


Beyond Wound Care: The Role of Social Determinants on Patient Outcomes
 Wounds develop due to a variety of factors. Acute wounds can result from trauma, surgery, or thermal injuries. At the same time, chronic wounds often develop complications from extrinsic factors such as pressure and shear or systemic disease conditions such as diabetes, venous insufficiency, and peripheral arterial disease (PAD). No matter the cause, wounds can have a considerable effect on the patient and the health care economy alike. Estimates contend that approximately 2 percent of the US population (greater than 6.5 million individuals) is affected by chronic wounds.1 These patients often suffer from pain, isolation, depression, loss of mobility, inability to work, and loss of autonomy. Increased hospitalization, as well as greater morbidity and mortality, further complicate the overall human toll.
Wounds develop due to a variety of factors. Acute wounds can result from trauma, surgery, or thermal injuries. At the same time, chronic wounds often develop complications from extrinsic factors such as pressure and shear or systemic disease conditions such as diabetes, venous insufficiency, and peripheral arterial disease (PAD). No matter the cause, wounds can have a considerable effect on the patient and the health care economy alike. Estimates contend that approximately 2 percent of the US population (greater than 6.5 million individuals) is affected by chronic wounds.1 These patients often suffer from pain, isolation, depression, loss of mobility, inability to work, and loss of autonomy. Increased hospitalization, as well as greater morbidity and mortality, further complicate the overall human toll.
Successful wound management requires the implementation of best clinical practices to overcome barriers to wound healing. Identifying and addressing factors that impact this process is essential in providing optimal patient care. Barriers to wound healing can be both clinical and patient-related.
Clinical factors affecting wound healing, in the author’s experience, include:
- Wound location/site
- Duration
- Size
- Tissue health
- Exudate amount
- Perfusion
- Infection
- Nutrition
- Medications
- Comorbid conditions
Patient-related factors affecting wound healing, in the author’s experience, include:
- Age
- Gender
- Race
- Culture
- Religious beliefs
- Education
- Access to care
- Adherence
- Social support network
- Ability to self-care
Published evidence on wound management heavily focuses on addressing pathophysiological factors affecting wound healing. Historically, there has been little focus on overcoming patient-related considerations. More recently, in a push to positively impact wound healing outcomes, there is increased attention directed towards developing ways clinicians can support patients and help overcome health care disparities. Despite advances and improvements in the health of US citizens, health care disparities remain. This article aims to shed light on how health care disparities affect wound care outcomes and highlight ways providers can support efforts to achieve health care equity.
Defining Health Care Disparity

A health care disparity exists when there is a higher burden of illness or injury experienced by one group compared to another.2 Race or ethnicity, gender, gender identity, education, age, disability, and geographic location all have an impact on health care outcomes.2 Health disparities often have a link to social and economic factors. Gaps in health insurance coverage, restricted access to care, and decreased medical service quality are all contributing factors—the more significant the disparity, the worse the health care outcome.
Inequities in health care exist when there are variations in the distribution of resources based on a population’s geographic location that contribute to the lack of opportunity and lead to unavoidable differences in health outcomes.3 The World Health Organization reports that the highest proportions of the global burden of disease and disability fall on regions that also suffer the most significantly from physician shortages.4 How do we, as wound care clinicians, bridge these gaps to produce the best healing outcomes? Understanding the contributing factors involved in developing disparities in health care will help providers ensure that their practice incorporates patient engagement strategies to minimize inequalities in care.
How Social Determinants Impact Health Care Outcomes
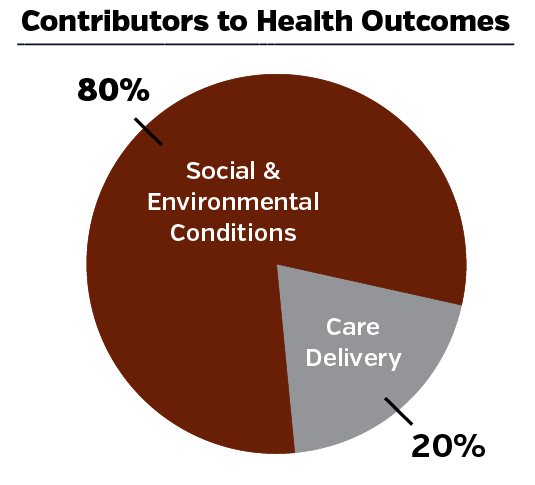
The social and environmental conditions in which people are born, grow, live, work, and age account for 80 percent of health outcomes, while only 20 percent result from care delivery.5 Socioeconomic status (SES) is one of the most well-recorded predictors of health care outcomes. Higher incomes generally allow for acquiring health insurance, access to doctors and hospitals, healthy food sources, and exercise programs. Conversely, studies have shown that lower socioeconomic groups are 3-4 times more likely to partake in activities that negatively affect their health outcomes than those with higher SES.6 Education can significantly impact a patient’s overall health status. A comparative study examined the overall mortality risk in people with only a high school degree versus those with a college education.7 The investigators concluded that having a college degree translated into half the mortality risk and essentially was the equivalent to being eight years younger.7 Patients with diabetes and lower education levels record higher rates of missed visits and non-adherence to treatment regimens.8

Community influences are integral to a patient’s health and overall wellbeing. Care is not always equitably provided in all neighborhoods. Access to specialists may be limited in some regions of the country. One should not overlook cultural considerations in diverse populations. Health care barriers in minority populations include lack of knowledge or understanding of health care screening or treatment options, language barriers, alternative beliefs, lack of culturally appropriate materials, mistrust of the health care system, and generalized fear.9 Having a strong social support network has also shown to have an impact on one’s overall health. Socially connected adults also live longer and healthier lives than their socially secluded peers.10
Mortality rates in rural areas of the US have exceeded those in urban areas since the 1980s, and the gap continues to widen.11 US life expectancy has also been found to be lower in rural versus urban areas.11 Although there is no pinpointed definitive cause of these differences, suggestions exist that social determinants of health such as income, education, unemployment, insurance coverage, and race/ethnicity are at play.11 Of note, primary care physician supply has steadily decreased from 2005–2016 in rural areas of the US.12 Patients residing in low-income environments exhibit an increased risk for cardiovascular disease, diabetes, cancer, hypertension, and higher overall mortality.13
Crucial Considerations in the Wound Care Patient
It is particularly important to consider social determinants of health in the at-risk chronic wound patient population. Many of our wound care patients are of advanced age and have multiple comorbid systemic conditions such as diabetes and PAD. Most patients suffering from chronic wounds seek help from hospitals or specialty clinics. Issues arising from transportation limitations, difficult topography, budget constraints, conflicting cultural ideology, lack of insurance, or a paucity of local health care providers in certain areas are a few barriers to wound healing our patients may encounter.
Transportation to and from hospital or doctors’ appointments can be costly, especially for patients living in rural areas. Patients may feel they are a burden to friends and family members and may choose not to impose on them for a ride. Patients in isolated communities may have limited access to wound care treatments and dressings. The author’s experience is that these patients tend to rely on folk treatments or home remedies to treat injuries. Cultural and religious beliefs and traditions also may play a role. Certain groups may not believe in many modern-day medical practices, such as skin graft substitutes or other animal-derived products. Health care providers must be aware of these traditions and respect these beliefs.
Preventive care practices such as smoking cessation, foot examinations, and annual checkups can prevent or delay the incidence and progression of diabetes-related complications. An investigation into patient practices stratified by social class determined that persons of lower social status with no insurance are at greater risk of not receiving preventative services. Health care coverage was strongly associated with all the preventive care practices.14 Persons with no health care coverage were twice as likely to have not visited the doctor in the previous year and 1.5 times more likely to have not had a foot exam.14 Persons without health care coverage also had a 30 percent increased smoking prevalence.14 These strong patterns further illustrated the disparity in socioeconomic status and the severity of chronic illness.
Diabetic foot ulcers have a higher rate of emergency room visits and hospitalizations than congestive heart failure, renal disease, depression, and most forms of cancer.15 In an attempt to illustrate that the consequences of developing a diabetic foot infection (DFI) are not homogenous throughout the diabetic population, one study evaluated the hospitalization outcomes of White, African American, and non–African American minorities (Hispanics and Native Americans).16 This study examined the records of 150,701 patients admitted for DFI, including 98,361 Whites, 24,583 African Americans (AAs), 24,472 Hispanics, and 1,654 Native Americans (NAs).16 The study found that the risk for major amputation was significantly higher for African American, Hispanic, and Native American patients with diabetic foot infections than their White counterparts.16 The study concluded that more action is necessary to mitigate racial and ethnic disparities to further promote equity in the treatment outcome in the at-risk diabetic patient population.
Moreover, African American and Hispanic patients with PAD were more likely to undergo a primary amputation without any attempt at revascularization.16 Minority patients are 2 to 3 times less likely to receive any endovascular procedure than Whites.16 These findings suggest that there appears to be reduced access to medical care or vascular intervention procedures. Increasing patient access to professional wound management services for the treatment and prevention of wound deterioration is crucial.
Addressing Health Care Disparities
Understanding the continuum of care in the context of health care disparities is essential to developing best practices and new policies to help close these gaps. Increasing awareness about health care disparities will strengthen all aspects of the delivery system. The Commission to End Health Care Disparities issued a guidance document outlining ways providers can help eliminate health care disparities.17
The 10 key principles include:17
- Relationship-centered care that includes the patient, the family, and the community
- Culturally and linguistically appropriate strategies and educational materials
- Targeted focus on recognizing gaps in health care
- Data-driven results
- Transparent, participatory, and collaborative practices to increase engagement of all constituency groups
- Both long and short-term plans to resolve underlying causes of disparities
- Comprehensive policies must be broad-based
- Judicious use of incentives and requirements for implementation of best practices
- Fiscally responsible bipartisan participation of all involved
- Continuous monitoring of health care outcomes in order to make appropriate adjustments
With the recent shift towards payment for performance incentives, the impetus is on improving the quality of care to reduce costs. The utilization of health care services is often disjointed in areas where health care disparities persist, thus resulting in inefficiency and poor outcomes. Awareness of health care disparities and implementation of the above-mentioned key principles will allow clinicians to make mindful adjustments to their care. Considerations of race, ethnicity, socioeconomic status, religious beliefs, and other factors will produce the best care plans for a diverse population. Chronic wounds have a significant impact on quality of life and are a drain on the health care system. The number of patients suffering from chronic wounds is increasing. Implementing these strategies will help health care providers make the best use of resources to produce the greatest long-term results for each patient in need.
Dr. Cole is an Adjunct Professor and Director of Wound Care Research at Kent State University College of Podiatric Medicine. She is the National Director of Clinical Safety Quality and Education for Woundtech.
References
1. Järbrink K, Ni G, Sönnergren H, et al. The humanistic and economic burden of chronic wounds: a protocol for a systematic review. Syst Rev. 2017;6(1):15.
2. Office of Disease Prevention and Health Promotion. Healthy People 2020. Available at: https://www.healthypeople.gov/2020/ . Accessed June 20, 2022.
3. WHO. Health inequities and their causes. Available at: https://www.who.int/news-room/facts-in-pictures/detail/health-inequities-and-their-causes . Published February 22, 2018. Accessed July 11, 2022.
4. WHO. Disability and health. Available at: https://www.who.int/news-room/fact-sheets/detail/disability-and-health . Published November 24, 2021. Accessed July 11, 2022.
5. Magnan S. Social determinants of health 101 for health care: five plus five. National Academy of Medicine. Available at: https://nam.edu/social-determinants-of-health-101-for-health-care-five-plus-five/ . Published October 9, 2017. Accessed June 22, 2022.
6. Chety R, Stepner M, Abraham S, et al. The association between income and life expectancy in the United States, 2001-2014. JAMA. 2016;315(16):1750-1766.
7. Meara ER, Richards S, Cutler DM. The gap gets bigger: changes in mortality and life expectancy, by education, 1981–2000. Health Affairs. 2008;27(2):350-360.
8. Bachmann MO, Eachus J, Hopper CD, et al. Socioeconomic inequalities in diabetes complications, control, attitudes and health service use: a cross-sectional study. Diab Med. 2003;20(11):921-929.
9. Wolff M, Bates T, Beck B, Young S, Ahmed SM, Maurana C. Cancer prevention in underserved African American communities: barriers and effective strategies--a review of the literature. WMJ. 2003;102(5):36-40.
10. Umberson D, Karas Montez, J. Social relaionships and health: A flashpoint for health policy. J Health Social Behav. 2010;51(1_suppl):S54-S66
11. Gong G, Phillips SG, Hudson C, Curti D, Philips BU. Higher US rural mortality rates linked to socioeconomic status, physician shortages, and lack of health insurance. Health Aff (Millwood). 2019;38(12):2003-2010.
12. Basu S, Berkowitz SA, Phillips RL, Bitton A, Landon BE, Phillips RS. Association of primary care physician supply with population mortality in the United States, 2005-2015. JAMA Intern Med. 2019;179(4):506–514. doi:10.1001/jamainternmed.2018.7624
13. Mode NA, Evans MK, Zonderman AB. Race, neighborhood economic status, income inequality and mortality. PLoS One. 2016;11(5):e0154535. Published 2016 May 12. doi:10.1371/journal.pone.0154535
14. Oladele, C.R.W., Barnett, E. Racial/Ethnic and social class differences in preventive care practices among persons with diabetes. BMC Public Health 6, 259 (2006). https://doi.org/10.1186/1471-2458-6-259
15. Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. N Engl J Med. 2017 Jun 15;376(24):2367-2375. doi: 10.1056/NEJMra1615439. PMID: 28614678.
16. Tan TW, Shih CD, Concha-Moore KC, et al. Disparities in outcomes of patients admitted with diabetic foot infections [published correction appears in PLoS One. 2019 Apr 11;14(4):e0215532]. PLoS One. 2019;14(2):e0211481. Published 2019 Feb 4.
17. https://www.ama-assn.org/sites/ama-assn.org/files/corp/media-browser/public/public-health/cehcd-goals-principles-strategies_1.pdf





