


Various Techniques for Transcatheter Retrieval of Atrial Septal Defect or Patent Foramen Ovale Closure Devices: A Systematic Review
Abstract
Atrial septal abnormalities are common congenital lesions that remain asymptomatic in many patients until adulthood. Adults with atrial septal defects (ASD) most commonly have ostium secundum ASD. Transcatheter closure has become increasingly popular in recent years as a successful alternative method to surgery for treating ASD and patent foramen ovale (PFO). The overall rate of ASD transcatheter closure device embolization has been reported to be less than 1%; however, retrieving the device via surgery or by trans-catheter route can be necessary. The current manuscript describes a systematic review of the techniques used to retrieve ASD closure devices, as well as their success rates, complications, and limitations. A comprehensive search was performed covering various databases including PubMed, MEDLINE, SCOPUS, Google Scholar, and Cochrane Library from inception until April 2022 for English-published case reports, case series, and experimental studies investigating the indications, safety, and limitations of ASD closure and ASD device retrieval by trans-catheter approaches. Finally, 20 studies were included in our review. Our findings showed that most of the studies used a single snare technique; of these, all but one reported 100% success. Double tool retrieval methods (snare plus snare, snare plus bioptome, or snare plus forceps) and the gooseneck snare technique yielded 100% success. One study that used the lasso technique reported unsuccessful retrieval and the need for surgical intervention. More recently, the novel "coronary wire trap technique" was introduced, which provides a simpler method for embolized device removal by trapping the device for retrieval using coronary wire.
Introduction
Atrial septal defect (ASD) closure device embolization is a rare but potentially fatal complication caused by various reasons such as device malposition, improper sizing defects along with an undersized occluder, and inadequate or floppy rim, which can occur even with an experienced operator.1 Though it is the most frequent complication requiring surgical intervention during or after percutaneous ASD closure, fortunately, the overall embolization rate requiring retrieval of the device via surgery or by transcatheter route (TC) has been reported to be less than 1%,2,3 and most embolized devices can be removed percutaneously. Usually, after retrieval of the embolized device, a second device with careful assessment can successfully be implanted.4,5 Some reports suggested the superiority of the surgical method for device retrieval, but many prioritize the various available TC techniques. In a large survey, the overall embolization rate was reported to be 0.55%. Surgical retrieval occurred in 28.5% of the cases, while the majority of retrievals (71.4%) were successfully performed via the TC approach.6 In another report on the MAUDE database, surgical and TC-based retrieval occurred in 77.2% and 16.7%, respectively.7
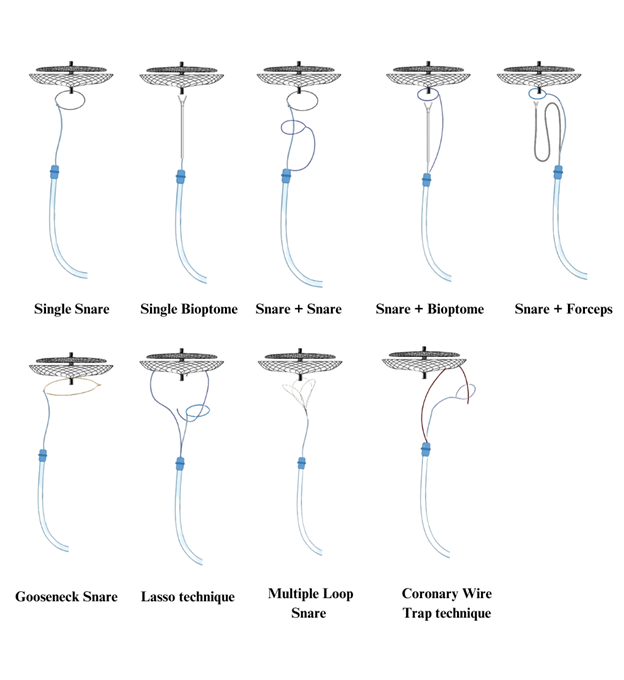
There are 3 major steps to follow when trying to retrieve a device after device malposition or embolization: (1) select the least invasive or surgical (if required) approach; (2) plan a stepwise algorithmic approach by integrating surgical or TC options according to patients' characteristics, defect-related parameters, and operator's experience; and (3) follow a safe approach by using multimodal imaging tools such as three-dimensional echocardiography and single-plane fluoroscopy.8 The TC and surgical options are available for retrieving embolized devices. However, the much less invasive TC approach is gaining popularity;9,10 in recent years, TC has been commonly utilized to treat secundum ASDs and patent foramen ovales (PFOs) as an alternative and successful method to surgery, as it is associated with a quicker recovery and leaves no scarring.11-14 In this review, we summarize and describe various catheter-based techniques for ASD or PFO-embolized device retrieval in detail (Figure 1).
Literature Search and Selection
A comprehensive systematic search of PubMed, MEDLINE, SCOPUS, Google Scholar, and Cochrane Library databases was performed from inception to April 2022. The search was performed by 2 independent researchers and used related keywords and the following MeSH terms: “atrial septal defect," “transcatheter closure,” “patent foramen ovale,” “device embolizations,” and “complications”. Disagreements in the assessment of data were resolved by discussion reaching consensus in all cases.
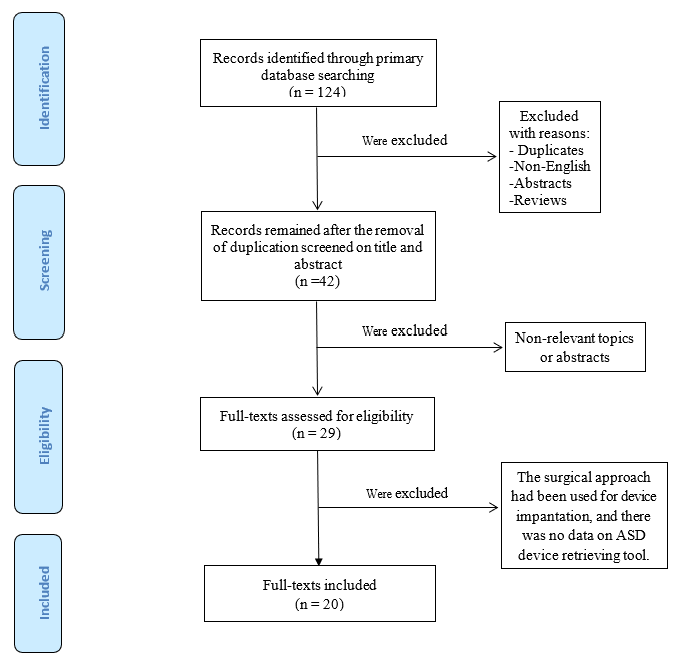
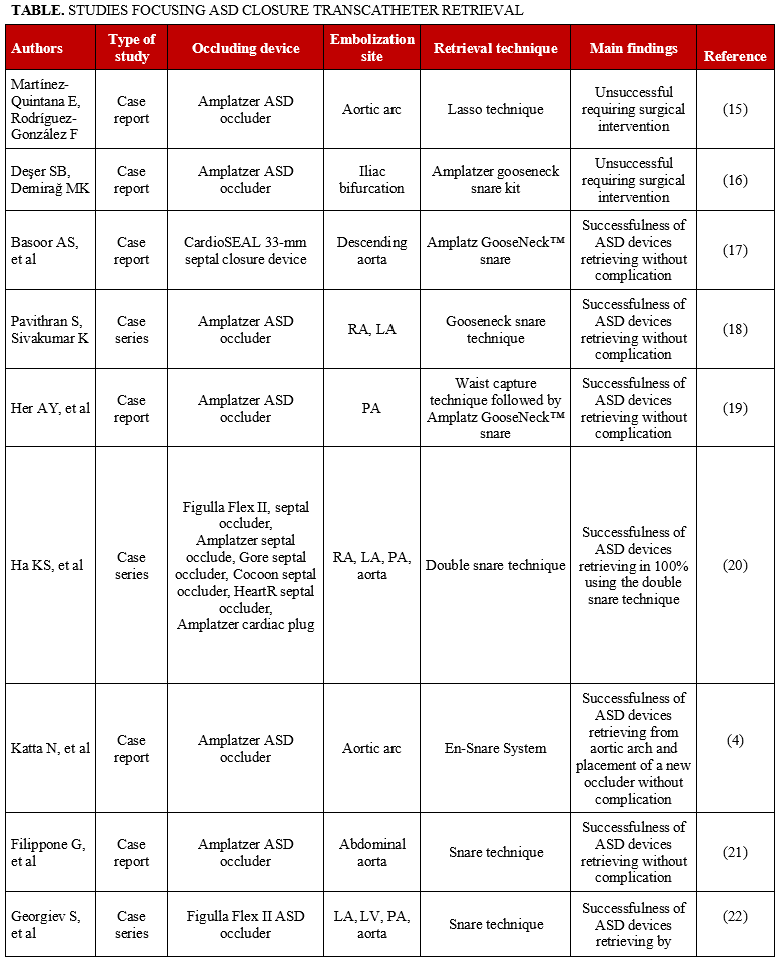
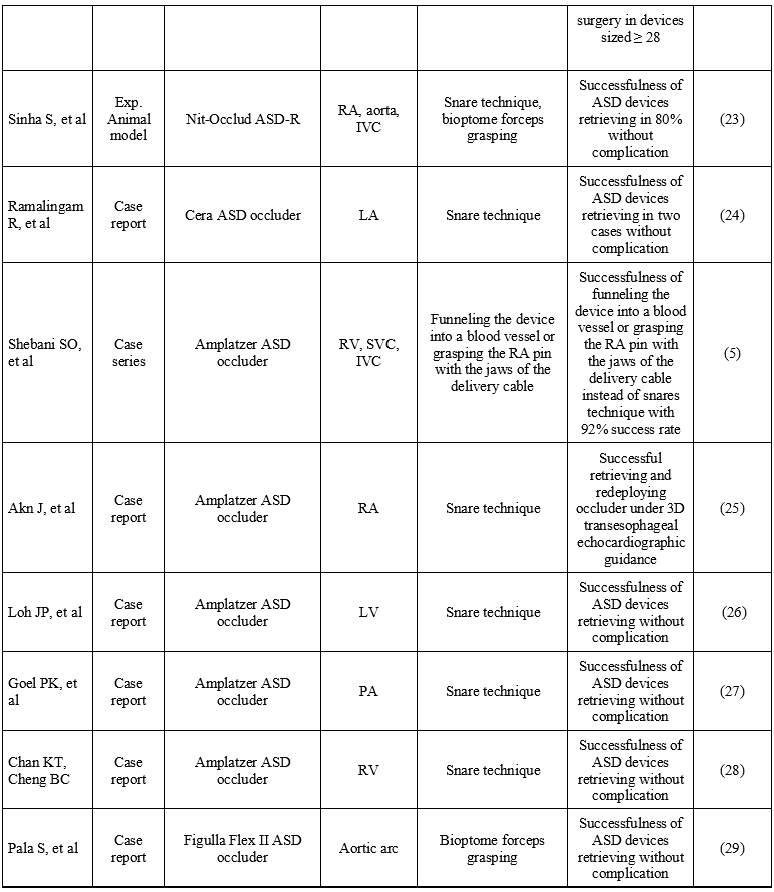
All articles were entered in EndNote and then screened for duplications. After removing the duplicates, the titles and abstracts of the remaining articles were screened, and those that were not related to the topic were removed. Finally, the full text of each article was read carefully and the papers that met our inclusion criteria were included. Eligible articles were case reports, case series, and interventional studies as long as the full texts were available. Only articles in English language were selected. Figure 2 shows the flowchart of the study selection process. The initial literature search revealed a total of 124 articles, 20 of which were included in this review (Table).4,5,15-32
Single Device Retrieval Technique: Snare or Bioptome
The first snaring tools included snares that were constructed manually using a 0.014-inch coronary wire and a 5-French (F) diagnostic catheter. Single-loop snares with a small diameter can be used for retrieving embolized devices by hooking their pin, while larger snares may be more applicable for encircling the device. Generally, a simple snare is used to capture and retrieve the device.33,34 In this technique, the snare is directly introduced via a retrieval sheath that facilitates the grasping of the device. There are various sheaths in terms of type, steerability, and size, usually 8.5- to 14-F sizes. Usually, the selected retrieval sheath is 2- to 4-F sizes larger than the sheath size required for device implantation. Furthermore, the site of snaring may be different based on the device type or the presence of screw pins.35-37 Moreover, according to the type of septal occluder (nitinol-based or non-nitinol-based occluders), embolized devices during retrieval can undergo substantial deformation when pulled through the sheath (commonly for non-nitinol-based occluders). The use of "lockable" pins provides an opportunity to recover the device in a seemingly reverse way from its deployment. However, holding a fixed tug after hitting the pins can often be challenging. If complete recapture is achieved, the device will be pulled through the sheath, however, in cases of recapture failure, other TC retrieval techniques can be tried.37 After advancing the snare, the pin of the embolized device will be snared and then pulled into the sheath. The major limitation of this technique is to be able to capture the pin. Multiple imaging tools may help to achieve successful grabbing of the device pin. Instead of a snare, a bioptome can be used to grab the pin of the embolized device in a similar manner to the snare (Figure 1).
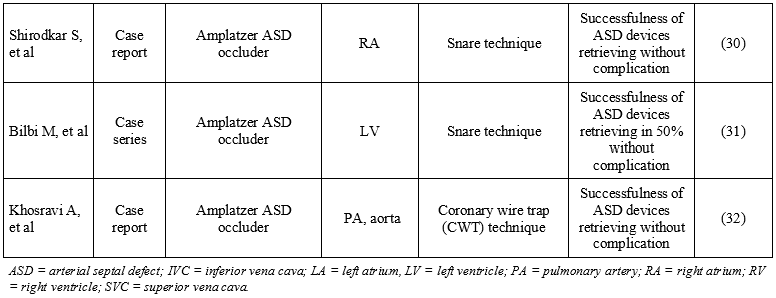
Snare techniques for device retrieval have been used in most of the included studies.21,22,24-28,30 With the exception of the Balbi et al study, which had the lowest successful retrieval rate of embolized ASD devices using snares (50%),31 all other studies had a 100% successful rate without any complication.22
Combined Device Retrieval Techniques
The use of a single tool (snare or bioptome) may not be sufficient for grasping the embolized occluder device in some cases, as it may increase the risk of re-embolization, or the sheath may be inadequate. In this regard, the simultaneous application of 2 retrieval devices (snare plus snare, snare plus bioptome, or snare plus forceps) may be more appropriate.36 Applying the double device retrieval technique has potential advantages, including the facilitation of safe device retrieval, a shortened retrieval procedure time, higher success rate, no need for retrieval sheath exchange, and reduced risk of cardiac injuries or cardiac arrhythmias.20,38 The detail of this technique is illustrated in Figure 1. After snaring the pin, a bioptome is also advanced and grabs the pin of the device for double security. Then, both retrieval devices are pulled back into the sheath with the embolized device.
A study in Taiwan reported 25 cases of successful misplaced port-catheter retrieval using a loop snare and grasping forceps as auxiliary instruments.39 In a case-series study of 14 patients undergoing ASD occlusion and 1 patient undergoing left atrial appendage closure, the success rate was 100% for embolized device retrieval without any complications.20 In another case, following the first snaring of the right atrial end screw, the second snare was inserted into the retrieval sheath following the snaring of the body of the atrial end screw. Thereafter, the 2 snare catheters were manipulated in different directions to change the orientation of the right atrial end screw for retrieval into the sheath.29 They also reported the use of combined bioptome and forceps for successful device retrieval without any complications.29
Gooseneck Snare Technique
In a case-report study, a minimally invasive and modified approach was applied successfully by Basoorer et al for ASD device removal.17 In this procedure, multipurpose biopsy forceps and an Amplatz Goose Neck snare (Medtronic) accompanied by a 16-F Cook sheath were applied to enable compressing and pulling of the migrated device within the sheath.
In another study, The Waist Capture Technique was successfully applied for device retrieval without any complication.19 In this technique, a guidewire was introduced through the right femoral vein via a sheath. The guidewire was passed into the right pulmonary artery that penetrated the mesh of the right atrial-sided disc. An Amplatz Goose Neck snare was then used to catch the tip of the guidewire. The device was pulled back into the inferior vena cava, and a neuro-guidewire was introduced through the sheath. To stabilize the device, the waist of the device was captured by a looped guidewire. Finally, the screw could be snared on the right atrial disc by an Amplatz Goose Neck snare.19
In 2015, Pavithran and Sivakumar published a case-series study that demonstrated use of the gooseneck snare technique with 100% success.18 In their novel experience following the deployment of the device in place, they passed a snare via the delivery sheath around the cable to grip the screw on the right atrial disc of the device. With the snare holding the screw end, the device was successfully released by unscrewing the cable. After confirming the device's stability, the snare was subsequently removed. In another report by Deser and Demirağ,16 the embolized ASD device migrated into the iliac bifurcation. They could not retrieve the device despite using an Amplatz Goose Neck snare kit from the right femoral artery, as it migrated into the abdominal aorta and required surgical removal. Figure 1 shows this technique in comparison to other methods.
Other Techniques
Lasso technique. In a 2017 study, Padala et al presented their successful experiences by using lasso catheters for ASD occluder retrieval for the first time.40 They applied 2 Lasso catheters and steerable sheaths for ASD occluder retrieval. In this technique, the lasso catheter enters the embolized device and then the tip of the lasso catheter is snared to trap the embolized device. Then, the lasso catheter and snare are retrieved with an embolized device altogether. Figure 1 illustrates the details of this technique.
However, in another case, the lasso technique was unsuccessful.15 After an Amplatzer Septal Occluder (Abbott) was successfully deployed using proper placement, echocardiography performed at 6-month follow-up revealed persistent ASD with an embolized device found in the aorta. For device retrieval, they used a lasso catheter to grab the screw of the right atrial disc. However, they were unsuccessful, and the patient required surgical removal.
En-Snare technique. In 2016, Katta et al were successful in ASD device retrieval from the aortic arch with successful placement of a new occluder device without complication. In their case, they used an En-Snare System (Merit Medical) through a Hockey Stick II guiding catheter (Merit Medical). The metallic tip was snared on the right atrial disc of the ASD device.4 Consequently, the entire device collapsed into the long sheath for removal.
Coronary wire trap technique. In 2018, Khosravi et al invented the "coronary wire trap technique” (CWT) and applied it successfully for the retrieval of embolized ASD occluders.32 Following the failure of other common retrieval techniques, the authors decided to use coronary wire to trap the embolized device for retrieval. They advanced a Pilot 50 coronary wire (Abbott) through the embolized device disk. Next, the distal tip of the 0.014-inch pilot wire was snared, allowing the embolized occluder device to be trapped and easily pulled back into the sheath with removal through the right femoral vein. The angiographic image of this method is shown in Figure 1.
Conclusions
With a single exception, all studies that used a single snare technique reported a very high success rate. Combined tools retrieval (snare plus snare, snare plus bioptome, or snare plus forceps) and the gooseneck snare technique have also been successfully reported. One study that used the lasso technique was unsuccessful in retrieval. CWT was reported to be a newly modified, successful method of trapping the device with coronary wire and snare for retrieval.
Affiliations and Disclosures
From the 1Hypertension Research Center, Cardiovascular Research Institute, Isfahan University of Medical Sciences, Isfahan, Iran; 2Department of Cardiology, Isfahan University of Medical Sciences, Isfahan, Iran; 3Isfahan Cardiovascular Research Center, Cardiovascular Research Institute, Isfahan University of Medical Sciences, Isfahan, Iran; 4Cardiovascular Research Center, Hormozgan University of Medical Sciences, Bandar Abbas, Iran; 5Department of Medical Genetics, Faculty of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd, Iran; 6Hypertension Research Center, Isfahan Cardiovascular Research Institute, Isfahan University of Medical Sciences, Isfahan, Iran; 7Department of Cardiology, School of Medicine and Modeling in Health Research Center, Shahrekord University of Medical Sciences, Shahrekord, Iran; 8Heart Failure Research Center, Cardiovascular Research Institute, Isfahan University of Medical Sciences, Isfahan, Iran; 9University of Arizona Sarver Heart Center, Tucson, Arizona, USA; 10University of Arizona College of Medicine, Phoenix, Arizona, USA.
Drs Khosravi and Mirbod contributed equally to writing and editing of the manuscript.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: M. Reza Movahed, MD, University of Arizona Sarver Heart Centre, Tucson, AZ, USA. Email: rmova@aol.com
References
1. Ghaderian M, Sabri MR, Ahmadi AR, Alipour MR, Dehghan B, Mehrpour M. Midterm follow-up results of transcatheter interatrial septal defect closure. Heart Views. 2019;20(1):1-5. doi: 10.4103/HEARTVIEWS.HEARTVIEWS_32_19
2. Snijder RJR, Renes LE, Bosshardt D, Suttorp MJ, Ten Berg JM, Post MC. Percutaneous atrial septal defect closure using the occlutech figulla device in adults: More than 800 patient-years of follow-up. J Interv Cardiol. 2020;2020:7136802. doi: 10.1155/2020/7136802
3. Takaya Y, Akagi T, Kijima Y, Nakagawa K, Sano S, Ito H. Long-term outcome after transcatheter closure of atrial septal defect in older patients: impact of age at procedure. JACC Cardiovasc Interv. 2015;8(4):600-606. doi: 10.1016/j.jcin.2015.02.002
4. Katta N, Gautam S, Webel R. Successful percutaneous retrieval of embolized septal occluder device from aortic arch and placement of a newer septal occluder device in combined procedure. Case Rep Cardiol. 2016;2016:1032801. doi: 10.1155/2016/1032801
5. Shebani SO, Rehman R, Taliotis D, et al. Techniques for transcatheter retrieval of the occlutech ASD device United Kingdom-European multicenter report. Catheter Cardiovasc Interv. 2017;89(4):690-698. doi: 10.1002/ccd.26838
6. Levi DS, Moore JW. Embolization and retrieval of the Amplatzer septal occluder. Catheter Cardiovasc Interv. 2004;61(4):543-547. doi: 10.1002/ccd.20011
7. DiBardino DJ, McElhinney DB, Kaza AK, Mayer JE, Jr. Analysis of the US Food and Drug Administration Manufacturer and User Facility Device Experience database for adverse events involving Amplatzer septal occluder devices and comparison with the Society of Thoracic Surgery congenital cardiac surgery database. J Thorac Cardiovasc Surg. 2009;137(6):1334-1341. doi: 10.1016/j.jtcvs.2009.02.032
8. Jalal Z, Hascoët S, Gronier C, et al. Long-Term outcomes after percutaneous closure of ostium secundum atrial septal defect in the young: A nationwide cohort study. JACC Cardiovasc Interv. 2018;11(8):795-804. doi: 10.1016/j.jcin.2018.01.262
9. Pillai AA, Satheesh S, Pakkirisamy G, Selvaraj R, Jayaraman B. Techniques and outcomes of transcatheter closure of complex atrial septal defects - single center experience. Indian Heart J. 2014;66(1):38-44. doi: 10.1016/j.ihj.2013.12.016
10.. Yang MC, Wu JR. Recent review of transcatheter closure of atrial septal defect. Kaohsiung J Med Sci. 2018;34(7):363-369. doi: 10.1016/j.kjms.2018.05.001
11. Rao PS, Harris AD. Recent advances in managing septal defects: atrial septal defects. F1000Res. 2017;6:2042. doi: 10.12688/f1000research.11844.1
12. Ooi YK, Kelleman M, Ehrlich A, et al. Transcatheter versus surgical closure of atrial septal defects in children: A value comparison. JACC Cardiovasc Interv. 2016;9(1):79-86. doi: 10.1016/j.jcin.2015.09.028
13. Villablanca PA, Briston DA, Rodés-Cabau J, et al. Treatment options for the closure of secundum atrial septal defects: A systematic review and meta-analysis. Int J Cardiol. 2017;241:149-155. doi: 10.1016/j.ijcard.2017.03.073
14. Butera G, Carminati M, Chessa M, et al. Percutaneous versus surgical closure of secundum atrial septal defect: comparison of early results and complications. Am Heart J. 2006;151(1):228-234. doi: 10.1016/j.ahj.2005.02.051
15. Martínez-Quintana E, Rodríguez-González F. Risks factors for atrial septal defect occlusion device migration. Int J Angiol. 2016;25(5):e63-e65. doi: 10.1055/s-0034-1395976
16. Deşer SB, Demirağ MK. Migration of an atrial septal occluder device with formation of abdominal aortic dissection. Ann Thorac Surg. 2017;103(4):e343-e344. doi: 10.1016/j.athoracsur.2016.08.048
17. Basoor AS, Cotant JF, Halabi AR, DeGregorio M, Chughtai H, Patel KC. Minimally invasive retrieval of patent foramen ovale closure device after device migration to the descending aorta. Tex Heart Inst J. 2012;39(4):582-584.
18. Pavithran S, Sivakumar K. A novel snare assistance safeguards against early embolization of devices and facilitates quick retrieval of malpositioned devices in atrial septal defects with deficient margins. Ann Pediatr Cardiol. 2015;8(3):189-195. doi: 10.4103/0974-2069.164685
19. Her AY, Lim KH, Shin ES. Transcatheter retrieval of embolized atrial septal defect occluder device by waist capture technique. Int Heart J. 2018;59(1):226-228. doi: 10.1536/ihj.17-227
20. Ha KS, Choi JY, Jung SY, et al. A novel double snare technique to retrieve embolized septal and left atrial appendage occluders. J Interv Cardiol. 2018;31(5):685-692. doi: 10.1111/joic.12513
21. Filippone G, La Barbera G, Valentino F, Ocello S, Talarico F. Transcatheter retrieval of Amplatzer Septal Occluder device embolized into the abdominal aorta. SAGE Open Med Case Rep. 2019;7:2050313x19842462. doi: 10.1177/2050313X19842462
22. Georgiev S, Tanase D, Genz T, et al. Retrieval of large Occlutech Figula Flex septal defect occluders using a commercially available bioptome: proof of concept. Cardiol Young. 2018;28(7):955-960. doi: 10.1017/S1047951118000586
23. Sinha S, Levi D, Peirone A, Pedra C. Techniques for trans-catheter retrieval of embolized Nit-Occlud(®) PDA-R and ASD-R devices. Catheter Cardiovasc Interv. 2018;91(3):478-484. doi: 10.1002/ccd.27423
24. Ramalingam R, Patil S, Setty N, et al. Tough, but not impossible - Retrieval of large atrial septal occluder devices embolized to left atrium. Interv Med Appl Sci. 2017;9(1):42-46. doi: 10.1556/1646.9.2017.1.03
25. Ahn J, Kim JH, Choi JH, Oh JH. Percutaneous retrieval and redeployment of an atrial septal occluder under three-dimensional transesophageal echocardiographic guidance: a case report. J Korean Med Sci. 2014;29(6):871-873. doi: 10.3346/jkms.2014.29.6.871
26. Loh JP, Satler LF, Slack MC. Management of a large atrial septal occluder embolized to the left ventricular outflow tract without the use of cardiac surgery. Catheter Cardiovasc Interv. 2014;84(3):497-502. doi: 10.1002/ccd.25361
27. Goel PK, Kapoor A, Batra A, Khanna R. Transcatheter retrieval of embolized AMPLATZER Septal Occluder. Tex Heart Inst J. 2012;39(5):653-656.
28. Chan KT, Cheng BC. Retrieval of an embolized amplatzer septal occluder. Catheter Cardiovasc Interv. 2010;75(3):465-468. doi: 10.1002/ccd.22297
29. Pala S, Açar G, Tigen K, Kırma C. Percutaneous retrieval of an interatrial septal occluder device embolized into the aortic arch. Turk Kardiyol Dern Ars. 2010;38(7):502-504.
30. Shirodkar S, Patil S, Pinto R, Dalvi B. Successful retrieval of migrated Amplatzer septal occluder. Ann Pediatr Cardiol. 2010;3(1):83-86. doi: 10.4103/0974-2069.64365
31. Balbi M, Pongiglione G, Bezante GP. Percutaneous rescue of left ventricular embolized amplatzer septal occluder device. Catheter Cardiovasc Interv. 2008;72(4):559-562. doi: 10.1002/ccd.21679
32. Khosravi A, Mirdamadi A, Movahed MR. Successful Retrieval of embolized atrial septal defect occluder and patent foramen ovale closure device using novel coronary wire trap technique. Catheter Cardiovasc Interv. 2018;92(1):189-192. doi: 10.1002/ccd.26955
33. Najafi A, Koulia K, Aubert P, Binkert CA. Multi loop snare technique for difficult inferior vena cava filter retrievals. CVIR Endovasc. 2018;1(1):33. doi: 10.1186/s42155-018-0042-0
34. Asirvatham R, Vaidya V, Thome T, Friedman P, Cha Y-M. Nanostim leadless pacemaker retrieval and simultaneous micra leadless pacemaker replacement: a single-center experience. J Interv Card Electrophysiol. 2020;57(1):125-131. doi: 10.1007/s10840-019-00647-3
35. Seong C, Kim YJ, Chung J, et al. Tubular foreign body or stent: safe retrieval or repositioning using the coaxial snare technique. Korean J Radiol. 2002;3(1):30-37. doi: 10.3348/kjr.2002.3.1.30
36. Alkhouli M, Aljohani S, Kucera R, Moiduddin N, Hull R. A double-snare technique for safe retrieval of embolized left atrial appendage occluders. JACC Cardiovasc Interv. 2017;10(5):e55-e56. doi: 10.1016/j.jcin.2016.12.022
37. Faccini A, Butera G. Atrial septal defect (ASD) device trans-catheter closure: limitations. J Thorac Dis. 2018;10(Suppl 24):S2923-s2930. doi: 10.21037/jtd.2018.07.128
38. Gheorghe L, Ielasi A, Rensing B, et al. Complications following percutaneous mitral valve repair. Front Cardiovasc Med. 2019;6:146. doi: 10.3389/fcvm.2019.00146
39. Wang PC, Liang HL, Wu TH, Huang JS, Lin YH, Huang YL, et al. Percutaneous retrieval of dislodged central venous port catheter: experience of 25 patients in a single institute. Acta Radiol. 2009;50(1):15-20. doi: 10.1080/02841850802524493
40. Padala SK, Saini A, Gertz ZM, Morano GS, Ellenbogen KA, Koneru JN. A novel percutaneous technique using lasso catheters for retrieval of an embolized amplatzer atrial septal occluder device. JACC Cardiovasc Interv. 2017;10(3):e25-e26. doi: 10.1016/j.jcin.2016.11.052













