

Quadricuspid Aortic Valve in a Neonate With Fallot’s Tetralogy
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
A 3-day-old male neonate was referred to our hospital for a cardiac echocardiogram. He was born at 40 + 5 weeks’ gestation via cesarean section with a birth weight of 3170 grams. The APGAR scores were 8 at 1 minute and 10 at 5 minutes. He had initial tachypnea and an episode of transient desaturation. An initial cardiac ultrasound scan revealed a “subaortic ventricular septal defect”.
On examination, he was fit and well with a heart rate of 130 beats per minute and an oxygen saturation of 97% in air. On auscultation, he had a grade II/VI holosystolic murmur over the fourth intercostal space.
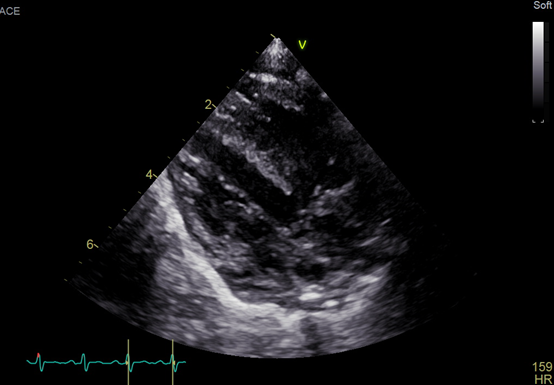
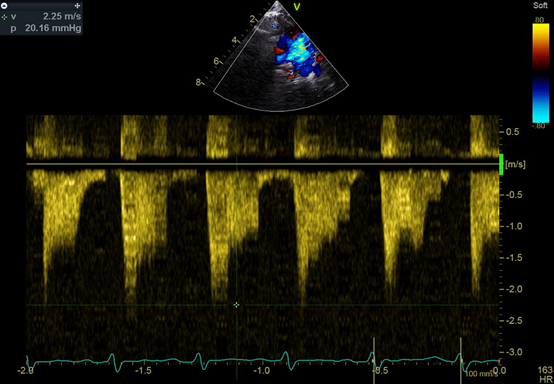
An echocardiogram showed a large ventricular septal defect overriding the aorta with septum and quadricuspid aortic valve (Figure). No stenosis or regurgitation was observed though the valve. The valve consisted of 3 equal cusps and a smaller one, which is type B according to the Hurwitz and Roberts classification (Video). Fluorescent in situ hybridization was negative for 22q11 deletion. The patient established feeds and was discharged home with the plan to have regular follow-ups.
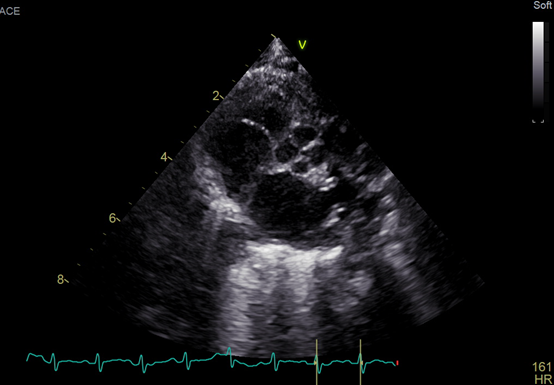
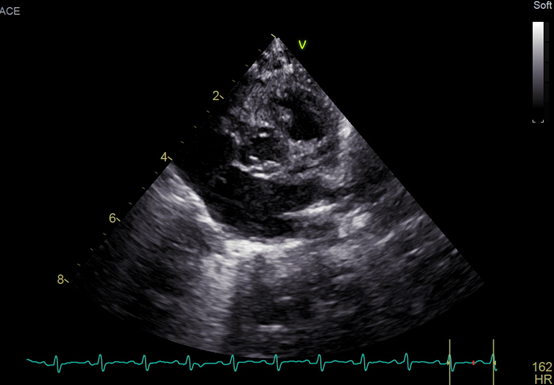
Quadricuspid aortic valve is a rare congenital anomaly with an observed frequency of 0.003% to 1.46%; the average age of diagnosis is 43 years (range, 2 days to 84 years).1 There are 2 classification systems used to describe quadricuspid aortic valve: one is by Hurwitz and Roberts, which is based on the cusps’ relative sizes, and the other is Nakamura’s classification system, which is based on the position of the supernumerary cusp.1
This is the first case of Fallot’s tetralogy and quadricuspid aortic valve described in a neonate. Follow-up would be needed to time the intervention and repair.
Affiliations and Disclosures
From the 1University of West Attica, Aigaleo, Greece; 2Cardiology Department, Agia Sofia Children’s Hospital, Athina, Greece; 3First Department of Pediatrics, National and Kapodistrian University of Athens, Athens, Greece.
Acknowledgments: The authors wish to thank Drs Sofia Chante and Margarita Pesmatzoglou for their valuable contribution.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Andriana Anagnostopoulou, MSc, MRCPCH, Thivon and Livathias, GR11527 Athens, Greece. Email: Mdyy18003@uniwa.gr
Reference
- Saith S, Saith S, Murthy A. Quadricuspid aortic valve: An introduction for clinicians. Cardiol Res. 2022;13(1):2-10. doi: 10.14740/cr1308










