

True Efficacy of LAA Closure: Patient Outcomes on Long-term Single-Antiplatelet or No Therapy: Insights From the EWOLUTION Registry
Abstract
Background. Left atrial appendage occlusion (LAAO) is recommended for patients with atrial fibrillation at increased stroke risk, where effective long-term oral anticoagulation (OAC) is not feasible. In order to assess long-term safety of LAAO with aspirin monotherapy or no therapy, we aimed to report on patients with the Watchman LAAO device (Boston Scientific) once postimplantation intensified antiplatelet or anticoagulation therapy is discontinued. Methods. A total of 1025 patients scheduled for elective LAAO therapy prospectively consented for participation in the EWOLUTION registry; 1005 patients received a successful implant and were followed for 2 years. We identified 766 patients in EWOLUTION on single-antiplatelet therapy (SAPT; n = 639) or no therapy (n = 127) for ≥1 year following LAAO. Results. Three to 6 months after LAAO, 766 patients were switched to SAPT or no therapy and were followed for at least 1 year until the study’s conclusion or with events while on SAPT/no therapy; mean time on SAPT/no therapy was 536.56 ± 177.59 days. Patients experienced 1.4 ischemic strokes per 100 patient years (PY) despite a CHA2DS2-VASC score of 4.3 ± 1.6. Major nonprocedural bleeding rates were low, with 1.3 major bleeds per 100 PY with a mean HAS-BLED score of 2.2 ± 1.2. Furthermore, the ischemic stroke rate in the SAPT/no-therapy subgroup was similar to the whole EWOLUTION collective and high-risk subgroups; the bleeding rate was even lower. When analyzed separately, strokes (2.1/100 PY) and bleedings (1.4/100 PY) of the no-therapy subgroup were similar to patients on SAPT (strokes 0.7/100 PY [P=.70]; bleedings 1.4/100 PY [P=.90]). Conclusions. Outcome data of patients on SAPT/no therapy for ≥1 year following Watchman implantation in the EWOLUTION registry suggest the efficacy and safety of LAAO.
J INVASIVE CARDIOL 2022;34(5):E348-E355.
Key words: atrial fibrillation, bleeding, left atrial appendage occlusion, stroke
Non-vitamin K oral anticoagulants (NOACs) have a favorable risk-benefit profile, yet extracranial bleeding (including gastrointestinal bleeding) is not reduced under NOAC therapy at adequate, effective drug doses compared with warfarin therapy.1 Interventional left atrial appendage occlusion (LAAO) is able to reduce the stroke risk in atrial fibrillation (AF) patients with relative or absolute contraindication to long-term oral anticoagulation (OAC) and has emerged as an attractive alternative. Current European Society of Cardiology (ESC) and American Heart Association guidelines recommend a class IIb, level of evidence B for LAAO in patients unsuitable for OAC as the randomized trials vs anticoagulation were performed at times where only warfarin was available and in patients tolerant to OAC.2,3 A meta-analysis of the final 5-year outcome data of the PROTECT-AF and PREVAIL randomized controlled trials showed that Watchman LAAO (Boston Scientific Corporation) was noninferior to warfarin therapy for the prevention of stroke, while nonprocedural bleeding and mortality were lower in the device arm.4 A new, randomized study (the Prague-17 trial) comparing LAAO with NOAC therapy in an all-comers population finds LAAO noninferior to NOAC therapy with a combined endpoint.5
In addition to these controlled trials, there is growing evidence from large multicenter registries supporting this interventional approach for stroke prevention as being safe.6,7 The EWOLUTION registry provides prospective, real-world data from Europe on LAAO employing the Watchman device following the ESC guideline recommendation.6,8 The overall 2-year results showed consistently low rates of stroke and nonprocedural bleeding.6 Herein, we report on LAAO efficacy and safety in a specific EWOLUTION subgroup: 766 patients after discontinuation of the intensified antiplatelet/OAC regime and on single-antiplatelet therapy (SAPT) or no therapy for ≥1 year following LAAO. We compared the observed event rates with the entire EWOLUTION cohort, including high-risk subgroups previously described (patients with history of ischemic/hemorrhagic stroke, bleeding, and elderly [defined as patients ≥85 years old]).6,9
Methods
The outline of the study has been previously described in detail.6,10 EWOLUTION is a multicenter, prospective, all-comer, nonrandomized cohort registry regarding the safety and efficacy of LAAO employing the Watchman device. The study adhered to international rules for scientific studies and the principles of the Declaration of Helsinki, with local ethics committee approval at all participating centers (ClinicalTrials.gov identifier NCT01972282). Decisions regarding LAAO as well as postprocedural drug therapy were at the discretion of the investigators; centers were encouraged to recruit consecutive patients to represent real-life practice and avoid selection bias. At least 83% (39 of the 47 participating centers) confirmed that they enrolled consecutive patients. All centers were monitored by an outside contract research organization. The Medical Safety Group (MSG) of the study sponsor (Boston Scientific Corporation) additionally reviewed events and relevant source documents. The electronic clinical report form provided fields for anticipated serious adverse events such as procedure-specific events (eg, perforation, tamponade, device embolization), neurological events, device thrombosis, and bleeding according to the Bleeding Academic Research Consortium criteria. Diagnostic criteria for stroke, transient ischemic attack, and bleeding (life threatening, major and minor bleeding) are in adherence to the definitions provided by the Munich consensus document on definitions, endpoints, and data collection requirements for LAAO.11
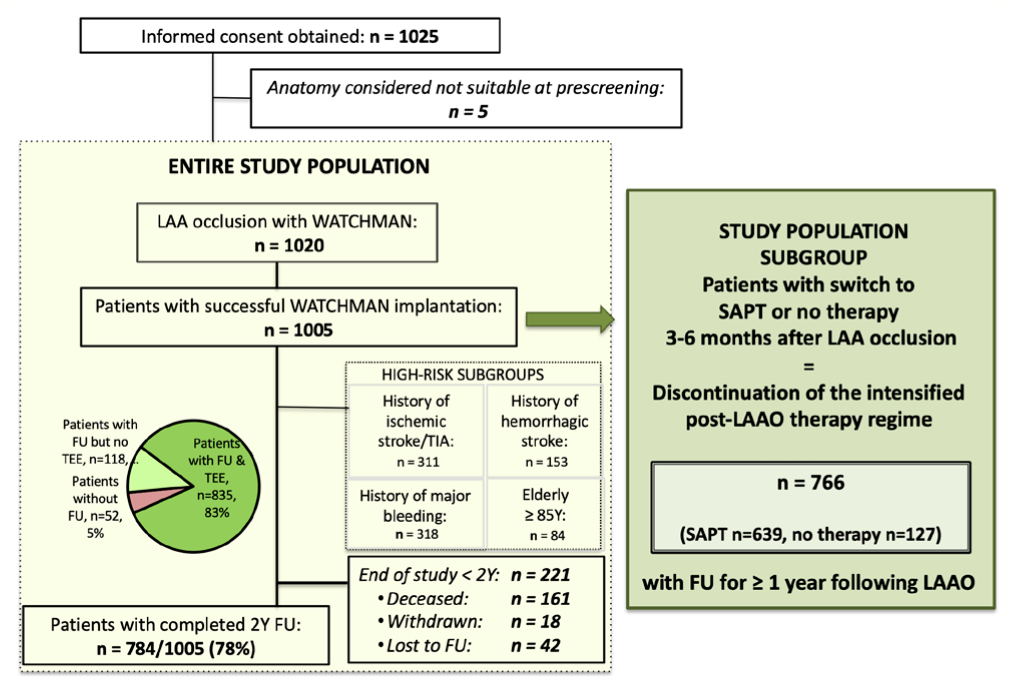
Study enrollment occurred from October 2013 to May 2015. A total of 47 centers in 13 countries recruited 1025 patients (Figure 1); 1005 patients underwent successful implantation of a Watchman device employing current techniques. Follow-up was according to the local institutions’ standards of care up to 2 years post enrollment. At the time of the final 2-year analysis, 784/1005 patients (78%) completed the 2-year follow-up period and 835/1005 (83%) had at least 1 transesophageal echocardiogram during follow-up. At hospital discharge, 27% of patients (274 total were suitable for OAC) were using OAC (16% vitamin K antagonists [VKAs]; 11% NOACs), 60% were using dual-antiplatelet treatment (DAPT), 7% were using SAPT, and 6% were using no antithrombotic or anticoagulation at all due to a very high bleeding risk (746 total were unsuitable for OAC). At the final follow-up of 2 years, 8% of active patients were still on OAC, 7% were on DAPT, and 71% were on SAPT, while 14% were not using any anticoagulant.
In order to assess LAAO true-device efficacy regarding stroke prevention, we identified 766 patients who switched after 3-6 months and were on SAPT (n = 639) or no therapy (n = 127) for ≥12 months until study completion or with events while on SAPT or no therapy (the SAPT/no-therapy subgroup) (Figure 1). Because of the limited number of patients on no therapy for ≥12 months and similar event rates to patients on SAPT, we analyzed events for both patient groups together. Additionally, we separately describe the results of each subgroup in order to show equal event rates between the SAPT and no-therapy groups. Furthermore, we compared the event rates of the SAPT/no-therapy subgroup with the EWOLUTION patient cohort and with patients on long-term OAC.
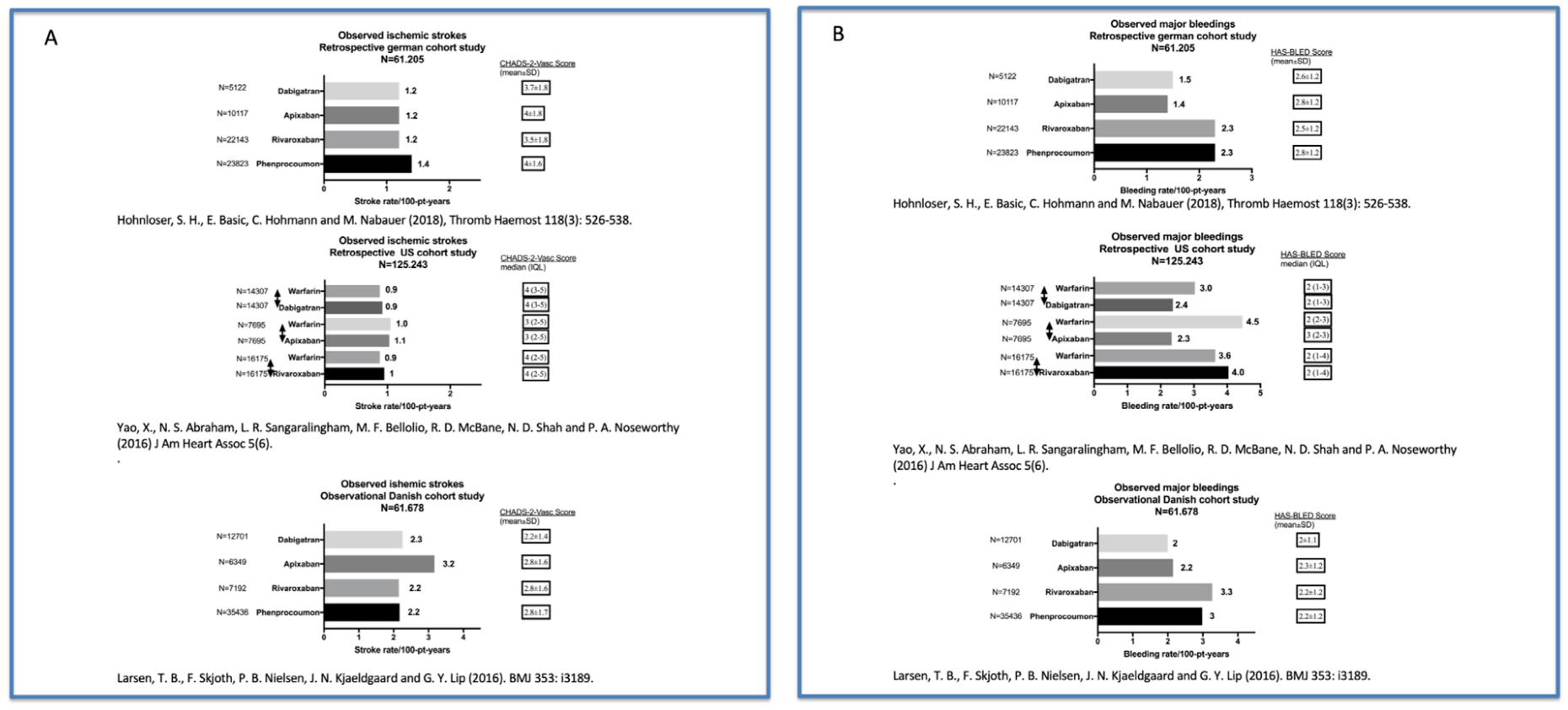
Statistical analysis. Continuous variables are summarized using mean ± standard deviation or median (range). Categorical variables are summarized using counts and percentages. Rates of stroke/bleeding events are calculated as the number of events per 100 patient years (PY). The individual patient annual risk for stroke and bleeding was recorded based on each subject’s CHA2DS2-VASc and HAS-BLED scores. Annual risks of stroke and bleeding were extrapolated from published risk score literature in similar cohorts of patients in order to determine the relative risk reduction (RRR). For stroke, this was compared with patients not using any form of anticoagulation matched for the CHA2DS2-VASc score,12 while for bleeding this was compared with patients using VKAs matched for the HAS-BLED score.13 Ischemic strokes and bleeding events were compared with patients on long-term OAC in 3 large cohort registries: (1) a retrospective cohort study using a German claims database was conducted to assess efficacy and safety during therapy with NOACs and phenprocoumon in 61,205 AF patients;14 (2) a nationwide Danish cohort study compared therapy with NOACs and warfarin in 61,678 patients with AF;15 and (3) a retrospective cohort study from the United States insurance database that included 125,243 patients with nonvalvular AF who were treated with apixaban, dabigatran, rivaroxaban, or warfarin.16 Clinical event rates per 100 PY were compared numerically between the groups without propensity-score matching, but annual risk scores for stroke and bleeding (CHA2DS2-VASc and HAS-BLED) were additionally described for each group (Supplemental Figure S1).
Results
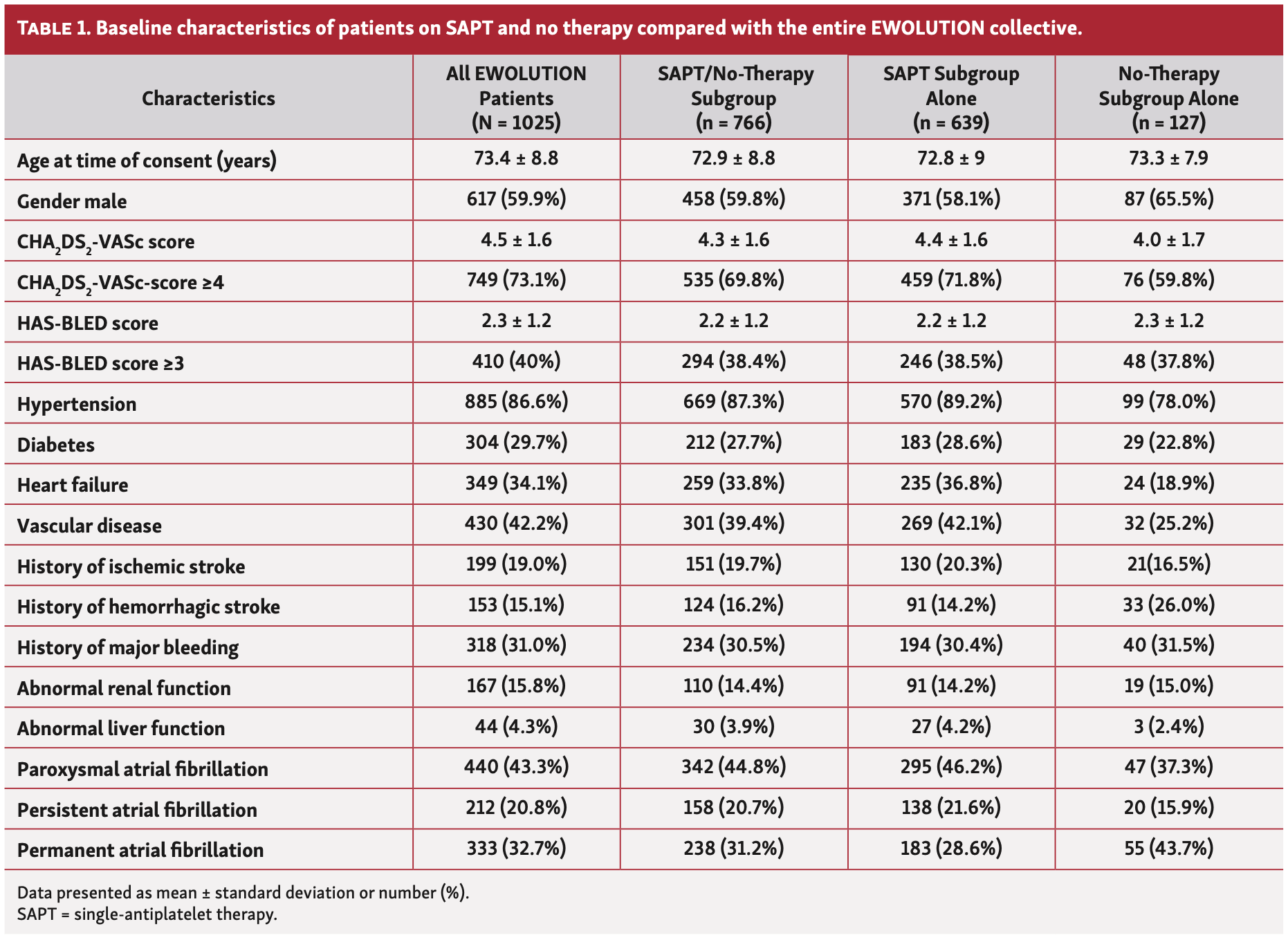
Patients on SAPT/no therapy. In order to assess LAAO efficacy, we analyzed 2-year outcomes of the 766 patients who switched to SAPT or no therapy for at least 1 year. Baseline demographics and risk factors of this patient collective compared with the entire EWOLUTION cohort are summarized in Table 1.
Mean age of the SAPT/no-therapy collective (n = 766) was 72.9 ± 8.8 years, 40.2% were female, and 78.8% had a contraindication to long-term OAC. A high stroke risk was present in 69.8%, with mean CHA2DS2-VASC score ≥4. At hospital discharge, the postimplant medications of this subgroup were 11% NOAC, 16% VKA, 58% DAPT, 8% SAPT, and 7% no anticoagulation. After 3 to 6 months, patients were switched to SAPT (n = 639) or no therapy (n = 127) and were followed for at least 1 year and up to 2 years; mean time on SAPT/no therapy was 536.56 ± 177.59 days.
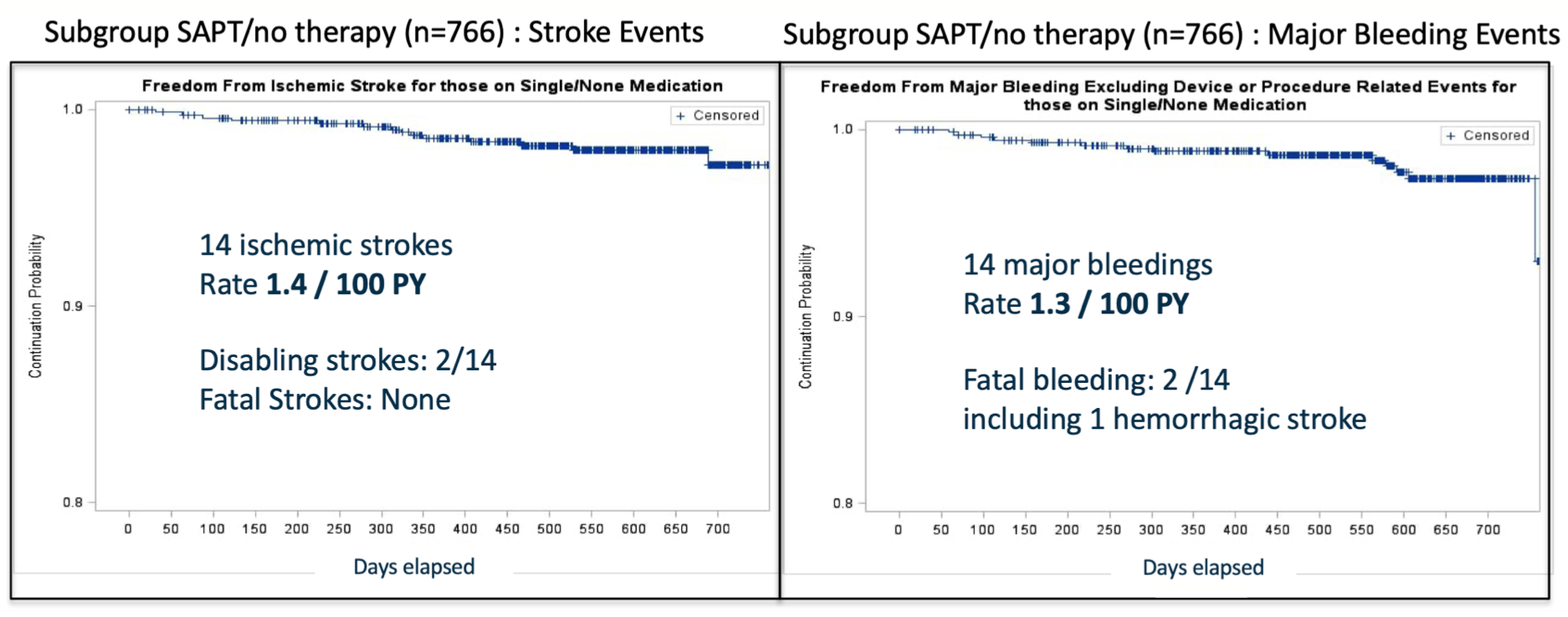
Kaplan-Meier curves of the SAPT/no-therapy subgroup for ischemic and bleeding events are depicted in Figure 2. The ischemic event rate in this cohort was low despite a CHA2DS2-VASC score of 4.3 ± 1.6. Patients switched to SAPT/no therapy showed an ischemic stroke rate of 1.4 strokes/100 PY (n = 14 strokes) at 2 years, with 2 disabling strokes but no fatal strokes. The expected rate for this cohort would have been 7 strokes/100 PY (80% RRR) (Figure 3A). As expected on SAPT/no therapy, major non-procedural bleeding rates were low despite a HAS-BLED score of 2.2 ± 1.2. The bleeding rate was 1.3 bleeds/100 PY (n = 14 major nonprocedural bleeds) at 2 years with an expected bleeding rate of 4.9 bleeds/100 PY (73% RRR) (Figure 3B) for this collective. Two observed bleedings were fatal.
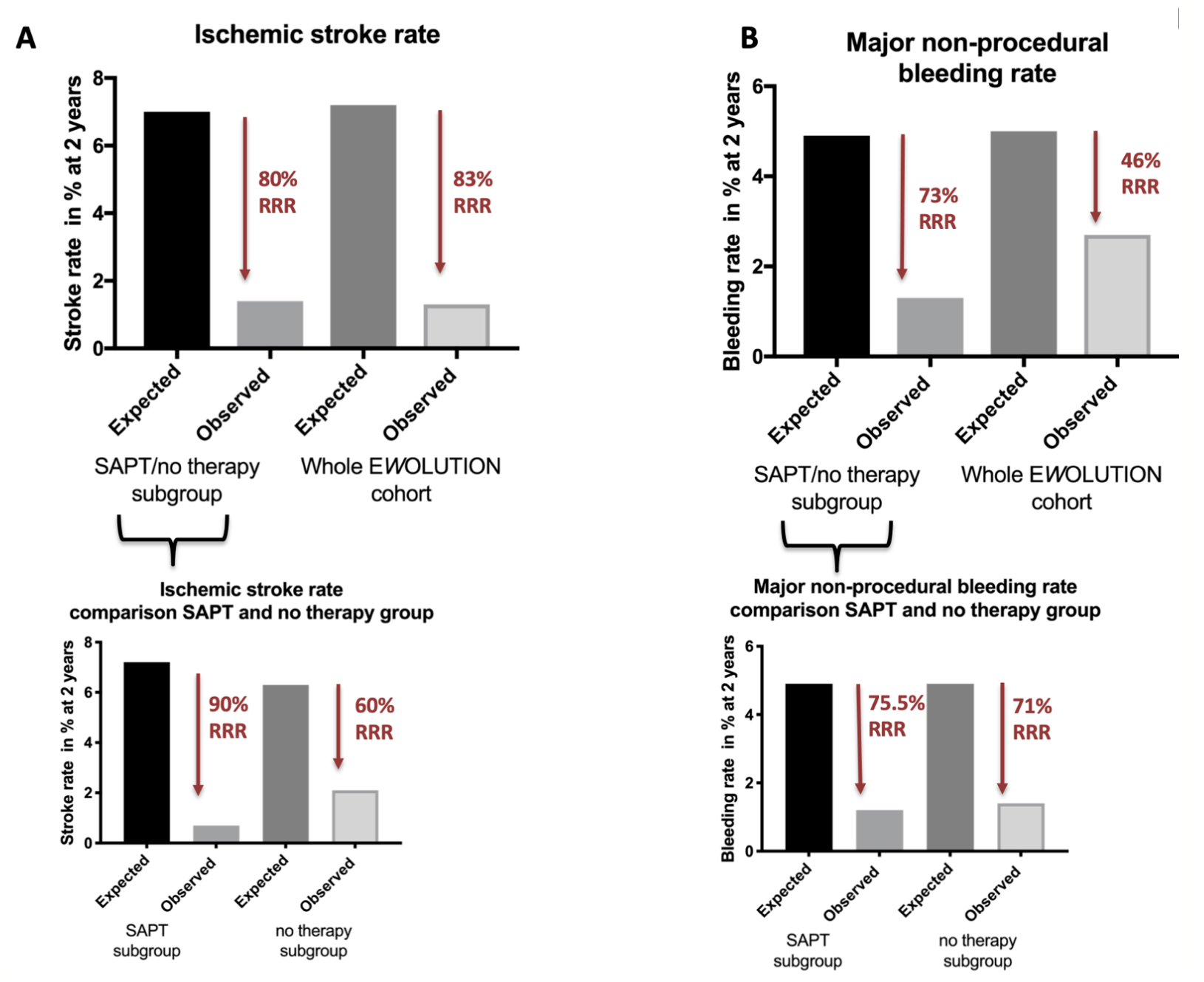
Furthermore, we separately analyzed the outcomes for patients on SAPT (n = 639) or no therapy (n = 127) to detect a possible difference in outcome after the switch to no therapy compared with patients on SAPT. Baseline demographics of each collective are summarized in Table 1. The rates of stroke (2.1 strokes/100 PY; n = 3) and bleeding (1.4 bleeds/100 PY; n = 2) of the no-therapy subgroup were similar to patients on SAPT (0.7 strokes/100 PY; n = 11 [P=.70] and 1.2 bleeds/PY; n = 12 [P=.90]). Both rates were comparable to the complete EWOLUTION collective and the other subgroups (Table 2).
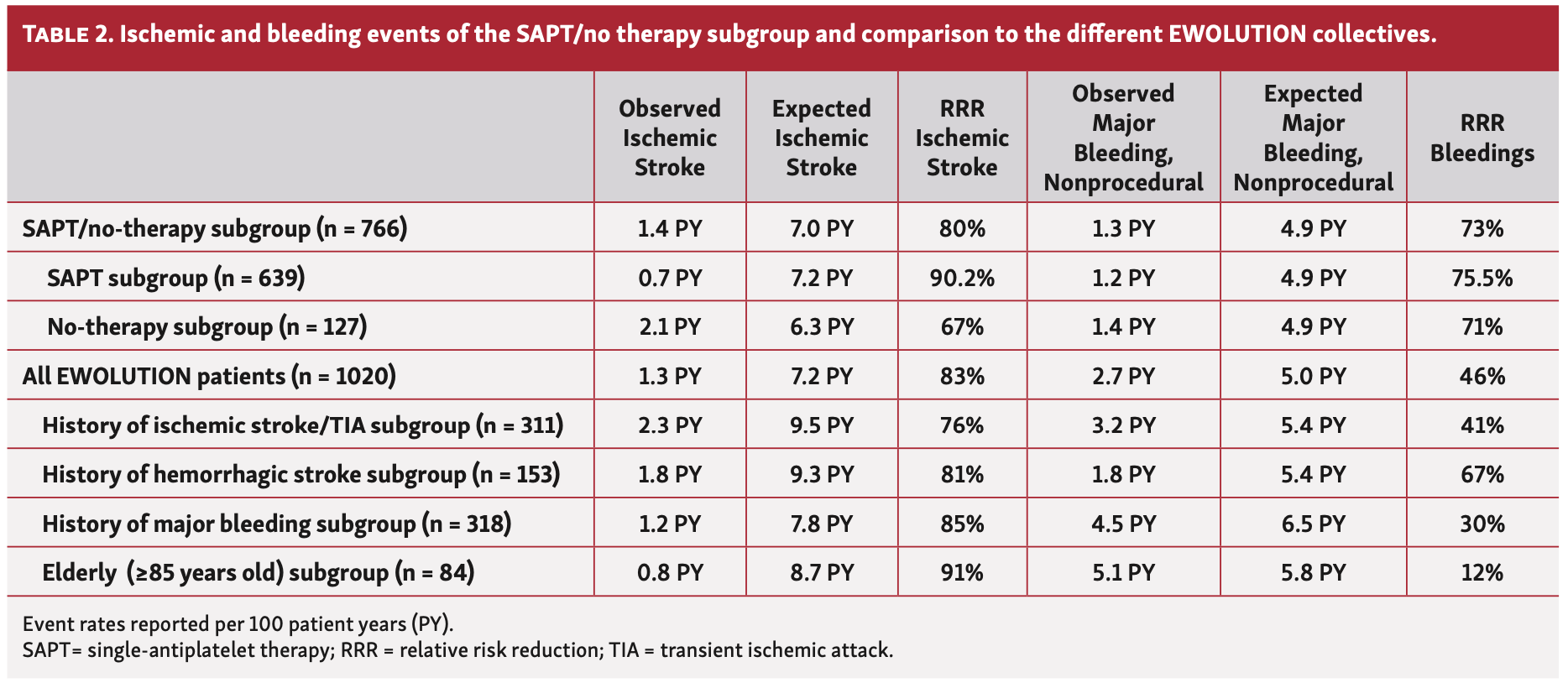
Comparison of outcome with the entire EWOLUTION cohort. We compared outcomes between patients on SAPT or no therapy to the complete EWOLUTION collective as well as to specific subgroups (Table 2). The ischemic stroke rate in the SAPT/no-therapy subgroup at 2 years was in line with the complete EWOLUTION collective and similar to the high-risk patient subpopulations previously analyzed (Figure 4A); stroke rate was generally low (0.8-2.3 strokes/100 PY). A thrombus on the device (DRT) was detected by transesophageal echocardiography in a total of 34 patients (4.1%) in the whole EWOLUTION cohort; DRT mainly occurred at <92 days; 31 out of 34 DRT patients were diagnosed within this time frame. The DRT rate in the SAPT/no-therapy subgroup was low (n = 3; 0.4%) with the SAPT/no-therapy regimen starting after 92 days. Two DRTs were detected in the SAPT subgroup and 1 in the no-therapy group. However, if we consider those patients with postimplant SAPT or no-therapy regimen, the DRT rate did not differ from other medication choices (OAC/DAPT), as described before.6
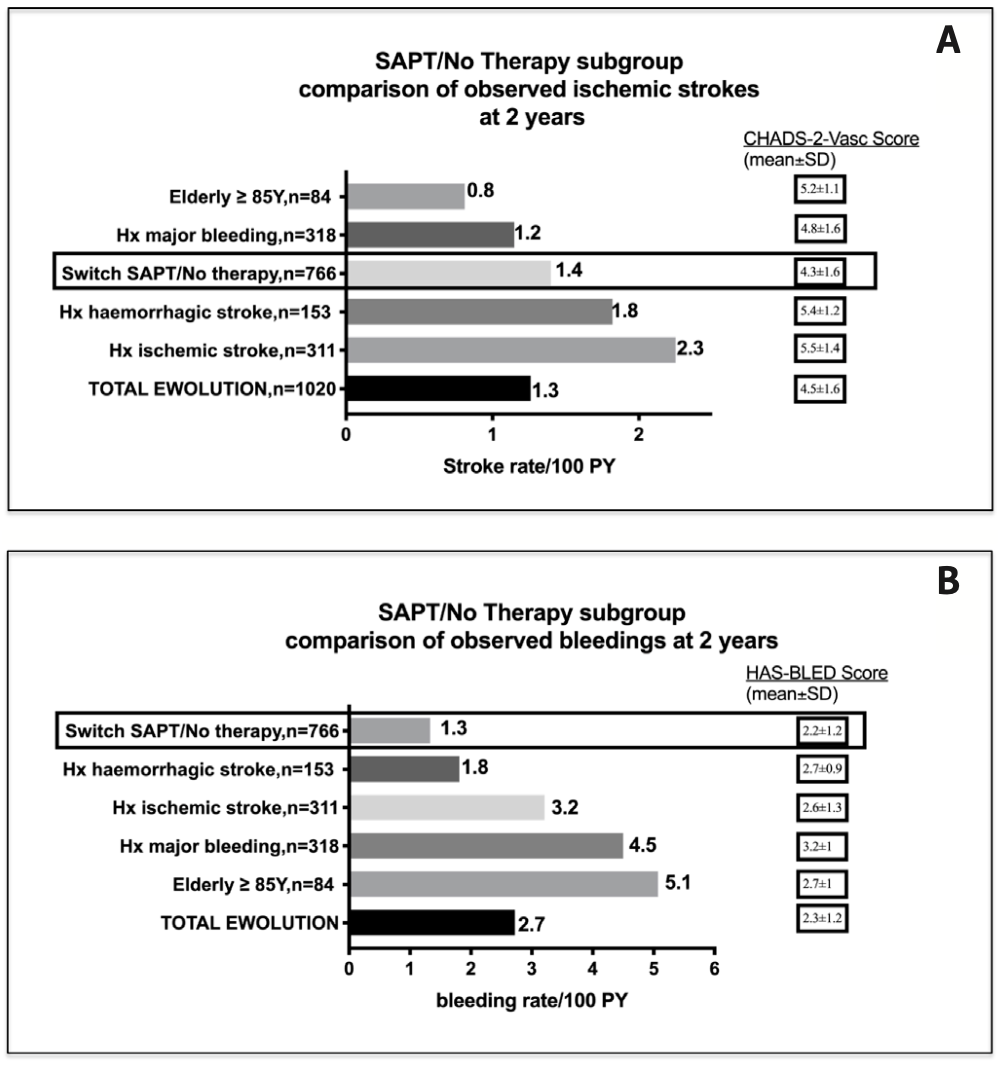
As expected, the lowest bleeding rate at 2 years was observed in patients switched to SAPT/no therapy after 3-6 months, when comparing the different EWOLUTION collectives (Figure 4B). However, overall bleeding rate in EWOLUTION was low and only between 1-5 bleeds/100 PY.
Discussion
EWOLUTION is the largest prospective registry providing data on LAAO employing the Watchman device in a real-world, high-risk population to date.6 Herein, we provide a detailed analysis of LAAO efficacy in a subgroup of patients on SAPT or no therapy for ≥1 year. The observed rates of ischemic stroke and major bleed suggest the efficacy and further safety of LAAO therapy after permanent discontinuation of the intensified postimplantation antiplatelet or transient anticoagulation regime 3-6 months after LAAO.
Postimplantation regime. Postimplantation medication in EWOLUTION was at the discretion of each investigator. Instructions for use of the Watchman device were recently updated for patient’s ineligible for (N)OAC outside the United States.8,17 They now specifically allow both DAPT as well as a 3-month course of NOAC depending on patient preference. Sixty percent of patients were on DAPT directly after the procedure in the EWOLUTION registry. After 3 to 6 months, 766 of all EWOLUTION patients (66%) were switched to SAPT (n = 639) or no therapy (n = 127), while at the study’s conclusion after 2 years, 84% of the active patients were on SAPT or no therapy. The main reasons for the high number of patients on long-term SAPT were comorbidities such as coronary artery disease that required long-term SAPT.
Device-related thrombus. A DRT was observed in 34 patients (4.1%) of the whole EWOLUTION cohort, but was not correlated to an increased ischemic event rate in this registry.6 Furthermore, the DRT rate in the SAPT/no-therapy subgroup was low (n = 3; 0.4%) with 2 DRTs in the SAPT and 1 DRT in the no-therapy group, suggesting safety after switching the treatment regimen post implant at 92 days due to device endothelialization. The pathogenesis of DRT is still likely to be multifactorial and so far, no consistent predictor has been identified. One important step to reduce LAAO-conferred risks and minimize DRT formation is to identify the optimal drug regimen post procedure and in the long term. Additionally, implanting a new-generation device with specific characteristics such as the Watchman FLX device, which has fewer exposed knobs on the atrial side, may further reduce the DRT rate.18
Stroke rate. The subgroup analysis of 766 patients who were on SAPT or no therapy ≥12 months following LAAO showed similar low ischemic rates and even lower bleeding rates with further risk reduction compared with the complete EWOLUTION cohort. We observed an RRR for ischemic strokes of 80% and no fatal strokes up to 2 years. Furthermore, we analyzed the stroke event rate separately for the no-therapy group and the SAPT group, showing a comparable low risk. These data support LAAO therapy as an effective and safe alternative for the prevention of thromboembolic events in patients with nonvalvular AF deemed unsuitable for long-term OAC. To confirm the noninferiority of LAAO compared with NOAC therapy, a randomized trial is necessary; PRAGUE-17 is the first such trial employing a combined endpoint.5 In 2021, randomized trials were ongoing with a direct comparison of LAAO to NOAC therapy in an all-comers population, aiming to show equal or even superior stroke protection (ie, OPTION [ClinicalTrials.gov identifier NCT03795298]; CHAMPION-AF [ClinicalTrials.gov identifier NCT0439454]; CLEARANCE [ClinicalTrials.gov identifier NCT04298723]; and CATALYST [ClinicalTrials.gov identifier NCT04226547]). CHAMPION-AF will randomize >2000 patients with a CHA2DS2-VASc score ≥2 to NOAC vs LAAO with the Watchman FLX device. The CATALYST trial will randomize 2650 participants with a CHA2DS2-VASc score ≥3 to NOAC therapy vs the Amulet LAAO (Abbott Structural Heart). Both trials have stroke, systemic embolism, and cardiovascular mortality as well as bleeding events as primary endpoints, with a follow-up of 2 years.
Bleeding rate. As expected, bleeding events at 2 years in EWOLUTION were lower (1.3 bleeds/100 PY) in patients switched to SAPT/no therapy compared with the complete EWOLUTION cohort (2.7 bleeds/100 PY) despite 71% of the patients being on long-term aspirin therapy. The overall EWOLUTION bleeding rate was mainly driven by a few high-risk cohorts (elderly patients ≥85 years old and patients with abnormal renal function). The similar low bleeding rate in the no-therapy subgroup (1.4 bleeds/100 PY) compared with patients on SAPT (1.2 bleeds/100 PY) supports this notion. This observation suggests a persistently increased bleeding risk in this patient cohort independent of a tailored postprocedural drug therapy; it is possible that short-term SAPT would be the best option here. However, the overall bleeding rate in EWOLUTION was significantly reduced compared with the expected rate in these patients. The favorable effect of LAAO on the bleeding rate in EWOLUTION of the SAPT/no-therapy cohort was also in line with patients in the 2 randomized controlled United States trials on LAAO, where the bleeding rate was 1.0 bleeds/100 PY despite an even higher HAS-BLED score in EWOLUTION.19
LAAO efficacy compared with NOACs. To date, LAAO is an alternative for patients unsuitable for long-term OAC treatment.20 However, the safety and efficacy of NOAC therapy depends on several factors, ie, the risk of nonadherence among AF patients is high (47.3%), with patients on warfarin and those with several comorbidities (including prior bleeding) having a higher risk for nonadherence.21 Rates of premature NOAC discontinuation are high and range from 2.3%-37.0%.22 Furthermore, real-world evidence suggests that patients are not being dosed appropriately, leading to a higher risk of stroke and thromboembolism.23 Data from the ongoing, observational European GARFIELD registry show that the use of NOAC decreased with increased HAS-BLED score; furthermore, anticoagulant therapy was not prescribed in 36.9% of patients with CHA2DS2-VASc score ≥2.24 Of note, the ischemic stroke rate (1.4 strokes/100 PY) of the EWOLUTION SAPT/no-therapy subgroup was in line with the low event rates described in the German, Danish, and United States NOAC registries (0.9-3.2 ischemic strokes/100 PY), although mean CHA2DS2-VASc score was higher in the EWOLUTION cohort.14-16 Observed nonprocedural major bleeding events in the SAPT/no-therapy subgroup (1.3 bleeds/100 PY) were numerically lower compared with event rates of patients on long-term NOAC (1.4-4.5 bleeds/100 PY), with a higher HAS-BLED score in EWOLUTION. An overview of the event rates of patients on long-term OAC in the 3 large, retrospective (N)OAC cohort studies is depicted in Supplemental Figure S1. Yet, this comparison of the EWOLUTION results with events of AF patients on long-term OAC is without statistical matching technique and interpretation should be done with caution. The outcome data with low ischemic and bleeding event rates of the SAPT/no-therapy cohort following Watchman implantation in the EWOLUTION registry now add further scientific efficacy information to this European perspective on LAAO therapy.
Study limitations. Despite the fact that EWOLUTION is a prospective registry without a randomized control group, the broad entry criteria and different postprocedural treatment regimens allow the analysis of a subpopulation like the SAPT/no-therapy cohort. We analyzed the event rates of patients on SAPT and no therapy (after switching the intensified post-LAAO regimen) combined in 1 group, as patients were mainly switched to SAPT and only a few to the no-therapy regimen. To detect a possible difference between the no-therapy group compared with patients on SAPT, we additionally reported on the subgroups separately, showing a similar baseline profile and outcome. However, results of the no-therapy group should be interpreted with caution, as numbers were low. As this study only included patients treated with the Watchman device, results will not necessarily apply to other devices.
Conclusion
The EWOLUTION registry provides data on LAA closure employing the Watchman device in a real-world population in Europe. Outcome data of patients on SAPT or no therapy following Watchman implantation in the EWOLUTION registry are consistent with the complete EWOLUTION population and similar to event rates in recent OAC registries. This suggests long-term efficacy for LAAO as an alternative for patients who are ineligible for OAC.
Affiliations and Disclosures
From 1Interventional Cardiology, Cardiologicum Hamburg, Hamburg, Germany; 2University Heart Center Lübeck, Medical Clinic II (Cardiology, Angiology, Intensive Care Medicine) University Schleswig-Holstein (UKSH); 4Vivantes Klinikum Am Urban, Berlin, Germany; 5Vivantes Klinikum im Friedrichshain, Berlin, Germany; 6E. Meshalkin National medical research center of the Ministry of Health of the Russian Federation, Novosibirsk, Russian Federation; 7Elisabeth Krankenhaus, Essen, Germany; 8Cardioangiologisches Centrum Bethanien, Frankfurt, Germany; 9Universitätsmedizin Mainz und DZHK Standort Rhein-Main, Mainz, Germany; 10Asklepios Klinik Altona, Hamburg, Germany; 11Regional State Hospital, Krasnoyarsk, Russia; 12John Radcliffe Infirmary Oxford, Oxford, United Kingdom; 13Boston Scientific Corporation, Diegem, Belgium; 14ASKLEPIOS proresearch, Hamburg, Germany; and 15St Antonius Hospital, Nieuwegein, the Netherlands.
Funding: EWOLUTION was funded by Boston Scientific; the authors have no potential conflict related to this analysis.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Bergmann reports personal fees from Boston Scientific (BSC), Abbott, Biosense Webster, and Johnson & Johnson, outside the submitted work. Dr Ince is a proctor for Watchman and Lotus (BSC) and has received personal fees from BSC, outside the submitted work. Dr Romanov is a speaker for Medtronic, BSC, and Biosense Webster. Dr Schmidt reports personal fees from BSC and Abbott, outside the submitted work. Dr Betts reports personal fees from BSC, outside the submitted work. Elisa Vireca is an employee and shareholder at BSC. Dr Boersma reports personal fees from BSC and Medtronic, outside the submitted work. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript accepted September 2, 2021.
Address for correspondence: Martin W. Bergmann, MD, PhD, FESC, Interventional Cardiology, Cardiologicum Hamburg, Schloßgarten 3-7, 22401 Hamburg, Germany. Email: docbergmann@mac.com
References
1. Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955-962. doi:10.1016/S0140-6736(13)62343-0
2. Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur J Cardiothorac Surg. 2016;50(5):e1-e88. doi:10.1093/ejcts/ezw313
3. January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm. 2019;16(8):e66-e93. Epub Jan 28 2019. doi:10.1016/j.hrthm.2019.01.024
4. Reddy VY, Doshi SK, Kar S, et al. 5-Year outcomes after left atrial appendage closure: from the PREVAIL and PROTECT AF trials. J Am Coll Cardiol. 017;70(24):2964-2975. doi:10.1016/j.jacc.2017.10.021
5. Osmancik P, Herman D, Neuzil P, et al. Left atrial appendage closure versus direct oral anticoagulants in high-risk patients with atrial fibrillation. J Am Coll Cardiol. 2020;75(25):3122-3135. doi:10.1016/j.jacc.2020.04.067
6. Boersma LV, Ince H, Kische S, et al. Evaluating real-world clinical outcomes in atrial fibrillation patients receiving the Watchman left atrial appendage closure technology. Circ Arrhythm Electrophysiol. 2019;12(4):e006841. doi:10.1161/CIRCEP.118.006841
7. Landmesser U, Tondo C, Camm J, et al. Left atrial appendage occlusion with the Amplatzer Amulet device: one-year follow-up from the prospective global Amulet observational registry. EuroIntervention. 2018;14(5):e590-e597. doi:10.4244/EIJ-D-18-00344
8. Bergmann MW, Ince H, Kische S, et al. Real-world safety and efficacy of Watchman LAA closure at one year in patients on dual antiplatelet therapy: results of the DAPT subgroup from the EWOLUTION all-comers study. EuroIntervention. 2018;13(17):2003-2011. doi:10.4244/EIJ-D-17-00672
9. Cruz-Gonzalez I, Ince H, Kische S, et al. Left atrial appendage occlusion in patients older than 85 years. Safety and efficacy in the EWOLUTION registry. Rev Esp Cardiol (Engl Ed). 2020;73(1):21-27. doi:10.1016/j.rec.2019.02.008
10. Boersma LV, Schmidt B, Betts TR, et al. EWOLUTION: design of a registry to evaluate real-world clinical outcomes in patients with AF and high stroke risk-treated with the Watchman left atrial appendage closure technology. Catheter Cardiovasc Interv. 2016;88(3):460-465. doi:10.1002/ccd.26358
11. Tzikas A, Holmes DR Jr, Gafoor S, et al. Percutaneous left atrial appendage occlusion: the Munich consensus document on definitions, endpoints and data collection requirements for clinical studies. EuroIntervention. 2016;12(1):103-111. doi:10.4244/EIJV12I1A18
12. Friberg L, Rosenqvist M, Lip GY. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182 678 patients with atrial fibrillation: the Swedish atrial fibrillation cohort study. Eur Heart J. 2012;33(12):1500-1510. doi:10.1093/eurheartj/ehr488
13. Lip GY, Frison L, Halperin JL, Lane DA. Comparative validation of a novel risk score for predicting bleeding risk in anticoagulated patients with atrial fibrillation: the HAS-BLED (hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile INR, elderly, drugs/alcohol concomitantly) score. J Am Coll Cardiol. 2011;57(2):173-180. doi:10.1016/j.jacc.2010.09.024
14. Hohnloser SH, Basic E, Hohmann C, Nabauer M. Effectiveness and safety of non-vitamin K oral anticoagulants in comparison to phenprocoumon: data from 61,000 patients with atrial fibrillation. Thromb Haemost. 2018;118(3):526-538. doi:10.1160/TH17-10-0733
15. Larsen TB, Skjoth F, Nielsen PB, Kjaeldgaard JN, Lip GY. Comparative effectiveness and safety of non-vitamin K antagonist oral anticoagulants and warfarin in patients with atrial fibrillation: propensity weighted nationwide cohort study. BMJ. 2016;353:i3189. doi:10.1136/bmj.i3189
16. Yao X, Abraham NS, Sangaralingham LR, et al. Effectiveness and safety of dabigatran, rivaroxaban, and apixaban versus warfarin in nonvalvular atrial fibrillation. J Am Heart Assoc. 2016;5(6):e003725. doi:10.1161/JAHA.116.003725
17. Bergmann MW, Betts TR, Sievert H, et al. Safety and efficacy of early anticoagulation drug regimens after Watchman left atrial appendage closure: three-month data from the EWOLUTION prospective, multicentre, monitored international Watchman LAA closure registry. EuroIntervention. 2017;13(7):877-884. doi:10.4244/EIJ-D-17-00042
18. Kar S, Doshi SK, Sadhu A, et al. Primary outcome evaluation of a next-generation left atrial appendage closure device: results from the PINNACLE FLX trial. Circulation. 2021;143(18):1754-1762. doi:10.1161/CIRCULATIONAHA.120.050117
19. Price MJ, Reddy VY, Valderrabano M, et al. Bleeding outcomes after left atrial appendage closure compared with long-term warfarin: a pooled, patient-level analysis of the Watchman randomized trial experience. JACC Cardiovasc Interv. 2015;8(15):1925-1932. doi:10.1016/j.jcin.2015.08.035
20. Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace. 2016;18(11):1609-1678. doi:10.1093/europace/euw295
21. Kachroo S, Hamilton M, Liu X, et al. Oral anticoagulant discontinuation in patients with nonvalvular atrial fibrillation. Am J Manag Care. 2016;22(1):e1-e8.
22. Rodriguez RA, Carrier M, Wells PS. Non-adherence to new oral anticoagulants: a reason for concern during long-term anticoagulation? J Thromb Haemost. 2013;11(2):390-394. doi:10.1111/jth.12086
23. Turpie AGG, Purdham D, Ciaccia A. Nonvitamin K antagonist oral anticoagulant use in patients with renal impairment. Ther Adv Cardiovasc Dis. 2017;11(9):243-256. doi:10.1177/1753944717714921
24. Bassand JP, Accetta G, Camm AJ, et al. Two-year outcomes of patients with newly diagnosed atrial fibrillation: results from GARFIELD-AF. Eur Heart J. 2016;37(38):2882-2889. doi:10.1093/eurheartj/ehw233
Related Articles
- Safety, Efficacy, and Cost-Effectiveness of Same-Day Discharge for Left Atrial Appendage Occlusion
- Left Atrial Appendage Occlusion as Adjunctive Therapy to Anticoagulation for Stroke Recurrence
- Preserved Left Atrial Function Following Left Atrial Appendage Closure for Stroke Prevention
- Combined Percutaneous Treatment of Severe Triscuspid Regurgitation and Left Atrial Appendage Closure
- Percutaneous Management of Left Atrial Appendage Perforation: Keep Calm and Think Fast
- A New Strategy for Transcatheter Left Atrial Appendage Closure With Cerebral Embolic Protection in Patient With Left Auricular Thrombosis and Total Contraindication to Long-Term Anticoagulation
- Left Atrial Appendage Occlusion Using Cardiac CT Angiography and Intracardiac Echocardiography: A Prospective, Single-Center Study
- Left Atrial Appendage Occlusion With the LAmbre Device: First-in-Human in the United States














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}