


How To Address Nail Bed Injuries
Injuries involving the toe nail bed and adjacent tissues are very common. Acute injuries to these structures are frequently caused by dropping a heavy object on the toe or by stubbing the toe into a solid object. Less common mechanisms of acute injury include nail bed lacerations and puncture wounds. Chronic nail trauma is usually caused by repetitive mechanical pressure associated with hammertoe or claw toe deformities aggravated by weightbearing and shoe gear contact. This can also lead to toe nail and bed hyperkeratosis and nail plate dystrophy. Failure to identify and repair an acute nail bed defect in a timely fashion may result in less than satisfactory nail plate regeneration. This would be due to the formation of a nail bed scar that prevents plate adherence to the bed and the subsequent development of onycholysis of the newly formed nail plate. Clinicians can provide appropriate acute care of most nail bed injuries in the office or emergency department. When it comes to nail bed injuries that are proximal to the lunula, those that are heavily contaminated or infected, or nail bed injuries among patients with less than optimal vascular status or uncontrolled systemic disease, it may be best to treat these injuries in the operating room. Functional as well as cosmetic defects can develop following injuries involving the nail bed and associated structures (also see “An Overview Of Nail Anatomy And Physiology” below). Sequellae of such injuries include permanent nail plate thickening and discoloration, distorted orientation and onychocryptosis, and chronic onycholysis with exposure of the subungual space and nail bed. It is not uncommon to observe a patient who relates the development of a deformed or mycotic toenail following an injury wherein a subungual hematoma developed secondary to disruption of the nail bed. Baden has described arrest of nail plate growth for up to three weeks following injury to the nail bed or significant systemic disease.4 This results in the development of a Beau’s line that involves relative thickening of the nail plate proximal and distal to a visibly thinner transverse line secondary to the temporary arrest of nail plate production. Injuries that simultaneously disrupt the proximal portion of the nail bed and the proximal nail fold (PNF) may heal with the nail fold adherent to the bed, thereby inhibiting matrix function at the site of the adhesion and resulting in a split nail (canaliformis) deformity.
An Overview Of Nail Anatomy And Physiology
The perionychium consists of the proximal nail fold (PNF), medial and lateral nail grooves and folds, the nail matrix and the nail bed.1 The nail plate is secured proximally in the groove of the PNF, where the stratum corneum of the PNF extends distally over the dorsum of the nail plate as the cuticle. The cuticle acts to seal the plate into the adjacent folds. The plate itself originates from the germinative matrix situated deep to the PNF and extending distally to the level corresponding to the distal margin of the lunula. The lunula is the whitish-appearing, semi-lunar area of matrix extending distally to the PNF and cuticle. Underlying the nail plate is the longitudinally furrowed nail bed, upon which the nail plate glides as it grows distally from the root matrix. It takes approximately five to six months, and frequently as long as seven to nine months, to grow an entirely new toenail in a healthy adult.2 In general, toenails grow faster in children than in adults, slightly faster in warmer climates, more slowly under the influence of ischemia, and typically slower than fingernails in the same individual. As a rule, at least 5 mm of stable nail bed are needed distal to the lunula in order to achieve satisfactory adherence of the plate to the bed. The skin of the nail bed is supported by a highly vascularized subcutaneous layer that intimately links the nail bed to the dorsal periosteum of the distal phalanx.3 The subungual glomus is a rich vascular network of microscopic vessels situated in the subcutaneous tissue deep to the nail bed, and plays a role in peripheral temperature regulation. Distal to the hyponychium and plantar to the medial and lateral nail folds, the digital pulp surrounds the distal phalanx and conveys vessels and nerves to and from the toe tip.
How To Handle Subungual Hematomas
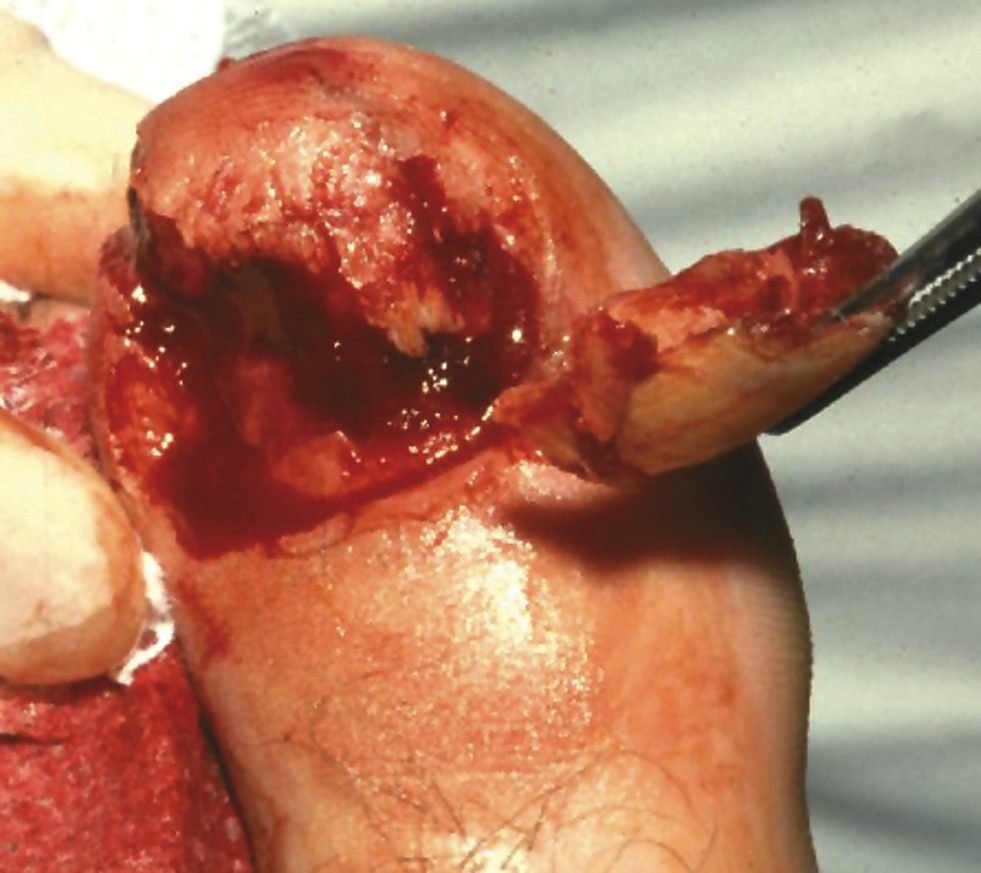
If sufficient blunt or sharp force is applied to the nail plate and surrounding folds, it can violate the structural integrity of the nail bed and the resultant hemorrhage can fill the potential space that normally exists between the nail plate and the underlying nail bed. The force of the injury as well as the hemorrhagic response can separate the nail plate from the bed, causing traumatic onycholysis. If the force is sufficient enough, the proximal margin of the plate will often separate from the root region in the PNF and elevate through the nail fold. This disrupts the seal of the cuticle and potentially exposes the underlying tissues to bacterial contamination. If there is an associated fracture, the patient may be at risk for distal phalangeal osteomyelitis.5 Whenever a patient presents with an acutely injured, throbbing toe with a subungual hematoma, one should consider disruption of the nail plate. If the patient maintains structural integrity of the nail folds and there is disruption of the nail bed, subungual pressure secondary to hemorrhage can cause persistent digital pain that may last for several hours to several days. Only drainage of the subungual hematoma will usually provide relief. As a rule, a subungual hematoma confirms the diagnosis of a disrupted nail bed. It is also important to keep in mind that approximately 20 to 25 percent of digital injuries displaying subungual hematoma are associated with a concomitant phalangeal fracture and one should consider radiographic inspection.6 There are many ways to drain a painful subungual hematoma safely. The method one uses is based on the structural integrity of the nail folds and the amount of the visible nail plate associated with the hematoma. As a rule, when there are stable nail folds and an injury displaying < 25 percent of the visible nail plate associated with the hematoma, one can drain the hematoma through the nail plate using a hand cautery unit, an 18 gauge needle, a small rotary bur or a #11 bayonet blade. The clinician may use any of these instruments to pierce or perforate the plate, and allow evacuation of the underlying, unclotted blood. In order to enable appropriate manipulation of the digit, it may be necessary to perform a local anesthetic block proximal to injured tissues (typically at the base of the digit or at the metatarsal level). As with all violations of the cutaneous barrier, clinicians should consider tetanus prophylaxis and antibiotic therapy, and use aseptic technique for tissue manipulation. If the blood has clotted firmly, direct an appropriately sized needle through the drainage portals for gentle lavage with normal sterile saline. After evacuating the hematoma, apply a water soluble antiseptic solution or antibiotic cream, and a dry sterile dressing with appropriate splinting. Proceed to schedule a follow-up inspection. If the subungual hematoma involves greater than 25 percent of the visible nail plate and/or the nail plate has been avulsed in such a way as to disrupt the proximal, medial or lateral nail folds contiguous with the bed, then a significant nail bed laceration is likely. Accordingly, one should remove the entire plate in order to facilitate direct visualization and surgical repair of the nail bed defect.
Pertinent Pointers On Treating Nail Bed Lacerations
Once one has removed the nail plate, clinicians may use dilute povidone iodine irrigation or another suitable antiseptic to flush away hematoma and debris. One should take care to avoid overaggressive debridement of the rather friable nail bed. Proceed to inspect the bed and repair the laceration with 4-0 or 5-0 absorbable suture on a tapered needle in a simple interrupted fashion. Alternatively, researchers have shown that tissue adhesives can be useful for nail bed repair.7,8 The primary goal of nail bed repair is to decrease the likelihood of hypertrophic nail bed scar formation that inhibits proper adherence of the plate to the bed as a new nail emerges during the post-repair period. One can easily repair lacerations of the surrounding nail folds with 4-0 or 5-0 nonabsorbable simple interrupted sutures on a reverse cutting needle. However, clinicians should be careful to avoid driving the needle through the germinative matrix. One can maintain the cul-de-sac nature of the proximal nail groove by positioning a non-adherent gauze between the proximal nail bed and the PNF, and placing it evenly over the repaired nail bed. Then clinicians should bandage the digit in a sterile fashion and, if indicated, use an appropriate splint to stabilize the injured digit. Clinicians should redress the wound in approximately one week or sooner if the degree of tissue disruption and contamination warrants an earlier inspection. One would remove nonabsorbable sutures, which are used to repair surrounding nail folds, or the skin of the digital pulp at approximately 10 to 14 days. Thereafter, schedule follow-up visits in order to monitor the emerging, new nail plate until it fully covers the bed. It is wise to warn the patient of the potential for permanent nail plate dystrophy, secondary fungal infection and other complications at the time of the initial repair.
Key Insights For Managing Nail Bed Lacerations And Phalangeal Fractures
Clinicians manage crushing nail bed lacerations in a fashion similar to the method one employs for simple nail bed lacerations. However, there is a greater degree of tissue disruption, more extensive debridement is often required and the closure may be more complicated. These injuries are almost always associated with underlying phalangeal fracture and large segments of unstable nail bed may be present. Once again, violation of the cutaneous barrier in these cases constitutes an open fracture. Accordingly, providing appropriate local wound care, tetanus prophylaxis and antibiotic therapy is warranted. When it comes to small, unstable fragments of bone that are exposed to the external environment or those that are far displaced, one should excise these as part of the debridement. If the wound is obviously infected or heavily contaminated, repeat surgical debridement as needed and consider delayed closure. When fragments remain in satisfactory alignment, clinicians can usually reduce and stabilize these by reapproximating the nail bed and splinting the digit in a fashion consistent with the extent of the osseous and articular injury. Due to the intimate proximity of the nail bed to the periosteum of the distal phalanx, satisfactory spontaneous reduction of transverse or short oblique distal phalangeal fractures usually occurs with nail bed repair. In regard to large fragments that remain grossly unstable, one can reduce these with a single axial Kirschner wire or, if necessary, open reduction and internal or percutaneous fixation. When treating patients less than 18 years of age, surgeons must consider the status of the distal phalangeal physis. Obtaining a contralateral digital radiograph may be useful for comparison. Severe stubbing or plantarflexory injuries can affect nail bed laceration and phalangeal fractures that propagate along the dorsal surface of the nail plate into the proximal nail fold and through the physeal plate of the distal phalanx, separating the nail plate from the ventral surface of the PNF.9 When this occurs, the basilar epiphysis is usually dorsally displaced relative to the nail bed because the epiphysis remains anchored to the interphalangeal collateral ligaments and the extensor tendon.10 One would treat this injury by removing the nail plate or at least the proximal portion of the nail plate and following up with cleansing debridement and inspection. Clinicians should then reapproximate the nail bed and adjacent medial and lateral nail folds in accordance with the degree of tissue contamination and disruption. Then proceed to splint the toe in slight dorsiflexion and maintain it in an appropriate splint. This injury rarely requires pin stabilization.
A Guide To Nail Bed Avulsion And Phalangeal Degloving
The likelihood of achieving a satisfactory functional and cosmetic result following acute care decreases substantially with nail bed avulsion injuries, phalangeal degloving and partial digital amputations. Rosenthal classified nail bed injuries according to the level and direction of tissue loss.3 The three levels of injury include: zone I, distal to the distal phalanx; zone II, distal to the lunula; and zone III, proximal to distal end of the lunula. The direction of tissue loss is classified as dorsal oblique, transverse, plantar oblique, tibial or fibular axial, or central (gouging). Zone I lesions usually do not involve bony defects and one can often allow these to heal by secondary intention. Surgeons have also described a variety of skin grafting procedures for lesions measuring greater than 1 cm2.11-13 Zone II injuries are amenable to closure using local advancement flaps in the form of the Atasoy V-to-Y flap and the Kutler biaxial medial and lateral V-flap advancements.14,15 These flap procedures are versatile and one can readily perform these in the office or emergency department. The goal of soft tissue advancement is coverage of the distal phalanx, which may itself require debridement and remodeling of the distal margin in order to enable adequate soft tissue coverage. If an excessive amount of the nail bed has been lost (proximal zone II and zone III injuries) and you anticipate subsequent nail plate instability (less than 5 mm of remaining intact nail bed), then one should consider ablation of the inadequate residual nail bed and reconstruction of the digital tip by means of distal interphalangeal joint disarticulation. Zone III injuries are generally not considered suitable for nail bed reconstruction and complete matrix excision is recommended. One should follow this with reconstruction of the toe tip at an appropriate level. Surgeons can frequently manage these injuries with a partial digital amputation that is often made at the distal interphalangeal level. One would usually perform this procedure after doing an initial debridement and establishing a clean wound that displays residual soft tissue and bone vitality.
Final Notes
Injuries to the nail bed and digital tip are common in the foot. The majority of these injuries are amenable to initial definitive treatment involving drainage of subungual hematoma; nail bed debridement and suture repair; identifying and stabilizing open distal phalangeal fracture; and ensuring subsequent follow-up to monitor nail plate regeneration and adherence. When treating these injuries among children, one has to consider the possibility of fracture cleavage along the plane of the distal phalanx base physis. Finally, one should inform patients to the potential for the development of posttraumatic nail plate dystrophy, particularly onycholysis, and secondary fungal infection of the nail over time. Dr. Malay is a Fellow of the American College of Foot and Ankle Surgeons, and is in private practice at the Ankle and Foot Medical Centers of the Delaware Valley. He is the Director of Podiatric Research at the University of Pennsylvania Medical Center-Presbyterian, and is a Fellow of the Center for Clinical Epidemiology and Biostatistics at the University of Pennsylvania. Dr. Malay is also a faculty member of the Podiatry Institute.
References:
1. Zook EG. The perionychium: anatomy, physiology and care of injuries. Clin Plast Surg 8:21-31, 1981.
2. Zaias N. Embryology of the nail. Arch Dermatol 87:37-53, 1963.
3. Rosenthal EA. Treatment of fingertip and nail bed injuries, Orthop Clin North Am 14:675-697, 1983.
4. Baden HP. Regeneration of the nail. Arch Dermatol 91:619-620, 1965.
5. Fox IM. Osteomyelitis of the distal phalanx following trauma to the nail. A case report. JAPMA 82(10):542-4, 1992.
6. Tucker DJ, Jules KT, Raymond F. Nailbed injuries with hallucal phalangeal fractures—evaluation and treatment. J Amer Podiatric Assoc 86:170-173, 1996.
7. Singer AJ, Hollander JE, Valentine SM, et al. Prospective, randomized, controlled trial of tissue adhesive (20-octylcyanoacrylate) vs standard wound closure techniques for laceration repair. Acad Emerg Med 5:94-100, 1998.
8. Clark RE, Madani S, Bettencourt MS. Nail surgery. Dermatologic Clinics 16:145-164, 1998.
9. Banks AS, Cain TD, Ruch JA. Physeal fractures of the distal phalanx of the hallux. JAPMA 78:310-313, 1989.
10. Hashisume H, Nishida K, Mizumoto D, Takagoshi H, Inoue H. Dorsally displaced epiphyseal fracture of the phalangeal base. J Hand Surg (British) 21:136-138, 1996.
11. Newmeyer WL, Kilgore ES. Fingertip injuries: a simple, effective method of treatment. J Trauma 14:58-64, 1974.
12. Clayburgh RH, Wood MB, Cooney WP. Nail bed repair and reconstruction by reverse dermal grafts. J Hand Surg 8:594-599, 1983.
13. Hsieh SC, Chen SL, Chen TM, Cheng TY, Wang HJ. Thin split-thickness toenail bed grafts for avulsed nail bed defects. Ann Plast Surg 52 (4):375-79, 2004.
14. Atasoy E, Iokimidis E, Kasdan ML, Kutz JE, Kleinert HE. Reconstruction of the amputated fingertip with a triangular volar flap, J Bone Joint Surg 52A:921-26, 1970.
15. Kutler W. A new method for fingertip amputation. JAMA 133:29-30, 1947.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}