


Addressing Jones Fractures in Athletes
Click here to view a related slideshow of Jones fracture patients.
As a longtime sports fan, I have seen how Jones fractures (Figure 1) can alter the success of a season and change the careers of athletes across professional and collegiate sports. The majority do return to their sport, but some do not, with multiple surgeries, nonunions or refractures complicating the course.

During my 30 years with the Army, I have fixed over 500 Jones fractures. I personally have only had 3 nonunions, but plenty of soldiers refractured. I also inherited a number of nonunions, refractures, and painful hardware cases over the years. Most recently, I have seen my share of Jones fractures in trainees who either resumed training or healed without surgical intervention.
This, frankly, surprised me. I had always been of the mindset that every athlete or soldier needs surgery in these cases. But over time, I have begun to question several paradigms related to Jones fractures. I feel that the nonunion rate for untreated/unprotected proximal diaphyseal fractures is likely overblown. I note that many of these fractures become asymptomatic sooner than such that these trainees can resume training. I question if we must keep patients non-weight-bearing for so long.
In my experience, I question the need for casting at all. I have seen my share of patients who heal despite not following crutch instructions. I have had my share of soldiers remove their cast days after application. Hundreds have shown up in Army boots in lieu of a cast boot. The numbers clearly show they can heal despite my recommendations. And, of course, I have had my share of refractures as a result of running too soon, or worse, being reinjured during training.
Despite the literature and Torg’s original articles in 1984 and 1990,1-2 in my experience, we don’t need to cast patients for 3 months. The proof is in the number of trainees who continue to train without intervention. Not every trainee receives a referral to our clinic.
After a review of all the Jones fractures at Ft. Leonard Wood over the past 7 years, only one-third were seen in our clinic. Out of the 70 cases identified within our X-ray database, only 14 underwent surgical repair during the past 7 years. That is not a high number especially considering the numbers we saw during my time at Ft. Liberty (formerly Ft. Bragg, NC) being over 400 cases in 10 years.
At Ft. Leonard Wood, we have only seen 3 true stress fractures of the fifth metatarsal with 67 of 70 military cases having a well-defined and documented injury. Whether it be during training or via sports injury, there was always a specific injury, patients felt a pop, had immediate pain and eventual swelling/bruising. Why some patients did not receive a referral is unclear. Without a systematic records review, one can only assume that the soldiers simply had reduced pain and continued training or separated from the military prior to having any follow-up. Of the 14 soldiers treated with surgery, all healed and resumed training within 3 months.
Despite years of success, every couple of years, whether it be surgeon or equipment company driven, a new surgical option arises. We all have seen the pendulum swing to and from screws, plates, solid screws, fully threaded screws, hook plates, plantar plates, headless screws and even external fixation.3-7 Across over 500 cases, to date, I have never used a plate for acute fractures. I have always utilized a percutaneous screw or external fixation for my acute fractures. Jones fractures are stable and rarely displace, so why open reduce and plate something that doesn’t need a reduction? In my experience, one benefit of these percutaneous approaches is potential avoidance of resultant sural neuritis. I have utilized open plating and grafting for nonunion cases, but even that is very rare for me today.
Do I personally think one particular type of screw is better? As I look back at cases that I originated and those I inherited with complications, I have seen nonunions and painful hardware with just about every technique. I have seen hardware breakage with solid and cannulated screw types as well. Additionally, I have seen cases heal despite malreduction or poor hardware placement. With no clear patterns emerging, I think you should use what is comfortable for you as the surgeon. Every surgeon has their own technique or flair that can work.
After 500 of my own cases and maybe another 150 revision or inherited cases, I have come up with some basic recommendations, which I will share here.
Always give your patients the choice of surgery versus conservative therapy. I am far less insistent when dealing with a unicortical fracture versus a bicortical fracture. If I see a bicortical or gapped fracture, I then strongly push for surgery or 3 months of casting. Despite advocating for surgery for all my soldiers and athletes, in nonathletes I try to give them much more say in deciding on how they would like to treat their injury. I have found the majority of cases will heal, in my experience, in much higher frequency than what the literature quotes.
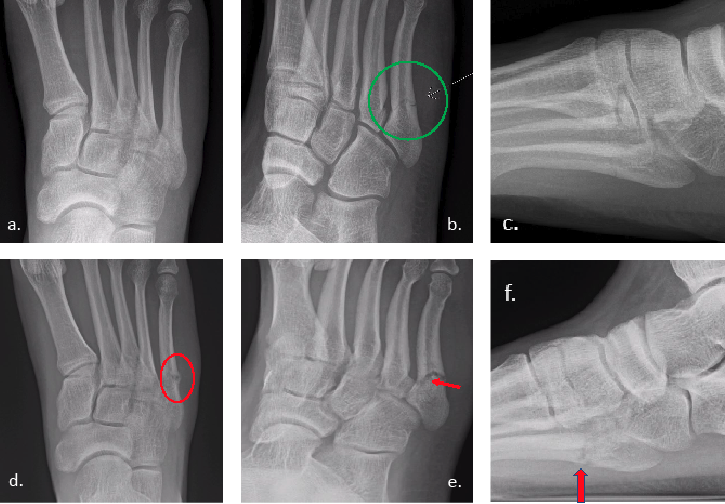
It is important to recognize the age of the fracture. I have noted radiologists routinely mistaking acute fractures for stress fractures based on location. I’ve heard surgeons tell patients that their fracture isn’t healing based on a 6-week-old injury, due to signs of bone resorption, which is normal sign of healing. Unfortunately, not all Jones fractures get X-rayed the same week, let alone within a month of the injury, so they may present already showing signs of radiographic healing. Either way, I find it is common that one may overread the imaging. See Figures 2-3.

Any screw utilized should have intramedullary purchase. Far too often in athletes, I find this does not happen. I also find screws of 4.5mm or greater are best, depending on the width of the metatarsal shaft. With digital radiology systems, surgeons can pre-plan and measure the canal in at least 2 views to ensure adequate intramedullary purchase. See Figure 4.
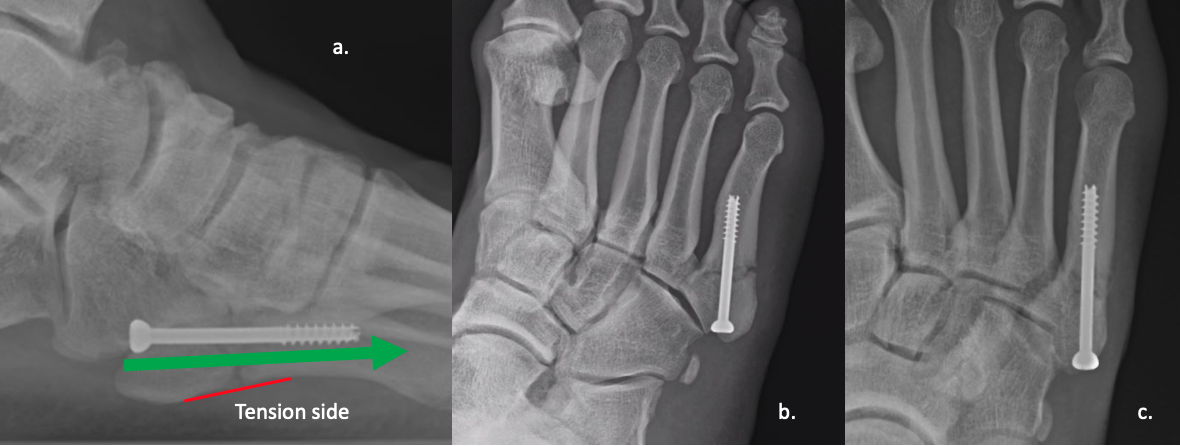
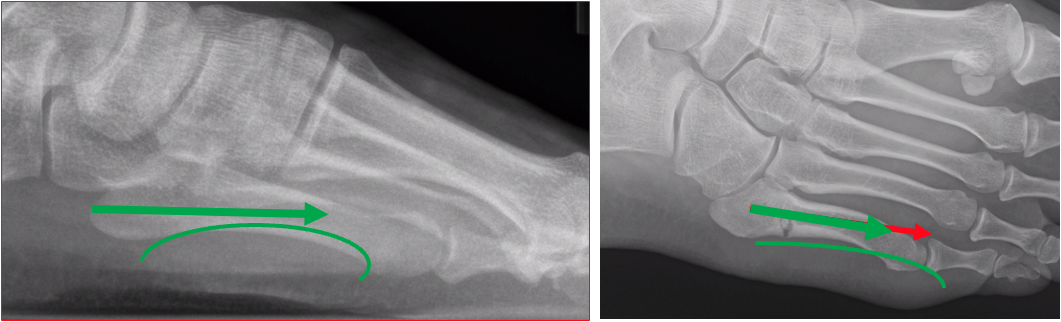
Keep the screw length as long as you can, unless you have a plantar curve on the lateral view. In my observation, too long a screw will distract the fracture with cases that have a plantar curve. Average screw length range from 50-55mm, in my experience. See Figure 5.
Starting position is crucial to avoid fifth metatarsal-cuboid joint pain and/or malreductions. Utilizing headless screws will give you far more freedom for start points.
The use of stem cells, platelet-rich plasma, amniotic tissue, or even bone marrow aspirate are excellent options to stimulate the fracture and potentially also reduce post-operative pain. I have used amniotic tissue injections since 2015, and PRP to stimulate delayed unions for over 15 years. I’ve seen colleagues use bone marrow aspirate from the calcaneus. As a result, I feel this is a significant contributor to my lack of nonunions.
Allow early weight-bearing as soon as the patient is able. There is no need to have protracted time on crutches. For years I have allowed soldiers to walk at a week, and in some cases sooner, especially if the reduction was a few weeks post-injury.
Do not clear patients for running or sports until the plantar cortex heals. I have had my share of refractures the first time they ran. The pain-free unhealed fracture is particularly precarious.
Refracture is more of a product of their activity. Just because patients are pain-free and radiographically healed doesn’t mean that they can’t or won’t refracture.
In Conclusion
Overall, Jones fractures are simple to manage, but what makes them challenging, I find, is that patients rarely have long-lasting pain. This lack of pain often leads to reinjury by resuming sports and/or running too soon. Patients need to receive medical clearance to resume these activities after proper imaging. Like with all athletes and soldiers, we as surgeons can speed up their recovery, we can eliminate the need for crutches or even casting, but their return to sports must be cautioned. As so many athletes have experienced, reinjury is a huge concern and realistically, there is little we can do prevent this. Sports and the military are contact sports. People can and will get hurt. As I tell my soldiers, I am here to fix you, so go have fun.
A. Douglas Spitalny, DPM is a Staff Podiatrist at General Leonard Wood Army Hospital in Ft. Leonard Wood, MO.
References
- Torg JS, Balduini FC, Zelko RR, Pavlov H, Peff TC, Das M. Fractures of the base of the fifth metatarsal distal to the tuberosity. Classification and guidelines for non-surgical and surgical management. J Bone Joint Surg Am. 1984;66(2):209–214
- Torg JS. Fractures of the base of the fifth metatarsal distal to the tuberosity. Orthopedics. 1990;13(7):731–737.
- Chopra A, Anastasio AT, Fletcher AN, Tabarestani TQ, Sharma A, Parekh SG. Short-term outcomes of Jones-specific implant versus intramedullary screw and plate fixation for proximal fifth metatarsal fractures. J Foot Ankle Surg. 2023;62(5):862-867.
- Umbel BD, Sharpe BD Jr, Hockman T, Philbin TM. Early results of a novel intramedullary fixation device for proximal fifth metatarsal fractures. Foot Ankle Orthop. 2022;7(1):2473011421S00476.
- Albloushi M, Alshanqiti A, Qasem M, Abitbol A, Gregory T. Jones type fifth metatarsal fracture fixation in athletes: A review and current concept. World J Orthop. 2021;12(9):640-650.
- Duplantier NL, Mitchell RJ, Zambrano S, et al. A biomechanical comparison of fifth metatarsal Jones fracture fixation methods. Am J Sports Med. 2018;46(5):1220-1227.
- Mitchell RJ. Treatment of proximal fifth metatarsal fractures and refractures with plantar plating in elite athletes. Foot Ankle Int. 2018;39(12):107110071879183.
Additional References
- O’Malley M, DeSandis B, Allen A, Levitsky M, O’Malley Q, Williams R. Operative treatment of fifth metatarsal Jones fractures (Zones II and III) in the NBA. Foot Ankle Int. 2016 May;37(5):488-500.
- Begly JP, Guss M, Ramme AJ, Karia R, Meislin RJ. Return to play and performance after Jones fracture in National Basketball Association athletes. Sports Health. 2016 Jul;8(4):342-6.
- Ficek K, Kedra N, Skowronek R, Kluczniok K, Strózik M, Gwiazdon P, Hajduk G. The fifth metatarsal bone fracture in athletes - modalities of treatment related to agility in soccer players. J Hum Kinet. 2021 Jul 28;79:101-110.






