


Pertinent Perspectives on the Plantar Plate
Over the past 12 years, the plantar plate of the lesser metatarsophalangeal (MTP) joint has been the topic of numerous investigations and publications in both scientific and non-scientific lower extremity literature. Questions and debate remain, however, about this structure, its significance in lower extremity pathology, and the treatment of pain and problems associated with the plantar plate of the lesser MTP joint.
When I started my fellowship at the Weil Foot and Ankle Institute (WFAI), Dr. Weil, Jr., had recently published a new and innovative technique to repair the plantar plate through a dorsal incision and a Weil metatarsal osteotomy.1 This technique was technically challenging with a steep learning curve, but, once mastered, it became a reliable and reproducible method to correct plantar plate pathology.
At approximately the same time, WFAI fellow Wenjay Sung, DPM, had just finished his American College of Foot and Ankle Surgeons (ACFAS) grant study investigating the accuracy of a specific magnetic resonance imaging (MRI) protocol to identify plantar plate tears.2 The authors compared MRI findings to the intraoperative exam in patients who progressed to operative management of this condition. This groundbreaking study created confidence in this new MRI protocol and allowed the fellowship faculty at WFAI to further investigate the plantar plate in a way that was not previously possible. These physicians have since published studies on the clinical exam3, radiographic findings4,5, and ultrasound findings6,7 of plantar plate pathology. This research continued, comparing MRI accuracy to ultrasound accuracy for the diagnosis of plantar plate tears.8 Over time, these authors compiled a deep portfolio of research about surgical correction of the plantar plate.
While lecturing on this topic, we frequently encounter several questions based on our research and experience. In this piece, we will aim to address those key questions on this important pathology.
How Does One Define Lesser MTP Joint Instability and Why Is This Important?
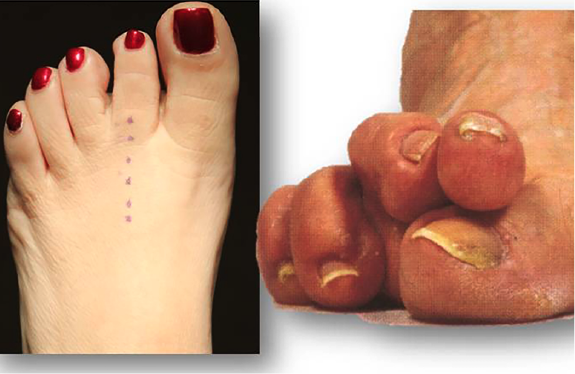
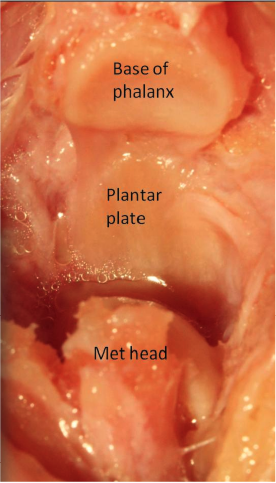
Most patients with lesser MTP joint instability/plantar plate pathology can present within a wide spectrum of pathology that ranges from a rectus foot with no obvious or notable deformity, to a positive drawer sign, or even a crossover toe where the second toe drifts medially and dorsally over the hallux.9 The most common presentation is chronic pain, likely unresolved for months to years.3,9,10 Early research identified that 95% of patients present with pain, edema, and a positive drawer sign at the affected MTP joint, while only 8% of patients present with a crossover toe deformity.3 The drawer sign is a vertical stress test that evaluates the integrity of the plantar plate.11 A positive test will exhibit increased vertical displacement and pain if there is compromise of plantar plate integrity.11 This pathology is important because disruption of the plantar plate can lead to pain, joint instability, deformity, dysfunction, and gait changes for our patient population.
What Are Some Nonsurgical Options for Plantar Plate Tears?
Not every patient is a surgical candidate. For this reason, there are nonsurgical treatment options for plantar plate tears. A good place to start is with their shoes. Patients need support throughout their day. Our experience shows that any patient with plantar plate pathology should be in sturdy, supportive, stiff shoes from the time they arise from bed in the morning until they get back into bed in the evening. Experience also shows that stiff-soled shoes that are adequately wide across the forefoot (eg, Hoka One One) can decrease the motion at the MTP joint, which may then help decrease pain. If the patient is unwilling or unable to wear gym shoes all day long, stiff-soled sandals (eg, Hoka slides or Oofos) with shock absorption can serve as house shoes.
In addition to shoes, one can use orthotics to decrease biomechanical abnormalities that may increase pressure on the second MTP joint. This can be accomplished with a second metatarsal head cutout or an appropriately placed metatarsal pad, in addition to whatever other customization patients require for their particular foot type and function.
Does Physical Therapy Help With Plantar Plate Pain?
Physical therapists that treat the foot (not just the ankle) are invaluable in treating patients with plantar plate pathology. The plantar plate is intimately intertwined with the intrinsic foot muscles and the plantar fascia. Accordingly, we find that a deep understanding of the anatomic and biomechanical features of this area is vital to a successful physical therapy collaboration.
The anatomy of the MTP joint is well-known, but in our observation, not well-applied to medical/surgical care of the lesser MTP joint. The long and short extensors have a more direct attachment to the base of the proximal phalanx via the extensor hood of the lesser MTP joint. This allows the extensors to have a more effective action (dorsiflexion) on the proximal phalanx. The plantarflexors, however, have an indirect attachment to the base of the proximal phalanx and act on the lesser MTP joint via the plantar fascia and the plantar plate. This means that, at their strongest, the action of the plantarflexors of the MTP joint may just not be as effective as the direct attachment/action of the dorsiflexors—particularly if there is any lack of integrity of the plantar fascia or the plantar plate.
From a gait perspective, the plantar plate, plantar fascia, and the plantarflexors assist in creating stability of the lesser MTP joint and creating a plantarflexory force that, during gait, is a major part of propulsion. Decreased strength in the direction of plantarflexion can create a relative instability of the lesser MTP joint and an apropulsive gait. A part of the propulsive phase of gait occurs when the MTP joints are at maximal dorsiflexion. If the plantar plate is torn/injured, then a part of the plantarflexory mechanism is not working and the strength of plantarflexion (which is also propulsion) will be significantly decreased. This allows a relative imbalance in which the dorsiflexors are stronger—accentuating any already existing dorsiflexory toe deformity. This situation is a positive feedback cycle that continues to get worse unless intervention (surgical or physical therapy) occurs.
Finally, the effect of the gastrocsoleal complex on forefoot pressure should be considered. Years ago, studies on diabetic forefoot ulcerations and equinus led to the innovative thought that lengthening the Achilles tendon decreased pressure on the forefoot, allowing forefoot ulcerations to better heal. In our observation, one may be able to extrapolate this to plantar plate pathology.
When combining each of these concepts, it is clear that there are physical medicine and physical therapy modalities that may be helpful for decreasing plantar plate pain.
We find that patients must have a full kinetic chain assessment. Hip weakness, core weakness, hip pathology, and knee pathology can all impact pain in the foot, and vice versa. A physical therapy plan that includes all relevant exercises or modalities may help the patient more than a physical therapy plan that focuses on just the foot.
Also in our experience, intrinsic strengthening of the foot muscles is a necessary rehabilitation technique to re-establish plantarflexory strength. This will assist with stability of the lesser MTP joint and, hopefully, get the patient back to a propulsive gait.
Finally, stretching of the gastrocsoleal complex is likely beneficial for this patient population if one identifies any decreased ankle joint motion. Accordingly, we find that pressures to the metatarsal heads/forefoot may lessen with increased ankle joint range of motion.
Do Biologic Injections Work on Plantar Plate Pathology?
The answer to this is unclear, as there are no current studies published on this specific topic to date. The plantar plate has been shown to have increased neovascularity in the presence of local pathology.12 This suggests that the plantar plate has reparative qualities and capacity. However, use of biologic injections has not yet been studied in plantar plate pathology. This is an avenue for future research.
Are There any Nonsurgical Treatments to Avoid?
Yes, our experience supports avoiding corticosteroid injections in and/or around the MTP joint, particularly when there is a known or suspected elongation of the second metatarsal. Although such injections may provide pain relief, the properties of the injected material can alter the biomechanical properties of the tissues in a way that decreases the forces needed to damage the plantar plate or dislocate the second MTP joint. It is believed that the injection of steroid into inflamed tissue suppresses inflammation, reduces or breaks up adhesions, prevents the production of certain types of collagen, and modulates the production of certain matrix molecules.
This should decrease and modulate locally derived pain.13 However, multiple studies identified that injecting steroids may cause the same inflammation that they are thought to reduce and there may be weakening in the tendon and ligamentous tissue, allowing patients to cause more damage without an increase in activity or trauma to the area.13
What About Avascular Necrosis of the Metatarsal Head?
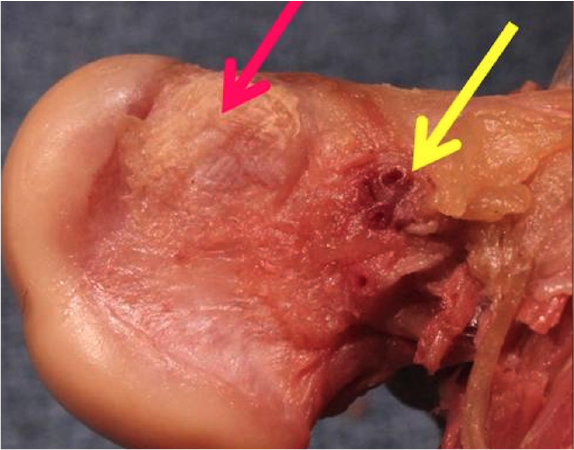
In our experience, avascular necrosis of the metatarsal head is an infrequent occurrence with surgical repair of the plantar plate. Complications do happen. However, if the surgeon dissects the collateral ligaments from the base of the proximal phalanx and not from the metatarsal head, the possibility of avascular necrosis may decrease. In Figure 3, it is very clear that there are nutrient arteries that enter the metatarsal at that level. Dissection of the collateral ligaments from the base of the proximal phalanx avoids manipulation of the tissues near those nutrient arteries.
Does the Plantar Plate Have Blood Flow? Can It Heal on Its Own?
This is a complicated question that does not, to date, have a clear-cut answer. The plantar plate is composed of collagen and has been compared to the meniscus of the knee and the rotator cuff in the shoulder. Both the meniscus and the rotator cuff do not necessarily anatomically heal on their own and frequently require surgical repair. However, there are patients who do well with physical therapy and may not have an anatomically healed meniscus or rotator cuff, but who are pain-free enough to function at an acceptable level for themselves.
Newer evidence would suggest, however, that the plantar plate does indeed have blood flow. Finney and team published a study in 2019 utilizing a novel technique with nano-computed tomography (CT) to image the plantar plate in 12 human adult cadavers.14 The anterior and posterior tibial arteries were injected with a barium solution and the soft tissues of each foot were counterstained with phosphomolybdic acid (PMA). The second through fourth MTP joints of 12 feet were imaged with a nano-CT at 14 micro-resolution. They found that the midsubstance of the plantar plate was relatively hypovascular. The vascular density increased consistently at the proximal 29% and the distal 22% of the plantar plate. This study identified that there is a vascular network extending from the surrounding soft tissues into the proximal and distal attachments of the plantar plate.14
Singer and colleagues continued this investigation by comparing intact plantar plates to torn plantar plates in 7 fresh frozen human cadaveric lower extremities with hammertoe and crossover toe deformities.12 There were 11 MTP joints with plantar plate tears and 35 MTP joints without plantar plate tears. It should be noted that a power analysis identified that this was a correct ratio to correctly power this study. The researchers used the same technique to image the vascularity of the plantar plate as Finney and team.14 At all segments imaged, there was significantly increased vascularity of the torn plantar plates when compared to the intact plantar plates. This analysis revealed that torn plantar plates exhibit neovascularization around the sites of plantar plate tears that does not exist in normal plantar plates. Clinically, the authors concluded that the increased vascularity may suggest that the plantar plate is a structure that is attempting to heal.12
Does Surgical Repair Work in the Lesser MTP Joint?
Yes. There is a growing body of evidence to suggest that repairing the plantar plate can decrease instability and pain at the lesser MTP joint.
The intermediate-to-long term patient-reported outcome study of the dorsal approach plantar plate repair followed 53 patients for a period of 10 years.15 Foot and ankle outcome scores (FAOS) were utilized as the primary patient reported outcome measure. At 2 years postoperative, FAOS scores were improved in 4 of 5 subscales. At 10 years postoperative, FAOS scores were improved in all 5 subscale scores. The authors concluded that the dorsal approach plantar plate repair was a safe procedure that improved patients’ pain, deformity and MTP joint instability.15
The largest study to date investigating the surgical efficacy of the direct plantar approach to plantar plate repair was that by Sharpe and colleagues.16 This study evaluated 204 plantar plate repairs in 185 patients. There were multiple types of plantar plate pathology included in this study—but all underwent an approach from the plantar aspect of the foot. There were 31 total complications (15%), which included 14 superficial infections (6.8%), 17 painful scars (8.3%), and 3 operations performed for subsequent repair of painful instability, but painful scarring (1.4%). Interestingly, this study specifically noted that there is a 9.8 times increased risk of superficial infection in tobacco users. This study also noted that there was not an increased risk of complications with ipsilateral procedures performed in the same surgical encounter.16
What Can Clinicians Conclude?
Overall, the literature suggests that repair of the plantar plate works to decrease instability of the MTP joint with low rates of complications.15,16 The results of these procedures are not perfect but they are promising with respect to patient satisfaction and pain relief.10,17 When examining common questions and debates such as those above, the literature provides important insights, and there are still opportunities to learn more in the future.
Dr. Klein is a Physician Owner and the Associate Director of Research at Weil Foot & Ankle Institute in Mount Prospect, Illinois. She is also a Clinical Instructor at the Dr. William M. Scholl College of Podiatric Medicine at Rosalind Franklin University of Medicine and Science.
Dr. Weil is the Executive Chairman of Balance Health/Weil Foot & Ankle Institute and the Founder of Foot and Ankle Business Innovations.
References
- Weil LJ, Sung W, Weil LS, Malinoski K. Anatomic plantar plate repair using the Weil metatarsal osteotomy approach. Foot Ankle Spec. 2011;4(3):145-150.
- Sung W, Weil LJ, Weil LS, Rofles R. Diagnosis of plantar plate injury by magnetic resonance imaging with reference to intraoperative findings. J Foot Ankle Surg. 2012; 51(5):570-574.
- Klein E, Weil LJ, Weil LS, Coughlin M, Knight J. Clinical examination of plantar plate abnormality: a diagnostic perspective. Foot Ankle Int. 2013;34(6):800-804.
- Klein E, Weil LJ, Weil LS, Knight J. The underlying osseous deformity in plantar plate tears: a radiographic analysis. Foot Ankle Spec. 2013;6(2):108-118.
- Fleischer A, Klein E, Ahmad M, et al. Association of abnormal metatarsal parabola with second metatarsophalangeal joint plantar plate pathology. Foot Ankle Int. 2017;38(3):289-297.
- Feuerstein C, Weil LJ, Weil LS, Klein E, Fleischer E, Argerakis N. Static versus dynamic musculoskeletal ultrasound for detection of plantar plate pathology. Foot Ankle Spec. 2014;7(4):259-265.
- Klein E, Weil LJ, Weil LS, Knight J. Musculoskeletal ultrasound for preoperative imaging of the plantar plate: a prospective analysis. Foot Ankle Spec. 2013;6(3):196-200.
- Klein E, Weil LJ, Weil LS, Knight J. Magnetic resonance imaging versus musculoskeletal ultrasound for identification and localization of plantar plate tears. Foot Ankle Spec. 2012;5(6):359-365.
- Hyer C, Consul D, McAlister J, Cottom J. Lesser metatarsophalangeal plantar plate repair. Clin Pod Med Surg. 2022;39(2):167-185.
- Akoh C, Phisitkul P. Plantar plate injury and angular toe deformity. Foot Ankle Clin. 2018;23(4):703-713.
- Thompson F, Hamilton W. Problems of the second metatarsophalangeal joint. Orthopedics. 1987;10:83-89.
- Singer N, Saunders N, Holmes J, et al. Presence of neovascularization in torn plantar plates of the lesser metatarsophalangeal joints. Foot Ankle Int. 2021;42(7):944-951.
- Paavola M, Kannus P, Jarvinen T, Jarvinen T, Jozsa L, Jarvinen M Treatment of tendon disorders. Is there a role for corticosteroid injection? Foot Ankle Clin. 2002;7(3):501-513.
- Finney F, McPheters A, Singer N, et al. Microvasculature of the plantar plate using nano-computed tomography. Foot Ankle Int. 2019;40(4):457-464.
- Klein E, Weil LJ, Baker J, Langer S, Fleischer A. Patient reported outcome of dorsal approach plantar plate repair – a ten year follow up. J Foot Ankle Surg.
- Sharpe B, Edaugh M, Philbin T, et al. Direct plantar approach to plantar plate repair and associated wound complications. Foot Ankle Spec. 2022:19386400221118500.
- Jastifer J. Plantar plate repair for metatarsophalangeal joint instability of the lesser toes. Orthop Clin North Am. 2022;53(3):349-359.






