


Pertinent Insights In Treating CrossFit-Related Injuries
 Due to the intensity of CrossFit workouts, athletes can sustain injuries such as ankle sprains, metatarsal fractures and shin splints. This author offers a guide to diagnosing and treating common CrossFit injuries, and provides a couple of illuminating case studies.
Due to the intensity of CrossFit workouts, athletes can sustain injuries such as ankle sprains, metatarsal fractures and shin splints. This author offers a guide to diagnosing and treating common CrossFit injuries, and provides a couple of illuminating case studies.
In a sports medicine-based private practice, patients with a host of injuries come through the door on a daily basis. The maladies range from chronic overuse to acute traumatic injuries. The majority of my patients are runners and triathletes, but CrossFit athletes are increasingly presenting with injuries.
The rise of CrossFit gyms, or “boxes,” has occurred with increased advertising and word of mouth. CrossFit is unique as it combines the core aspects of gymnastics, Olympic-style weightlifting, running, rowing and high-intensity movements. As CrossFit’s popularity rises, so does the amount of CrossFit-related injuries. A 2014 survey of CrossFit athletes found that almost 20 percent of the 386 athletes surveyed had experienced injuries related to CrossFit.1 Due to the movements associated with CrossFit, the most common areas for injury are the shoulder, lower back and the knee, but there is a fair amount of lower extremity injuries as well.
Even if athletes do CrossFit correctly, an athlete who trains in any sport or activity for a length of time will eventually have an injury. Muscles get fatigued, joints become achy and old injuries flare up. Athletes can work around some injuries and others need treatment and rest, depending on whether the injuries are acute trauma or overuse injuries. When CrossFit started, there were very few physicians who knew anything about treating these athletes as they were unsure what was involved with CrossFit.2 Being a CrossFit athlete myself, I have treated and dealt with a multitude of injuries. The key in treating CrossFit athletes is to understand CrossFit.
Understanding The Dynamics Of CrossFit
Retired gymnast Greg Glassman founded CrossFit in the year 2000 but the program had been in development for years.3 The workouts are based on three principles: mechanics, consistency and intensity. Mechanics refers to the technique. Consistency describes the execution of the movements. Intensity varies based on the fitness level of the athlete.4
Basic foundational movements are key to CrossFit and Olympic-style weightlifting. One of the most basic of these movements is the squat. Variations of the squat include air squats without weight; a front squat, holding a weighted barbell in your hands on the front of your chest; an overhead squat, holding the barbell pressed in the air above your head; and a back squat, holding the barbell against your shoulders behind your neck. Other foundational movements include the shoulder press, push press, push jerk and deadlifts. The gymnastics elements include handstands, handstand push-ups and ring dips among others. Other types of movements vary from pull-ups, chin-ups, push-ups, sit-ups, burpees and box jumps. There is usually some incorporated cardiovascular exercise including short distance sprints, rowing and jump rope.
 The workouts are an hour long and incorporate stretching for mobility and flexibility, a period of either Olympic-style weightlifting or a skill move (such as handstands or handstand pushups), followed by the “Workout of the Day” (WOD). The workout of the day is usually a combination of strength and aerobic exercise, done either for time or in rounds. Data drives the workouts. The score between athletes is based on the number of rounds in a certain timeframe or time to get through the rounds.3 This provides measurable results that can further motivate the workouts.
The workouts are an hour long and incorporate stretching for mobility and flexibility, a period of either Olympic-style weightlifting or a skill move (such as handstands or handstand pushups), followed by the “Workout of the Day” (WOD). The workout of the day is usually a combination of strength and aerobic exercise, done either for time or in rounds. Data drives the workouts. The score between athletes is based on the number of rounds in a certain timeframe or time to get through the rounds.3 This provides measurable results that can further motivate the workouts.
Is Footwear A Key Factor?
A common mistake that beginner athletes make is not understanding the correct footwear for the activity. There are a multitude of different running shoes depending on foot type and the terrain. Most running shoes are built for forward motion, providing stability and shock absorption. They typically have thicker heels and midsoles, and are heavier in weight. Most of the CrossFit workouts involve agility drills, linear exercises and side to side movements that make the running shoe less than ideal.5 In fact, there are many weightlifters who prefer being barefoot or wearing a minimalist shoe. The thought is that this will require greater proprioception and give the athlete a better awareness of the ground, and an ability to adjust foot position for better stability.6
Training shoes or CrossFit-specific shoes are a good option. They have more flexibility in the forefoot to allow increased agility, added support to the lateral sides and added cushioning for extra shock absorption. This allows CrossFit athletes to move seamlessly between flexibility movements, like lunges, directly into a run and still have the support they need.5 Much like any other sport, you have to find the shoe that is right for you. The wrong shoe for your foot type can create a variety of different injuries.
 How A Lack Of Flexibility Can Contribute To Injury
How A Lack Of Flexibility Can Contribute To Injury
I have found that many patients think they do enough stretching but they rarely ever do enough, especially when they have an injury. Studies have often cited a lack of flexibility as a factor responsible for various sports-related complaints.7 Researchers have shown a strong correlation between tight ligaments and muscle groups in association with lower extremity injuries.7
Restricted ankle dorsiflexion is a major factor in pain in the ankle during many of the CrossFit squatting movements. Limited dorsiflexion of the hallux can create pain in many of the lunge and burpee movements as well as planks and push-ups. Most CrossFit trainers spend a significant portion of the hour-long workout session on flexibility and mobility in order to prevent injury, but patients cannot overcome some range of motion limitations due to the structure of their foot or ankle.
An Overview Of Common CrossFit Injuries
Ankle sprains. Lateral ankle sprains are the most common injury in sports and make up the majority of the sports-related injuries I see in my practice. Ankle injuries in CrossFit are very common. Some common activities that may lead to ankle injury are jump rope, burpees and box jumps.
The lateral ankle ligaments, including the anterior talofibular, the calcaneofibular and the posterior talofibular ligaments, work together to stabilize the ankle and the subtalar joint. The most commonly injured ligament is the anterior talofibular ligament, which has the lowest load to failure of the three ligaments.7 Injury usually results from lack of proprioception or a reduced sense of joint position, which is especially prone to occur with movements that involve jumping up and landing back onto the ground.
The athlete will usually have swelling and tenderness to the affected ankle ligaments, and may have difficulty bearing weight. A range of motion evaluation will often show pain with passive plantarflexion and inversion, and pain with active eversion. Treatment in my practice is based on severity of the symptoms. Immobilization is usually necessary with a pneumatic walker unless the patient is able to tolerate ambulation in an ankle brace and has minimal swelling. Once the acute pain has resolved, the focus turns to strengthening and stability in order to prevent re-injury. Re-injury is a common issue leading to chronic ankle instability.
 Sinus tarsi syndrome or lateral ankle impingement. Many athletes suffer from a vague pain or “pinching” feeling over the lateral ankle. This commonly occurs during heavy weight squatting at the base of the squat. These athletes may have excessive pronation and when their flexible shoe gear does not accommodate this pronation, the talus and calcaneus impact laterally, causing pain. This condition is known as sinus tarsi syndrome or lateral ankle impingement. On exam, there may be pinpoint tenderness over the lateral subtalar joint.
Sinus tarsi syndrome or lateral ankle impingement. Many athletes suffer from a vague pain or “pinching” feeling over the lateral ankle. This commonly occurs during heavy weight squatting at the base of the squat. These athletes may have excessive pronation and when their flexible shoe gear does not accommodate this pronation, the talus and calcaneus impact laterally, causing pain. This condition is known as sinus tarsi syndrome or lateral ankle impingement. On exam, there may be pinpoint tenderness over the lateral subtalar joint.
Conservative treatment is usually successful and includes a change in shoe gear, custom orthotics, physical therapy and possible cortisone injection.
Fractures. Fractures in CrossFit athletes can occur in a variety of different situations. Most commonly, fractures result from blunt trauma to the foot from dropping a weight, hitting the anterior shin on a wooden box during a box jump or from rotational injuries, such as the fracture of the fifth metatarsal with an inversion ankle injury. Physicians must take care to diagnose an open fracture, especially when it is present in the hallux distal phalanx in conjunction with a subungual hematoma. Base the diagnosis on serial radiographs.
Patients usually need protected weightbearing in a pneumatic walker for a period of six to eight weeks if minimally displaced. If there is displacement greater than 2 mm, open reduction with internal fixation is usually required for faster recovery in higher level CrossFit athletes.
Stress fractures of the tibia and fibula. Certain CrossFit activities put repetitive strain on the tibia and fibula, including squatting with heavy weights, jump rope and box jumps. Stress fractures are a result of abnormal repetitive loads on the bone that cause bone to resorb faster than it can repair itself.7 The pain is usually a gradual onset, worsening over time. The pain often begins with an ache in the lower leg that is nonspecific and not limiting so the athlete is able to continue to exercise through the pain. It will eventually worsen to the point of increased pain, swelling and pinpoint tenderness over the area of the stress fracture. Base the diagnosis on clinical symptoms as initial radiographs are usually normal at the onset of the symptoms. There may be a mild lucency in the cortex of the bone at two to three weeks after injury, which will become a cortical thickening over time.7 A magnetic resonance image (MRI) or bone scan may be warranted early for a more immediate and definitive diagnosis.
Stress fractures usually have conservative treatment. Immobilization is often appropriate but one can choose treatment based on the severity of the symptoms. The athlete may need a modification or “scaling” of the activities to lower impact movements that will still work the same muscle groups.
Inflammation, stress fractures and fractures of the sesamoids. The sesamoids are often injured due to their position and lack of blood supply. They function to assist in push off of the hallux and help stabilize the first metatarsophalangeal joint (MPJ).8 Due to the repetitive jumping movements and movements (such as burpees, push-ups, planks and lunges) that require a greater flexibility in the first MPJ, the sesamoids are commonly injured in CrossFit.
 Symptoms can vary from an ache with high-impact activity to a sharp pain with simple walking. The clinical exam will include pain on palpation to the injured sesamoid and pain with range of motion of the first MPJ, especially dorsiflexion. Injury may be difficult to diagnose on radiographs if the fracture is not overt. An MRI may be necessary if the initial imaging is inconclusive or if one must differentiate between a bipartite sesamoid and a fracture.
Symptoms can vary from an ache with high-impact activity to a sharp pain with simple walking. The clinical exam will include pain on palpation to the injured sesamoid and pain with range of motion of the first MPJ, especially dorsiflexion. Injury may be difficult to diagnose on radiographs if the fracture is not overt. An MRI may be necessary if the initial imaging is inconclusive or if one must differentiate between a bipartite sesamoid and a fracture.
Initial conservative treatment consists of rest, ice, compression, elevation, activity modifications, offloading, orthotics and immobilization.8 Due to the poor blood supply to the sesamoids, healing can be delayed. If the symptoms persist for greater than six months and there is minimal improvement on serial radiographs, one should explore the surgical option of a sesamoidectomy.
Stress fracture of the metatarsals. Stress fractures are due to a repetitive strain on the bone with the bone resorption being faster than bone repair. Foot structure and biomechanics play large roles with metatarsal stress fractures. Of the patients I treat for metatarsal stress fractures, a majority have long second or third metatarsals, and a flexible flatfoot. Due to the more flexible nature of training barefoot, in CrossFit-specific shoes and minimalistic shoes, the incidence of metatarsal stress fractures is high. Patients usually have a diffuse swelling to the dorsal foot with pinpoint tenderness over the injured metatarsals. Radiographs may initially be negative and usually show a bone callus around three weeks after injury.
Protected weightbearing in a pneumatic walker and activity modification with low impact activities are the recommended treatment. Low vitamin D is a factor that we often overlook in patients with stress fractures. Therefore, it would be prudent to order a 25(OH)D blood test. I usually recommend at least 2,000 IU of vitamin D3 daily for my patients during healing with the goal to maintain athletes at around a 40 ng/mL vitamin D blood level. I will increase the vitamin D supplementation to 4,000 IU daily if the patient is at too low a level. Symptoms may resolve in six to eight weeks with a slow, gradual increase in weightbearing and high-impact activity over an additional two to four weeks. For those with structural or biomechanical issues, one should consider accommodation with shoe gear changes and custom orthotics.
Subungual hematomas. Subungual hematomas often occur in the big or the second toenail due to long second toes. They are common in CrossFit athletes due to the repetitive movements, ill-fitting shoes or blunt trauma to the toenail from dropping a weight on the toe. Once weightlifters finish a move, they will often release the barbell and let it drop to the ground. Carelessness may lead to the weight landing on the athlete’s own foot or that of a fellow athlete. The acute phase is often very painful.
Large hematomas may need drainage. One may need to perform a total nail avulsion to alleviate the pressure. I usually find the toe remains painful for about two weeks and then resolves. The nail may eventually loosen as the new nail grows in and falls off on its own.
Plantar fasciitis. Plantar fasciitis is the most common type of heel and arch pain in all athletes. The athlete will usually get a “bruised” feeling in the heel or a cramping in the arch with repetitive activities, such as jump rope, burpees or running. The pain arises at the medial plantar insertion and proximal medial band of the plantar fascia.7 CrossFit athletes may be more prone to plantar fasciitis due to their flexible footwear and lack of arch support in those who overpronate.
Conservative treatment for plantar fasciitis includes rest from high-impact activity, stretching, changes to footwear, custom orthotics and possible injection. In my practice, I frequently utilize extracorporeal shockwave therapy (ESWT) or extracorporeal pulse activation technology (EPAT), a low-energy, pulse-activated shockwave technology, as well.
Medial tibial stress syndrome. There are two types of shin splints, anterior and posterior, and both are common among CrossFit athletes. Anterior shin splints come from anterior tibial muscle weakness or tightness while posterior shin splints originate from the deep posterior muscle group, most commonly the flexor digitorum longus.8 The flexors usually activate more in CrossFit athletes who grab the floor with their toes in order to stabilize themselves on the ground during weightlifting. Jumping rope and a high rep count of box jumps may be aggravating factors. These athletes will usually complain of a more diffuse area of tenderness along the medial or anterior shin.
Treat shin splints with rest from high-impact repetitive activities until symptoms resolve, custom orthotics, shoe gear changes, stretching and strengthening of the tight or weak muscle groups, physical therapy, and compressive sleeves.
Achilles tendinitis and ruptures. The Achilles tendon is one of the most vulnerable tendons in the body due to its low blood supply. Injury to this tendon can be linked to overuse in almost every sport. The incidence of rupture is on the rise, especially in CrossFit athletes, due to the larger and stronger athletes, increased weight training, abrupt repetitive movements and popularity amongst middle-aged men and women.7 Overpronation and lack of flexibility in the ankle due to the tight gastrocnemius-soleus complex are two major factors. There is usually a prodrome of pain in the Achilles prior to rupture, which the athlete will often feel at the base of the squat when the Achilles is in full stretch. Achilles injuries may also occur during jump rope and burpees when kicking out into plank position. On clinical exam, there may be pinpoint tenderness and swelling in the Achilles tendon and pain with passive dorsiflexion and active plantarflexion.
Conservative treatment has variable results and will depend on the severity of the symptoms. Treatment of Achilles tendinitis can include immobilization, anti-inflammatories, heel lifts, stretching and strengthening and other physical therapy modalities. Treatment of acute ruptures in CrossFit athletes usually includes surgery.
How To Address The Needs Of CrossFit Athletes To Keep Training Despite Injuries
Most CrossFit coaches and athletes would tell you that they would prefer to train during treatment for their injury. I encourage this as it allows the athlete to stay in the habit of training, even if the training is rather easy during that time period.2 Athletes can accommodate most lower extremity injuries that require minimal weightbearing during treatment by focusing on the upper body. Flat and incline benches, seated dumbbell presses and dips, leg extensions, leg curls, and adductor work on machines are good alternatives.2
Athletes can work around other injuries by “scaling” the workouts. Scaling may occur by reducing the load and the repetitions in the workout. For example, rather than performing 50 squats with a 26-pound kettlebell, reduce it to 25 squats with a 13-pound kettlebell.8 Another way of scaling is to substitute the prescribed movement for an easier variation of the exercise.
Case Study: When A CrossFit Athlete Has A Sesamoid Fracture
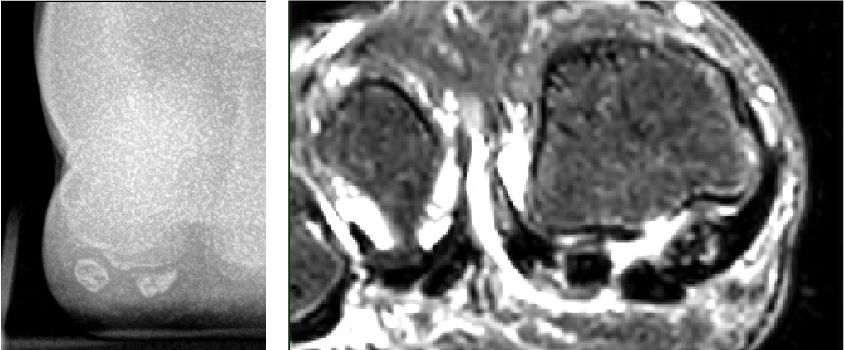
A 22-year-old female runner and CrossFit athlete presented after having pain in the ball of her right foot under her big toe for about three months. She did not recall any trauma but had pain with jumping rope, lunges and anytime she moved her big toe back and forth. The vague pain worsened to a sharp pain with any exercise and day-to-day activities. Initial X-rays revealed a fibular sesamoid fracture in three distinct fragments. The MRI confirmed a comminuted fibular sesamoid fracture with no avascular necrosis.
Initially, I had the patient weightbearing in a pneumatic walker with a dancer’s pad. After four months of conservative treatment and serial X-rays with minimal improvement, the patient went on to have a fibular sesamoidectomy. She had resolution of plantar symptoms in about two weeks and was back to full CrossFit exercise in four weeks. During her time of protected weightbearing, she was able to continue in CrossFit with upper body exercise, core work and the exercise bike.
Case Study: When A 47-Year-Old Athlete Has A Displaced Second Metatarsal Fracture
A 47-year-old male CrossFit athlete presented with pain and swelling to the dorsal left foot that he had experienced for two months prior to presenting to my office. The pain began as an ache dorsally in the foot when he was at the base of his squat and then progressed to a sharp pain with any weightbearing activity. He recalled the pain started after he felt fatigued during box jumps and did not make it up onto the box, falling forward and hitting his dorsal foot on the edge of the box. X-rays showed a displaced second metatarsal fracture with a butterfly fragment.
I recommended open reduction with internal fixation but the patient refused surgical treatment. The patient used a pneumatic walker and remained weightbearing. After three weeks, X-rays revealed minimal improvement. The patient admitted to continuing his weightbearing activities in his pneumatic walker. He wore a non-weightbearing, below-knee cast. The patient is still undergoing treatment.
In Conclusion
Most CrossFit-related injuries occur in the upper extremities, knees and the back, but there are a fair share of lower extremity injuries as well. Early diagnosis and treatment are pivotal as they are with most sports injuries. Scaling the workouts is the better choice, when possible, for athletes.
Dr. Robles is in private practice at Foot and Ankle Specialists of the Mid-Atlantic. She is an Associate of the American College of Foot and Ankle Surgeons.
References
- Weisenthal BM, Beck CA, Maloney MD, et al. Injury rate and patterns among CrossFit athletes. Orthop J Sports Med. 2014; 2(4): 1177.
- Starr B. Injury and opportunity. CrossFit Journal. 2014; 1-7.
- Glassman G. What is fitness? CrossFit Journal. 2002; 1-11.
- Widman R. A CrossFit Startup Guide: Part 1. CrossFit Journal. 2006; 20-26.
- Lauth I. Training shoes vs running shoes. Available at https://crossfitanaerobic.com/2012/02/01/training-shoes-vs-running-shoes/ . Published Feb. 1, 2012.
- Alloway RG, Alloway TP, Magyari PM, Floyd S. An exploratory study investigating the effects of barefoot running on working memory. Percept Mot Skills. 2016; 122(2):432-443.
- Clanton TO, McGarvey W. Athletic injuries in the soft tissues of the foot and ankle. In (Coughlin MJ, Mann RA, Saltzman CL, eds.): Surgery of the Foot and Ankle, Eighth Edition. Mosby, St. Louis, 2007, pp. 1425-1563.
- Hamilton WG, Bauman PA. Foot and ankle injuries in dancers. In (Coughlin MJ, Mann RA, Saltzman CL, eds.): Surgery of the Foot and Ankle, Eighth Edition. Mosby, St. Louis, 2007, pp. 1603-1640.
- Widman T. A CrossFit Startup Guide: Part 2. CrossFit Journal. 2009; 25-31.
For further reading, see “Key Insights On Managing CrossFit Injuries” in the March 2015 issue of Podiatry Today.

