


A Guide to Surgical Technique for Harvesting Calcaneal Bone Marrow Aspirate
The practice of utilizing bone marrow aspirate (BMA) is becoming a cornerstone in foot and ankle surgeries, aimed at enhancing the healing of conditions such as joint cartilage degeneration, various types of fusions, fracture repair, and nonunion repairs.1–5 Although the iliac crest has traditionally been preferred for BMA harvest due to its rich concentration of osteoprogenitor cells,6 recent studies, along with our institutional practices, have identified the calcaneus and tibia as viable and convenient alternatives.7
At our institution, we frequently utilize BMA in primary and revisional pedal arthrodesis procedures. The implementation of bone marrow aspirate in our procedures has significantly enhanced fusion outcomes, effectively reducing our personal fusion failure rate to zero.
Bone marrow is beneficial, containing an array of factors including platelet-derived growth factor, vascular endothelial growth factor, fibroblast growth factor, insulin-like growth factor, granulocyte-macrophage colony-stimulating factor, bone morphogenetic protein, and interleukins.6,8 Consequently, the bioactive components in BMA concentrate (BMAC) can facilitate healing by reducing cell death and inflammation, and by promoting cell proliferation, differentiation, and angiogenesis. While the efficacy of BMA is well-documented in orthopedic literature for spine and hip surgeries,1,9,10 reports are less extensive for foot and ankle arthrodesis procedures.

It has been found in animal models of long bone healing that BMAC significantly improves bone formation and accelerates healing compared to controls, lending further support to BMAC’s role in orthopedic applications. A study by Gianakos and colleagues systematically reviewed the efficacy of BMAC containing bone mesenchymal stem cells (BMSCs) for treating segmental defects in animal long bones.11 The comprehensive review found that BMAC significantly increased bone formation, evidenced by radiographic improvement in 100% of the studies included. Additionally, 90% of the studies observed substantial acceleration in bone healing through histologic assessment, while 81% reported increases in bone area on micro-computed tomography. The authors concluded that BMAC offers considerable benefits for bone healing in animal models and provides a proof-of-concept for treating similar bone defects.

We utilize a bone marrow harvesting technique similar to that previously described in literature.3,7,12 Prior studies have discussed the optimal donor site location and volume of bone marrow aspirate; however, there is no general consensus.13 Hyer and colleagues looked at the presence of mesenchymal stem cell concentrations in bone marrow aspirate samples from the iliac crest, tibial, and calcaneus. They concluded that osteoblastic progenitor cells are available in the iliac crest, proximal aspect of the tibia, and calcaneus. However, the iliac crest provided the highest yield of osteoblastic progenitor cells.11 At our institute, we harvest from the calcaneus, but when that is not feasible due to the surgery’s location, we opt for the distal tibia, achieving similar success rates and, in our experience, encountering no complications. These findings emphasize the potential of calcaneal-derived BMA in enhancing healing and recovery, while maintaining a low-risk profile.5 This report provides surgeons with a step-by-step guide for the safe and efficient harvesting of bone marrow aspirate concentrate.

A Closer Look at the Authors’ Surgical Technique
This surgical technique description focuses on the calcaneal extraction method from the ipsilateral limb. The procedure is done in the operating room and it begins with the standard preparation of the foot, followed by draping. Then, we carry out the aspiration process before exsanguination.

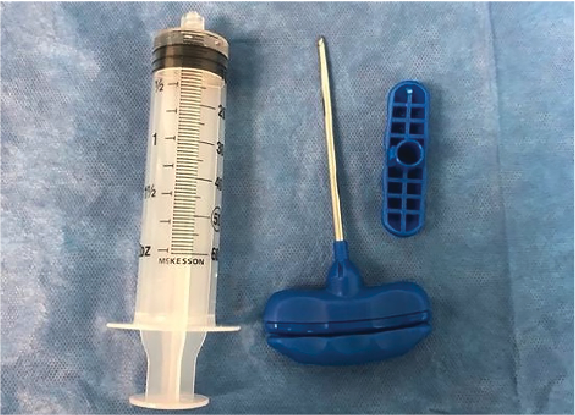
For the aspiration, we employ an 8G Jamshidi needle along with a 60 mL syringe. With the help of a skin marker, we delineate a line on the lateral side of the calcaneus, extending from the anterior insertion of the Achilles tendon to the origin of the plantar fascia. The midpoint of this line is marked as the needle entry site, taking care to avoid the sural nerve.

We then insert the needle through the lateral calcaneal wall, after which we remove the trocar, and attach the syringe to the needle, applying continuous retrograde pressure to extract 30cc of bone marrow aspirate. Once withdrawing the needle, we close the puncture with a single 4-0 nylon suture. Centrifuging the aspirate for 15 minutes usually results in 5-6 cc of BMAC to inject into the surgical site.

After preparing the joint, we inject half of the BMAC into it. Upon securing the joint with the necessary fixation, we then administer the remaining BMAC into the joint capsule. The procedure is completed with the suturing of subcutaneous tissues and skin. Following surgery, patients are in a below-knee cast and instructed to refrain from bearing weight on the operative limb.
Dr. Naei is a staff physician at University Foot and Ankle Institute.
Dr. Baravarian is Director and Fellowship Director at University Foot and Ankle Institute.
References
1. Kim GB, Seo MS, Park WT, Lee GW. Bone marrow aspirate concentrate: its uses in osteoarthritis. Int J Molec Sci. 2020; 21(9):3224. https://doi.org/10.3390/ijms21093224
2. Fortier LA, Potter HG, Rickey EJ, et al. Concentrated bone marrow aspirate improves full-thickness cartilage repair compared with microfracture in the equine model. J Bone Joint Surg Am. 2010 Aug 18;92(10):1927-37. doi: 10.2106/JBJS.I.01284. PMID: 20720135.
3. Li C, Kilpatrick CD, Smith S, et al. Assessment of multipotent mesenchymal stromal cells in bone marrow aspirate from human calcaneus. J Foot Ankle Surg. 2017;56(1):42-46. doi:10.1053/j.jfas.2016.09.006
4. Roukis TS, Hyer CF, Philbin TM, Berlet GC, Lee TH. Complications associated with autogenous bone marrow aspirate harvest from the lower extremity: an observational cohort study. J Foot Ankle Surg. 2009 Nov-Dec;48(6):668-71. doi: 10.1053/j.jfas.2009.07.016. Epub 2009 Aug 26. PMID: 19857823.
5. Encinas R, Phillips T, Hall S, Jackson JB, Gonzalez T. Outcomes and complications after bone marrow aspirate harvest from the calcaneus. Foot Ankle Orthop. 2023;8(3). doi:10.1177/24730114231194056
6. Cucchiarini M, Venkatesan JK, Ekici M, Schmitt G, Madry H. Human mesenchymal stem cells overexpressing therapeutic genes: from basic science to clinical applications for articular cartilage repair. Biomed Mater Eng. 2012;22(4):197-208. doi: 10.3233/BME-2012-0709. PMID: 22785363.
7. Schweinberger MH, Roukis TS. Percutaneous autologous bone marrow harvest from the calcaneus and proximal tibia: surgical technique. J Foot Ankle Surg. 2007;46(5):411-414. doi:10.1053/j.jfas.2007.05.009
8. Cassano JM, Kennedy JG, Ross KA, Fraser EJ, Goodale MB, Fortier LA. Bone marrow concentrate and platelet-rich plasma differ in cell distribution and interleukin 1 receptor antagonist protein concentration. Knee Surg Sports Traumatol Arthrosc. 2018 Jan;26(1):333-342. doi: 10.1007/s00167-016-3981-9. Epub 2016 Feb 1. PMID: 26831858.
9. Johnson, Robert G. MD. Bone marrow concentrate with allograft equivalent to autograft in lumbar fusions. Spine. 2014; 39(9):695-700.. | DOI: 1097/BRS.0000000000000254
10. Hernigou P, Trousselier M, Roubineau F, Bouthors C, Chevallier N, Rouard H, Flouzat-Lachaniette CH. Stem cell therapy for the treatment of hip osteonecrosis: a 30- year review of progress. Clin Orthop Surg. 2016 Mar;8(1):1-8. https://doi.org/10.4055/cios.2016.8.1.1
11. Gianakos A, Ni A, Zambrana L, Kennedy JG, Lane JM. Bone marrow aspirate concentrate in animal long bone healing. J Orthop Trauma. 2016;30(1):1-9. doi:10.1097/bot.0000000000000453
12. Schade VL, Roukis TS. Percutaneous bone marrow aspirate and bone graft harvesting techniques in the lower extremity. Clin Podiatr Med Surg. 2008;25(4):733-742. doi:10.1016/j.cpm.2008.05.001
13. Oliver K, Awan T, Bayes M. Single- versus multiple-site harvesting techniques for bone marrow concentrate: evaluation of aspirate quality and pain. Orthop J Sports Med. 2017 Aug 29;5(8):2325967117724398. doi: 10.1177/2325967117724398. PMID: 28890905; PMCID: PMC5580846.






