


A Guide To Early Intervention For The Charcot Foot
The Charcot syndrome is a devastating condition that can affect the feet or ankles of those with diabetes and peripheral neuropathy. The reports on the incidence and prevalence of Charcot foot vary widely, and range between 0.1 to 29 percent among people with diabetes. These studies indicate a trend for a higher frequency in those with peripheral neuropathy and in specialty clinics.1 The specialty clinic providers may have a higher clinical suspicion and may accordingly arrive at a diagnosis more rapidly and definitively. The risk of amputation increases as the Charcot foot becomes more complicated. Therefore, early intervention is paramount to prevent deformity and ulceration. Effective management of the Charcot foot centers on early diagnosis, medical therapies and surgical interventions. The timeliness of diagnosis is one of the most vital “interventions” that one can perform. The diagnostic delay averaged 29 weeks in one Charcot foot study.2 If one misses the Charcot syndrome diagnosis, joint subluxations and deformity can occur. Joint deformity is a risk factor for ulceration.3 The natural history of the Charcot foot is one of inflammation, deformity, ulceration and amputation.4 The “early” diagnosis is primarily clinical. It requires a heightened suspicion for the syndrome.5 The clinical signs and symptoms include a warm, edematous foot. The temperature difference is often near 10º F between feet while 4º is considered significant for diagnosis.6 One can measure the temperature with a non-contact infrared thermometer or a digital dermal thermometer (TempTouch, Diabetica Solutions). Approximately half of the time, the patient will recall a minor, rather innocuous trauma that sparked the event.7 There must be some level of peripheral neuropathy although some patients report a deep pain with their Charcot foot. One may detect autonomic neuropathy during the clinical exam by using the Neuropad (Miro Verbandstoffe) or by checking for a lack of heart rate variability to deep breathing. When it comes to more advanced presentations with rocker bottom deformity or ulceration, the diagnosis of Charcot foot might be more evident but differentiating it from osteomyelitis (or a concomitant presentation) can be difficult.8 In these cases, it can be useful to have an algorithm to determine if osteomyelitis is present.
Key Insights On Diagnostic Imaging
The decision process begins with clinical suspicion and subsequent evaluation of plain radiographs. If there is no bone destruction on plain radiography, a standard three-phase technetium-99 bone scan can help to uncover increased bone turnover near the suspected joint. If there is bone destruction on X-ray, the three-phase bone scan might not be of much use as it would likely be positive. In this case and with the presence of an ulcer, obtaining a white blood cell-labeled scan can help to confirm osteomyelitis. If this scan is negative, the diagnosis is likely Charcot foot. If it is positive, it is either osteomyelitis or Charcot joint disease with osteomyelitis. There is some controversy about using magnetic resonance imaging (MRI) to differentiate Charcot syndrome from osteomyelitis as both appear similar with this method of imaging. While the white blood cell-labeled scan is extremely sensitive, it is of benefit to observe “secondary signs” on the MRI.9 Accordingly, physicians should keep the following points in mind with osteomyelitis. • Osteomyelitis generally affects a single bone. • Osteomyelitis generally has an extending tract. • Osteomyelitis rarely results in joint deformity. Additionally, C-reactive protein seems to be elevated in acute infection and not in the Charcot foot. This may aid in the differentiation of the two disease processes.9 More recently, researchers have proven that positron emission tomography (PET) scans are useful in differentiating Charcot foot from osteomyelitis, capitalizing on the metabolic rate differences of the two diseases.10
A Pertinent Overview Of Charcot Staging
Clinical staging or classification can help to facilitate communication between professionals, prognosticate outcome and facilitate treatment.11 Classification of the Charcot foot can be anatomic, pathologic or clinical/prognostic. The Sanders-Frykberg classification is the most widely used anatomic classification.12 These authors note that Charcot may affect the forefoot, the tarsometatarsal joint, the Chopart’s or naviculocuneiform joints, the ankle or subtalar joints, or be isolated to the calcaneus. The most recognized pathologic classification is the Eichenholtz classification.13 While this classification is not specific to the foot, Eichenholtz described the pathology at the joint level both histologically and radiographically. Stage I is the stage of development characterized by osseous fragmentation and articular debris. Stage II is the stage of coalescence in which the debris absorbs and edema lessens. Stage III is the stage of reconstruction, which occurs indefinitely and is characterized by the rounding of bone ends and exuberant bone formation in an attempt to restore normal architecture. Stage 0, which was added later by Shibata, is a prodromal period initiated by trauma but without the radiographic findings of Charcot’s arthropathy.14 Examples could be an acute ankle sprain or an ankle fracture in someone with diabetes and neuropathy.15 Rogers and Bevilacqua recently offered a clinical classification that uses a common sense approach to follow the natural history of Charcot.5 This classification uses a two-axis system, similar to the University of Texas Diabetic Foot Ulcer Classification System, which uses a grade and a stage. The X axis represents the anatomical pattern (forefoot, midfoot and rearfoot/ankle). The Y axis accounts for the complexity of the disease: acute (no deformity), deformity, ulceration and osteomyelitis. The authors hypothesize that as one moves to the right on the X axis (more proximal) or down the Y axis (more complicated), the risk of amputation increases.
Current Concepts In Non-Surgical Treatment
The decision to operate or to treat medically is multifaceted. The goals of treatment are to prevent deformity, avoid further trauma, obtain a shoeable foot and avoid excess pressure on the skin that might lead to ulceration.16 The least invasive mechanism to obtain the above goals is the most appropriate. Generally in earlier stages, one can avoid surgery. Offloading is an important component of early management. The best method of offloading is non-weightbearing but this is not always practical. The total contact cast (TCC) reduces peak plantar pressure and patients can utilize it with partial weightbearing. The TCCs are time consuming to apply and improper application can cause ulcerations.17 The instant TCC (iTCC) is another option whereby the practitioner uses a removable cast walker that is rendered irremovable. One can accomplish this by securing the device with fiberglass, plaster or a cohesive bandage. The mean length of time required for TCC before the Charcot foot becomes quiescent is 18.5 weeks. This illustrates the prolonged time needed for the conservative treatment of this disorder.4 One of the targets for pharmacologic therapy is the increased osteoclastic activity, which results in decreased bone mineral density that may occur with Charcot syndrome. Research has shown that the bisphosphonates pamidronate (IV) and alendronate (PO) (Fosamax, Merck) arrest the bone resorptive process.18 They have shown promise in normalizing foot temperatures and reducing urinary markers of bone turnover. Another antiresorptive agent is calcitonin (intranasal), which inhibits osteoclasts. This medication has also reduced bone-specific alkaline phosphatase and skin temperatures in the Charcot foot (see “What About Antiresorptive Treatments For The Charcot Foot?” above).19 Future therapies may center around modulating the balance of osteoprotegerin (OPG) and the receptor activator of nuclear kappa-B ligand (RANK-L).20 The receptor activator of nuclear factor kappa-B ligand (RANK-L) activates osteoclast progenitor cells and leads to bone resorption. The exaggerated inflammatory response in acute Charcot foot has shown overexpression of tumor necrosis factor-alpha (TNF-alpha) and interleukin 1 and 6 (IL-1 and IL-6).18 The theory is that TNF-alpha inhibitors, such as infliximab (Remicade, Centocor) or etanercept (Enbrel, Amgen/Wyeth), or high-dose corticosteroids may halt the inflammatory process.21 However, these agents have not yet been studied in the Charcot foot. Additionally, physicians should be cautious with these agents since they have immunosuppressive properties and could lead to soft tissue infections. Research has shown that external bone stimulation through ultrasonic and electromagnetic fields speeds bony consolidation.22,23 Other authors have noted the use of implantable DC electric bone stimulators may be of adjunctive benefit during surgical treatment.24
When Surgical Intervention Is Indicated
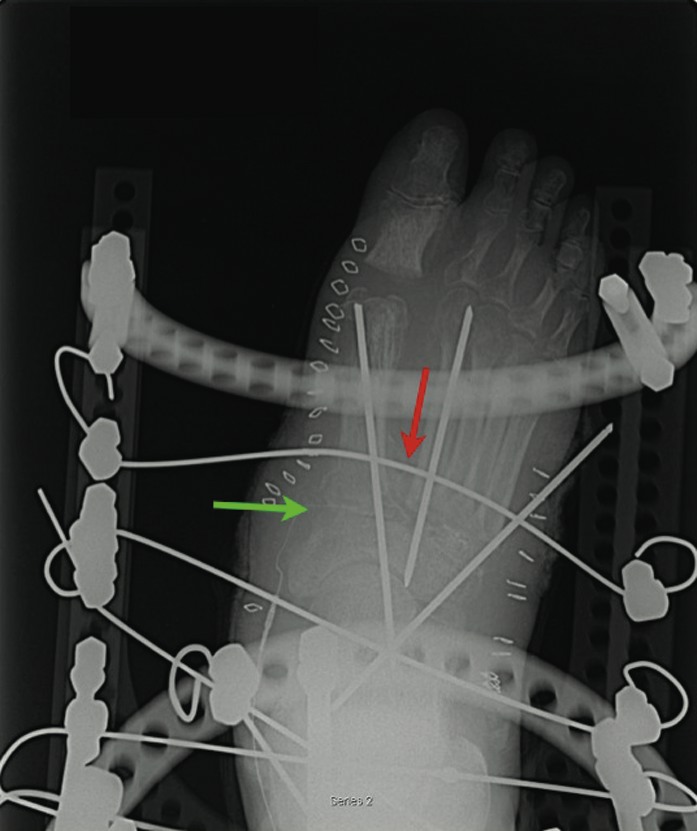
Surgical interventions vary from Achilles tendon lengthening and exostecomy to foot reconstruction. Achilles tendinopathy leading to equinus is a contributor to midfoot dislocation and ulceration. The Achilles tendon is less elastic in Charcot foot.25 In many cases, surgeons perform tendo-Achilles lengthening in combination with medical therapies or more advanced surgical procedures. Exostectomy is a viable option for medial plantar prominences (i.e., navicular). However, this procedure has a higher rate of failure when surgeons attempt to employ it for central and lateral prominences.26 When a surgeon decides to reconstruct, he or she should isolate and fuse the affected joint. The choice of internal or external fixation depends on the quality of the bone. Generally in the Charcot syndrome, the bone stock is poor and external fixation results in better compression with fewer fixation failures. When one uses internal fixation, locking plates may prevent backing out of hardware. The operative technique depends on the pathology but typically involves resection of the affected joint surface. When it comes to midfoot deformities, utilizing a plantar-based wedge resection across the tarsometatarsal joint or naviculocuneiform joints is an option. Apply the external fixator with two tibial rings for stability and drive the wires proximal and distal to the fusion site. One would walk the distal wires back on the foot plate. This provides transverse plane compression across the fusion site. While postoperative recommendations vary, we have found that post-op non-weightbearing reduces complication in Charcot midfoot fusions that have been fixated externally.27 For rearfoot and ankle arthrodesis in the Charcot foot, the technique is slightly different. One would use two tibial rings but the decision to use a talar ring depends on surgeon preference. The addition of this ring allows one to isolate the subtalar joint or the ankle joint for compression. Other methods can accomplish similar compression without completely isolating the non-operative joint. Alternatively, if there is severe frontal plane deformity of the ankle or subtalar joints and both joints require fusion, one may consider intramedullary rod fixation.28 In rearfoot and ankle deformities, dynamization with protected weightbearing after surgery might improve union rates. However, this has not specifically been studied with regard to the Charcot foot. External fixation is associated with a high rate of complications (pin tract infections and wire breakage). However, if physicians recognize these complications early, they can easily address these issues and they are non-limb-threatening.29
Pertinent Insights On Post-Op Prevention
Equally as important as the treatment phase is the post-treatment prevention of recurrence, contralateral Charcot’s joint and ulceration. Once the foot becomes stable and shoeable through medical or surgical means, one must emphasize prevention. The Charcot restraint orthotic walker (CROW) is a custom device that can be an effective method to brace a deformed extremity.30 We recommend using the CROW for at least six months after reconstructive surgery and some patients may require the device for their lifetimes. One may also want to consider prescribing a home dermal thermometer with instructions on proper customized use. The home dermal thermometer can alert the patient to an inflammatory response occurring in his or her foot as this inflammatory response may be a pre-ulcer or a Charcot event. According to the University of Texas Diabetic Foot Risk Classification System, the post-Charcot patient would have a level 3 risk and be at 36 times greater risk for developing a foot ulcer than a patient without diabetes.31 This high-risk patient requires close follow-up and reinforcement of what to do if signs of a foot ulcer or Charcot develop.
Final Notes
Early intervention in the Charcot foot depends entirely on early diagnosis and subsequent treatment depending on the severity of the deformity. A team approach works best to prevent the patient with diabetes and a high-risk foot from succumbing to limb loss. Dr. Rogers is the Director of the Amputation Prevention Center at Broadlawns Medical Center in Des Moines, Iowa. Dr. Frykberg is the Chief of Podiatry at the Carl T. Hayden Veterans Affairs Medical Center in Phoenix. Editor’s note: For related articles, see “Point-Counterpoint: Active Charcot: Should You Proceed With Surgery?” in the March 2005 issue of Podiatry Today, “A Closer Look At Redefining Charcot” in the August 2006 issue or “A Closer Look At Bone Stimulators For Charcot” in the December 2006 issue. For other articles, visit the archives at www.podiatrytoday.com.
References:
1. Frykberg RG, Belczyk R. Epidemiology of the charcot foot. Clin Podiatr Med Surg. Jan 2008;25(1):17-28.
2. Pakarinen TK, Laine HJ, Honkonen SE, Peltonen J, Oksala H, Lahtela J. Charcot arthropathy of the diabetic foot. Current concepts and review of 36 cases. Scand J Surg. 2002;91(2):195-201.
3. Bevan WP, Tomlinson MP. Radiographic measures as a predictor of ulcer formation in diabetic charcot midfoot. Foot Ankle Int. Jun 2008;29(6):568-573.
4. Armstrong DG, Todd WF, Lavery LA, Harkless LB, Bushman TR. The natural history of acute Charcot's arthropathy in a diabetic foot specialty clinic. J Am Podiatr Med Assoc. Jun 1997;87(6):272-278.
5. Rogers LC, Bevilacqua NJ. The diagnosis of Charcot foot. Clin Podiatr Med Surg. Jan 2008;25(1):43-51.
6. Armstrong DG, Lavery LA. Monitoring healing of acute Charcot's arthropathy with infrared dermal thermometry. J Rehabil Res Dev. 1997;34:317-321.
7. Foltz KD, Fallat LM, Schwartz S. Usefulness of a brief assessment battery for early detection of Charcot foot deformity in patients with diabetes. J Foot Ankle Surg. Mar-Apr 2004;43(2):87-92.
8. Rogers LC, Bevilacqua NJ. Imaging of the charcot foot. Clin Podiatr Med Surg. Apr 2008;25(2):263-274.
9. Morrison WB, Schweitzer ME, Batte WG, Radack DP, Russel KM. Osteomyelitis of the foot: relative importance of primary and secondary MR imaging signs. Radiology. Jun 1998;207(3):625-632.
10. Hopfner S, Krolak C, Kessler S, et al. Preoperative imaging of Charcot neuroarthropathy in diabetic patients: comparison of ring PET, hybrid PET, and magnetic resonance imaging. Foot Ankle Int. Dec 2004;25(12):890-895.
11. Frykberg RG, Rogers LC. Classification of the Charcot Foot. In: Frykberg RG, ed. The Charcot Foot. Brooklandville, Md.: Data Trace Publishing. (In Press)
12. Sanders LJ, Frykberg RG. The Charcot Foot. In: Frykberg, ed. The High Risk Foot in Diabetes Mellitus. New York: Churchill Livingstone; 1991:325-335.
13. Eichenholtz SN. Charcot Joints. Springfield: Charles C. Thomas; 1966.
14. Shibata T, Tada K, Hashizume C. The results of arthrodesis of the ankle for leprotic neuroarthropathy. J Bone Joint Surg. 1990;72A:749-756.
15. Yu GV, Hudson JR. Evaluation and treatment of stage 0 Charcot's neuroarthropathy of the foot and ankle. J Am Podiatr Med Assoc. Apr 2002;92(4):210-220.
16. Sanders LJ, Frykberg RG. The Charcot Foot (Pied de Charcot). In: Bowker JH, Pfeifer MA, eds. The Diabetic Foot. Seventh ed. Philadelphia: Mosby Elsevier; 2008.
17. Crews RT, Wrobel JS. Physical management of the Charcot foot. Clin Podiatr Med Surg. Jan 2008;25(1):71-79.
18. Jostel A, Jude EB. Medical treatment of charcot neuroosteoarthropathy. Clin Podiatr Med Surg. Jan 2008;25(1):63-69.
19. Bem R, Jirkovska A, Fejfarova V, Skibova J, Jude EB. Intranasal calcitonin in the treatment of acute Charcot neuroosteoarthropathy: a randomized controlled trial. Diabetes Care. Jun 2006;29(6):1392-1394.
20. Jeffcoate WJ, Game F, Cavanagh PR. The role of proinflammatory cytokines in the cause of neuropathic osteoarthropathy (acute Charcot foot) in diabetes. Lancet. Dec 10 2005;366(9502):2058-2061.
21. Jeffcoate WJ. Theories concerning the pathogenesis of the acute charcot foot suggest future therapy. Curr Diab Rep. Dec 2005;5(6):430-435.
22. Hanft JR, Goggin JP, Landsman A, Surprenant M. The role of combined magnetic field bone growth stimulation as an adjunct in the treatment of neuroarthropathy/Charcot joint: an expanded pilot study. J Foot Ankle Surg. Nov-Dec 1998;37(6):510-515; discussion 550-511.
23. Petrisor B, Lau JT. Electrical bone stimulation: an overview and its use in high risk and Charcot foot and ankle reconstructions. Foot Ankle Clin. Dec 2005;10(4):609-620, vii-viii.
24. Hockenbury RT, Gruttadauria M, McKinney I. Use of implantable bone growth stimulation in Charcot ankle arthrodesis. Foot Ankle Int. Sep 2007;28(9):971-976.
25. Grant WP, Foreman EJ, Wilson AS, Jacobus DA, Kukla RM. Evaluation of Young's modulus in Achilles tendons with diabetic neuroarthropathy. J Am Podiatr Med Assoc. May-Jun 2005;95(3):242-246.
26. Catanzariti AR, Mendicino R, Haverstock B. Ostectomy for diabetic neuroarthropathy involving the midfoot. J Foot Ankle Surg. Sep-Oct 2000;39(5):291-300.
27. Bevilacqua NJ, Rogers LC. Surgical management of charcot midfoot deformities. Clin Podiatr Med Surg. Jan 2008;25(1):81-94.
28. Mendicino RW, Catanzariti AR, Saltrick KR, et al. Tibiotalocalcaneal arthrodesis with retrograde intramedullary nailing. J Foot Ankle Surg. Mar-Apr 2004;43(2):82-86.
29. Rogers LC, Bevilacqua NJ, Frykberg RG, Armstrong DG. Predictors of postoperative complications of Ilizarov external ring fixators in the foot and ankle. J Foot Ankle Surg. Sep-Oct 2007;46(5):372-375.
30. Morgan JM, Biehl WC, 3rd, Wagner FW, Jr. Management of neuropathic arthropathy with the Charcot Restraint Orthotic Walker. Clin Orthop Relat Res. Nov 1993(296):58-63.
31. Lavery LA, Armstrong DG, Vela SA, Quebedeaux TL, Fleischli JG. Practical Criteria for Screening Patients at High Risk for Diabetic Foot Ulceration. Arch Intern Med. 1998;158:158-162.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}