Managing Acute and Subacute Charcot Neuroarthropathy with Placental Amnion Injections to Mediate Cytokine Dysregulation
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.
Charcot neuroarthropathy can have detrimental effects on the foot and ankle if not managed appropriately and rapidly. In this author’s experience, regenerative medicine therapies offer new and exciting modalities that may control the ill effects of inflammation and accelerate healing in the acute Charcot patient. Along with traditional immobilization and medical management, this may limit the progression of structural deformities that lead to wounds and surgery.
Numerous studies discuss the role of inflammatory cytokines in acute and subacute Charcot fractures.1 Immunomodulation imbalances create an environment of inflammatory cytokines in the acute neuroarthropathic foot that inhibit normal fracture repair mechanisms. This “cytokine storm” causes a chronic inflammatory environment that results in edema, erythema, and pain. Placental tissue is a potent mediator of cytokines.2 Injecting placental tissue into an acute or subacute Charcot fracture controls inflammatory cytokines and allows for a normal bone healing environment.3
A Closer Look at the Case Studies
The following 3 cases present scenarios of placental tissue injection into acute neuroarthropathic joints. All 3 patients had a history of diabetes with elevated HbA1c levels. In addition, these patients all underwent immobilization in a cast boot for at least 6 weeks before the injection. None of these patients had ulcerations or infectious processes. All acute areas of Charcot neuroarthropathy resolved.
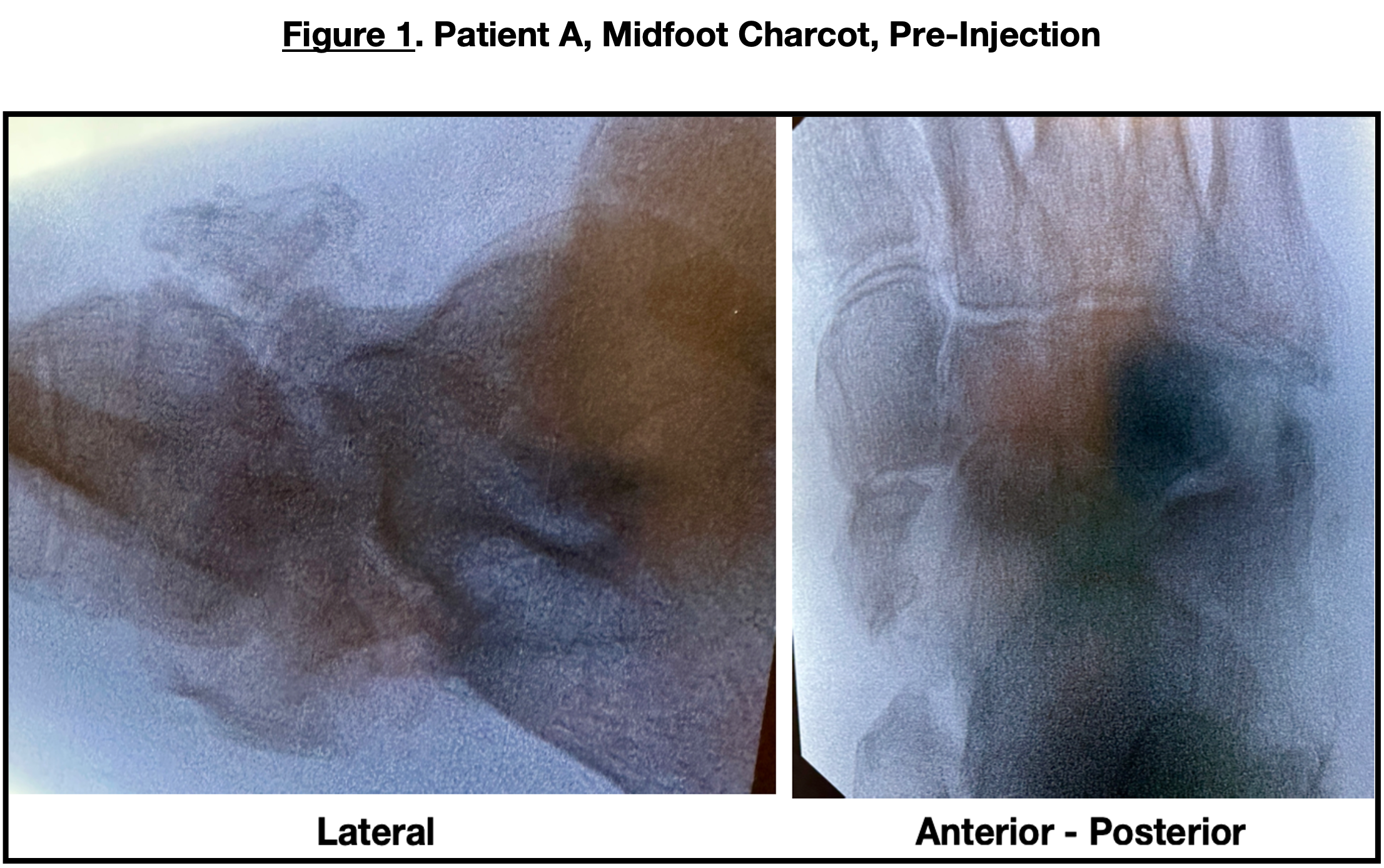
Patient A is a 68-year-old female with a body mass index (BMI) of 45. She had presented to the author’s office with a warm, painful, swollen right foot and ankle. She was afebrile, and there were no open wounds. Magnetic resonance imaging (MRI) ruled out an abscess. A white blood cell-labeled bone scan did not reveal osteomyelitis. Her past medical history included obesity, diabetes (HbA1c 8.2), hypertension, degenerative joint disease, diabetic retinopathy, and seasonal allergies. Medications included amlodipine-valsartan, cetirizine, dextromethorphan-guaifenesin, flecainide, furosemide, glipizide, insulin glargine, liraglutide, and tramadol. She was recently hospitalized for “cellulitis” of the foot. C-reactive protein was 19 mg/dL and had a white blood cell count 10,000 cells/mL. She had no open wounds and had been placed on IV antibiotics; she maintained non-weight-bearing with her leg elevated. The foot and ankle improved clinically during her 2-week admission. After her discharge, the symptoms returned, and she presented to the office.
X-ray examination (Figure 1) revealed osteolysis and the midtarsal, talonavicular, and calcaneocuboid joint collapse. Computed tomography (CT) scans confirmed Charcot ununited fractures at the talonavicular joint with dorsal fragmentation of the navicular.

After confirming no acute infectious process, the patient underwent placental tissue injections into the midfoot fracture areas in the clinic setting. She was placed in a controlled ankle motion (CAM) boot for 4 weeks. She was seen 2 weeks, 6 weeks, and 8 weeks post-injection. The erythema and calor had subsided, and there was radiological evidence of microfracture consolidation. An 8-week follow-up X-ray (Figure 2) revealed continued calcification and consolidation. Follow-up C-reactive protein was 6 mg/dL. The patient then transferred into an extra-depth shoe with appropriate plastizote inserts for full weight-bearing.
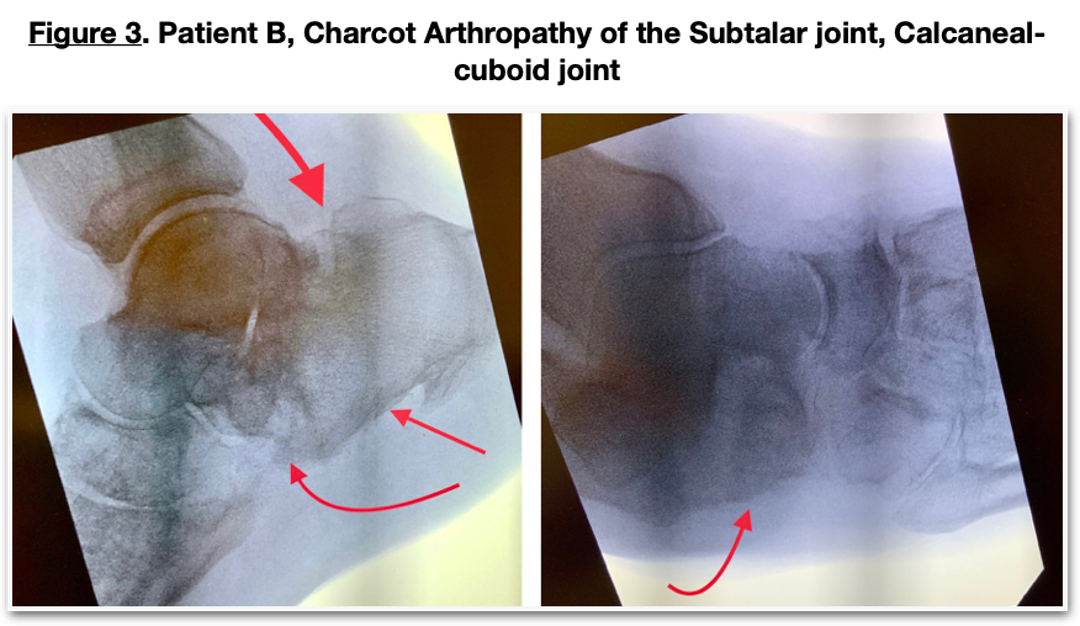
Patient B is a 55-year-old female with a BMI of 40. Her past medical history included diabetes, hypertension, chronic kidney disease (Stage V), end-stage renal disease on dialysis, degenerative joint disease, retinopathy, secondary hyperparathyroidism, and obesity. Medications included rosuvastatin, sertraline, toujeo insulin, auryexia, ferric citrate, furosemide, calcitriol, ezetimibe, vitamin D, and lisinopril. Her HbA1c was 8.7, hematocrit 44%, hemoglobin 13 g/dL, creatinine 3.66 mg/dL, BUN 54 mg/dL, Vitamin D 21 ng/mL, parathyroid hormone 785 ng/L, and C-reactive protein 35 mg/dL. She had been initially immobilized in a CAM boot which was unsuccessful in managing the acute Charcot process. X-rays (Figure 3) revealed subtalar joint collapse, talonavicular joint collapse, anterior calcaneal body fracture, and slight joint depression fracture of the calcaneal body.
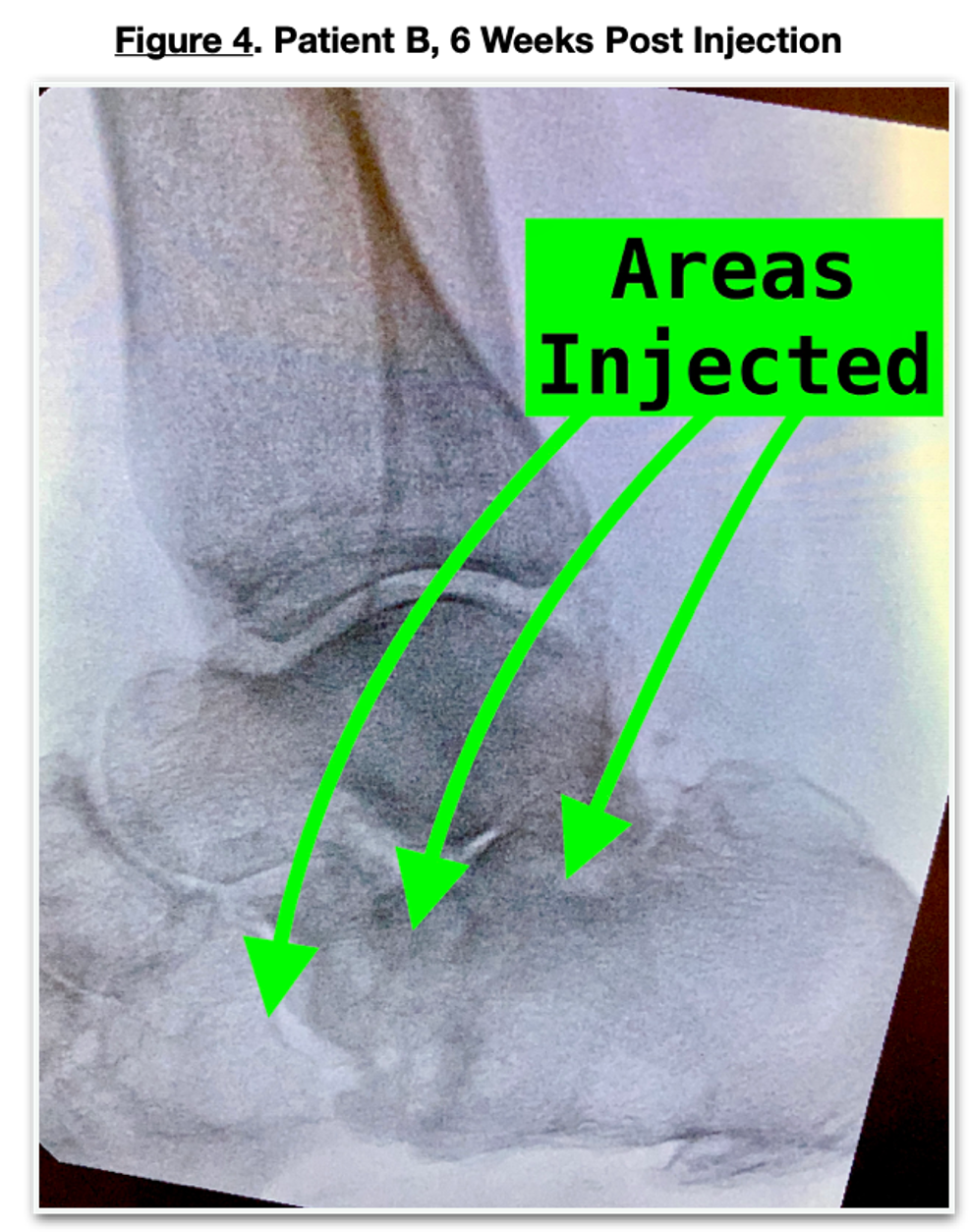
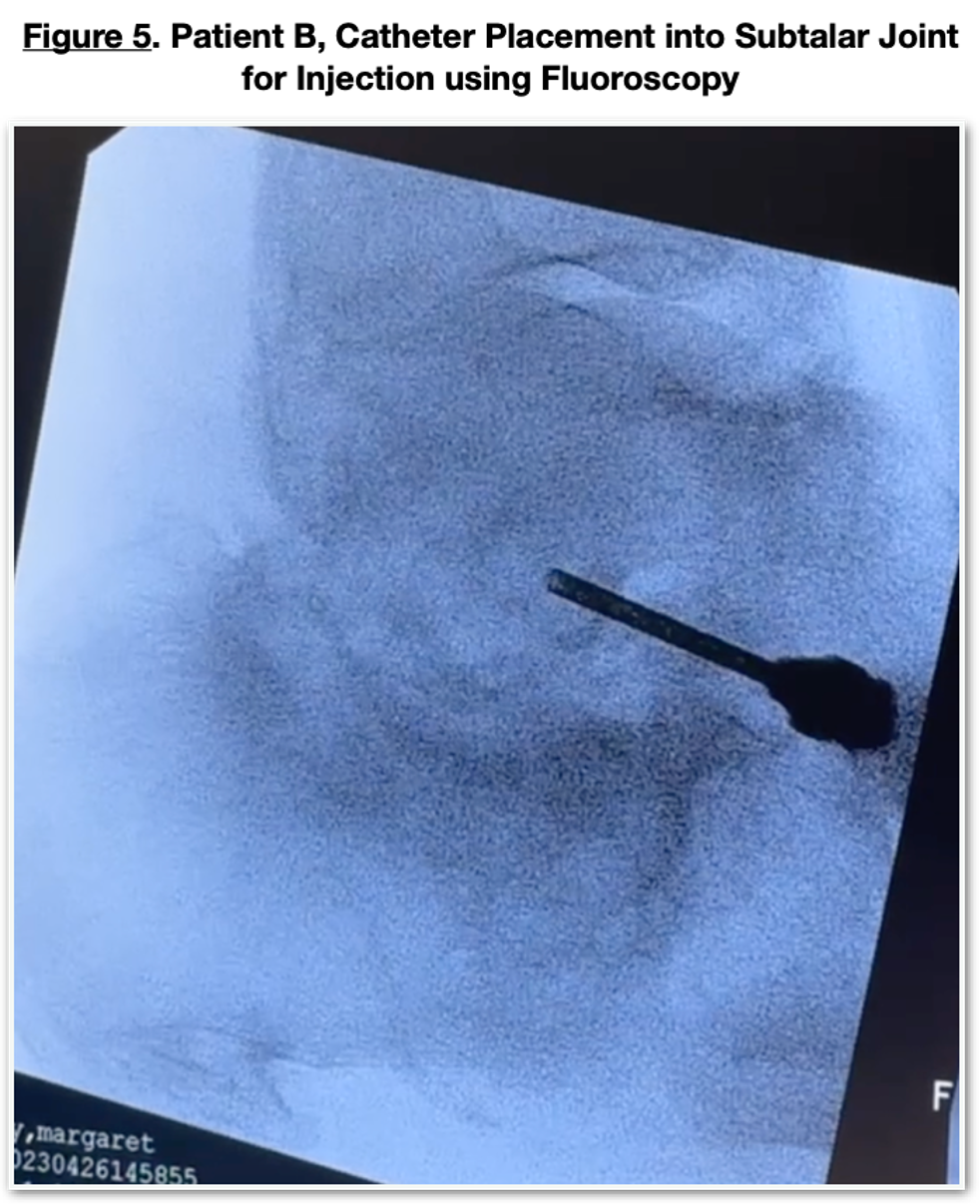
The patient underwent placental tissue injections (Figure 4) into the fracture areas, which were edematous, erythematous, and painful despite having neuropathy. Injections took place percutaneously with the assistance of fluoroscopy (Figure 5) into the anterior calcaneus, calcaneocuboid joint, subtalar joint, and posterior calcaneal body. Administration of these injections used a lateral approach with 2 percutaneous incisions. The patient was seen 2 weeks post-injection, with a significant decrease in erythema, calor, and minimal pain. Her C-reactive protein was 8 mg/dL. Six weeks later, X-rays revealed further calcification and consolidation. She then transferred to appropriate diabetic footwear and began full weight-bearing.

Patient C is a 72-year-old male with a BMI of 23. His past medical history included coronary artery disease (CAD), diabetes with neuropathy, hypertension, osteoarthritis, atrial fibrillation, hypothyroidism, hyperlipidemia, venous hypertension, and diabetic retinopathy. Medications included an insulin pump, levothyroxine, cetirizine, apixaban, calcium, vitamin D, flecainide, pravastatin, bumetanide, insulin aspart, and verapamil.
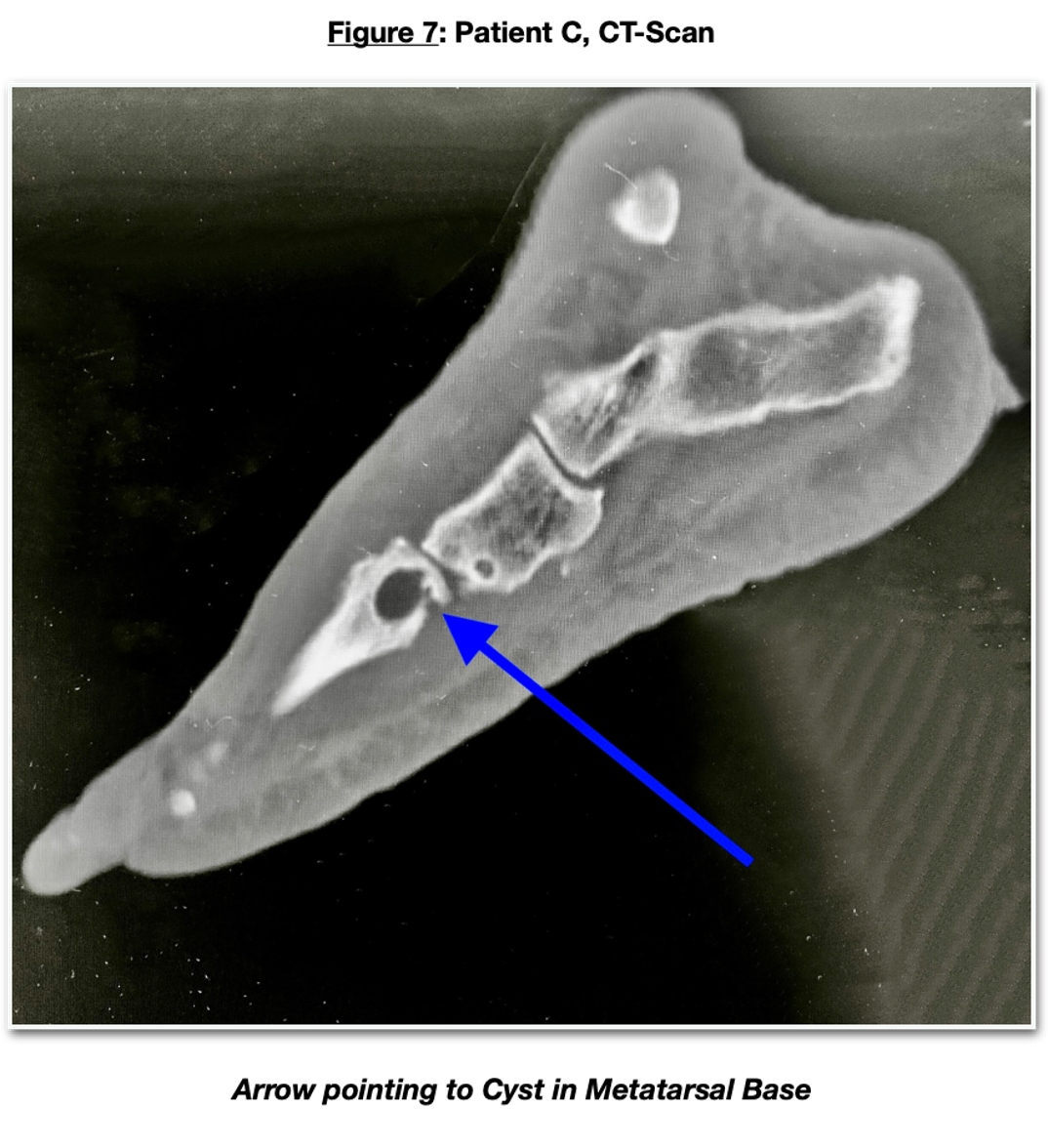
The patient presented to the office with a swollen, painful left midtarsal joint. X-rays (Figure 6) revealed numerous subchondral cysts with osteolysis at the lateral midtarsal joint consistent with an acute Charcot neuroarthropathy. CT confirmed the Charcot arthropathy showing multiple subchondral cysts (Figure 7) and subchondral edema. He was immobilized with a diabetic CAM boot. Follow-up X-rays revealed an increase in osteolysis and a slight lateral shift of the lateral column, indicating a progression of the acute neuroarthropathic process. He chose to have percutaneous placental tissue injections into the acute areas of the midfoot. This procedure was done under fluoroscopic guidance with placental cells injected into the metatarsal bases at the cystic and intercuneiform regions. He was immobilized with the CAM boot, and this area progressed uneventfully to a stable but arthritic construct. (Figure 8) The acute inflammatory component of the Charcot subsided within days of the injection.

Understanding the Treatment Pathway
Placental injections have been explored as a potential treatment option for chronic wounds due to their rich source of growth factors, cytokines, and other bioactive molecules that can aid tissue repair.4 Placental-derived products, such as amniotic membranes or amniotic fluid, contain factors that can modulate inflammation, promote angiogenesis, enhance cell proliferation, and support healing processes.
In my observation, these placental-derived products are typically applied topically to wounds or used as injectables. They have shown promising results in some cases, including improved wound healing, reduced inflammation, and enhanced tissue regeneration. The specific mechanisms of action are still under investigation. Still, it is believed that the presence of growth factors and other bioactive molecules in placental-derived products can stimulate the healing cascade and provide a supportive environment for chronic wound repair.5
A Closer Look at Historic Management
Historically, management of acute Charcot foot involves the patient being non-weight-bearing, having proper glycemic control, infection control, and occasionally reconstructive surgery. Several studies show that Charcot foot reconstruction surgery can significantly improve foot function, reduce ulceration, and decrease the need for amputation.6 It's important to note that this is a complex surgical procedure with inherent risks, including infection, nonunion, and the possible need for further surgeries.
In general, Charcot reconstruction surgery aims to stabilize and realign the affected foot to restore its function and reduce the risk of complications such as ulcers and deformities. The success rate of Charcot reconstruction surgery can vary depending on several factors, including the severity of the condition, the extent of bone and joint involvement, the overall health of the patient, and the specific surgical techniques employed. While there is no universally defined success rate for Charcot reconstruction surgery, studies have reported varying rates of success, ranging from 50% to 90%.7–10 Success is typically defined by achieving surgical goals, which include proper alignment, stability, improved foot function, and reduced risk of wound complications.
Examining the Role of Cytokines
The “cytokine storm” concept has been well-documented in neuroarthropathy, chronic wounds, and fractures.11,12 Inflammatory cytokines propagate the “hallmarks of inflammation”: edema, erythema, and pain. Combined with faulty biomechanics, the compounding detrimental effect on the foot and ankle may be catastrophic. Therefore, the management of inflammatory cytokines is imperative for normal tissue repair.
Cytokines can interfere with the normal bone healing process and contribute to delayed or impaired bone healing in several ways:
1. Excessive inflammation: While inflammation is a necessary part of the initial bone healing response, an excessive or prolonged inflammatory response can be detrimental. Pro-inflammatory cytokines, such as interleukin-1 (IL-1) and tumor necrosis factor-alpha (TNF-alpha), can lead to chronic inflammation that inhibits proper bone healing. Excessive inflammation can disrupt the delicate balance between bone resorption and formation, impair cell migration, and delay tissue repair.13
2. Imbalanced bone remodeling: Cytokines are critical in regulating the balance between bone resorption and formation during remodeling. However, an imbalance in cytokine signaling can disrupt this equilibrium. Suppose there is an excess of bone-resorbing cytokines or a deficiency in bone-forming cytokines. In that case, it can result in excessive bone resorption and reduced bone formation, leading to impaired healing.14
3. Dysregulated cell differentiation: Cytokines influence the differentiation of various cells involved in bone healing, such as mesenchymal stem cells (MSCs), osteoblasts, and osteoclasts. Imbalances in cytokine levels or abnormal signaling can disrupt these cells' proper differentiation and function. For example, an imbalance favoring osteoclast activation or inhibiting osteoblast activity can hinder bone formation and remodeling, impairing healing.15
4. Altered angiogenesis: Adequate blood supply is crucial for delivering oxygen, nutrients, and immune cells to the fracture site. Cytokines, such as vascular endothelial growth factor (VEGF), play a role in promoting angiogenesis. However, imbalances in cytokine levels can affect angiogenesis negatively, impairing the blood supply to the fracture site and compromising the healing process.16
The interplay of cytokines and other factors in bone healing is complex, and the effects can vary depending on the specific cytokine, its concentration, timing, and the injury context. The delicate balance of cytokines and their interactions are crucial for successful bone healing, and disruptions in this balance can contribute to delayed or impaired healing. Several cytokines can have detrimental effects on fracture healing.
Here are a few examples:
1. Interleukin-1 (IL-1): IL-1 is a pro-inflammatory cytokine inhibiting bone formation and promoting bone resorption. It can also stimulate the production of other pro-inflammatory cytokines, leading to an imbalance in the healing process.17
2. Tumor necrosis factor-alpha (TNF-alpha): TNF-alpha is another pro-inflammatory cytokine that can interfere with the normal bone healing process. It promotes the activation of osteoclasts, cells responsible for bone resorption, and can inhibit the formation of new bone tissue.18
3. Interleukin-6 (IL-6): IL-6 is involved in inflammatory and regenerative processes. While it has beneficial effects during the early stages of fracture healing, excessive or prolonged IL-6 production can disrupt the balance between bone resorption and formation, leading to impaired healing.19
4. Transforming growth factor-beta (TGF-beta): Although TGF-beta is generally known for its positive role in tissue repair, its excessive production can hinder fracture healing. High levels of TGF-beta can lead to abnormal bone formation, impairing the quality of the newly formed bone.20,21
In Summary
Cytokine interactions and their effects on fracture healing are complex, and the balance between pro-inflammatory and anti-inflammatory cytokines is crucial for successful bone repair. In my experience, managing the acute Charcot process by mediating cytokine dysregulation with placental tissue injections could be a “game changer” for patients who would otherwise undergo extensive surgery. Early intervention in treating acute neuroarthropathic fractures is imperative to prevent severe structural defects that frequently lead to ulcerations, infections, and amputations. Certainly, long-term evaluation of these patients will be helpful to see if the injection areas remain stable.
In addition, comparing the CT scans at various periods after the injection would be advantageous, but insurance restrictions limit this. The author acknowledges that these case studies represent a small sample size, but this study will be continued and results reported. However, it is worth noting that the author has injected over 50 patients without Charcot, but with various fractures, including nonunions and delayed unions, all with favorable results. This study will be submitted for publication in the near future. In my experience, these placental tissue injections are minimally invasive, well-tolerated options that could post cost efficiency benefits compared to the economical burdens of reconstruction or complications of Charcot arthropathy.
Dr. Weiss is a Fellow of the American College of Foot and Ankle Surgeons and practices at West End Foot and Ankle in Richmond, VA and the Weiss Institute for Regenerative Medicine. He is the Assistant Fellowship Director for the Virginia Fellowship in Reconstruction, Revision, and Limb Preservation.
References
1. Jeffcoate WJ, Game F, Cavanagh PR. The role of proinflammatory cytokines in the cause of neuropathic osteoarthropathy (acute Charcot foot) in diabetes. Lancet. 2005 Dec 10;366(9502):2058-61. doi: 10.1016/S0140-6736(05)67029-8. Epub 2005 Aug 10. PMID: 16338454.
2. Parolini O, Alviano F, Bergwerf I, et al. Toward cell therapy using placenta-derived cells: disease mechanisms, cell biology, preclinical studies, and regulatory aspects at the round table. Stem Cells Dev. 2010 Feb;19(2):143-54. doi: 10.1089/scd.2009.0404. PMID: 19947828.
3. Maruyama M, Rhee C, Utsunomiya T, Zhang N, Ueno M, Yao Z, Goodman SB. Modulation of the Inflammatory Response and Bone Healing. Front Endocrinol (Lausanne). 2020 Jun 11;11:386. doi: 10.3389/fendo.2020.00386. PMID: 32655495; PMCID: PMC7325942.
4. Choi JS, Kim JD, Yoon HS, Cho YW. Full-thickness skin wound healing using human placenta-derived extracellular matrix containing bioactive molecules. Tissue Eng Part A. 2013 Feb;19(3-4):329-39. doi 10.1089/ten.TEA.2011.0738. Epub 2012 Sep 24. PMID: 22891853; PMCID: PMC3542901.
5. Pogozhykh O, Prokopyuk V, Figueiredo C, Pogozhykh D. Placenta and placental derivatives in regenerative therapies: experimental studies, history, and prospects. Stem Cells Int. 2018 Jan 18;2018:4837930. doi 10.1155/2018/4837930. PMID: 29535770; PMCID: PMC5822788.
6. Ha J, Hester T, Foley R, et al. Charcot foot reconstruction outcomes: A systematic review. J Clin Orthop Trauma. 2020 May-Jun;11(3):357-368. doi: 10.1016/j.jcot.2020.03.025. Epub 2020 Apr 20. PMID: 32405193; PMCID: PMC7211810.
7. Wukich DK, Sung W. Charcot arthropathy of the foot and ankle: modern concepts and management review. J Diabetes Complications. 2009 Nov-Dec;23(6):409-26. doi: 10.1016/j.jdiacomp.2008.09.004. Epub 2008 Oct 17. PMID: 18930414.
8. Loyola University Health System. High success rate reported for diabetic Charcot foot surgery: Most patients are infection-free and able to walk normally, study finds. ScienceDaily. ScienceDaily, 14 December 2017.
9. Carrington AL, Mawdsley SK, Morley M, Kesteven P, Crisp AJ. Charcot foot. Br J Hosp Med. 2002; 63(3):115-118. doi: 10.12968/hmed.2002.63.3.2007
10. Rogers LC, Frykberg RG, Armstrong DG, et al. The Charcot foot in diabetes. J Am Podiatr Med Assoc. 2011 Sep-Oct;101(5):437-46. doi: 10.7547/1010437. PMID: 21957276.
11. Beloosesky Y, Hendel D, Weiss A, Hershkovitz A, Grinblat J, Pirotsky A, Barak V. Cytokines and C-reactive protein production in hip-fracture-operated elderly patients. J Gerontol A Biol Sci Med Sci. 2007 Apr;62(4):420-6. doi: 10.1093/gerona/62.4.420. PMID: 17452737.
12. DuBois K, Cates NK, Brandao R, Wynes J. Is an acute Charcot event a similar process to a cytokine storm? Podiatry Today. 2021; 34(10).
13. Zheng J, Yao Z, Xue L, Wang D, Tan Z. The role of immune cells in modulating chronic inflammation and osteonecrosis. Front Immunol. 2022 Dec 13;13:1064245. doi: 10.3389/fimmu.2022.1064245. PMID: 36582244; PMCID: PMC9792770.
14. Kitaura H, Marahleh A, Ohori F, et al. Osteocyte-related cytokines regulate osteoclast formation and bone resorption. Int J Mol Sci. 2020 Jul 21;21(14):5169. doi: 10.3390/ijms21145169. PMID: 32708317; PMCID: PMC7404053.
15. Feng X, McDonald JM. Disorders of bone remodeling. Annu Rev Pathol. 2011;6:121-45. doi: 10.1146/annurev-pathol-011110-130203. PMID: 20936937; PMCID: PMC3571087.
16. Niu G, Chen X. Vascular endothelial growth factor as an anti-angiogenic target for cancer therapy. Curr Drug Targets. 2010 Aug;11(8):1000-17. doi: 10.2174/138945010791591395. PMID: 20426765; PMCID: PMC3617502.
17. Seong S, Kim JH, Kim N. Pro-inflammatory cytokines modulating osteoclast differentiation and function. J Rheum Dis. 2016; 23(3):148-153.
18. Glass GE, Chan JK, Freidin A, Feldmann M, Horwood NJ, Nanchahal J. TNF-alpha promotes fracture repair by augmenting the recruitment and differentiation of muscle-derived stromal cells. Proc Natl Acad Sci U S A. 2011 Jan 25;108(4):1585-90. doi: 10.1073/pnas.1018501108. Epub 2011 Jan 5. PMID: 21209334; PMCID: PMC3029750.
19. Blanchard F, Duplomb L, Baud'huin M, Brounais B. The dual role of IL-6-type cytokines on bone remodeling and bone tumors. Cytokine Growth Factor Rev. 2009 Feb;20(1):19-28. doi: 10.1016/j.cytogfr.2008.11.004. Epub 2008 Nov 26. PMID: 19038573.
(FJ) URL=https://www.frontiersin.org/articles/10.3389/fendo.2020.00386
20. Xu X, Zheng L, Yuan Q, Zhen G, Crane JL, Zhou X, Cao X. Transforming growth factor-β in stem cells and tissue homeostasis. Bone Res. 2018 Jan 31;6:2. doi: 10.1038/s41413-017-0005-4. PMID: 29423331; PMCID: PMC5802812.
21. Chen G, Deng C, Li YP. TGF-β and BMP signaling in osteoblast differentiation and bone formation. Int J Biol Sci. 2012;8(2):272-88. doi: 10.7150/ijbs.2929. Epub 2012 Jan 21. PMID: 22298955; PMCID: PMC3269610.
Additional References
22. Trieb K. The Charcot foot: pathophysiology, diagnosis, and classification. Bone Joint J. 2016 Sep;98-B(9):1155-9. doi 10.1302/0301-620X.98B9.37038. PMID: 27587513.
23. Zhang JM, An J. Cytokines, inflammation, and pain. Int Anesthesiol Clin. 2007 Spring;45(2):27-37. doi: 10.1097/AIA.0b013e318034194e. PMID: 17426506; PMCID: PMC2785020.
24. Moudgil KD, Choubey D. Cytokines in autoimmunity: role in induction, regulation, and treatment. J Interferon Cytokine Res. 2011 Oct;31(10):695-703. doi: 10.1089/jir.2011.0065. Epub 2011 Sep 23. PMID: 21942420; PMCID: PMC3189547.
25. Kany S, Vollrath JT, Relja B. Cytokines in inflammatory disease. Int J Mol Sci. 2019 Nov 28;20(23):6008. doi: 10.3390/ijms20236008. PMID: 31795299; PMCID: PMC6929211.
26. Makhoul NM, Tarride JE, Inacio MC, Beaton DE, Dervin GF. The role of cytokines in delayed healing of orthopedic fractures: a systematic review. Bone Joint Research. 2016; 5(10):556-563. doi 10.1302/2046-3758.510.BJR-2016-0027.R1
27. Murthy MH, Pathak JL, Fox WC. Pathophysiology of delayed fracture healing. Clin Podiatr Med Surg. 2019; 36(2):143-152. doi 10.1016/j.cpm.2018.12.001
28.Riew KD, Wright NM, Cheng S, Avioli LV, Lou J. Induction of osteoblast activity by cytokine-stimulated human monocytes/macrophages: the relationship between the increased bone mineral density of hematopoietic malignancies and osteoinduction. Bone. 1998; 23(5):399-404. doi: 10.1016/S8756-3282(98)00115-7
29. Abbas AK, Lichtman AH, Pillai S. Basic Immunology: Functions and Disorders of the Immune System (5th ed.). Elsevier, 2017.
30. Dinarello CA. Overview of the interleukin-1 family of ligands and receptors. Semin Immunol. 2013 Dec 15;25(6):389-93. doi: 10.1016/j.smim.2013.10.001. Epub 2013 Nov 23. PMID: 24275600.
31. Marik PE, Flemmer M. The immune response to surgery and trauma: Implications for treatment. J Trauma Acute Care Surg. 2012 Oct;73(4):801-8. doi: 10.1097/TA.0b013e318265cf87. PMID: 22976420.
32. Hunter CA, Jones SA. IL-6 as a keystone cytokine in health and disease. Nat Immunol. 2015 May;16(5):448-57. doi: 10.1038/ni.3153. Erratum in: Nat Immunol. 2017 Oct 18;18(11):1271. PMID: 25898198.
33. Sinha S, Munichoodappa CS, Kozak GP. Neuro-arthropathy (Charcot joints) in diabetes mellitus (clinical study of 101 cases). Medicine (Baltimore). 1972 May;51(3):191-210. doi: 10.1097/00005792-197205000-00006. PMID: 5021769.
34. Armstrong DG, Todd WF, Lavery LA, Harkless LB, Bushman TR. The natural history of acute Charcot's arthropathy in a diabetic foot specialty clinic. Diabet Med. 1997 May;14(5):357-63. doi: 10.1002/(SICI)1096-9136(199705)14:5<357::AID-DIA341>3.0.CO;2-8. PMID: 9171250.