lesion treated during the index procedure, and the remaining patients (6.0%) had 2 target lesions treated. Two lesions (3.8%) required bailout implantation of a DES, 1 for a flow-limiting dissection and 1 with a grade B dissection without compromise of distal flow. Device success was achieved in 50/53 lesions (94.3%), lesion success was achieved in 50/53 lesions (94.3%), and procedural success occurred in 48/50 patients (96.0%).
Angiographic outcomes. The study was successful, with a mean in-stent (in-balloon) LLL of 0.05 ± 0.44 mm at 6 months post procedure, below the predefined performance goal of 0.50 mm. When analyzed by lesion type, the mean in-stent (in-balloon) LLL at 6 months was –0.04 ± 0.41 mm for de novo lesions and 0.12 ± 0.45 mm for ISR lesions. The mean in-stent (in-balloon) diameter stenosis by QCA at 6 months for all target lesions was 23.23 ± 17.77%, and the rate of in-stent (in-balloon) binary angiographic restenosis was 10.0%. Angiographic outcomes are summarized in Table 3.
Clinical outcomes. There were no deaths, MIs, or stent (lesion) thrombosis events within 12 months (Figure 2). The incidence of MACE at 12 months was 6.0%, TVF was 10.0%, and clinically driven TLR was 6.0%. Clinical outcomes by lesion cohort are reported in Supplemental Table S2.
Discussion
PREVAIL was a prospective, multicenter, single-arm study of the paclitaxel-coated Prevail DCB for the treatment of de novo and ISR lesions. The study met the primary endpoint of in-stent (in-balloon) LLL at 6 months post procedure, and the incidence of clinical events within 12 months was low, including no deaths, MIs, or stent (lesion) thromboses. The incidence of clinically driven TLR was also low.
While results cannot be directly compared between studies or specific devices without a head-to-head comparison, clinical outcomes with the Prevail DCB compare favorably to what has been reported for other paclitaxel DCBs at 12 months in similar populations with mixed lesion types, including coronary de novo lesions, ISR lesions, and small-vessel disease.1,5,19,20 While the overall 12-month incidence of MACE in PREVAIL (6.0%) was in the range of what has been reported in these studies (5.7%-21.7%),1,5,19 there was no all-cause death, MI, or stent (lesion) thrombosis in PREVAIL, which is less than what was reported in any of the other studies (4.9%-5.8% for all-cause death, 1.6%-1.7% for MI, and 0.5%-0.9% for stent thrombosis).1,19,20 The MACE rate in PREVAIL was solely due to clinically driven TLR (6.0%), which itself was at the low end of what has been reported for paclitaxel DCBs for mixed lesion types (4.0%-17.8%).1,5,19,20 The DCBs from these previous studies were coated with paclitaxel concentrations of 2 µg/mm2 (Agent; Boston Scientific) or 3 µg/mm2 (SeQuent Please, [B. Braun], IN.PACT Falcon [Medtronic]; Pantera Lux [Biotronik]),1,5,19,20 which is lower than the concentration used in the Prevail DCB (3.5 µg/mm2), suggesting that increased paclitaxel exposure was not associated with worse clinical outcomes through 12 months. More recently, a meta-analysis for randomized controlled trials comparing DCB with non-DCB devices for the treatment of ISR or de novo lesions demonstrated a trend toward lower mortality with paclitaxel-coated balloons.21 Similarly, a recent multicenter, randomized, open-label registry of 2289 patients with symptomatic peripheral artery disease demonstrated no difference in 1-year mortality between patients treated with paclitaxel-coated devices and those with uncoated devices.22
In addition to differing doses of paclitaxel, DCBs vary in terms of balloon technology, drug-coating process, and how the drug is actually delivered to the vessel wall, which may result in different clinical outcomes. For example, the IN.PACT Falcon DCB, coated with 3 µg/mm2 of paclitaxel, was evaluated in the BELLO study, which randomized patients to the DCB and provisional bare-metal stenting vs a paclitaxel-eluting stent. The primary endpoint of in-stent (in-balloon) LLL was met (P<.01 for superiority), and the DCB was associated with similar rates of restenosis and revascularization as the paclitaxel-eluting stent.16 However, similar results were not achieved in the PICCOLETO trial, where the Dior paclitaxel-coated balloon (also 3 µg/mm2 of paclitaxel; Palex Medical) was randomized to the Taxus DES (Boston Scientific), and the trial stopped early when the superiority of the DES was noted. As such, the primary endpoint of percent diameter stenosis at 6 months was not met, with higher rates of both percent diameter stenosis and angiographic restenosis noted in the Dior balloon group. Regardless of the balloon technology used, optimizing lesion preparation and DCB technique are critical to improving clinical outcomes. Tanaka and colleagues23 showed how an optimal angiographic result after predilation predicts better clinical outcomes. As a result, in PREVAIL, patients were only enrolled after the operators were able to achieve an optimal angiographic result as recommended by the recently published International DCB Consensus.24 Angiographic outcomes also compared favorably to those from other DCBs, such as the SeQuent Please DCB, which was recently evaluated in the AGENT ISR randomized trial.25 The 6-month in-stent LLL in that study was 0.39 ± 0.54 mm, compared with 0.12 ± 0.45 mm in this study for ISR patients.
The Prevail DCB, which received CE mark approval in July 2020, leverages technology from the IN.PACT Falcon catheter, SC Euphora Balloon, and FreePac drug coating (all from Medtronic) and incorporates the same key design features of the Euphora platform, including the hydrophilic coating. Prevail DCB incorporates improvements over the first-generation IN.PACT Falcon DCB but is expected to deliver similar clinical performance (ie, no change in clinical effect and intended purpose). Prevail DCB shares the same proven FreePac coating with IN.PACT Falcon DCB, but differs in the delivery system (PowerTrac technology), coating process, target drug dose on the balloon, and size matrix (33 sizes available). The hydrophilic coating is applied to the distal section of the balloon, between the proximal balloon bond and the rapid exchange joint, to allow for optimized application of the FreePac drug coating. The same FreePac drug formulation is used in all IN.PACT DCBs, with the dose density differing. For the Prevail DCB, a target paclitaxel dose density of 3.5 µg/mm2 is applied, compared with 3.0 µg/mm2 used on the IN.PACT Falcon. The angiographic and clinical outcomes reported here for the Prevail DCB are comparable to those reported in the BELLO study from IN.PACT Falcon (for de novo small-vessel disease)16 and a separate study for ISR lesions.26
Despite the inherent limitations when comparing outcomes across studies, the outcomes of the PREVAIL study compare favorably with what has been reported and support the conclusion that the Prevail DCB is safe and effective for the treatment of coronary artery disease, including cases that are associated with lesions that can be challenging to treat, such as ISR and small-vessel disease. As a premarket study with a small sample size and no comparator group, further investigation is needed to support these findings.
Study limitations. Limitations include those typical of a premarket study, including small sample size and a single-arm design without a comparator group. The findings of the present study therefore cannot be directly compared with other coronary DCBs in the absence of a head-to-head comparison.
Conclusion
In a prospective, multicenter, single-arm study of patients with symptomatic ischemic heart disease, treatment of coronary de novo or ISR lesions with the paclitaxel-coated Prevail DCB was associated with favorable LLL at 6 months and low rates of safety events and revascularization at 12 months. While further investigation is required, results of this premarket study suggest that the Prevail paclitaxel DCB is a safe and effective option for the treatment of coronary de novo and ISR lesions.
Acknowledgments. The authors thank the patients involved with the study for their participation. Jessica Dries-Devlin, PhD, CMPP, of Medtronic, and Zachary Harrelson, PhD, provided medical writing support in accordance with Good Publication Practice guidelines (http://www.ismpp.org/gpp3).
Affiliations and Disclosures
From the 1Ospedale San Raffaele – Milano, Milano, Italy; 2Division of Cardiology, Montefiore Medical Center, Albert Einstein College of Medicine, New York, New York; 3St. Antonius Ziekenhuis, Nieuwegein, the Netherlands and HartCentrum, Ziekenhuis Netwerk Antwerpen (ZNA) Middelheim, Antwerp, Belgium; 4Ziekenhuis Oost Limburg – Campus Sint-Jan, Genk, Belgium; 5Onze Lieve Vrouwe Gasthuis – Locatie Oosterpark, Amsterdam, the Netherlands; 6University of Liège Hospital, GIGA Cardiovascular Sciences, Department of Cardiology, CHU SartTilman, Liège, Belgium, and Gruppo Villa Maria Care and Research, Maria Cecilia Hospital, Cotignola, and Anthea Hospital, Bari, Italy; 7Queen Mary Hospital, University of Hong Kong, Hong Kong; 8HagaZiekenhuis, Den Haag, the Netherlands; 9Isala Hartcentrum, Zwolle, the Netherlands; 10University Medical Center Utrecht, Utrecht, the Netherlands; 11Medtronic PLC, Santa Rosa, California; and 12IRCCS Policlinico San Donato, San Donato, Italy.
Funding: This study was supported by Medtronic.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Latib reports honoraria/consultation fees from Abbott, Edwards Lifesciences, CorFlow, ICS, Medtronic, Nuvera, Philips, Supira Medical, NeoChord, and Venus Medtech. Dr Kedhi is a consultant for Medtronic and Abbott. C. Shen and Dr Wetzels are full-time employees and shareholders of Medtronic. Dr Testa reports consultant fees, advisory board, medical proctor, and speaker’s fee honoraria from Abbott, Medtronic, Boston Scientific, Meril Life Sciences, and Concept Medical. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript accepted April 28, 2021.
Address for correspondence: Azeem Latib, MD, Montefiore-Einstein Center for Heart and Vascular Care, 111 East 210th Street, Bronx, NY 10467. Email: alatib@gmail.com
References
1. Basavarajaiah S, Latib A, Shannon J, et al. Drug-eluting balloon in the treatment of in-stent restenosis and diffuse coronary artery disease: real-world experience from our registry. J Interv Cardiol. 2014;27:348-355.
2. Hehrlein C, Dietz U, Kubica J, et al. Twelve-month results of a paclitaxel releasing balloon in patients presenting with in-stent restenosis first-in-man (PEPPER) trial. Cardiovasc Revasc Med. 2012;13:260-264.
3. Unverdorben M, Kleber FX, Heuer H, et al. Treatment of small coronary arteries with a paclitaxel-coated balloon catheter. Clin Res Cardiol. 2010;99:165-174.
4. Unverdorben M, Kleber FX, Heuer H, et al. Treatment of small coronary arteries with a paclitaxel-coated balloon catheter in the PEPCAD I study: are lesions clinically stable from 12 to 36 months? EuroIntervention. 2013;9:620-628.
5. Widder JD, Cortese B, Levesque S, et al. Coronary artery treatment with a urea-based paclitaxel-coated balloon: the European-wide FALCON all-comers DCB registry (FALCON registry). EuroIntervention. 2019;15:e382-e388.
6. Wöhrle J, Zadura M, Möbius-Winkler S, et al. SeQuent Please world wide registry: clinical results of SeQuent Please paclitaxel-coated balloon angioplasty in a large-scale, prospective registry study. J Am Coll Cardiol. 2012;60:1733-1738.
7. Baan J Jr, Claessen BE, Dijk KB, et al. A randomized comparison of paclitaxel-eluting balloon versus everolimus-eluting stent for the treatment of any in-stent restenosis: the DARE trial. JACC Cardiovasc Interv. 2018;11:275-283.
8. Byrne RA, Neumann FJ, Mehilli J, et al. Paclitaxel-eluting balloons, paclitaxel-eluting stents, and balloon angioplasty in patients with restenosis after implantation of a drug-eluting stent (ISAR-DESIRE 3): a randomised, open-label trial. Lancet. 2013;381:461-467.
9. Jensen CJ, Richardt G, Tölg R, et al. Angiographic and clinical performance of a paclitaxel-coated balloon compared to a second-generation sirolimus-eluting stent in patients with in-stent restenosis: the BIOLUX randomised controlled trial. EuroIntervention. 2018;14:1096-1103.
10. Pleva L, Kukla P, Kusnierova P, Zapletalova J, Hlinomaz O. Comparison of the efficacy of paclitaxel-eluting balloon catheters and everolimus-eluting stents in the treatment of coronary in-stent restenosis: the treatment of in-stent restenosis study. Circ Cardiovasc Interv. 2016;9:e003316.
11. Rittger H, Brachmann J, Sinha AM, et al. A randomized, multicenter, single-blinded trial comparing paclitaxel-coated balloon angioplasty with plain balloon angioplasty in drug-eluting stent restenosis: the PEPCAD-DES study. J Am Coll Cardiol. 2012;59:1377-1382.
12. Unverdorben M, Vallbracht C, Cremers B, et al. Paclitaxel-coated balloon catheter versus paclitaxel-coated stent for the treatment of coronary in-stent restenosis. Circulation. 2009;119:2986-2994.
13. Wong YTA, Kang DY, Lee JB, et al. Comparison of drug-eluting stents and drug-coated balloon for the treatment of drug-eluting coronary stent restenosis: a randomized RESTORE trial. Am Heart J. 2018;197:35-42.
14. Xu B, Gao R, Wang J, et al. A prospective, multicenter, randomized trial of paclitaxel-coated balloon versus paclitaxel-eluting stent for the treatment of drug-eluting stent in-stent restenosis: results from the PEPCAD China ISR trial. JACC Cardiovasc Interv. 2014;7:204-211.
15. Jeger RV, Farah A, Ohlow MA, et al. Drug-coated balloons for small coronary artery disease (BASKET-SMALL 2): an open-label randomised non-inferiority trial. Lancet. 2018;392:849-856.
16. Latib A, Colombo A, Castriota F, et al. A randomized multicenter study comparing a paclitaxel drug-eluting balloon with a paclitaxel-eluting stent in small coronary vessels: the BELLO (balloon elution and late loss optimization) study. J Am Coll Cardiol. 2012;60:2473-2480.
17. Tang Y, Qiao S, Su X, et al. Drug-coated balloon versus drug-eluting stent for small-vessel disease: the RESTORE SVD China randomized trial. JACC Cardiovasc Interv. 2018;11:2381-2392.
18. Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation. 2007;115:2344-2351.
19. Toelg R, Merkely B, Erglis A, et al. Coronary artery treatment with paclitaxel-coated balloon using a BTHC excipient: clinical results of the international real-world DELUX registry. EuroIntervention. 2014;10:591-599.
20. Uhlemann M, Möbius-Winkler S, Adam J, et al. The Leipzig prospective drug-eluting balloon-registry — outcome of 484 consecutive patients treated for coronary in-stent restenosis and de novo lesions using paclitaxel-coated balloons. Circ J. 2016;80:379-386.
21. Scheller B, Vukadinovic D, Jeger R, et al. Survival after coronary revascularization with paclitaxel-coated balloons. J Am Coll Cardiol. 2020;75:1017-1028.
22. Nordanstig J, James S, Andersson M, et al. Mortality with paclitaxel-coated devices in peripheral artery disease. N Engl J Med. 2020;383:2538-2546.
23. Tanaka A, Latib A, Jabbour RJ, et al. Impact of angiographic result after predilatation on outcome after drug-coated balloon treatment of in-stent coronary restenosis. Am J Cardiol. 2016;118:1460-1465.
24. Jeger RV, Eccleshall S, Wan Ahmad WA, et al. Drug-coated balloons for coronary artery disease: third report of the International DCB Consensus Group. JACC Cardiovasc Interv. 2020;13:1391-1402. Epub 2020 May 27.
25. Hamm CW, Dorr O, Woehrle J, et al. A multicentre, randomised controlled clinical study of drug-coated balloons for the treatment of coronary in-stent restenosis. EuroIntervention. 2020;16:e328-e334.
26. Basavarajaiah S, Naganuma T, Latib A, et al. Treatment of drug-eluting stent restenosis: comparison between drug-eluting balloon versus second-generation drug-eluting stents from a retrospective observational study. Catheter Cardiovasc Interv. 2016;88:522-528.










