


Platelet FcγRIIa Expression in Patients With Stable Coronary Artery Disease
Abstract
Objectives. FcɣRIIa amplifies platelet activation and greater expression increases platelet reactivity. In patients with myocardial infarction (MI), high platelet FcɣRIIa identifies patients with an approximately 4-fold greater risk of MI, stroke, and death. We compared platelet FcɣRIIa in 2 groups: (1) patients who had not had an MI in the previous year and were undergoing cardiac catheterization and percutaneous coronary intervention (PCI) labeled as stable coronary artery disease (CAD), and (2) previously obtained results in patients with MI (n = 197).
Methods. Patients undergoing cardiac catheterization and PCI were enrolled. FcɣRIIa expression was quantified with the use of flow cytometry. Comparisons were made with Mann-Whitney Rank Sum Test and Chi Squared analysis. Significance was defined as P < .05.
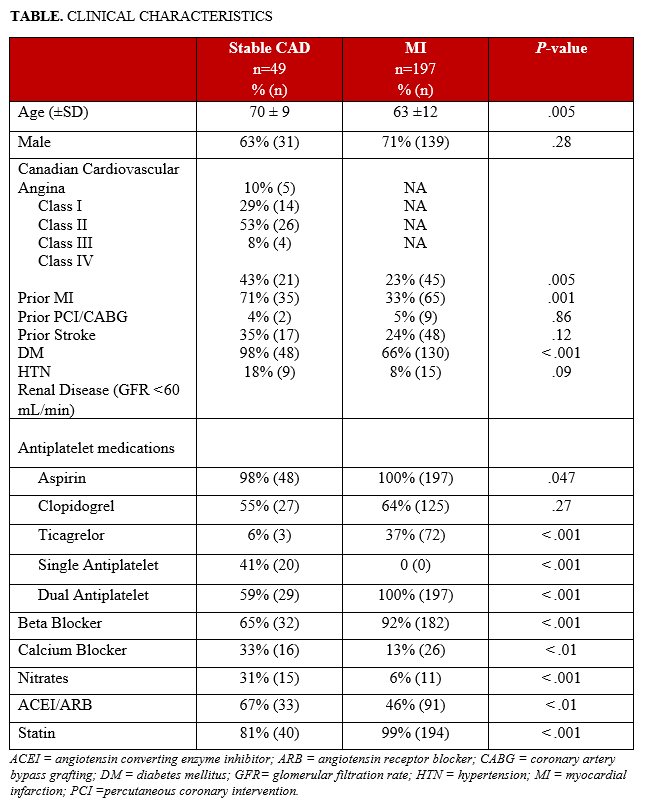
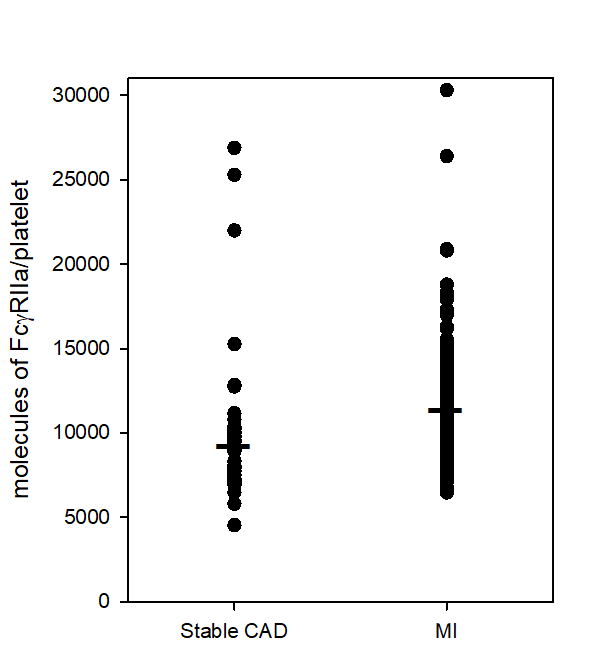
Results. Compared to patients with MI, patients with stable CAD (n = 49) were older (70 ± 9 years vs 63 ± 12 years) and were more likely to have had prior MI (43% vs 23%), prior revascularization (62% vs 33%), diabetes (35% vs 24%), and hypertension (98% vs 66%). In patients with stable CAD, platelet FcɣRIIa was, on average, lower than that seen in patients with acute MI (9746 ± 4316 vs 11 479 ± 2405 molecules/platelet, P < .001). Patients with stable CAD exhibited a range of platelet FcɣRIIa (~4500 to ~27 000 molecules/platelet) similar to that seen in acute MI patients (~6500 to ~30 000 molecules/platelet).
Conclusions. Compared to patients with MI, patients with stable CAD had, on average, lower platelet FcɣRIIa. However, the range of platelet FcɣRIIa was similar to that seen in patients with MI. These results support future studies designed to assess the prognostic implications of platelet FcɣRIIa in patients with stable CAD.
Introduction
FcγRIIa on the surface of platelets binds to an Ig‐bound (opsonized) entity such as a bacterium, and this binding triggers platelet activation.1,2 Another function of FcγRIIa is to amplify the activation of platelets. Cytoskeletal rearrangement that occurs during the activation of platelets leads to the clustering of FcɣRIIa in signaling domains referred to as lipid rafts. This clustering leads to crosslinking of FcɣRIIa and downstream signaling that amplifies the activation of platelets.3,4 In previous work, we have demonstrated that greater platelet expression of FcγRIIa is associated with greater activation of platelets in response to a range of agonists including thrombin, adenosine diphosphate, and platelet activating factor and a collagen mimetic, convulxin.5
A broad range of platelet expression of FcɣRIIa has been identified in patients with atherosclerotic vascular disease that ranges from low expression seen in healthy young subjects to high expression (> 4-fold higher). 6,7 Increased platelet FcɣRIIa in patients with myocardial infarction (MI) identified individuals with an approximately 4-fold greater risk of subsequent MI, stroke, and death.6 The objective of this study was to compare both the median and range of platelet FcɣRIIa in patients who had not had an MI in the previous year, and were undergoing cardiac catheterization and percutaneous coronary intervention (PCI) labeled as stable coronary artery disease (CAD) with results obtained previously in patients with MI.
Methods
The aim of this study was to compare platelet expression of FcɣRIIa in patients with stable CAD undergoing PCI with that observed previously in patients with acute MI. Blood was taken from patients undergoing PCI. Authors have conformed to institutional guidelines and those of the American Physiological Society.
Patients. Patients provided written informed consent to participate in our protocol, which was approved by the University of Vermont Institutional Review Board. We enrolled patients undergoing cardiac catheterization at the University of Vermont Medical Center between May and December 2021. Analysis of our previous study on MI patients demonstrated a broad range of platelet FcɣRIIa in patients at increased risk based on clinical characteristics.8 Because of this, we chose to enroll patients at increased risk based on clinical factors.9 Inclusion criteria included at least 2 of the following risk factors: age greater than or equal to 65, multivessel CAD (≥ 2 vessels or left main with a stenosis of ≥ 50%), chronic kidney disease (estimated glomerular filtration rate [GFR] below 60 mL/min/1.73 m2), diabetes mellitus, or prior history of myocardial infarction (> 1 year before PCI). Exclusion criteria included MI in the previous year, indication for long-term oral anticoagulation (eg, atrial fibrillation), or non-cardiovascular comorbidities that limited estimated survival to less than 3 years.
After written informed consent was obtained, patient characteristics were recorded, and a sample of blood was drawn into a standard blue top tube (anticoagulated with 3.2% trisodium citrate). Patients with MI were recruited for a previous study6 shortly before discharge from the hospital after MI. Patients with both ST elevation MI and non-ST elevation MI were enrolled between July 2015 and January 2017. Exclusion criteria were the same as described for this study.
Platelet expression of FcɣRIIa. Flow cytometry was used to quantify platelet FcɣRIIa. Aliquots (3 µL) of whole blood were added to tubes containing HEPES-Tyrode’s buffer plus 2 antibodies. A phycoerythrin labeled anti-CD32 was used to quantify FcɣRIIa, and a phycoerythrin-CY5 anti-CD42b antibody was used to identify platelets. After 15 minutes, red blood cells were lysed, and platelets were fixed by the addition of 100 μL of Optilyse C (Beckman Coulter). After dilution with 1 mL of HEPES-Tyrode’s buffer, samples were analyzed with the use of Attune NXT flow cytometer (Thermo Fisher). Platelets were identified by size and expression of CD42b. To quantify molecules of FcɣRIIa/platelet, the flow cytometry output (mean fluorescence intensity) was calibrated with the use of Quantum simply cellular anti-mouse beads (Bangs Laboratories). Platelet expression of FcγRIIa was quantified with the use of QuickCal software (Bangs Laboratories).
Statistical analysis. Platelet expression of FcɣRIIa was not normally distributed. For this reason, platelet expression of FcɣRIIa in patients with stable CAD was compared with that in patients with MI with the use of a Mann-Whitney Rank Sum Test. Clinical characteristics were compared with a Chi Squared analysis. Significance was defined as P < .05
Results
Patients with stable CAD (n = 49) were older and were more likely to have had prior MI, prior revascularization, diabetes, and hypertension compared with patients enrolled in our previous study of MI (n = 197, Table).6
Platelet FcɣRIIa expression. In patients with stable CAD, platelet FcɣRIIa was, on average, lower than that seen in patients with acute MI (stable CAD mean = 9746; median = 8908; SD = 4316; MI mean = 11 479; median = 11 211; SD = 2405 molecules/platelet, P < .001). Patients with stable CAD exhibited a range of platelet FcɣRIIa (~4500 to ~27 000 molecules/platelet) similar to that seen in acute MI patients (~6500 to ~30 000 molecules/platelet) (Figure).
Discussion
FcɣRIIa is a cell surface receptor that has an addition function of amplifying platelet activation.3,4 We found that greater platelet expression of FcɣRIIa was associated with increased platelet reactivity.5 Increased platelet reactivity has been consistently associated with a greater risk of cardiovascular events.10,11 Consistent with these observations, we found that greater platelet expression of FcɣRIIa was associated with an approximately 4-fold greater risk of MI, stroke, and death in patients enrolled shortly after MI.6 A broad range of platelet expression of FcɣRIIa was seen in patients with MI.
This study was designed to compare platelet FcɣRIIa in patients with stable CAD undergoing PCI with that in our prior study of MI. We found that the mean and median platelet expression of FcɣRIIa was lower in patients with stable CAD, however the range of expression was similar. Accordingly, while platelet expression of FcɣRIIa was, on average, lower in patients with stable CAD undergoing PCI, we found both low- and high-platelet FcɣRIIa similar to that seen in patients shortly after MI.
We propose that platelet FcɣRIIa is a biomarker capable of discriminating risk of subsequent cardiovascular events. The ability to discriminate risk has been demonstrated in patients with MI.6 The broad range of platelet expression demonstrated in patients with MI as well as stable CAD supports delineation of high and low expression corresponding to high and low risk of cardiovascular events. Mechanistically, platelet FcɣRIIa augments platelet reactivity.3-5 Accordingly, quantifying platelet FcɣRIIa leverages the prognostic implications of high platelet reactivity demonstrated by platelet function tests and overcomes key weaknesses.
The prognostic implications of high platelet reactivity have been demonstrated in more than 100 studies (> 22 000 patients) with CAD.10,11 Based on these consistent findings, 2 large clinical trials were designed to determine whether platelet function testing could effectively guide antiplatelet therapy. These 2 trials failed to demonstrate that currently available tests of platelet function can be used to guide treatment.12,13 Based on these findings, consensus guidelines recommend against the use of platelet function testing to guide individualized care of patients.14
Platelet function tests have inherent limitations. Platelets must be activated in vitro, and thus technical aspects such as the method of phlebotomy, the choice and concentration of agonist, and the use of anticoagulant influence results.15-17 We have hypothesized that intraindividual variability is a key determinant of the inability of platelet function tests to guide individualized treatment. It has been known for decades that platelet function varies substantially over the course of just 1 day.18 Consistent with this, substantial intraindividual variability has been demonstrated in patients with CAD,19-21 with more than 40% of patients exhibiting a greater than 20% change in platelet function over the course of 2 weeks.20 Thus, a measurement of high platelet reactivity may not reflect consistently high platelet reactivity over time, in the same way that a high random glucose measurement may not accurately reflect glycemic control.
Quantifying platelet expression of FcɣRIIa mitigates many limitations of platelet function tests. It does not require activation of platelets in vitro. We have found that neither anticoagulants nor antiplatelet agents alter quantification of FcɣRIIa.7 We have found that interferon ɣ increases megakaryocyte production of FcɣRIIa.22 Because megakaryocyte production determines platelet expression of FcɣRIIa, platelet expression of FcɣRIIa would be expected to exhibit less variability over the course of 1 month, an observation that we have confirmed in healthy subjects.7 We hypothesize that the substantially lower intra-individual variability will differentiate this test and enable it to guide individualized care. Future studies will assess the variability of platelet FcɣRIIa over time in patients with CAD.
The prognostic implications of high platelet reactivity measured with platelet function tests have been demonstrated in patients with acute coronary syndromes as well as in patients with stable CAD undergoing PCI.10,11 Consistent with these observations, we anticipate that platelet FcɣRIIa will have similar prognostic implications in patients with MI and those with stable CAD. This study contributes to the assessment of this biomarker by demonstrating a similar range of expression in patients with stable CAD and MI. Identification of patients at low risk of subsequent cardiovascular events would support a strategy of early transition to less powerful antiplatelet therapy (eg, an early transition from dual antiplatelet therapy to monotherapy). Conversely, patients at high risk of subsequent cardiovascular events are more likely to benefit from long-term treatment with more powerful therapy.
Conclusions
We found that, compared to patients with MI, patients with stable CAD undergoing PCI had, on average, lower platelet FcɣRIIa. The range of platelet FcɣRIIa was similar in patients with stable CAD undergoing PCI compared with that seen in patients with MI. These results support our plans for future studies designed to assess the prognostic implications of platelet FcɣRIIa in patients with stable CAD.
Affiliations and Disclosures
From the Department of Medicine, Cardiovascular Research Institute, The University of Vermont, Burlington, Vermont, USA.
Acknowledgments: The authors wish to thank Heidi Taatjes for her technical support in performing the platelet assays.
Disclosures: Dr Schneider is the named inventor on a patent (Patent No.: 10,502,737) that proposes the use of FcγRIIa for assaying platelet reactivity and treatment selection. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Funding: This work was supported by institutional funds of the corresponding author.
Address for correspondence: David J. Schneider, MD, Cardiovascular Research Institute, The University of Vermont, 308 S. Park Drive, Colchester, VT 05446, USA. Email: David.Schneider@med.uvm.edu
References
- Arman M, Krauel K, Tilley DO, et al. Amplification of bacteria-induced platelet activation is triggered by FcγRIIA, integrin αIIbβ3, and platelet factor 4. Blood. 2014;123(20):3166-3174. doi: 10.1182/blood-2013-11-540526
- Kelton JG, Sheridan D, Santos A, et al. Heparin-induced thrombocytopenia: laboratory studies. Blood. 1988;72(3):925-930.
- Boylan B, Gao C, Rathore V, Gill JC, Newman DK, Newman PJ. Identification of FcgammaRIIa as the ITAM-bearing receptor mediating alphaIIbbeta3 outside-in integrin signaling in human platelets. Blood. 2008;112(7):2780-2786. doi: 10.1182/blood-2008-02-142125
- Lova P, Paganini S, Sinigaglia F, Balduini C, Torti M. A Gi-dependent pathway is required for activation of the small GTPase Rap1B in human platelets. J Biol Chem. 2002;277(14):12009-12015. doi: 10.1074/jbc.M111803200
- Serrano FA, El-Shahawy M, Solomon RJ, Sobel BE, Schneider DJ. Increased platelet expression of FcGammaRIIa and its potential impact on platelet reactivity in patients with end stage renal disease. Thromb J. 2007;5:7. doi:10.1186/1477-9560-5-7
- Schneider DJ, McMahon SR, Chava S, et al. FcɣRIIa: a new cardiovascular risk marker. J Am Coll Cardiol. 2018;72(2):237-238. doi: 10.1016/j.jacc.2018.04.046
- McMahon SR, Chava S, Taatjes-Sommer HS, Meagher S, Brummel-Ziedins KE, Schneider DJ. Variation in platelet expression of FcγRIIa after MI. J Thromb Thrombolysis. 2019;48(1):88-94. doi: 10.1007/s11239-019-01852-7
- Schneider DJ, McMahon SR, Ehle GL, Chava S, Taatjes-Sommer HS, Meagher S. Assessment of cardiovascular risk by the combination of clinical risk scores plus platelet expression of FcγRIIa. Am J Cardiol. 2020;125(5):670-672. doi: 10.1016/j.amjcard.2019.12.008
- Droppa M, Tschernow D, Müller KAL, et al. Evaluation of clinical risk factors to predict high on-treatment platelet reactivity and outcome in patients with stable coronary artery disease (PREDICT-STABLE). PloS One. 2015;10(3):e0121620. doi:10.1371/journal.pone.0121620
- Wiseman PP, Roest M, Asselbergs FW, et al. Platelet-reactivity tests identify patients at risk of secondary cardiovascular events: a systematic review and meta-analysis. J Thromb Haemost. 2014;12(5):736-747. doi: 10.1111/jth.12538
- Reny JL, Fontana P, Hochholzer W, et al. Vascular risk levels affect the predictive value of platelet reactivity for the occurrence of MACE in patients on clopidogrel. Systematic review and meta-analysis of individual patient data. Thromb Haemost. 2016;115(4):844-855. doi: 10.1160/TH15-09-0742
- Price MJ, Berger PB, Teirstein PS, et al; GRAVITAS Investigators. Standard- vs high-dose clopidogrel based on platelet function testing after percutaneous coronary intervention: the GRAVITAS randomized trial. JAMA. 2011;305:1097-1105. doi: 10.1001/jama.2011.290
- Collet JP, Cuisset T, Rangé G, et al; ARCTIC Investigators. Bedside monitoring to adjust antiplatelet therapy for coronary stenting. N Engl J Med. 2012;367:2100-2109. doi: 10.1056/NEJMoa1209979
- Sibbing D, Aradi D, Alexopoulos D, et al. Updated expert consensus statement on platelet function and genetic testing for guiding P2Y(12) receptor inhibitor treatment in percutaneous coronary intervention. JACC Cardiovasc Interv. 2019;12(16):1521-1537. soi: 10.1016/j.jcin.2019.03.034
- Schneider DJ, Tracy PB, Mann KG, Sobel BE. Differential effects of anticoagulants on the activation of platelets ex vivo. Circulation. 1997;96(9):2877-2883. doi: 10.1161/01.cir.96.9.2877
- Madsen NJ, Holmes CE, Serrano FA, Sobel BE, Schneider DJ. Influence of preparative procedures on assay of platelet function and apparent effects of antiplatelet agents. Am J Cardiol. 2007;100(4):722-727. doi: 10.1016/j.amjcard.2007.03.091
- Lippi G, Ippolito L, Zobbi V, Sandei F, Favaloro EJ. Sample collection and platelet function testing: influence of vacuum or aspiration principle on PFA-100 test results. Blood Coagul Fibrinolysis. 2013;24(6):666-669. doi: 10.1097/MBC.0b013e32835fada7
- Brezinski DA, Tofler GH, Muller JE, et al. Morning increase in platelet aggregability. Association with assumption of the upright posture. Circulation. 1988;78(1):35-40. doi: 10.1161/01.cir.78.1.35
- Frelinger AL III, Bhatt DL, Lee RD, et al. Clopidogrel pharmacokinetics and pharmacodynamics vary widely despite exclusion or control of polymorphisms (CYP2C19, ABCB1, PON1), noncompliance, diet, smoking, co-medications (including proton pump inhibitors), and pre-existent variability in platelet. J Am Coll Cardiol. 2013;61(8):872-879. doi: 10.1016/j.jacc.2012.11.040
- Hochholzer W, Ruff CT, Mesa RA, et al. Variability of individual platelet reactivity over time in patients treated with clopidogrel: insights from ELEVATE-TIMI 56 trial. J Am Coll Cardiol. 2014;64(4):361-368. doi: 10.1016/j.jacc.2014.03.051
- Nührenberg TG, Stratz C, Leggewie S, et al. Temporal variability in the antiplatelet effects of clopidogrel and aspirin after elective drug-eluting stent implantation. An ADAPT-DES substudy. Thromb Haemost. 2015;114(5):1020-1027. doi: 10.1160/TH15-03-0257
- Schneider DJ, Taatjes-Sommer HS. Augmentation of megakaryocyte expression of FcgammaRIIa by interferon gamma. Arterioscler Thromb Vasc Biol. 2009;29(7):1138-1143. doi: 10.1161/ATVBAHA.109.187567













