The Relationship Between Venous Insufficiency and the Diabetic Foot: It's Complicated
Venous insufficiency and the diabetic foot: is there a link? Let’s just say the relationship is “complicated.” This article will explore the overlapping pathophysiological processes of glucose toxicity, diabetic neuropathy and venous insufficiency and introduce an updated diabetic foot ulcer (DFU) care algorithm.
The Basics of Diabetes and Glucose Toxicity
Contributing fuel for cellular processes, dietary glucose primarily comes from complex and simple carbohydrate sources. The body digests complex carbs slower to supply a steadier energy source, making them the healthier option.1 During the process of glycolysis, glucose from food breaks down through the Krebs cycle, an aerobic process that uses oxygen to break down sugar, culminating in the synthesis of adenosine triphosphate (ATP).2 This process, called cellular respiration, occurs in the mitochondria of a cell. ATP is the body’s energy currency and is consumed in multiple ways.
The hormone insulin is required for cellular uptake of glucose and plays a crucial role in glucose homeostasis. After eating, the body signals the pancreas to release insulin to manage the rising blood glucose level. Cells will absorb and utilize glucose according to their specific needs and function.3 In humans, glucose is carried throughout the body in the blood, with normal levels of 70–110mg/dL. Regulation of blood glucose occurs by maintaining a balance between sources (diet) and removal (glycolysis, glycogenesis, urinary system).
Type 1 and Type 2 diabetes have different pathophysiologies. In Type 1 diabetes, the immune system destroys pancreatic beta cells, thus limiting the organ’s ability to secrete insulin.3 Type 2 diabetes results when pancreatic beta cells cannot manufacture enough insulin to meet metabolic requirements.3 Hyperglycemia, inflammation, obesity and other factors can play a role in the development of insulin resistance.4 Insulin resistance stimulates the pancreas to produce more insulin, with overstimulation leading to beta cell burnout. Consequently, elevated blood glucose levels persist.4 Chronic hyperglycemia leads to glucose toxicity and cell damage.
Glucose toxicity occurs readily in capillary endothelial cells commonly seen in the retina, renal glomerulus, and neurons of the peripheral nerves resulting in retinopathy, nephropathy, and neuropathy. An estimated 50% of patients with diabetes will be affected by neuropathy.4 As neural glucose levels rise, neuronal damage occurs due to glucose neurotoxicity, with multiple existing theories on mechanism of action. Of note, glucose toxicity can also result in parasympathetic nerve damage causing dysregulation of the vasomotor response. The result is loss of control of the diameter of blood vessels, thus vasoconstriction will not occur to counter gravity. Venous hypertension and engorgement of the superficial venous system will ensue.5 Peripheral polyneuropathy is the key contributing factor in the pathways to foot ulceration published by the American Diabetes Association.6
What You Should Know About Venous Insufficiency
The common etiology of venous insufficiency is the reversal of blood flow from the deep venous system to the superficial venous system, which causes pooling of the blood and fluid in the legs.7 The first sign of disease may be lower extremity edema. Hallmark trophic changes in the tissues will appear over time, including hyperpigmentation, venous stasis dermatitis, hemosiderin deposits, loss of hair, thickened nails, atrophy blanche and lipodermatosclerosis. These changes can cause skin breakdown leading to ulceration. Venous leg ulcers (VLUs) usually arise in the medial gaiter region of the lower leg. This corresponds to the position of the perforating veins connecting the superficial and deep systems.
There are several competing theories to describe the progression from chronic venous hypertension to skin breakdown and ulceration. One popular hypothesis is that hypertension in the venous system leads to the development of a pericapillary fibrin cuff that forms a barrier to oxygen diffusion.8 As a result, the skin and subcutaneous tissue become hypoxic and subsequently ulcerate. The final common pathway for all the theories is tissue ischemia: another theory suggests that white cells plug the capillaries causing tissue hypoxia.9
A more recent theory of ulcer pathogenesis suggests that skin breakdown results from increased inflammation brought on by a cycle of chronic ischemia-reperfusion.10 Neutrophils, activated by repeated ischemia-reperfusion, release oxygen-derived free radicals which stimulate the formation of capillary cuffs that impair oxygenation and trap more neutrophils. This creates a vicious cycle of inflammation. Eventually the repeated activation of this cascade overwhelms the body’s compensatory capacity and the balance tips toward tissue destruction.10 In many cases the immediate cause of the ulceration is a traumatic event; however, healing is disrupted by one or a combination of factors described above. Correcting the underlying venous hypertension is the crux of VLU treatment.
Additionally, with venous insufficiency, the lymphatic system will fail to effectively clear inflammatory fluids from the tissues. Fluid overload leads to amplification of the immune response and increases inflammation.11 Common symptoms include aching or heavy-feeling legs; difficult movements; hard, tight skin; folds developing in the skin; wart-like growths of the skin, and fluid leakage through the skin.
Fibrosis of the endothelium and other tissues occur leading to skin breakdown and necrosis, and eventually ulcerations can develop if venous insufficiency is not properly managed. This condition is called phlebolymphedema.11 It is often undiagnosed and is increasingly thought to be a factor in non-healing chronic wounds.11
Linking Diabetes and Venous Insufficiency
What do we know about venous disease in the diabetic neuropathic foot? Clinicians have begun to question the prevalence of venous incompetence in the diabetic population and new clinical evidence is mounting. Mani and colleagues investigated the prevalence of venous incompetence, impaired calf vein hemodynamics, and loss of microvascular control in the skin over the dorsum of the foot in patients with and without diabetes.5 The investigators found significantly higher levels of venous incompetence in the diabetic study cohort along with venous hemodynamic and morphologic changes.
The results of this study lead me to wonder: If these hemodynamic changes can be controlled early in the disease process, can the number of diabetic foot ulcers be decreased? Let’s take a deeper dive.
Microcirculation is the terminal vascular network of the circulatory system comprised of arterioles, post-capillary venules, and capillaries. The functions of microcirculation include oxygen transfer, regulation of solute exchange between the intravascular and tissue space, and the exchange of nutrients to the tissue.12 Microcirculation is arguably the most important compartment of the cardiovascular system. Impaired microcirculation of the foot is commonly seen in patients with diabetes. A myriad of biochemical pathways has been implicated as contributing factors of this microcirculation impairment.13
Secondary to sympathetic denervation, the diabetic foot is often unable to mount a vasodilatory response under conditions of stress making it functionally ischemic even in the presence of satisfactory blood flow.13 Conversely, resting blood flow can increase in the feet of patients with diabetic neuropathy resulting in warm skin, bounding pulses, and venous distension.13 Venous engorgement increases fluid filtration and causes edema to form in the foot tissue.
Microcirculation vessels are almost entirely lined by endothelial cells. One of the most important subcellular structures mediating the function of the endothelium is the glycocalyx present on the luminal side of the endothelium.12 The glycocalyx serves several critical functions:
- Acts a reservoir for antithrombotic factors to prevent clotting
- Regulates production of nitric oxide (NO)
- Modulate the permeability of macromolecules
- Modulates leukocyte adhesion
Chronic hyperglycemia as seen in patients with diabetes causes thinning of the glycocalyx. In response to hyperglycemia the thickness of the glycocalyx is reduced leading to loss of the critical functions of the blood vessel endothelia. This increased permeability and fluid leakage into the immediate surrounding tissue also causes edema of the foot, increased leukocyte adhesion, and the release of cytokines resulting in an inflammatory environment. Chronic inflammation causes further impairment of vascular endothelial cells and impedes neovascularization and tissue regeneration. Fibroblast migration, proliferation, and function are also affected by this cytokine-rich environment, thus contributing to tissue breakdown and acting as barriers to tissue repair and wound healing.
Introducing an Updated DFU Care Algorithm
Using the information from literature reviews along with the author’s clinical experience, an updated easy-to-use DFU care algorithm was established (Figure 1).
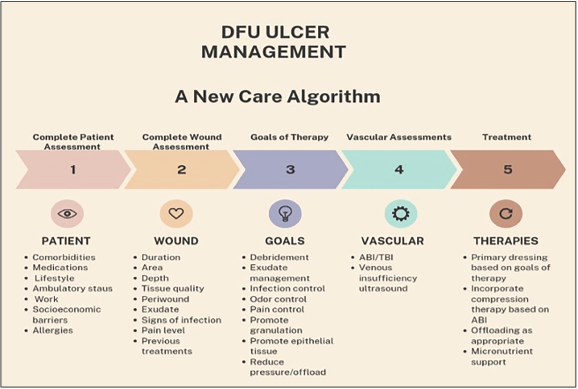
The initial essential steps of wound management include an in-depth evaluation of the individual patient. This process includes collecting all the pertinent information needed to create a treatment plan to optimize the wound environment so healing progresses in a timely fashion.
Step 1. Thorough patient assessment should be performed to identify any underlying disease states, such as diabetes, autoimmune disorders, vascular impairment, inflammatory conditions, anemia, kidney disease, history of radiation therapy, and malignancy—known factors contributing to wound chronicity. These conditions often result in impaired collagen, impairment of angiogenesis, delayed infiltration of inflammatory cells, macrophages, and lymphocytes due to decreased host resistance, and poor cutaneous or epidermal vasculature.14 Obtain current medications and dosage schedules at this stage. Non-steroidal anti-inflammatory drugs (NSAIDs), chemotherapy, immunosuppressive drugs, and corticosteroids are just a few agents known to disrupt the healing cascade.14
Step 2. Detailed wound assessment should include wound duration, etiology, amount of tissue loss, appearance of the wound bed, measurements, exudate amount and quality, clinical signs of infection, pain level, and history of previous treatments.
A high level of care is provided in steps 1 and 2, which includes patient and caregiver education about barriers to wound healing such as proper nutrition, exercise, pressure relief, and smoking cessation.
Step 3. Establishing treatment goals of the clinician and the patient occurs here. Clinician goals may include infection control, debridement, granulation tissue augmentation, and epithelialization. Patient goals and concerns are also vital. Exudate management, pain control, odor control, and mobility are common patient concerns for my patients with chronic wounds. Merging the provider’s knowledge and expertise with the patient’s goals to produce shared decision making on treatment options and care plans can support patient-centered outcomes, improve overall care satisfaction, and also potentially reduce health care expenditures.
Step 4. One can perform vascular screening tests including ankle brachial index/toe brachial index (ABI/TBI) and, in addition, venous competency ultrasound to evaluate both superficial and deep venous anatomy for valvular reflux and venous insufficiency.
Step 5. Choosing the best therapies:
- Dressing selection: The appropriate dressing can have a significant effect on the rate and quality of healing, minimize bacterial contamination, and manage exudate and pain associated with wound care. Selecting the appropriate dressings should always be based on mechanism of action and scientific evidence.
- Edema control: Providers should appropriately apply compression/2-layer systems to control the interstitial edema and lymphedema. Alternatively, a fuzzy wale compression stockinette can be employed to improve microvascular perfusion and lymphatic drainage. Please note compression therapies should be used with caution prior to treating underlying peripheral arterial disease (PAD).
- Offloading: Plantar surface DFUs often form as a direct result of increased pressure in the presence of neuropathy. Elimination of repetitive stresses and decreasing plantar pressures must be achieved to have any success in wound healing. Common methods to offload the foot include bed rest, wheelchair, crutch-assisted gait, total contact casts, felted foam, half shoes, therapeutic shoes, and removable cast walkers.
- Nutritional support: Proper nutrition is something that every wound care clinician should discuss with their patients. Caloric needs increase during wound healing and it is estimated that patients should consume 30–35kcal/kg daily.15 Macronutrients such as proteins, fats, and carbohydrates have been shown to play a vital role in wound healing.15 Additionally, naturally occurring flavonoids are dietary supplements that have been shown to helpful in the prevention and management of diabetes complications.16 Flavonoids have been shown to improve glucose metabolism, improve lipid profiles, regulate hormones and enzymes, protect against neuropathy, and are cardioprotective.16
In Conclusion
While diabetes mellitus does not directly cause venous insufficiency there is an undeniable venous component contributing to the complexity of the diabetic foot. The effects of chronic hyperglycemia are seen throughout the tissues of the lower extremities including the venous system. When diagnosed together, these disease states can have an overwhelming negative effect. Clinicians should be cognizant of the effects of glucose toxicity on all tissues including those of the lower extremity. Evaluating all patients with diabetes for subtle signs of venous pathology and implementing preventative measures such as compression therapy could have a positive impact and decrease the rate of DFU formation. It is the authors’ opinion that implementation of the updated evidence based DFU care algorithm presented in this article will decrease the incidence of chronic non-healing wounds of the at-risk diabetic foot.
Windy Cole, DPM is an Adjunct Professor and Director of Wound Care Research at Kent State University College of Podiatric Medicine. She is board certified by the American Board of Foot and Ankle Surgery and the American Board of Wound Management. Cole is a member of the American College of Clinical Wound Specialists Board of Directors. Additionally, she holds multiple advisory and editorial positions with various medical and wound care publications, and sits on the advisory board of multiple emerging biotech companies and has been integral in collaborating on innovative research protocols in the space.
References
- American Heart Association. Carbohydrates. Accessed October 16, 2023.
- Dunn J, Grider MH. Physiology, Adenosine Triphosphate. In: StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK553175/
- Nakrani MN, Wineland RH, Anjum F. Physiology, Glucose Metabolism. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. https://www.ncbi.nlm.nih.gov/books/NBK560599/
- Giri B, Dey S. Chronic hyperglycemia mediated physiological alteration and metabolic distortion leads to organ dysfunction, infection, cancer progression and other pathophysiological consequences: An update on glucose toxicity. Biomed Pharmacother. 2018;306-328.
- Mani R, Yarde S, Edmonds M. Prevalence of deep venous incompetence and microvascular abnormalities in patients with diabetes mellitus. Int J Low Extrem Wounds. 2011;10(2):75-79.
- Boulton AJM, Armstrong DG, Kirsner RS, et al. Diagnosis and Management of Diabetic Foot Complications. Arlington (VA): American Diabetes Association; 2018.
- Olivencia JF. Pathophysiology of venous ulcers: surgical implications, review and update. Dermatol Surg. 1999; 25(11):880-885.
- Browse NL. Venous ulceration. BMJ. 1983; 286(6382):1920-1922.
- Coleridge Smith PD, Thomas P, Scurr JH, Dormandy JA. Causes of venous ulceration: a new hypothesis. BMJ. 1988;296(6638):1726-1727.
- Falanga V. The “trap” hypothesis of the venous ulceration. Lancet. 1993; 341(8851):1006-1008.
- Farrow W. Phlebolymphedema-a common underdiagnosed and undertreated problem in the wound care clinic. J Am Col Certif Wound Spec. 2010;2(1):14-23.
- Guven G, Hilty MP, Ince C. Microcirculation: physiology, pathophysiology, and clinical application. Blood Purif. 2020;49(1-2):143-150.
- Dinh T, Veves A. Microcirculation of the diabetic foot. Curr Pharm Des. 2005;11(18):2301-2309.
- Cole W. Wound Management: setting the stage. Wound Manage Prevention. 2022; 68(10):3-5.
- Quain A, Khardori N. Nutrition in wound care management: a comprehensive overview. Wounds. 2015;27(12):327-335.
- Testa R, Bonfigli AR, Genovese S, De Nigris V, Ceriello A. The possible role of flavonoids in the prevention of diabetic complications. Nutrients. 2016;8(5):310.