


What Caused This Nodular, Ulcerated Lesion on the Lower Mucosal Lip?
Case Report

A 69-year-old man with a history notable for nonmelanoma skin cancer and being a nonsmoker sought dermatologic evaluation for a persistent, nonhealing lesion on his right lower lip (Figure). The lesion, evolving over the course of a year, exhibited gradual growth and occasional bleeding upon trauma. Upon examination, a 2.5-cm x 2.3-cm nodule with ulceration and crust was identified on the right lower lip, extending to the mucosal surface. A shave biopsy was performed from the nonulcerated area.
Diagnosis: Basal Cell Carcinoma
Basal cell carcinomas (BCCs) originate from keratinocytes in the basal layer of the epidermis, constituting approximately 80% of all nonmelanoma skin cancers in the United States.1,2 The development of BCC is influenced by various risk factors, including exposure to ultraviolet radiation, fair complexion, and distinctive features such as red or blond hair and light eye color.2 Although BCC predominantly manifests on sun-exposed areas, particularly the face and nose, there are rare instances of mucosal BCC (mBCC) occurring on the vermilion lip (VL) and oral mucosa.1,3 The rarity of BCC on the VL and oral mucosa can be attributed to historical beliefs that BCC originates from hair follicles and sweat glands, structures absent in normal vermilion tissues. However, emerging research challenges this notion, emphasizing the need for a nuanced understanding of BCC development in these less common sites.1,3
Clinical Presentation
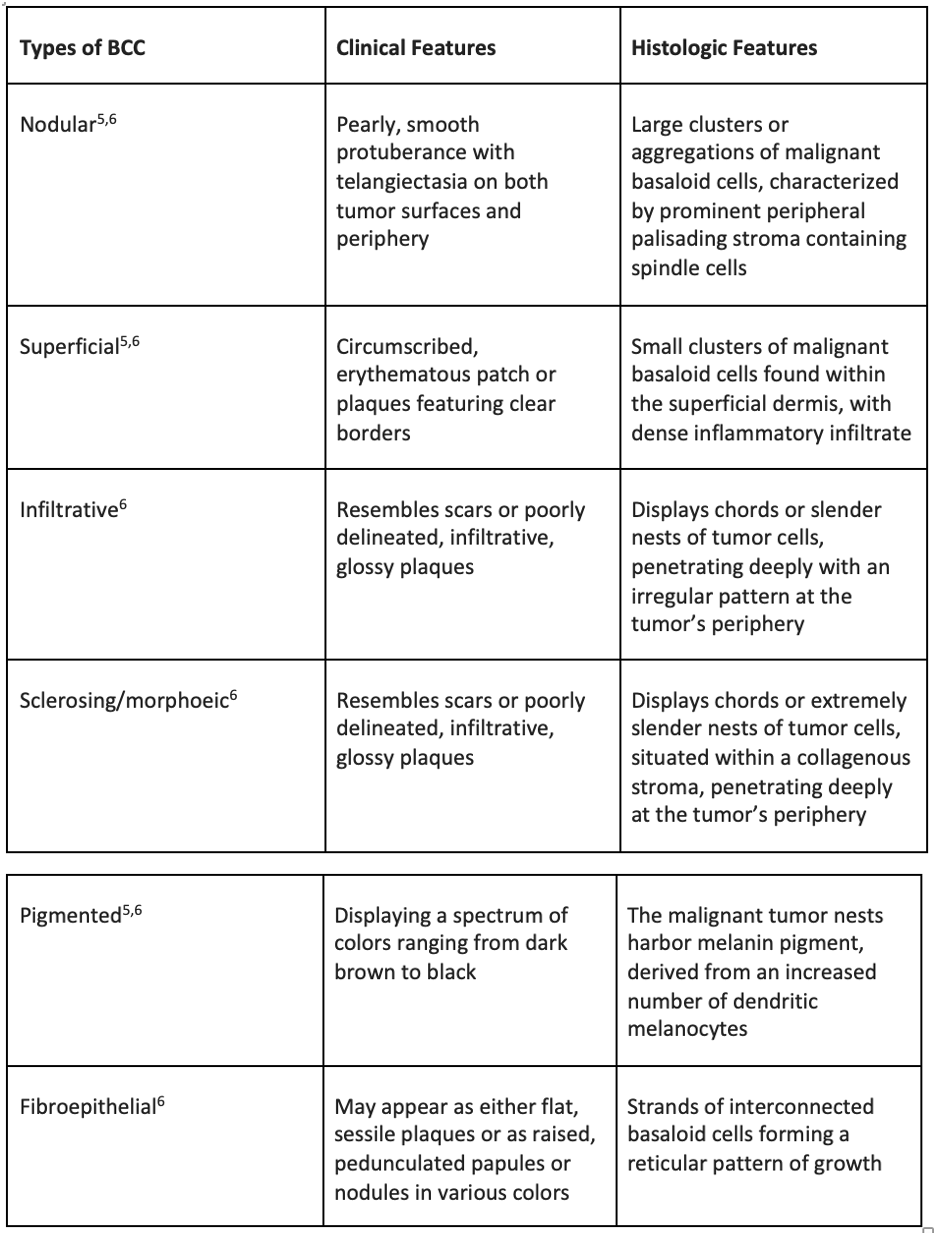
BCC typically emerges in sun-damaged skin, often characterized by nonhealing, enlarging lesions that may occasionally bleed and be accompanied by pruritus.4 Although this presentation is frequently encountered, BCC encompasses numerous types, each demonstrating unique clinical and histopathologic attributes (Table 1).5,6
mBCC remains infrequently documented in the literature, with most cases involving the VL and displaying distinctive features, such as crusted lesions, ulceration, and occasional bleeding. The rarity of mBCC, coupled with its unique clinical presentation, often leads to misdiagnosis, with herpes simplex being a common point of confusion. A comprehensive literature review delved into this rare entity, identifying 35 cases.1 Among these cases, 64% (n = 18) exhibited lesions on the upper VL, whereas 31% (n = 11) were situated on the lower VL. Notably, 6% (n = 2) of the lesions were located on the lower mucosal lip, and 11% (n = 4) were found on other oral mucosal sites. The average patient age was 66.8 years, with a balanced distribution between women (49%, n = 17) and men (51%, n = 18).1 mCCC appearing on the VL presents a distinctive growth pattern, demonstrating continuous expansion from the vermilion border to the mucosal surface at an earlier stage compared to BCC in other regions. This intriguing observation can be attributed to the thin submucosal layer of the lip, bringing nerves and muscles into close proximity to the lip surfaces.7
Additionally, it is important to distinguish mBCC from the other conditions. The most frequent diagnosis of lip ulceration is herpes simplex, thus mBCC of the lip can be misdiagnosed as a herpes simplex flare. Another common misdiagnosis is squamous cell carcinoma (SCC), especially if the lesion is located on the lower VL, because most BCC locates on the upper lip and SCC locates on the lower lip.1,7 Suspected lesions should undergo prompt biopsy to secure a definitive diagnosis, facilitating timely and precise treatment interventions.2
Clinical Differential Diagnosis
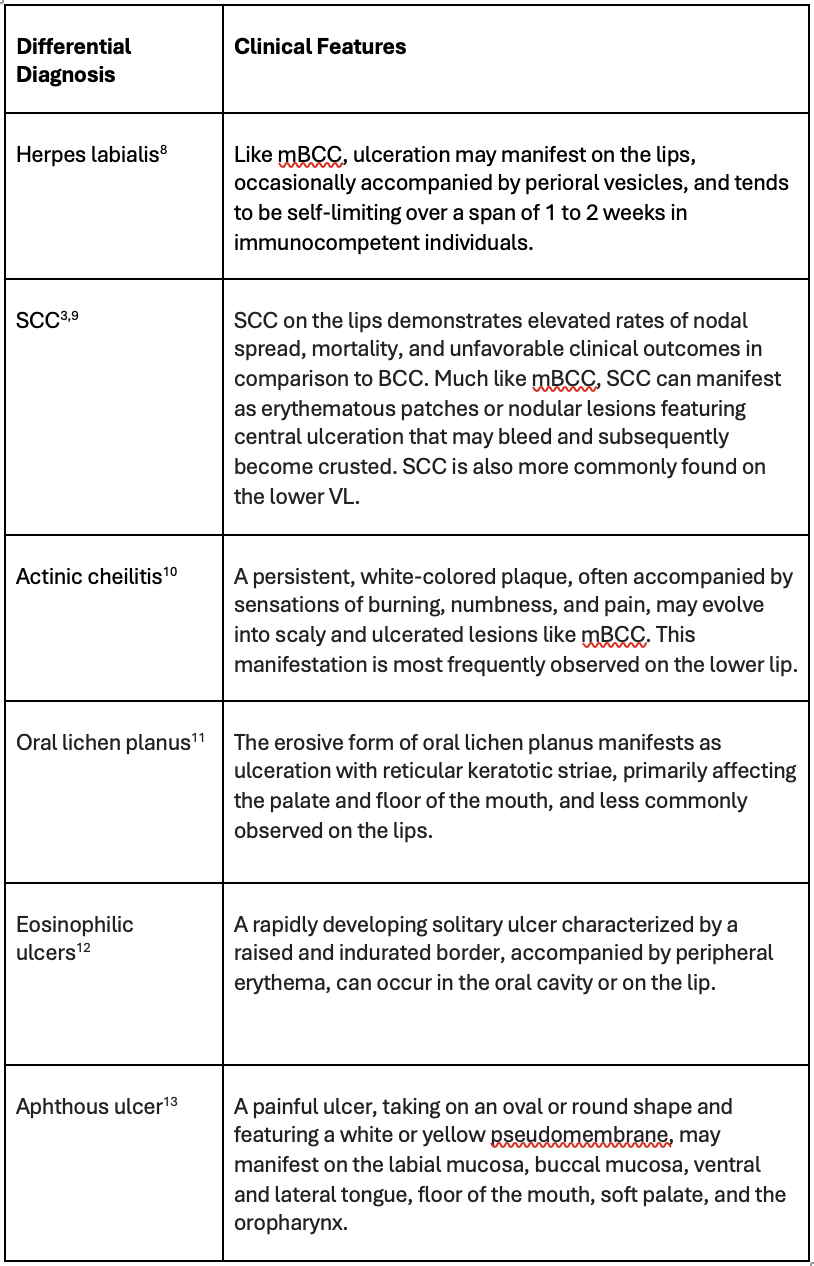
Distinguishing mBCC on the lip poses a challenging task, not only because of its anatomic location but also due to the overlap in clinical features with various other diseases. The differential diagnosis encompasses conditions such as herpes labialis, SCC, actinic cheilitis, oral lichen planus, eosinophilic ulcers, and aphthous ulcers (Table 2).8-13
Management
Various treatments are available for addressing BCC, encompassing standard excision, Mohs micrographic surgery, radiotherapy, and the application of 5-fluorouracil with imiquimod 5% cream. However, surgical options, specifically surgical excision and Mohs surgery, continue to uphold their status as the gold standard in BCC treatment. The choice of surgery as a treatment modality should be meticulously considered, taking into account the tumor's characteristics, including size, location, and the patient's medical history. Mohs surgery is typically reserved for high-risk tumors, particularly those that exhibit recurrence or are situated in critical anatomic sites.14 Mohs surgery emerges as the optimal treatment modality for mBCC, owing to its strategic alignment with the anatomic location and cosmetic concerns associated with mBCC. Existing literature strongly endorses Mohs surgery as the superior choice for treating BCC, particularly in the context of the VL.1,7 One study detailed 15 cases of mBCC on the VL, all of which were successfully treated with Mohs surgery; notably, no recurrences were observed during the average follow-up period of 38 months (ranging from 4 to 67 months).7 Similarly, a comprehensive literature review reported 22 cases of mBCC on the VL, all of which underwent Mohs surgery with no instances of recurrence.1 This compelling evidence highlights the efficacy of Mohs surgery in ensuring comprehensive treatment and long-term success in mBCC, particularly on the VL.
Our Patient
Upon evaluating the clinical presentation, a diagnosis of BCC was established, and histopathologic confirmation was sought through a biopsy. Subsequently, the chosen course of treatment during the follow-up appointment involved the implementation of Mohs surgery for comprehensive and targeted management of the condition.
Conclusion
Although BCC is a prevalent nonmelanoma skin cancer, the occurrence of mBCC on the VL is a distinctly rare phenomenon, sparsely documented in existing literature. This scarcity presents challenges in both differential diagnosis and the formulation of effective treatment strategies. Clinicians are tasked with considering mBCC as a potential differential diagnosis, especially when confronted with an ulcerated lesion on the lower lip, and confirming the diagnosis through biopsy.
Upon confirming mBCC, engaging in informed discussions with patients becomes imperative. These discussions should explore various treatment modalities, with a prominent recommendation for Mohs surgery as the gold standard due to its established efficacy. This approach underscores the importance of a tailored and comprehensive strategy for managing mBCC, recognizing its uniqueness and clinical intricacies in the landscape of skin cancers.
References
1. Loh T, Rubin AG, Brian Jiang SI. Management of mucosal basal cell carcinoma of the lip: an update and comprehensive review of the literature. Dermatol Surg. 2016;42(12):1313-1319. doi:10.1097/DSS.0000000000000790
2. Rubin AI, Chen EH, Ratner D. Basal-cell carcinoma. N Engl J Med. 2005;353(21):2262-2269. doi:10.1056/NEJMra044151
3. Hwang JR, Khachemoune A. Lower lip basal cell and squamous cell carcinomas: a reappraisal of the similarities and differences in clinical presentation and management. Arch Dermatol Res. 2023;315(2):117-125. doi:10.1007/s00403-022-02345-z
4. Cameron MC, Lee E, Hibler BP, et al. Basal cell carcinoma: epidemiology; pathophysiology; clinical and histological subtypes; and disease associations [published correction appears in J Am Acad Dermatol. 2021;85(2):535]. J Am Acad Dermatol. 2019;80(2):303-317. doi:10.1016/j.jaad.2018.03.060
5. Dourmishev LA, Rusinova D, Botev I. Clinical variants, stages, and management of basal cell carcinoma. Indian Dermatol Online J. 2013;4(1):12-17. doi:10.4103/2229-5178.105456
6. Niculet E, Craescu M, Rebegea L, et al. Basal cell carcinoma: comprehensive clinical and histopathological aspects, novel imaging tools and therapeutic approaches (review). Exp Ther Med. 2022;23(1):60. doi:10.3892/etm.2021.10982
7. Silapunt S, Peterson SR, Goldberg LH, Friedman PM, Alam M. Basal cell carcinoma on the vermilion lip: a study of 18 cases. J Am Acad Dermatol. 2004;50(3):384-387. doi:10.1016/j.jaad.2003.08.027
8. Fatahzadeh M, Schwartz RA. Human herpes simplex labialis. Clin Exp Dermatol. 2007;32(6):625-630. doi:10.1111/j.1365-2230.2007.02473.x
9. Bota JP, Lyons AB, Carroll BT. Squamous cell carcinoma of the lip—a review of squamous cell carcinogenesis of the mucosal and cutaneous junction. Dermatol Surg. 2017;43(4):494-506. doi:10.1097/DSS.0000000000001020
10. Muse ME, Crane JS. Actinic cheilitis. In: StatPearls [Internet]. StatPearls Publishing; 2023.
11. Alrashdan MS, Cirillo N, McCullough M. Oral lichen planus: a literature review and update. Arch Dermatol Res. 2016;308(8):539-551. doi:10.1007/s00403-016-1667-2
12. Segura S, Pujol RM. Eosinophilic ulcer of the oral mucosa: a distinct entity or a non-specific reactive pattern? Oral Dis. 2008;14(4):287-295. doi:10.1111/j.1601-0825.2008.01444.x
13. Messadi DV, Younai F. Aphthous ulcers. Dermatol Ther. 2010;23(3):281-290. doi:10.1111/j.1529-8019.2010.01324.x
14. Basset-Seguin N, Herms F. Update in the management of basal cell carcinoma. Acta Derm Venereol. 2020;100(11):adv00140. doi:10.2340/00015555-3495










