


Where Do Orthotics Fit Into A Comprehensive Plan For Plantar Plate Pathology?

Once clinicians identify a patient with plantar plate pathology, how might they incorporate orthotics into their treatment regimen? What modifications might they choose? Does the stage of pathology impact decision making? In this column, the panelists share their algorithms for working up plantar plate pathology, including where orthotics and other biomechanical interventions play a role in management.
Q: What diagnostic pearls do you find helpful when addressing plantar plate pathologies?
A:
Richard Blake, DPM, starts by stressing that plantar plate injuries, typically to the second MTPJ, but sometimes the third, need serious attention.
“You have to treat plantar metatarsal pain, acute or chronic, with a “rule out approach” to these often-confusing plantar plate injuries, he says. “Of course the Lachman test in digit neutral, and where the digit is slightly dorsiflexed, as per Richard Bouché, DPM, in Seattle, WA, is vital diagnostically. I feel all suspected or confirmed plantar plate injuries should have Budin splints for walking, and FixToe® (Herbitas Laboratorios, Spain) or DARCO® digital splints for sleeping.”
Jenny Sanders, DPM says that in her diagnostic process for any suspected plantar plate injury, she finds imaging is key to both staging and treatment determinations.
“In addition to radiographs, we use musculoskeletal ultrasound and magnetic resonance imaging (MRI) to diagnose plantar plate injuries,” she says. “It is not uncommon to find a second intermetatarsal neuroma in addition to plantar plate degeneration or tear, which when treated separately, completely eliminates a patients painful forefoot symptoms.”
Q: How do orthotics fit into your overall algorithm for treating plantar plate pathology? What is your stepwise process for evaluating and managing these types of cases?
A:
Dr. Kirby shares that on an initial visit for a patient with a suspected plantar plate tear, his goals of treatment are to reduce the compression and tension stresses that are acting on the plantar plate, so the patient can: become more comfortable during weight-bearing activities; experience reduced plantar forefoot swelling; and heal the plantar plate tear itself more rapidly.
“I will first suggest plantar forefoot icing therapy, 20 minutes, twice a day, to help reduce the plantar edema often associated with more acute plantar plate tears,” he says. “In addition, I will add an accommodative pad into the shoe and/or shoe insole/sock liner for the affected MTPJ to reduce the ground reaction force acting on the plantar plate.”
He also adds digital plantarflexion taping to the affected digit as a modality to reduce the tension stress acting on the plantar plate during gait and directs them toward his YouTube video on the specific digital plantarflexion taping technique.1 Using this video resource, he instructs patients to perform this helpful technique on themselves on a daily basis. He suggests patients seek out a highly-cushioned, rocker-soled athletic shoe, such as the HOKA® One One Bondi, to wear in order to relieve both the compression and tension stress on the plantar plate injury.
“For standing and walking activities at home, I also recommend the purchase of a highly cushioned sandal, such as OOFOS® sandals, and to avoid barefoot walking, to reduce the compression stress on the plantar plate.”
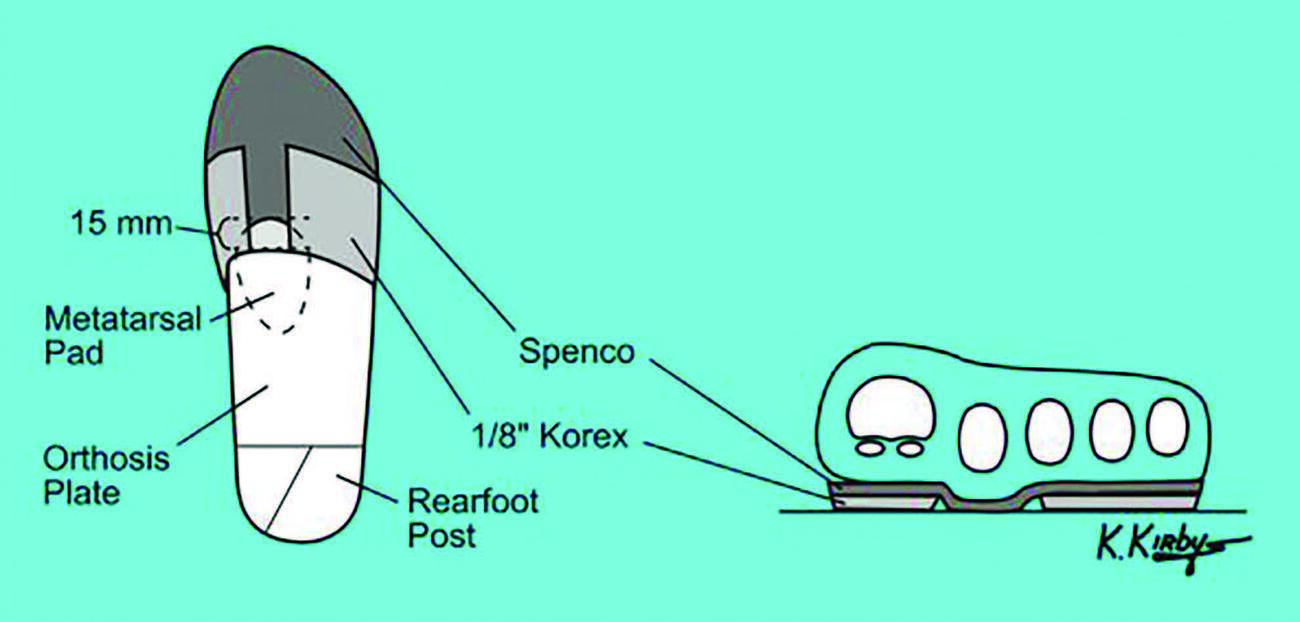
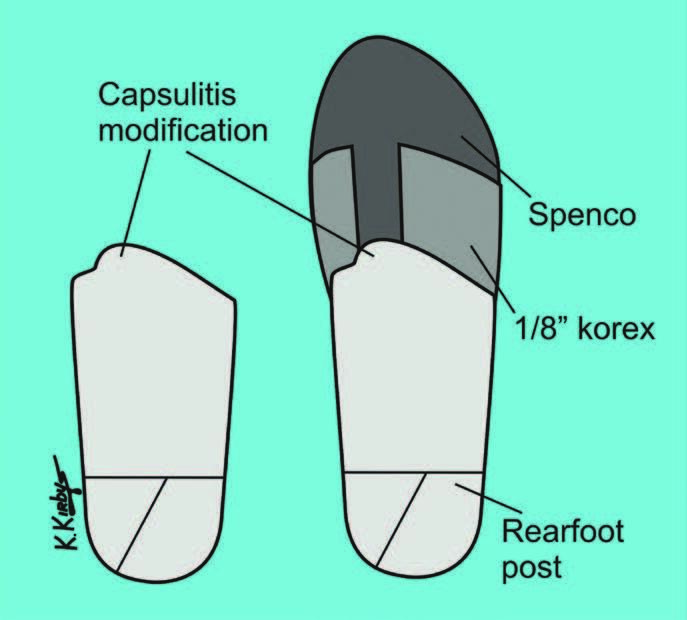
Orthotics come into play for Dr. Kirby when the patient does not progress well with the aforementioned treatments, or if the plantar plate injury is more significant. In these cases, he orders full-length custom foot orthoses with a three-to-six mm thick neoprene or PPT top cover, a thicker anterior edge (three-to-four mm thick), a metatarsal pad and an accommodation (three-to-five mm thick Korex) for the affected MTPJ in the forefoot extension of the orthosis (see left figure above). In addition, he offers an extra-articular injection of a corticosteroid solution to the patient if they have persistent plantar swelling that does not responding to the above-mentioned conservative therapies.
“I recommend plantar plate repair surgery if the patient has not made good progress with these treatments, even though I find surgery is not often necessary when one executes the above-listed, stepwise approach to conservative care for the patient with plantar plate pathology,” he says.
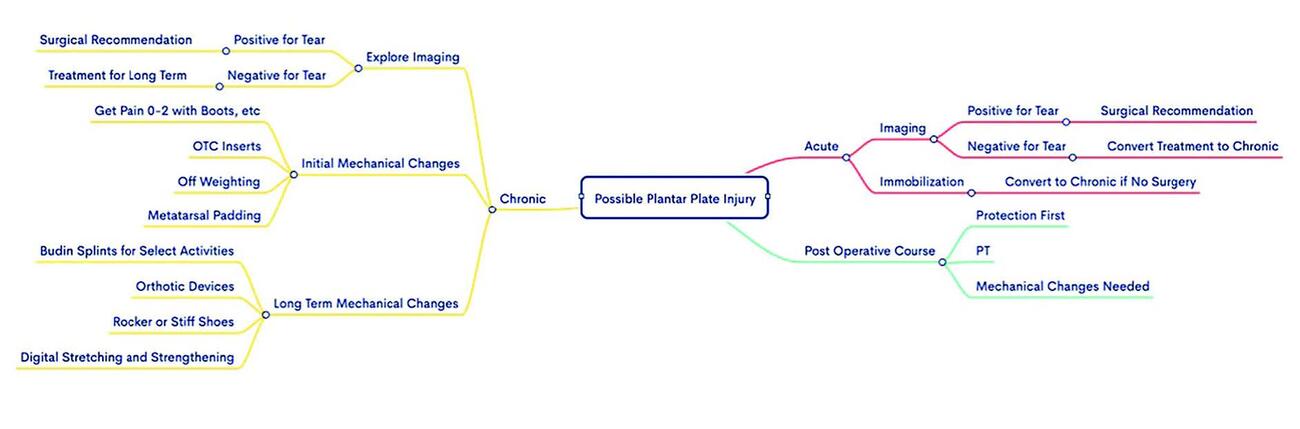
Dr. Blake shares a schematic for his stepwise approach to plantar plate issues, dividing it into acute, chronic, and postoperative concerns (see figure on page 18). When it comes to the importance of orthotic devices in treating plantar plate pathology, Dr. Blake feels they are crucial when attempting to avoid surgery, or simply in an effort to make the patient more comfortable. Additionally, he feels they can play a role following surgery to decrease the load on the involved joint for several years, at least. He shares that in his experience, plantar plate-specific modifications to standard custom orthotic devices may include:
• intrinsically supporting all forefoot deformities as best as one possibly can (he finds full forefoot valgus support is easier to accomplish than full forefoot varus support);
• capturing a high intrinsic metatarsal arch in pes cavus feet;
• requesting that the laboratory leave the end of the plastic just before the metatarsal heads (typically a longer orthotic device);
• not skiving the distal edge of the orthotic device; and
• extrinsic orthotic modifications, including off-weighting the metatarsal head with forefoot extensions distal to the plastic and a variety of soft metatarsal pads to hold the involved metatarsal superiorly.
Initially, he adds, when the patient is antalgic, one can attempt to use a full-length rigid insert to immobilize the MTPJs.
“I like to dispense from my office SOLE™, PowerStep®, or Pure Stride over-the-counter inserts at the first visit, which I can easily add or subtract from,” he explains.
Dr. Blake goes on to stress the importance of remembering that plastic functional foot orthotic devices immobilize and support the metatarsals, but actually create motion at the MTPJs. This, he says, is why Morton’s extensions become necessary at times when he finds functional foot orthotic devices actually contribute to or increase pain at the first MTPJ after dispensing the devices.
“You are creating motion, when the injury dictates less motion for a while,” says Dr. Blake. “This concept is the same for plantar plate injuries. Due to the severity or the injury, or the need for immediate or planned elective surgery, you may need to adjust treatments at each visit. At times you immobilize more, and times you just support and off-weight some. For example, custom orthotic devices with Budin splints for immobilization is a common recipe. Yet, sometimes, patients will only need the Budin splint when jogging up hills and one can predict more likelihood of bending.”
Jenny Sanders, DPM relates that as someone in a non-surgical, sports medicine practice, shoes, taping, and custom orthotics are a mainstay of treatment for plantar plate injuries. Should conservative methods prove insufficient in eliminating painful symptoms, then she says she makes a referral for surgical correction and repair.
First, when it comes to shoes, she says that determining the correct heel-to-ball length is critical to ensure proper MTPJ loading and weight-bearing in footwear. A previous blog Dr. Sanders wrote outlines how one may go about obtaining this measurement.2 Similarly to Dr. Kirby, she advises patients on the best types of shoes, including an inflexible forefoot sole, as an essential component to minimize forefoot dorsiflexion.
“I recommend shoe models including HOKA One One Bondi, HOKA One One Clifton, Brooks® Addiction, Brooks Beast (Men), Brooks Ariel (Women) and New Balance 1080,” she explains. “I also advise patients to avoid going barefoot and to wear supportive slippers or sandals when at home. We recommend OOFOS, Vionic® or Haflinger® brands, which we find provide significant arch support and forefoot cushion.”
Dr. Sanders also utilizes dorsal taping of the affected digit in a plantarflexed position, and says she finds this can alleviate painful plantar MTPJ symptoms.
“We recommend patients use RockTape® or Kinesiotape through self-application continuously during acute periods of pain and inflammation,” she explains. “We also recommend taping during sports to stabilize the MTPJ.”
She continues by saying that she finds orthotics to be an important treatment modality in addressing both acute and chronic plantar plate injuries as well as post-surgical plantar plate repairs. Specifically, she notes orthotics can significantly decompress the metatarsophalangeal joints and off-weighting forefoot padding can also help alleviate painful symptoms. She typically incorporates a metatarsal raise proximal to the affected MTPJ into a 3D-printed orthotic shell. Next, she applies an 1/8” EVA full-length top cover and adds a 1/16” Poron forefoot extension with a slot aperture corresponding to the affected MTPJ. She also frequently replaces top cover padding approximately every six months to maintain cushioning and off-weighting capabilities.
Q: Are there any final thoughts you’d like to add to the discussion?
A:
Dr. Blake shares some additional aspects of his approaches to plantar plate pathology by stressing a focus on the biomechanical nature of the concern. He reminds us that plantar plate injury can present as a complete tear or just a degenerative process with perhaps microtearing.
“It is so important to take stock of the amount of inflammation and nerve sensitivities in the area,” he says. “These factors can make or break your treatment success. For every patient, for every injury, when they present to your office with pain, one of the three causes of pain may be the most prevalent for them. Therefore, you have to treat each (the mechanics, the inflammation, and the nerve sensitivities) with different modalities.”
He uses icing and contrast baths as vital tools for inflammation. Additionally, he advocates for reducing pain immediately to between zero and two out of ten on a visual analog scale, non-painful massage, neural flossing, and topical nerve medications like Neuro-Eze™ (Primavera Essentials) or Neuro One® Nerve Support Cream (Neuro One)are vital for reducing nerve pain. This being said, he points out that the mechanical treatments tend to be the most important whether surgery is done or not with off-weighting and immobilizing.
Dr. Blake is in practice at the Center for Sports Medicine, which is affiliated with St. Francis Memorial Hospital in San Francisco. He is a past president of the American Academy of Podiatric Sports Medicine. Dr. Blake is the author of the recently published book, “The Inverted Orthotic Technique: A Process Of Foot Stabilization For Pronated Feet,” which is available at www.bookbaby.com.
Dr. Kirby is an Adjunct Associate Professor within the Department of Applied Biomechanics at the California School of Podiatric Medicine at Samuel Merritt University in Oakland, Calif. He is in private practice in Sacramento, Calif.
Dr. Sanders is an Adjunct Professor with the California School of Podiatric Medicine at Samuel Merritt University. She is a Diplomate of the American Board of Podiatric Medicine and is in private practice in San Francisco.
1. Kirby K. Plantarflexion taping for plantar plate tears. Available at: https://www.youtube.com/watch?v=meUFV2UQyf8 . Published July 8, 2016. Accessed January 10, 2022.
2. Sanders J. Determining proper shoe size – Brannock device. Available at: https://drshoereviews.com/2011/11/03/determing-proper-shoe-length-brannock-device/ . Published November 3, 2011. Accessed January 10, 2022.





