


How To Treat Puncture Wounds
 A seemingly trivial puncture wound can be at risk for infection, osteomyelitis or other complications due to a delayed diagnosis or inappropriate management. Accordingly, these authors provide a comprehensive guide to the diagnosis and management of puncture wounds.
A seemingly trivial puncture wound can be at risk for infection, osteomyelitis or other complications due to a delayed diagnosis or inappropriate management. Accordingly, these authors provide a comprehensive guide to the diagnosis and management of puncture wounds.
Podiatric physicians commonly encounter puncture wounds. Although most of these wounds heal uneventfully, delayed or inadequate treatment can lead to complications.1 Outcomes often depend on the location and severity of the injury, the patient’s medical status and the type of penetrating object.
Potential complications include cellulitis, deep space abscess, septic arthritis, retained foreign body granuloma, harm to underlying anatomical structures and osteomyelitis.2 Schwab and Powers reported infection rates of 6 to 11 percent in pedal puncture wounds in patients presenting to the emergency room.3 Many of these wounds are the result of nails, sewing needles, broken glass, wooden toothpicks, tacks, thorns and animal bites.4 Puncture wounds often occur in children with and without shoes while they are playing outdoors.5
Osteomyelitis is the most severe complication secondary to a puncture wound. The incidence of osteomyelitis is associated with the location of the injury, delay in treatment and whether patients were wearing footwear at the time of injury.6
Various authors have reported the occurrence of osteomyelitis in puncture wounds but with differences in the incidence rate. The classic article by Patzakis and colleagues divided the foot up into three zones and reported associated osteomyelitis.7 Zone 1 extends from the metatarsal necks distally to the end of the toes. Zone 2 includes the distal aspect of the calcaneus to the metatarsal necks. Zone 3 includes the plantar aspect of the calcaneus. They found that patients with puncture wounds in zone 1 had the highest risk of osteomyelitis development followed by those with zone 3 puncture wounds. Of the 36 patients in their study, 34 (94 percent) developed osteomyelitis, pyarthrosis or both. Fitzgerald and Cowan have reported the incidence of puncture wounds that progress to osteomyelitis to be 1.8 percent in the pediatric population.4 Houston and colleagues reported that only 51 of 2,303 patients (2.2 percent) developed wound infection and only one of these 51 (2 percent) developed osteomyelitis.8
 The course of osteomyelitis is often slow and indolent. Patients with osteomyelitis will often recall a puncture wound, which may or may not have had professional treatment. The wound often resolves. Then several days to months later, the patient develops increased pain and swelling with or without drainage from the puncture site. At this point, one should consider a diagnosis of osteomyelitis and/or a retained foreign body.
The course of osteomyelitis is often slow and indolent. Patients with osteomyelitis will often recall a puncture wound, which may or may not have had professional treatment. The wound often resolves. Then several days to months later, the patient develops increased pain and swelling with or without drainage from the puncture site. At this point, one should consider a diagnosis of osteomyelitis and/or a retained foreign body.
The Importance Of Ascertaining An Accurate Patient History
In managing pedal puncture wounds, the obvious goal is to prevent complications and/or limit the spread of infectious processes. One should start with a comprehensive medical history, including the patient’s current medications and allergies. It is critical to ascertain the time and date of the injury, and any treatment that may have occurred. Clinicians should also try to determine the type of shoe gear the patient wore (if any) and the environment in which the wound occurred as well as the type of penetrating object. This information can offer clues as to the type of organism that can cause infection and the possibility of a retained foreign body.
 Gathering information on the patient’s tetanus status is also important. Puncture wounds can be Clostridium-prone, leading to severe systemic infection. The Centers for Disease Control and Prevention (CDC) frequently update tetanus immunization guidelines and recommend checking with current protocols before administering treatment. For current treatment guidelines, see “What The CDC Recommends For Tetanus Vaccines” at left.9
Gathering information on the patient’s tetanus status is also important. Puncture wounds can be Clostridium-prone, leading to severe systemic infection. The Centers for Disease Control and Prevention (CDC) frequently update tetanus immunization guidelines and recommend checking with current protocols before administering treatment. For current treatment guidelines, see “What The CDC Recommends For Tetanus Vaccines” at left.9
A Guideline For Wound Inspection/Evaluation
One should carefully inspect the wound. The puncture site usually exhibits signs of acute injury, such as localized erythema and edema. If time has elapsed, the wound may have closed over and it can be difficult to locate the area of penetration. A seemingly benign puncture wound may have inadequate treatment, which often leads to complications.1
Depth of penetration is an important factor. According to Patzakis and coworkers, the deeper the penetration, the more likely a serious complication will occur.7 However, it is often difficult to accurately estimate the true depth. Penetration into deep structures such as tendons, bursae and joint capsule may allow infectious organisms to establish themselves due to the relative avascularity of these structures. Evaluation of the patient’s motor and sensory function is important so as not to miss a lacerated tendon or nerve.
Inspection of wound edges is crucial. Clean wound edges/margins are less likely to harbor bacteria. Jagged, irregular wound margins can lead to skin necrosis due to an increase in surface area of multiple skin apices. Not only are such wounds relatively avascular, they have a greater potential for inoculation and infection.
What Diagnostic Studies Can Reveal
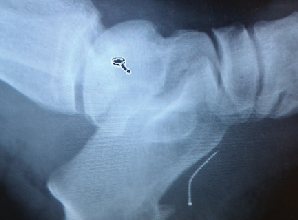
Always take standard radiographs after any puncture wound. X-rays can determine the presence of a retained foreign body or if any osseous structure has been breached. However, X-rays may be inadequate in the detection of small pieces of glass, wood or rubber. In those cases, advanced imaging studies may be necessary.
Computed tomography (CT) can provide superior imaging when it comes to detecting wood deep in tissues.10 Magnetic resonance imaging (MRI) may be helpful, especially in detecting osteomyelitis as MRI provides a precise anatomic location of the infection and assists the surgeon when planning surgical debridement.11 Ultrasound is a very helpful modality in detecting non-radiopaque foreign bodies and is cost-effective.
 Radionuclide imaging is important and very helpful when one suspects osteomyelitis. Plain films do not detect osteomyelitis for 10 to 14 days after the establishment of bone infection. Technetium-99m-methylene diphosphonate (Tc99m MDP) bone scans are very sensitive and can detect bone infection within 24 hours of the onset of infection. However, Tc99m MDP has a low specificity. Therefore, tagged white blood cell scans (i.e. hexamethylpropyleneamine oxime scans) may be more specific for localizing infection.12
Radionuclide imaging is important and very helpful when one suspects osteomyelitis. Plain films do not detect osteomyelitis for 10 to 14 days after the establishment of bone infection. Technetium-99m-methylene diphosphonate (Tc99m MDP) bone scans are very sensitive and can detect bone infection within 24 hours of the onset of infection. However, Tc99m MDP has a low specificity. Therefore, tagged white blood cell scans (i.e. hexamethylpropyleneamine oxime scans) may be more specific for localizing infection.12
One should also obtain laboratory studies. A white blood cell count and comprehensive metabolic panel can provide insight during suspected infectious processes. Notably, the erythrocyte sedimentation rate (ESR) may be elevated, especially when osteomyelitis is present.
Key Insights On The Microbiology Of Puncture Wounds
Many forms of bacteria have been isolated in puncture wounds of the foot. The most common Gram-positive organisms isolated are Staphylococcus aureus, alpha-hemolytic Streptococci and Staphylococcus epidermidis.13 Authors have also identified Gram-negative organisms such as Escherichia coli, Proteus and Klebsiella sp. Pasteurella multocida has been isolated from dog and cat bites as well as Eikenella corrodens in human bite wounds.14 Miscellaneous organisms that researchers have isolated from puncture wounds occurring in brackish water include Aeromonas hydrophila and Mycobacterium marinum.15
Pseudomonas is the most common organism responsible for osteomyelitis secondary to puncture wounds.7,16 There is a documented association between rubber soled shoes and Pseudomonal osteomyelitis.16,17 When a nail or other object penetrates the shoe and then the foot, it inoculates the wound with the Pseudomonas organism found on the shoe.
Addressing Puncture Wounds In Patients With Diabetes
When a p atient with diabetes presents with a puncture wound, one must consider a unique set of factors. These wounds can be limb- or life-threatening, and need aggressive management. Peripheral neuropathy, immunopathy and peripheral arterial disease result in a greater risk for complications. Patients with diabetes are often unaware of the initial injury due to a loss of protective sensation. Wounds may go undetected and are at greater risk for infection. Due to immunopathy, these patients may not develop systemic signs of sepsis, such as chills, fever, or night sweats. Laboratory studies may also be under-representative of a severe infection.18
atient with diabetes presents with a puncture wound, one must consider a unique set of factors. These wounds can be limb- or life-threatening, and need aggressive management. Peripheral neuropathy, immunopathy and peripheral arterial disease result in a greater risk for complications. Patients with diabetes are often unaware of the initial injury due to a loss of protective sensation. Wounds may go undetected and are at greater risk for infection. Due to immunopathy, these patients may not develop systemic signs of sepsis, such as chills, fever, or night sweats. Laboratory studies may also be under-representative of a severe infection.18
Tetanus immunization history is vital in the patient with diabetes. Researchers have shown tetanus to be three times more common and associated fatalities are four times more prevalent in this patient population.19 Armstrong and colleagues reviewed the course of patients with diabetes who suffered puncture wounds and found them 46 times more likely to have an amputation than those without diabetes.20
Patients with diabetes are also prone to polymicrobial infections such as Gram-positive, Gram-negative and anaerobic bacteria. Accordingly, one should choose the appropriate antibiotics as outlined below and/or consult an infectious disease specialist.
 Pertinent Treatment Considerations
Pertinent Treatment Considerations
Banks and colleagues have noted that “The delay between the time of injury and the initiation of treatment is perhaps the most critical factor in determining whether or not an infection develops and the severity of complications following a puncture wound.”21
Upon the initial presentation of a pedal puncture wound, one must first perform a problem-focused history and physical exam, paying close attention to details involving the source and time-lapse of injury. Furthermore, clinicians should pay special consideration to any comorbidities such as diabetes mellitus with or without neuropathy, peripheral vascular disease or other immunocompromised conditions.
During the physical examination, be sure to evaluate the size, depth and shape of the punctured foot wound. Pay close attention to the skin edges. Many times, traumatic objects may leave a jagged appearance. To determine depth and possible fascial/capsular/bony involvement, use a blunt, sterile probe.1
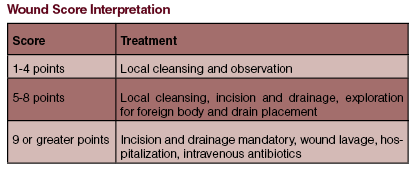
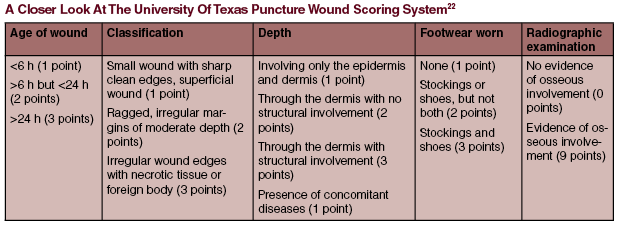 If there is no evidence of a retained foreign body and the wound is superficial, small and one discovers it in less than six hours, it is reasonable to cleanse the wound with saline (preferably with a large 20 cc syringe), and cover it with a sterile dressing (see “A Closer Look At The University Of Texas Puncture Wound Scoring System” at right).22
If there is no evidence of a retained foreign body and the wound is superficial, small and one discovers it in less than six hours, it is reasonable to cleanse the wound with saline (preferably with a large 20 cc syringe), and cover it with a sterile dressing (see “A Closer Look At The University Of Texas Puncture Wound Scoring System” at right).22
When a puncture wound presents in the delayed treatment setting, is deep or has significant clinical contamination, one should perform incision and drainage. If there is a retained foreign body, triangulation with fluoroscopy and/or ultrasound can be helpful. Nonetheless, all necrotic/non-viable soft tissue and bone should have aggressive debridement with high pressure pulse lavage.23 Sharply incise jagged skin edges to decrease the chance of skin necrosis. Pack the wounds open or closed over a drain (i.e. Penrose, closed suction). In the operating room setting, obtain deep wound and tissue cultures. If there is suspected bony involvement, bone cultures can rule out osteomyelitis.
 Address and appropriately administer antibiosis when a patient sustains a traumatic puncture wound. Patients who present early (less than six hours) with a clean, non-infected puncture wound with no medical comorbidities should receive clinical treatment. In this setting, empiric antibiotics are not required. However, if a patient does have certain risk factors for developing infection, presents in the delayed treatment setting or presents with a grossly contaminated wound, provide antibiotics.
Address and appropriately administer antibiosis when a patient sustains a traumatic puncture wound. Patients who present early (less than six hours) with a clean, non-infected puncture wound with no medical comorbidities should receive clinical treatment. In this setting, empiric antibiotics are not required. However, if a patient does have certain risk factors for developing infection, presents in the delayed treatment setting or presents with a grossly contaminated wound, provide antibiotics.
First-generation cephalosporins such as cephalexin (Keflex, Aspen Pharmacare) or cefadroxil (Duricef) are sufficient for most superficial puncture wounds. If the wound is grossly contaminated and/or a metallic object has penetrated the skin or shoe, adjust empiric antibiotics accordingly. Typical anti-Pseudomonas antibiotics include ciprofloxacin (Cipro, Bayer) or levofloxacin (Levaquin, Janssen Pharmaceuticals). Ceftazidime (Fortaz, Sagent Pharmaceuticals) and aztreonam (Azactam, Bristol-Myers Squibb) are strictly intravenous anti-Pseudomonas antibiotics yet work well for the inpatient setting.
Broad-spectrum antibiotics are also a good idea for the patient with diabetes or for a dirty wound. Amoxicillin/clavulanic acid (Augmentin, GlaxoSmithKline), trimethoprim/sulfamethoxazole or combination antibiotics such as clindamycin and ciprofloxacin provide appropriate bacterial coverage. If the patient requires hospital admission and an intravenous line, one can give broad-spectrum antibiotics such as piperacillin/tazobactam (Zosyn, Pfizer) or imipenem/cilastatin (Primaxin, Merck).
With  the emergence of resistant organisms such as methicillin-resistant Staphylococcus aureus (MRSA), vancomycin resistant Enterococcus (VRE) and multi-drug resistant Pseudomonas, one may argue that empiric antibiotics to cover such resistant organisms are warranted. In New York City, the prevalence of MRSA is an astounding 24 percent.23 Furthermore, community-acquired MRSA is on the rise throughout the United States.23
the emergence of resistant organisms such as methicillin-resistant Staphylococcus aureus (MRSA), vancomycin resistant Enterococcus (VRE) and multi-drug resistant Pseudomonas, one may argue that empiric antibiotics to cover such resistant organisms are warranted. In New York City, the prevalence of MRSA is an astounding 24 percent.23 Furthermore, community-acquired MRSA is on the rise throughout the United States.23
In a large, multicenter study in the New England Journal of Medicine, authors determined that “MRSA is the most common identifiable cause of skin and soft tissue infections among patients presenting to emergency departments in eleven U.S. cities. Moreover, when antimicrobial therapy is indicated for the treatment of skin and soft tissue infections, clinicians should consider obtaining cultures and modifying empirical therapy to provide MRSA coverage.”23
Therefore, it is the senior author’s recommendation that if a patient who sustains a traumatic puncture wound presents with an abscess or cellulitis, has multiple comorbidities, or certain risk factors for MRSA (i.e. history of MRSA, healthcare worker who is exposed to resistant Staph, multiple hospitalizations, steroid use, etc.), it would be prudent to treat these patients empirically with anti-MRSA antibiotics.23
Currently, at our institution, if a patient presents without risk factors for MRSA colonization, we do not administer routine anti-MRSA antibiotics. In time, however, our protocol may change as drug resistance patterns change. It is important to have a working relationship with infectious disease specialists in your community to ensure the best approach to handle this challenging and evolving dilemma.
In Conclusion
Puncture wounds are a common traumatic pedal injury. Serious complications can occur, including skin necrosis, deep abscess formation and osteomyelitis. When the podiatric physician obtains a thorough history and physical examination in conjunction with the use of imaging and clinical insight, one can avoid most complications. Consider appropriate antibiosis and surgical intervention when necessary. Remember that timely treatment is essential and consider all risk factors when evaluating these wounds.
Dr. Keller is the Director of Podiatric Medical Education and the Residency Director of Podiatric Surgery at Health Alliance of the Hudson Valley in Kingston, NY.
Dr. Thun is a third-year podiatric surgical resident at Health Alliance of the Hudson Valley.
Dr. Curfman is a second-year podiatric surgical resident at Health Alliance of the Hudson Valley.
References
1. Haverstock BD, Grossman JP. Puncture wounds of the foot: evaluation and treatment. Foot Ankle Trauma. 1999;16(4):583-596.
2. Chudnofsky CR, Sebastian S. Special wounds: nail bed plantar puncture and cartilage. Emerg Med Clin. N Am. 1992;10(4):801-821.
3. Schwab R, Powers R. Conservative therapy of plantar puncture wounds. J Emerg Med. 1995;13(3):291-5.
4. Fitzgerald RH Jr, Cowan JD. Puncture wounds of the foot. Orthop Clin North Am. 1975;6(4):965-972.
5. Baldwin G, Colbourne M. Puncture wounds. Pediatr Rev. 1999;20(1):21-23.
6. Lavery LA, Harkless LB, Ashry HR, et al. Infected puncture wounds in the adult with diabetes: Risk factors for osteomyelitis. J Foot Ankle Surg. 1994;33(6):561-566.
7. Patzakis MJ, Wilkens J, Brien WW, et al. Wound site as a predictor of complications following deep nail punctures to the foot. West J Med. 1989;150(5):545-547.
8. Houston A, Roy W, Faust R. Tetanus prophylaxis in the treatment of puncture wounds of patients in the deep South. J Trauma. 1962;2:439-446.
9. Belin R, Carrington S. Management of pedal puncture wounds. Clin Podiatr Med Surg. 2012;29(3):451-8.
10. Nyska M, Pomeranz S, Porat S. The advantage of computerized tomography in locating a foreign body in the foot. J Trauma. 1986;26(1):93-95.
11. Lau LS, Bin G, Jaovisidua S, et al. Cost-effectiveness of magnetic resonance imaging in diagnosing Pseudomonas aeruginosa infection after a puncture wound. J Foot Ankle Surg. 1997;36(1):36-43
12. Blume PA, Dey HM, Daley LJ, Arrighi JA, et al. Diagnosis of pedal ostomyelitis with Tc-99m HMPAO labeled leukocytes. J Foot Ankle Surg. 1997;36(2):120-126.
13. Joseph WS, LeFrock JL. Infections complicating puncture wounds of the foot. J Foot Surg. 1987;26(3):530-532.
14. Butt TS, Khan A, Ahmad MA, et al. Pasteurella multiocida infectious arthritis with gout after a cat bite. J Rheumatol. 1997;24(8):1649-1652.
15. Joseph WS. Infections following trauma. In: Handbook of Lower Extremity Infections, Second Edition. Churchill Livingstone, New York, 2003, pp. 84-90.
16. Fisher MC, Goldsmith JF, Gilligan PH. Sneakers as a source of Pseudomonas aeruginosa in children with osteomyelitis following puncture wounds. J Pediatr. 1985;106:607-609.
17. Saha P, Parrish CA, McMillan. Pseudomonas osteomyelitis after a plantar puncture wound through a rubber sandal. Pediatr Infect Dis. 1996;15:710-711.
18. Lavery LA, Armstrong DG, Quebedeaux TL, et al. Normal laboratory values in the face of severe infection in diabetics and non-diabetics. Am J Med. 1996;101(5):521-525.
19. Lavery L, Harkless LB. Infected puncture wounds in the adult with diabetes: risk factors for osteomyelitis. J Foot Ankle Surg. 1994;33(6):561-566.
20. Armstrong DG, Lavery LA, Quebedeaux TL, et al. Surgical morbidity and the risk of amputation due to infected puncture wounds in diabetic versus nondiabetic adults. J Am Podiatr Med Assoc. 1997;87(7):321-326.
21. Banks AS, Downey MS, Martin DE, et al. McGlamry’s Comprehensive Textbook of Foot and Ankle Surgery. JB Lippincott, Philadelphia, 2001, pp. 1653-1658.
22. Krych SM, Lavery LA. Puncture wounds and foreign body reactions. Clin Podiatr Med Surg. 1990; 7(4):725-731.
23. Moran GJ, Krishnadasan A, Gorwitz, RJ, et al. Methicillin-Resistant S. aureus Infections among patients in the emergency department. N Engl J Med. 2006;355(7):666-673.

