


A Closer Look at the Syndesmotic Complex in Rotational Ankle Fractures
As our understanding of the syndesmotic complex advances, so do emerging techniques and fixation constructs. A complete understanding of the distal tibiofibular joint will afford the surgeon a better appreciation of how these ligaments behave in both uninjured and injured patients. This article will review the syndesmotic complex and additional options for surgical stabilization.
The Syndesmotic Complex: What You Should Know
 The syndesmotic complex is a dense, fibrous joint composed of 4 main ligaments: the anterior inferior tibiofibular ligament (AITFL), the interosseous ligament (IO), the posterior inferior tibiofibular ligament (PITFL), and the deep transverse ligament. Traditional teaching stated that the posterior ligaments served as the primary stabilizers of this complex; however, previously published studies evaluated the ligaments with lateral translation testing only.1 Clanton and colleagues recently re-evaluated the syndesmotic complex, finding that the AITFL was the strongest ligament out of the syndesmotic complex when testing for resistance of external rotation forces rather than lateral translation.2 Injuries associated with the syndesmotic complex typically result from lower energy forces, subjecting the tibiofibular and ankle joints to an external rotation force. The external rotation energy will result in an “open book” disruption from anterior-to-posterior through the syndesmosis. In the author’s experience, one can liken this event to a “peel-back” injury disrupting the AITFL first, followed by the IO ligament, then the PITFL with conventional rotational ankle fractures. Intraoperative assessment with direct visualization while performing a dorsiflexion and external rotation stress test, combined with multiplanar fluoroscopy, is paramount to ensure appropriate syndesmotic evaluation.
The syndesmotic complex is a dense, fibrous joint composed of 4 main ligaments: the anterior inferior tibiofibular ligament (AITFL), the interosseous ligament (IO), the posterior inferior tibiofibular ligament (PITFL), and the deep transverse ligament. Traditional teaching stated that the posterior ligaments served as the primary stabilizers of this complex; however, previously published studies evaluated the ligaments with lateral translation testing only.1 Clanton and colleagues recently re-evaluated the syndesmotic complex, finding that the AITFL was the strongest ligament out of the syndesmotic complex when testing for resistance of external rotation forces rather than lateral translation.2 Injuries associated with the syndesmotic complex typically result from lower energy forces, subjecting the tibiofibular and ankle joints to an external rotation force. The external rotation energy will result in an “open book” disruption from anterior-to-posterior through the syndesmosis. In the author’s experience, one can liken this event to a “peel-back” injury disrupting the AITFL first, followed by the IO ligament, then the PITFL with conventional rotational ankle fractures. Intraoperative assessment with direct visualization while performing a dorsiflexion and external rotation stress test, combined with multiplanar fluoroscopy, is paramount to ensure appropriate syndesmotic evaluation.
What is the Role of Rigid Screw Fixation?
Historically, rigid screw fixation stabilized the syndesmotic complex with various debates ensuing regarding the size of the screws, how many screws, and 3 versus 4 cortices of engagement. Although this construct, in my experience, can provide excellent stability to the syndesmotic complex, complications such as screw breakage, malreduction, decreased ankle joint range of motion, and the potential requirement for additional operations are not uncommon observations. With this in mind, I find rigid screw fixation may be necessary for specific fracture patterns and patient populations, such as injuries in older patients and complicated patients with diabetes and peripheral neuropathy.
Concerning Consequences of Malreduction
One of the most dreaded complications observed with rigid screw fixation of the syndesmosis is malreduction. Gardner and team, in 2006, evaluated 25 ankle fractures undergoing rigid screw fixation followed by postoperative computed tomography (CT) examination.3 The authors observed a 52% rate of fibular incongruity within the incisura on postoperative CT scans. In 77% of the ankles with the incongruity of the fibula, the posterior gap was larger than the anterior gap, indicating internal rotation or anterior translation of the fibula was occurring within the incisura.3 Although it is not clear the functional or long-term sequelae of this occurrence with malreduction, further studies are important to provide clarity on this observation. Of note, surgeons used a large point-to-point clamp tenaculum to reduce the syndesmotic complexes in this study.3 Research has shown that using an improperly placed and compressed tenaculum is likely the underlying culprit of malreduction.4 Preferred technique involves direct inspection of the syndesmosis, followed by evacuation of invaginated AITFL within the incisura. Then, one can manually reduce and temporarily stabilize the fibula with a Kirschner wire if needed.
Flexible Syndesmotic Fixation and Augmentation Options to Consider
 Once the fibula is properly seated within the incisura, definitive syndesmosis stabilization can occur. Flexible suture buttons and/or suture with screw fixation devices continue to emerge within foot and ankle markets. The exact amount of tension required to properly stabilize the fibula within the incisura is still unclear. Morellato and coworkers, in the Journal of Orthopaedic Trauma, evaluated 10 cadaveric specimens stabilized with one suture button and tension loads of 4, 8, and 12 kg.5 They then obtained and reviewed postprocedure CT scans. The authors recorded over-compression in the 8 and 12 kg groups, but the incidence of overcompression was less in the 4 kg group. It is unclear if overcompression of the syndesmotic complex, despite anatomic reduction, results in long-term complications. Albeit, the goal remains to anatomically restore the ankle joint and syndesmosis to near normal following injury. Intraoperative devices to objectively quantify the amount of compression delivered could potentially prevent over-compression; however, such devices are not currently available. An anatomically stabilized ankle will provide patients with the best possible functional outcome and mitigate long-term post-traumatic degenerative joint disease.
Once the fibula is properly seated within the incisura, definitive syndesmosis stabilization can occur. Flexible suture buttons and/or suture with screw fixation devices continue to emerge within foot and ankle markets. The exact amount of tension required to properly stabilize the fibula within the incisura is still unclear. Morellato and coworkers, in the Journal of Orthopaedic Trauma, evaluated 10 cadaveric specimens stabilized with one suture button and tension loads of 4, 8, and 12 kg.5 They then obtained and reviewed postprocedure CT scans. The authors recorded over-compression in the 8 and 12 kg groups, but the incidence of overcompression was less in the 4 kg group. It is unclear if overcompression of the syndesmotic complex, despite anatomic reduction, results in long-term complications. Albeit, the goal remains to anatomically restore the ankle joint and syndesmosis to near normal following injury. Intraoperative devices to objectively quantify the amount of compression delivered could potentially prevent over-compression; however, such devices are not currently available. An anatomically stabilized ankle will provide patients with the best possible functional outcome and mitigate long-term post-traumatic degenerative joint disease.
Another area of debate concerning flexible fixation is the number of suture button devices required to properly stabilize the syndesmosis. Clanton and colleagues, in 2017, evaluated 3 constructs in the cadaveric model: screw fixation, one suture button, and two divergent suture buttons.6 The authors found that one suture button alone demonstrated the largest degree of posterior sagittal translation of the fibula within the incisura. They concluded that one suture button alone might not provide sufficient resistance to sagittal translation.6
To obviate the potential for the persistence of further instability in the sagittal plane, surgeons may elect to either place two suture buttons or directly repair the AITFL. It can often be challenging to place two suture buttons due to the location of the fibular fracture or lag screw, if previously inserted. To avoid violating another drill hole through the fracture site or weakening the bone around the lag screw, direct augmentation of the AITFL continues to grow in popularity. The surgeon can loop suture material through the lateral fibular hardware, inserting it into the Chaput tubercle of the distal lateral aspect of the tibia, securing it with a PEEK or bio-composite screw (see photo to left). This construct will directly stabilize the interosseous component of the syndesmosis and the AITFL, resulting in a multi-ligament augmentation.
This Author’s Preferred Approach
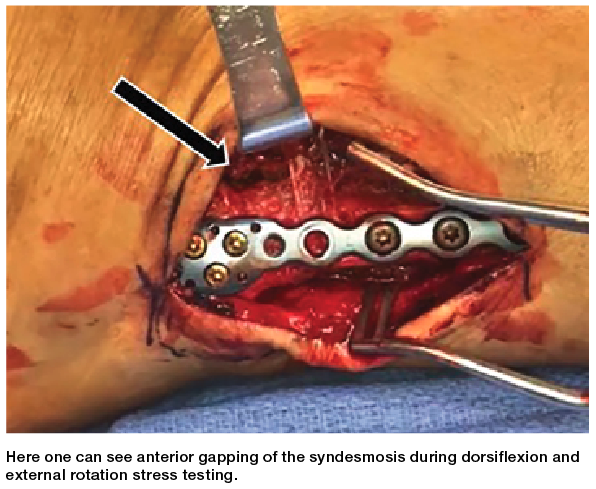
Once stabilizing the osseous components with plates and screws, one evaluates the syndesmosis no matter the mechanism of injury. The surgeon can perform a dorsiflexion, external rotation stress test by stabilizing the distal end of the tibia and externally rotating the hindfoot while dorsiflexing the ankle. It is important to note that direct visualization is of utmost importance during this exam, as radiographic parameters may not be reliable.7
Utilizing an Army-Navy retractor to retract the superior flap and ensuring no osseous or soft tissue entrapment within the incisura will aid in the proper fibular reduction. Then, the surgeon manually reduces the syndesmosis by applying direct pressure to the lateral fibula in an approximately 20-degree fashion. A Kirschner wire can temporarily stabilize the reduction if the syndesmosis is grossly unstable; otherwise, the suture button device will properly seat the fibula during tensioning. A repeat stress test evaluates for residual anterior gapping, which would result in AITFL augmentation as described above.
In Conclusion
Our goal as foot and ankle surgeons is to restore the ankle and syndesmotic complex to the best of our ability in these fractures. Direct inspection of the syndesmosis and clearing debris within the incisura will mitigate malreduction. Not all fracture patterns and patient populations will require dynamic syndesmotic stabilization using flexible suture button constructs. Applying one’s understanding of the syndesmotic complex and how this structure becomes disrupted with rotational ankle fractures can contribute to the best possible outcomes for our patients.
Dr. Monaco practices at Premier Orthopaedic and Sports Medicine in West Chester, PA. He is a Diplomate of American Board of Foot and Ankle Surgeons, Faculty for the Penn-Presbyterian Podiatry Residency in Philadelphia, and Faculty for the Phoenixville Hospital Podiatry Residency in Phoenixville, PA.
References
1. Ogilvie-Harris DJ, Reed SC, Hedman TP. Disruption of the ankle syndesmosis: biomechanical study of the ligamentous restraints. Arthroscopy. 1994;10(5):558-560.
2. Clanton TO, Williams BT, Backus JD, et al. Biomechanical analysis of the individual ligament contributions to syndesmotic stability. Foot Ankle Int. 2017;38(1):66-75.
3. Gardner MJ, Demetrakopoulos D, Briggs SM, Helfet DL, Lorich DG. Malreduction of the tibiofibular syndesmosis in ankle fractures. Foot Ankle Int. 2006;27(10):788-792.
4. Westermann RW, Rungprai C, Goetz JE, Femino J, Amendola A, Phisitkul P. The effect of suture-button fixation on simulated syndesmotic malreduction: a cadaveric study. J Bone Joint Surg Am. 2014:96(20):1732-1738.
5. Morellato J, Louati H, Bodrogi A, et al. The effect of varying tension of a suture button construct in fixation of the tibiofibular syndesmosis—evaluation using stress computed tomography. J Orthop Trauma. 2017;31(2):103-110.
6. Clanton TO, Whitlow SR, Williams BT, et al. Biomechanical comparison of 3 current ankle syndesmosis repair techniques. Foot Ankle Int. 2017;38(2):200-207.
7. Beumer A, van Hemert WLW, Neiseing R, et al. Radiographic measurement of the distal tibiofibular syndesmosis has limited use. Clin Orthop Rel Res. (1976-2007) 2004;423:227-234.






