


Hammertoe Fixation And Cost-Effectiveness: What Are The Best Options?
 K-wires? Absorbable fixation? Intramedullary devices? What is the most cost-effective fixation for hammertoe procedures? With this question in mind, this author reviews the literature on the subject and discusses key considerations in reducing complication risk.
K-wires? Absorbable fixation? Intramedullary devices? What is the most cost-effective fixation for hammertoe procedures? With this question in mind, this author reviews the literature on the subject and discusses key considerations in reducing complication risk.
Symptomatic hammertoes remain among the most common ailments that foot and ankle surgeons treat. While there have been advances in our understanding of digital deformities and the importance of adjunctive soft tissue procedures, end-to-end arthrodesis remains the most common surgical treatment for repair of rigid hammertoes. Hammertoe fixation can come in many forms. Despite many new advances in types of fixation, Kirschner wire (K-wire) fixation remains the standard as it has been for nearly 100 years.1
In addition to fixating interphalangeal procedures, K-wires can simultaneously stabilize adjunctive procedures such as metatarsal osteotomies and soft tissue procedures of the lesser metatarsophalangeal joints (MPJs). Additional forms of fixation include various intramedullary devices, such as headless screws, Smart Toe (Stryker), StayFuse (Wright Medical) and absorbable implants. K-wire fixation has proven efficacious and inexpensive, but also has known complications. Reported complications including pin tract infections, pin migration, hardware failure, loss of correction, recurrence of deformity and amputation.2-6
 Researchers have described cost-effectiveness analysis in healthcare as “An economic study design in which consequences of different interventions are measured using a single outcome. Alternative interventions are then compared in terms of cost per unit of effectiveness.”7 Furthermore, the World Health Organization notes that cost-effective analysis of a specific intervention occurs to compare the new or novel intervention to current practice.8 The implication is that we should allocate health resources to maximize the outcome of interventions. Therefore, one should not use interventions that have not proven to be cost-effective.
Researchers have described cost-effectiveness analysis in healthcare as “An economic study design in which consequences of different interventions are measured using a single outcome. Alternative interventions are then compared in terms of cost per unit of effectiveness.”7 Furthermore, the World Health Organization notes that cost-effective analysis of a specific intervention occurs to compare the new or novel intervention to current practice.8 The implication is that we should allocate health resources to maximize the outcome of interventions. Therefore, one should not use interventions that have not proven to be cost-effective.
Stated more simply, a cost-effectiveness analysis compares the relative costs and outcomes of two or more treatments. This becomes more abstract as it pertains to surgical interventions given that costs and results are multivariate. Costs include direct medical costs (insurance benefit, coinsurance, co-pays, etc.), lost wages (time off work during recovery) as well as intangible costs to the patient (morbidity/pain during recovery, time spent in recovery and going to follow-ups). Outcomes are generally favorable or unfavorable.
A favorable outcome in hammertoe repair would, in theory, result in a satisfied patient. However, there are multiple variables with the perception of a “favorable outcome.” What means satisfaction for one patient may not mean satisfaction for another and vice versa. Somewhere in the middle of cost and outcome are those variables that are not necessarily a cost, but are normal components of treatment without being complications. For example, K-wire removal is an expected, normal component of hammertoe repair, but may be a component of the intervention that may deter patients or cause them to have a lower satisfaction with the procedure. While K-wire removal is an in-office procedure, some patients do find this painful and a cause of anxiety.
 Assessing The Costs And Post-Op Impact On The Patient
Assessing The Costs And Post-Op Impact On The Patient
As I previously stated, procedure costs are variable. In the current health environment, true financial costs will likely depend on contracts between industry and health systems, hospitals or surgery centers. As Jacobs reported in 2013, digital implants cost between $500 to $1,500 (which he accurately notes is more than the surgeon’s fee for the procedure itself) whereas the cost of a K-wire is between $10 to $20.9 Other financial costs to consider, which may vary depending on fixation method, include: time in the operating room on the day of surgery; implementation and delivery (delivery and sterilization of surgery sets for specialized equipment, etc.); the number and frequency of postoperative visits; and the requirement for hardware removal (planned or unplanned).
The cost of patient morbidity is difficult to quantify. Time off work or simply the ability to bear weight in a supportive shoe versus a postoperative boot can significantly affect a patient’s life during the recovery period. Buried fixation could in theory improve patient satisfaction by allowing an earlier return to closed-toe shoes, earlier full weightbearing and an earlier return to work.
In contrast, prominent K-wire fixation will generally require heel touch weightbearing, a cast boot or postoperative shoe. Depending on job requirements, patients may not be able to return to regular duty until they are in regular shoes. This can affect factory workers, construction workers and flight attendants to name a few. Finally, additional procedures, whether it is planned in-office K-wire removal or an unplanned revisional surgery, will contribute to patient dissatisfaction and anxiety about the procedure.
Pertinent Insights On Reducing Complication Risk
 First and foremost, it is important to recognize that not all complications of hammertoe repair are related to the type of fixation one employs but are more a reflection of inappropriate use of fixation or improper technique. Proper joint preparation and adjunct soft tissue procedures are warranted regardless of the choice of fixation. Common complications that are relatively independent of implant choice are chronic swelling and pain (although in some cases nonunion may be the cause, which may be related to fixation), lack of toe purchase and malposition. Intramedullary implantable devices rely on proper interphalangeal joint preparation and joint apposition, making it extremely difficult to implant the device without proper technique. Therefore, it is reasonable to assume that these implants may “encourage” better technique.
First and foremost, it is important to recognize that not all complications of hammertoe repair are related to the type of fixation one employs but are more a reflection of inappropriate use of fixation or improper technique. Proper joint preparation and adjunct soft tissue procedures are warranted regardless of the choice of fixation. Common complications that are relatively independent of implant choice are chronic swelling and pain (although in some cases nonunion may be the cause, which may be related to fixation), lack of toe purchase and malposition. Intramedullary implantable devices rely on proper interphalangeal joint preparation and joint apposition, making it extremely difficult to implant the device without proper technique. Therefore, it is reasonable to assume that these implants may “encourage” better technique.
With K-wire fixation, while joint preparation and apposition are necessary for a successful outcome, one can erroneously implant the fixation even without proper technique. During interphalangeal joint arthrodesis, the surgeon must ensure adequate preparation of the joint surfaces to avoid nonunion, avoid interposing soft tissues and appropriately compress the bone surfaces with sufficient bony apposition. The joint capsule or extensor tendon can easily become entrapped between the bony surfaces, and one must take care to reflect soft tissues prior to hardware insertion and compression.
Authors have described modifications to proximal interphalangeal joint end-to-end arthrodesis that improve bony apposition.10 These modifications include the peg-in-hole arthrodesis and the chevron arthrodesis. However, these modifications typically require more bone resection and contribute to toe shortening.
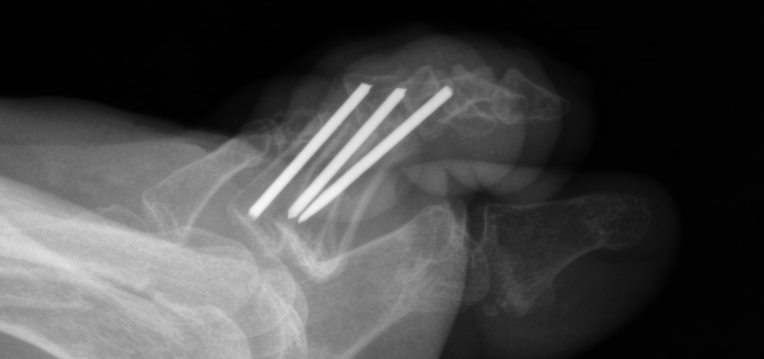
Implant sizing is important to avoid complications. Many of the newer hammertoe implants feature expanding “memory” metals, which not only aid in arthrodesis compression but also lend stability by expanding within the intramedullary canal. When using screws or K-wires, the surgeon must ensure that the diameter of the implant is appropriate for the diameter of the phalangeal intramedullary canals. Otherwise, rotation or residual flexion can occur as one can see in the photo above. In this example, the diameter of the embedded K-wires was too small and allowed for flexion and toggling within the intramedullary canal as well as loss of correction.
 Furthermore, poor patient adherence can be detrimental to any procedure and contribute to hardware breakage and procedure failure. The left photo shows a foot two weeks after the patient had a well positioned and fixated proximal interphalangeal arthrodesis. However, by the four-week follow-up, the patient had returned to regular shoes against medical advice and returned to full duty at his job as a construction worker, contributing to implant failure.
Furthermore, poor patient adherence can be detrimental to any procedure and contribute to hardware breakage and procedure failure. The left photo shows a foot two weeks after the patient had a well positioned and fixated proximal interphalangeal arthrodesis. However, by the four-week follow-up, the patient had returned to regular shoes against medical advice and returned to full duty at his job as a construction worker, contributing to implant failure.
What The Literature Reveals About Hammertoe Fixation
There are several types of fixation available with the standard being K-wires, which surgeons insert percutaneously for later in-office removal. Other fixation options include intramedullary implantable screws or other specialized devices, embedded K-wires and absorbable fixation. Below is a brief literature review of outcomes for each of these types of devices.
Kirschner wires. Various authors have discussed this “gold standard” of hammertoe fixation. Most foot and ankle surgeons keep temporary wires in place for an average of six weeks but Klammer and colleagues in 2012 reported no difference in complication rate following hammertoe correction with K-wire left in place for three weeks versus six weeks.11 The complications they assessed included infection, loosening and wire breakage.
 Kramer and coworkers in 2015 retrospectively reviewed 1,115 digital procedures on 876 patients with an average 20.8-month follow-up.2 They reported low overall complication rates including pin migration (3.5 percent), pin tract infection (0.3 percent), pin breakage (0.1 percent), recurrent deformities (5.6 percent), need for revision (3.5 percent), malalignment (2.1 percent), vascular compromise (0.6 percent) and amputation (0.4 percent). Revision was necessary in cases of recurrent deformity. The authors concluded that K-wire fixation maintains correction and has a low complication rate. Accordingly, K-wire provides an effective option at a low cost.2,9
Kramer and coworkers in 2015 retrospectively reviewed 1,115 digital procedures on 876 patients with an average 20.8-month follow-up.2 They reported low overall complication rates including pin migration (3.5 percent), pin tract infection (0.3 percent), pin breakage (0.1 percent), recurrent deformities (5.6 percent), need for revision (3.5 percent), malalignment (2.1 percent), vascular compromise (0.6 percent) and amputation (0.4 percent). Revision was necessary in cases of recurrent deformity. The authors concluded that K-wire fixation maintains correction and has a low complication rate. Accordingly, K-wire provides an effective option at a low cost.2,9
Several authors have reported on a modified technique of embedded K-wire fixation, which provides the benefit of an implantable device but at a much more reasonable cost.6,12 This technique involves standard joint preparation and insertion of the K-wire into the base of the proximal phalanx. One then trims the distal end of the wire about 0.5 to 1 cm prominent and impacts the distal phalanx upon the wire. When surgeons use the embedded K-wire technique appropriately, it can aid in an earlier return to closed-toed shoes in comparison to percutaneous wires.
Intramedullary devices. Researchers have described several specialized intramedullary devices with various outcomes but earlier reports note complication rates as high as 55.3 percent.13 However, more recent literature indicates these devices appear to be at least equivalent to K-wires in terms of effectiveness and avoidance of complications. Guelfi and colleagues reported on a systematic review of device options for proximal interphalangeal joint arthrodesis.3 Major complications occurred in up to 8.6 percent of cases with no statistical difference in complications between device options. The authors concluded that newer intramedullary devices provided equivalent results to K-wire fixation although at a higher price point.
 Scholl and coworkers in 2013 compared Smart Toe fixation to buried K-wires and found no statistical difference in rates of malunion, fracture, nonunion or the need for revision.14 Successful fusion occurred in 82.1 percent of patients with buried K-wires in comparison to 68.9 percent with Smart Toe fixation. The researchers reported hardware failure in 20.7 percent of the cases involving Smart Toe implants and 7.1 percent of cases in which surgeons used buried K-wires. The authors concluded that both implant options are viable options for implantable internal fixation.14
Scholl and coworkers in 2013 compared Smart Toe fixation to buried K-wires and found no statistical difference in rates of malunion, fracture, nonunion or the need for revision.14 Successful fusion occurred in 82.1 percent of patients with buried K-wires in comparison to 68.9 percent with Smart Toe fixation. The researchers reported hardware failure in 20.7 percent of the cases involving Smart Toe implants and 7.1 percent of cases in which surgeons used buried K-wires. The authors concluded that both implant options are viable options for implantable internal fixation.14
Digging deeper into the literature does reveal some outliers with some studies favoring newer devices and others favoring traditional K-wires. In a 2012 retrospective review that involved 28 cases, Angirasa and colleagues compared the Smart Toe implant to K-wire fixation with a focus on pain, complications, return to work and successful arthrodesis.5 They reported that the Smart Toe outperformed the K-wire and patients were able to resume full activity in less time.
Surveys of patients occurred on postoperative day seven, 14, 21, 28, 56 and at six months.5 At each visit, K-wire fixation had consistently higher Visual Analog Scale (VAS) pain scores than the Smart Toe group. The average return to full activity was 37.33 days in the K-wire group in comparison to 29.19 days in the Smart Toe group although this was not statistically significant. In the K-wire group, the authors reported complications including loss of correction, nonunion, malunion, persistent pain, hardware failure and the need for revision surgery. They reported no complications with the Smart Toe device. Of note, MMI-USA, the manufacturer of the Smart Toe implant at the time of the study, funded the study.5
 Basile and colleagues reported on their prospective study of a one-piece intramedullary fixation system for 60 proximal interphalangeal arthrodesis procedures.4 At an 18-month follow-up, they reported satisfactory radiographic alignment in 51 toes and one device failure (dislocation). Four patients had occasional pain in the toe. Likewise, Sandhu and colleagues reported on the use of the Smart Toe implant for 65 proximal interphalangeal joint fusions.15 They reported a 93.8 percent fusion rate and a 6.1 percent overall complication rate including 1.5 percent nonunion, three percent hardware failures and 1.5 percent implant displacement. Catena and coworkers reported a similar 81 percent union rate with an intramedullary implant.16 They noted that 87 percent of patients returned to preoperative activity level without limitations at an average 12-month follow-up.
Basile and colleagues reported on their prospective study of a one-piece intramedullary fixation system for 60 proximal interphalangeal arthrodesis procedures.4 At an 18-month follow-up, they reported satisfactory radiographic alignment in 51 toes and one device failure (dislocation). Four patients had occasional pain in the toe. Likewise, Sandhu and colleagues reported on the use of the Smart Toe implant for 65 proximal interphalangeal joint fusions.15 They reported a 93.8 percent fusion rate and a 6.1 percent overall complication rate including 1.5 percent nonunion, three percent hardware failures and 1.5 percent implant displacement. Catena and coworkers reported a similar 81 percent union rate with an intramedullary implant.16 They noted that 87 percent of patients returned to preoperative activity level without limitations at an average 12-month follow-up.
Absorbable devices. Similar to intramedullary devices, absorbable devices have the added benefit of eventually incorporating, leaving no hardware in the long term. These devices appear to have similar efficacy to that of K-wires and intramedullary devices. Kominsky and coworkers reported on the use of allograft for proximal interphalangeal arthrodesis.17 They reported on 63 toes in 32 patients and found a 97 percent fusion rate with no complications.
Konkel and colleagues in 2007 reported a 73 percent fusion rate with minimal complications using a soft polydioxanone embedded intramedullary pin.18 Several years later, Konkel and coworkers reported good outcomes for stiffer poly-L-lactate absorbable pins at an average 18-month follow-up.1 The researchers noted an 83 percent fusion rate with stable partial nonunion in 4 percent of cases and stable fibrous union in 13 percent of the cases. The authors reported no transfer lesions, no hyperextension deformities and high patient satisfaction. Konkel and colleagues did acknowledge that most patients had minor toe swelling and toe tenderness for up to a year after surgery. Floating toe occurred in 34 percent of the cases.
In Conclusion
A cursory review of recent literature demonstrates the complication rate of newer fixation options to be similar to that of traditional K-wire fixation, suggesting that traditional K-wire fixation remains the most cost-effective approach due to a much lower price point. Regardless of fixation type, one can minimize complications by having a thorough understanding of the deformity including appropriate adjunctive procedures as well as adequate joint preparation and compression of the fusion site.
Ultimately, fixation selection should depend on multiple factors, including cost-effectiveness, adjunctive procedures and patient selection. Percutaneous K-wire fixation is certainly cheaper and allows for stabilization of lesser metatarsal osteotomies and soft tissue balancing procedures of the metatarsophalangeal joint. However, embedded implants (K-wires or otherwise) may be more desirable in isolated proximal interphalangeal joint fusions without adjunctive procedures or in patients who would otherwise not tolerate percutaneous fixation.
Dr. Clifford is affiliated with CHI Franciscan Orthopedic Associates at St. Francis in Federal Way, Wash. He is the Research Director at Franciscan Foot and Ankle Institute in Federal Way, Wash., and is also a member of the Advisory Board of the International Foot and Ankle Foundation for Education and Research.
References
- Konkel KF, Sover ER, Menger AG, Halberg JM. Hammer toe correction using an absorbable pin. Foot Ankle Int. 2011;32(10):973-8.
- Kramer WC, Parman M, Marks RM. Hammertoe correction with K-wire fixation. Foot Ankle Int. 2015; 36(5):494–502.
- Guelfi M, Pantalone A, Daniel JC, Vanni D, Guelfi MG, Salini V. Arthrodesis of proximal inter-phalangeal joint for hammertoe: intramedullary device options. J Orthop Traumatol. 2015;16(4):269-73.
- Basile A, Albo F, Via AG. Intramedullary fixation system for the treatment of hammertoe deformity. J Foot Ankle Surg. 2015;54(5):910-6.
- Angirasa AK, Barrett MJ, Silvester D. SmartToe® implant compared with Kirschner wire fixation for hammer digit corrective surgery: a review of 28 patients. J Foot Ankle Surg. 2012;51(6):711-3.
- Moon JL, Kihm CA, Perez DA, Dowling LB, Alder DC. Digital arthrodesis: current fixation techniques. Clin Podiatr Med Surg. 2011;28(4):769-83.
- National Clinical Guideline Centre. National Clinical Guideline Centre for Acute and Chronic Conditions, 2010. Available at www.guideline.gov/browse/by-organization.aspx?orgid=1696 .
- World Health Organization. WHO Guide to Cost-Effectiveness Analysis, 2003. Available at www.who.int/choice/publications/p_2003_generalised_cea.pdf .
- Jacobs A. Are digital implants more cost-effective than K-wires? Podiatry Today DPM Blog. Available at www.podiatrytoday.com/blogged/are-digital-implants-more-cost-effective-k-wires . Published July 19, 2013. Accessed Nov. 1, 2015.
- Kernbach KJ. Hammertoe surgery: arthroplasty, arthrodesis or plantar plate repair? Clin Podiatr Med Surg. 2012;29(3):355-66.
- Klammer G, Baumann G, Moor BK, Farshad M, Espinosa N. Early complications and recurrence rates after Kirschner wire transfixion in lesser toe surgery: a prospective randomized study. Foot Ankle Int. 2012; 33(2):105–112.
- Canales MB, Razzante MC, Ehredt DJ, Clougherty CO. A simple method of intramedullary fixation for proximal interphalangeal arthrodesis. J Foot Ankle Surg. 2014;53(6):817-24.
- Ellington JK, Anderson RB, Davis WH, Cohen BE, Jones CP. Radiographic analysis of proximal interphalangeal joint arthrodesis with an intramedullary fusion device for lesser toe deformities. Foot Ankle Int. 2010; 31(5):372–376.
- Scholl A, Mccarty J, Scholl D, Mar A. Smart Toe® implant versus buried Kirschner wire for proximal interphalangeal joint arthrodesis: a comparative study. J Foot Ankle Surg. 2013; 52(5):580–583.
- Sandhu JS, Decarbo WT, Hofbauer MH. Digital arthrodesis with a one-piece memory nitinol intramedullary fixation device: a retrospective review. Foot Ankle Spec. 2013;6(5):364-6.
- Catena F, Doty JF, Jastifer J, Coughlin MJ, Stevens F. Prospective study of hammertoe correction with an intramedullary implant. Foot Ankle Int. 2014;35(4):319-25.
- Kominsky SJ, Bermudez R, Bannerjee A. Using a bone allograft to fixate proximal interphalangeal joint arthrodesis. Foot Ankle Spec. 2013;6(2):132-6.
- Konkel KF, Menger AG, Retzlaff SA. Hammer toe correction using an absorbable intramedullary pin. Foot Ankle Int. 2007;28(8):916-20.
For further reading, see “Current Concepts In Hammertoe Correction” in the September 2015 issue of Podiatry Today.

