


Bicortical Trephination for the Treatment of Chronic Diabetic Wounds with Exposed Bone: A Case Report
Diabetes mellitus continues to increase globally. One of the most common and severe complications affecting 15% of those with diabetes is the diabetic foot ulcer (DFU).1 Patients with diabetes have a 12–25% lifetime risk of developing a foot ulcer, with 5–8% requiring major amputation within 1 year.2-6 Foot ulcerations precede approximately 85% of lower extremity amputations.7-8
Healing by secondary intention is indicated for many different types of wounds, including wounds over exposed noninfected bone. One must have a proper understanding of treatment of exposed bone to avoid complications and optimize wound healing. In this case study, we report a method of managing a wound over chronically exposed midfoot bone. The bicortical drilling method described here is a variation of a method previously described in which one fenestrates cortical bone to increase the rate of granulation tissue formation.
In chronic open wounds that have denuded bone exposed (devoid of periosteum), granulation tissue forms at the soft tissue-bone interface and migrates centrally to cover the exposed bone.9-10 Chronic exposure of denuded bone usually results devitalization, thus making healing more challenging. However, if the underlying bone is viable, the cortical drilling technique can encourage growth of additional granulation tissue. This works by thinning down the outer layer of compact bone to enter the Haversian system or by fenestrating compact bone to expose the spongy (cancellous) bone.10-12 Following this drilling maneuver, islands of granulation tissue from the drill site coalesce with granulation tissue from the soft tissue-bone interface. One can then allow this new bed of granulation tissue to either re-epithelialize from the wound margins, or apply skin grafts.12
Here we present a challenging case in which conservative and surgical measures failed to achieve wound closure, thus we proceeded with the novel technique of bicortical trephination to assist.
Key Case Details
A 62-year-old male presented with a history of type 2 diabetes mellitus (HbA1c: 6.3%), end-stage renal disease (ESRD), congestive heart failure, midfoot Charcot neuroarthropathy with previous reconstruction, and a chronic non-healing diabetic ulcer of greater than 2 years to the dorsomedial left foot (Figure 1). Diagnostic imaging included plain film radiographs and magnetic resonance imaging (MRI) of the foot and ankle, as well as vascular noninvasive studies (ankle brachial index). X-rays and MRI did not reveal osteomyelitis, and vascular assessment did not show any significant peripheral arterial disease. Previous wound treatments included serial office debridements, offloading with a surgical boot and custom modified shoe wear, negative pressure wound therapy, application of allografts, and surgical debridements including fenestration of cortical bone. The wound became stagnant for approximately 1 month over the exposed midfoot bone at a size of 2.5cm x 2.0cm.

The patient underwent a V-to-Y advancement flap and cortical bone debridement in an attempt to cover the exposed bone (Figure 2).

The postoperative course became complicated by flap necrosis at 2 weeks postop, ultimately ending in wound regression (Figures 3–4).


Due to multiple comorbidities, the patient was not a candidate for free tissue transfer and as such alternatives became limited. We theorized that access to plantar soft tissue would bring an additional source of granulation tissue to the area of the wound. The patient underwent bicortical trephination of the midfoot bone, which included cylindrical bone resection (slightly larger than the wound 0.5cm x 0.5cm) with the use of a 2mm x 20mm Shannon burr to include the plantar cortex (Figure 5a-d).
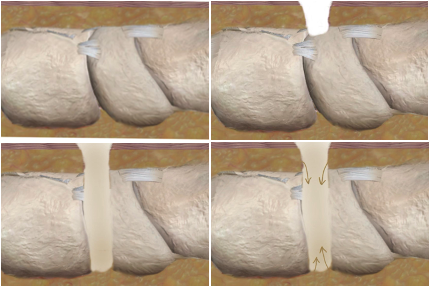
We then packed the wound with a cryopreserved umbilical tissue graft and secured a nonadhesive dressing to the wound site, followed by an overlying bolster dressing to aid in graft incorporation. The postoperative course at this point involved weekly office visits with serial debridements as needed and local wound care until achieving full epithelialization and safe transition into custom diabetic shoes (Figures 6-8).



The patient unfortunately died one year following the healing of his wound due to cardiovascular complications.
Details on Decision-Making
Chronic diabetic nonhealing wounds present a challenge for limb salvage and reconstructive surgeons, especially when bone is exposed. A DFU is one of the most common causes of nontraumatic lower extremity amputations. DFUs with exposed bone are prone to infection, which has been reported to increase amputation rates to as high as 92%.13 In patients with chronic wounds with or without bone exposure, the risk of developing osteomyelitis increases 5-fold13; therefore, when strategizing soft tissue coverage, surgeons have to take into account the size and location of the defect; chronicity of the wound; medical comorbidities; and social history, especially as it pertains to adherence to medical advice.
The reconstructive ladder provides the surgical principles of wound closure from simple (secondary intention) to most complex (free tissue flap), via soft tissue coverage of bone, tendons, and neurovascular structures.14 Free tissue transfer is considered the gold standard in distal lower and upper extremity wounds with exposed bone and tendon.15-16 However, we considered free tissue transfer high-risk in this patient due to his history of ESRD on hemodialysis.
Local flaps, on the other hand, may prove advantageous when the defect is small and can take place under minimal anesthesia, which is particularly favorable in high-risk patients.17 Despite these advantages, local flaps carry a higher complication rate when compared to other flap options. Kim and colleagues reported a postoperative wound complication rate of 67% for local random flaps, 11% for regional flaps, and 21% for free flaps, when comparing flap options for plantar diabetic foot ulcers.17 In addition, they reported partial skin necrosis as the most common cause of local flap failure, which was consistent with our observations with this patient, resulting in regression of wound healing.
We propose the bicortical trephination as a novel option for treating chronic nonhealing wounds with exposed bone. In this technique, the soft tissue adjacent to the far cortex will be exposed and can act as an additional source forming granulation tissue in order to fill the defect. The technique will not be suitable for large wounds as it can negatively affect the stability of the bone. However, it can be considered if performing stabilization with internal or external fixation.
Concluding Thoughts
Our patient did not initially respond to serial debridement or drilling/fenestration of the cortical bone. This could have been due to wound chronicity contributing to deeper devitalization of the bone. By resecting a cylindrical portion of the bone, not only did we expose the soft tissue adjacent to the opposite cortex, but we also resected any nonviable bone that hindered wound healing. As such, bicortical trephination could apply in cases where traditional options have failed in promoting granulation tissue for wound coverage in the setting of exposed bone, as long as it does not compromise the stability of the involved osseous structures.
Dr. Sharif is currently practicing in Atlanta, where he serves as the director of the Emory Midtown Foot and Ankle Fellowship.
Dr. Bergen is a board qualified fellowship-trained foot and ankle surgeon and currently practicing at Charlotte Limb Preservation and Diabetic Foot Center in Charlotte, NC.
References
- Jiang XY, Lu DB, Chen B. Progress in stem cell therapy for the diabetic foot. Diabetes Res Clin Pract. 2012;97(1):43-50.
- Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA. 2005;293(2):217–228.
- Abbott CA, Garrow AP, Carrington AL, Morris J, Van Ross ER, Boulton AJ. Foot ulcer risk is lower in South-Asian and African-Caribbean compared with European diabetic patients in the U.K.: the North-West diabetes foot care study. Diabetes Care. 2005;28(8):1869–1875.
- Katz IA, Harlan A, Miranda-Palma B, et al. A randomized trial of two irremovable off-loading devices in the management of plantar neuropathic diabetic foot ulcers. Diabetes Care. 2005;28(3):555–559.
- Prompers L, Schaper N, Apelqvist J, et al. Prediction of outcome in individuals with diabetic foot ulcers: focus on the differences between individuals with and without peripheral arterial disease. The EURODIALE Study. Diabetologia. 2008;51(5):747–755.
- Jonasson JM, Ye W, Sparen P, Apelqvist J, Nyren O, Brismar K. Risks of nontraumatic lower-extremity amputations in patients with type 1 diabetes: a population-based cohort study in Sweden. Diabetes Care. 2008;31(8):1536–1540.
- Larsson J, Agardh CD, Apelqvist J, Stenstrom A. Long-term prognosis after healed amputation in patients with diabetes. Clin Orthop Relat Res. 1998;350:149–158.
- American Diabetes Association. Consensus development conference on diabetic foot wound care: 7–8 April 1999, Boston, Massachusetts. Diabetes Care. 1999;22(8):1354–1360.
- Bloom RF. Non repair of exposed frontal bone after Mohs surgery for extensive basal cell carcinoma. South Med J. 1980;73:971-974
- Brown PW. The fate of exposed bone. Am J Surg. 1979;137:464-469
- Widmaier Q. The surgical closure of exposed skull. J Maxillo-Surgery. 1975;3:149-155
- Latenser J, Snow SN, Mohs FE, Weltman R, Hruza G. Power drills to fenestrate exposed bone to stimulate wound healing. J Dermatol Surg Oncol. 1991;17(3):265-270.
- Cazzell S, Moyer PM, Samsell B, Dorsch K, McLean J, Moore MA. A prospective, multicenter, single-arm clinical trial for treatment of complex diabetic foot ulcers with deep exposure using acellular dermal matrix. Adv Skin Wound Care. 2019;32(9):409-415.
- Aston SJ, Beasley RW, Throne CHM. Grabb and Smith’s Plastic Surgery (5th ed). Lippincott-Raven Publishers; 1997:13–14.
- Parrett BM, Pomahac B, Demling RH, Orgill DP. Fourth-degree burns to the lower extremity with exposed tendon and bone: a ten-year experience. J Burn Care Res. 2006;27(1):34-39.
- Ducic I, Attinger CE. Foot and ankle reconstruction: pedicled muscle flaps versus free flaps and the role of diabetes. Plast Reconstr Surg. 2011;128(1):173-180.
- Kim YS, Roh SG, Kim JL, Lee NH, Shin JY. Reconstruction of plantar forefoot in diabetic foot ulcers: a comparative study of perforator flaps and random flaps. J Wound Manag Res. 2021;17(1):19-23.






