This ongoing feature series was taken from the 4th annual postgraduate course and workshop in medical mycology-dermatomycology, July 27-30, 1979, Newport Beach, CA.
Dr. James H. Graham was the former head of dermatopathology at the Armed Forces Institute of Pathology and the former chair of dermatology at UC Irvine. He has made available his personal library of kodachromes, slides and lectures collected throughout his career by means of a generous donation to the Wake Forest University Baptist Medical Center library. Dr. Graham’s lectures and personal images in dermatomycology are highlighted in this series to refresh the practicing clinician on deep cutaneous mycotic disease.
Coccidioidomycosis is caused by the highly infectious, dimorphic fungus Coccidioides immitis. Initially, isolated cases were thought to be caused by a protozoal infection; a fungal etiology was subsequently identified in the early 1900s and primitive cases generally resulted in disseminated, fatal disease.1 The broad clinical presentation of coccidioidomycosis was appreciated in the 1930s, when it was identified as the etiologic pathogen of “Valley fever” in the San Joaquin Valley in California.2 Cutaneous involvement is generally secondary to disseminated disease but can represent primary disease from direct inoculation. Systemic involvement, especially in immunocompromised hosts, has a poor prognosis, warranting timely diagnosis and prompt management.
Epidemiology and Pathogenesis
C. immitis is a soil-inhabiting fungus and has been isolated from contaminated vegetation. It is endemic in the southwestern United States, northern Mexico and Central and Southern America.3 Epidemics occur when soil is disrupted to a depth greater than 20 cm.4 The species exist in two phases, saprophytic and parasitic. The soil-growing filamentous mycelia form into arthroconidia, which are dispersed into the air. In the host they transform into and reside as spherules.
The organism enters the body by inhalation and generally causes a self-limited mild pulmonary disease. Dissemination may occur via hematogenous spread to the meninges, bones, lymph nodes, joints and, most commonly, the skin.2,5 Primary pulmonary infection does not show a gender or age preference. However, many genetic and co-morbid risk factors predispose an individual to systemic spread: some ethnic groups, African Americans and Filipinos, patients with decreased cellular immunity, HIV-infected persons and organ transplant recipients are at increased risk of severe disseminated disease.4,6 The Th1 cell-mediated immune system is responsible for establishing an effective response to infection. By impairing this mechanism, immunosuppressive medications like prednisone and methotrexate and newly developed biologics like TNF-alpha antagonists can predispose to severe primary infections or reactivation of latent infection.
Primary cutaneous coccidioidomycosis is very rare, with fewer than 20 case reports in the literature since 1926.7 It results from direct inoculation into the skin via contaminated foreign material and has been reported in agricultural and laboratory workers and from splinter injuries or lacerations in endemic areas.1
Clinical Presentation
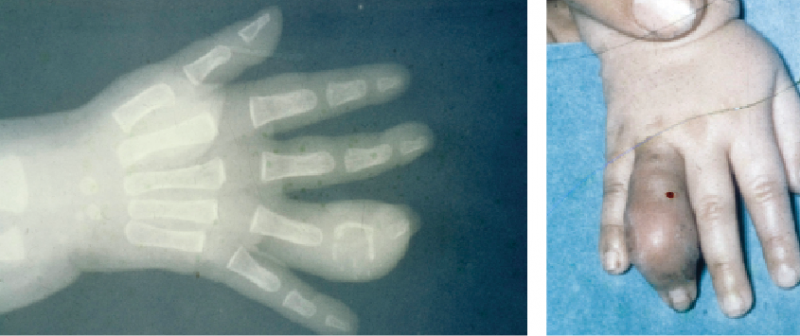
 Cutaneous presentations may be divided into organism-specific or reactive reactions (Table 1, left).1 Patients with primary pulmonary infection may present with reactive erythema nodosum, erythema multiforme or a generalized morbilliform rash. San Joaquin Valley fever includes the triad of fever, erythema nodosum and arthralgias. The skin is the most common site of dissemination and the classic cutaneous finding is a verrucous papule or plaque on the nasolabial fold (Figure 1).1 Cutaneous lesions are often papules, nodules or plaques typically localized to the head and neck (Figure 2). Later, these lesions may develop ulceration, sinus tracts or abscesses. Other common areas of dissemination include the meninges and bones (Figure 3). Primary cutaneous infections present as ulcerated nodules at the site of inoculation with associated lymphadenopathy with further development of nodules along the draining lymph tracts.
Cutaneous presentations may be divided into organism-specific or reactive reactions (Table 1, left).1 Patients with primary pulmonary infection may present with reactive erythema nodosum, erythema multiforme or a generalized morbilliform rash. San Joaquin Valley fever includes the triad of fever, erythema nodosum and arthralgias. The skin is the most common site of dissemination and the classic cutaneous finding is a verrucous papule or plaque on the nasolabial fold (Figure 1).1 Cutaneous lesions are often papules, nodules or plaques typically localized to the head and neck (Figure 2). Later, these lesions may develop ulceration, sinus tracts or abscesses. Other common areas of dissemination include the meninges and bones (Figure 3). Primary cutaneous infections present as ulcerated nodules at the site of inoculation with associated lymphadenopathy with further development of nodules along the draining lymph tracts.

Figure 1: Secondary cutaneous lesion in disseminated coccidioidomycosis presenting as a verrucous plaque on the nasolabial fold.

Figure 2: Secondary cutaneous coccidioidomycosis presenting as multiple papules on the face and neck.

Figure 3: Bone involvement of the right 4th finger in a young child with disseminated coccidioidomycosis.
Histopathology
 Biopsy of suspicious secondary lesions often reveals epidermal changes that range from acanthosis to pseudoepitheliomatous hyperplasia (Figure 4, left).8 A granulomatous infiltrate composed of epithelioid cells, plasma cells and a variable number of giant cells, lymphocytes and histiocytes are seen in the dermis and/or subcutaneous adipose tissue.1,8 In the acute stage, primary cutaneous lesions demonstrate a dense inflammatory infiltrate composed of neutrophils, lymphocytes and plasma cells and later show similar changes as those seen in secondary lesions.8
Biopsy of suspicious secondary lesions often reveals epidermal changes that range from acanthosis to pseudoepitheliomatous hyperplasia (Figure 4, left).8 A granulomatous infiltrate composed of epithelioid cells, plasma cells and a variable number of giant cells, lymphocytes and histiocytes are seen in the dermis and/or subcutaneous adipose tissue.1,8 In the acute stage, primary cutaneous lesions demonstrate a dense inflammatory infiltrate composed of neutrophils, lymphocytes and plasma cells and later show similar changes as those seen in secondary lesions.8
 Visualization of organisms by routine hematoxylin and eosin stains is variable and dependent on the immune status of the host. Utilization of special stains like Gomori’s methenamine silver nitrate or periodic acid schiff may produce a higher yield of demonstrating organisms.8 Organisms are seen as spherules containing numerous endospores measuring 5 µm to 10 µm, present either within giant cells or free in the tissue (Figure 5, left).6
Visualization of organisms by routine hematoxylin and eosin stains is variable and dependent on the immune status of the host. Utilization of special stains like Gomori’s methenamine silver nitrate or periodic acid schiff may produce a higher yield of demonstrating organisms.8 Organisms are seen as spherules containing numerous endospores measuring 5 µm to 10 µm, present either within giant cells or free in the tissue (Figure 5, left).6
Differential Diagnosis
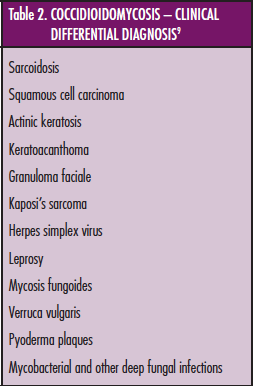
 The variable cutaneous morphology of coccidioidomycosis lesions has earned C. immitis a title as one of the “great imitators.”1,9 Lesions are generally non-specific; therefore, the clinical differential diagnosis is broad (Table 2, left). Disseminated cutaneous coccidioidomycosis should be considered in the differential diagnosis of any chronic nodular or verrucous skin lesions, especially when associated with pulmonary symptoms.9
The variable cutaneous morphology of coccidioidomycosis lesions has earned C. immitis a title as one of the “great imitators.”1,9 Lesions are generally non-specific; therefore, the clinical differential diagnosis is broad (Table 2, left). Disseminated cutaneous coccidioidomycosis should be considered in the differential diagnosis of any chronic nodular or verrucous skin lesions, especially when associated with pulmonary symptoms.9
 Histologically, the thick-walled refractile spherules are usually distinguishable from other fungal organisms by their relatively large size, ranging from 10 to 80 microns (Figure 6, left).1,9 Demonstration of spherules showing the characteristic endosporule formation differentiates them from lesions of North American blastomycosis and other deep fungal infections.
Histologically, the thick-walled refractile spherules are usually distinguishable from other fungal organisms by their relatively large size, ranging from 10 to 80 microns (Figure 6, left).1,9 Demonstration of spherules showing the characteristic endosporule formation differentiates them from lesions of North American blastomycosis and other deep fungal infections.
Diagnostic Tests
Biopsy of suspicious skin lesions and the histological demonstration of spherules and their endospores are necessary to make a correct diagnosis.9 Tissue cultures are the gold standard for organism identification, which appear as rapidly growing white colonies on standard culture media within 2 to 5 days.1,9 Qualitative and quantitative serologic tests can also be used to establish a diagnosis. Enzyme immunoassay is a highly sensitive test and provides a quick assessment of IgM and IgG coccidioidal antibodies. A positive test can be confirmed by more specific techniques, such as quantifying IgG complement-fixing antibodies by immunodiffusion or other complement fixation techniques.1 Titers generally correlate with the severity of disease and even low titers (1:2) are likely to signify a true infection.1 Molecular techniques, including in situ hybridization and polymerase chain reaction tests, are available to detect C. immitis but are less commonly used since other methods can accurately establish the diagnosis.
Treatment
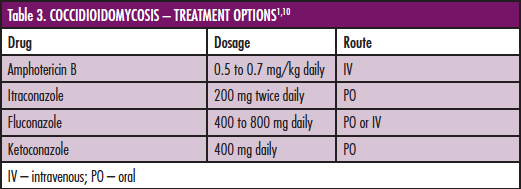
 Disseminated infection may progress to severe disease and a potentially fatal outcome, thus warranting timely recognition and accurate treatment and management. The Infectious Disease Society of America published detailed guidelines on the treatment of systemic disease.10 Management involves assessment of the extent and severity of infection and the patient’s demographics and risk factors that predispose disease severity.1,10 Symptomatic disseminated disease requires immediate treatment with Amphotericin B or an azole antifungal (Table 3, left). After initial treatment of the disseminated infection, maintenance therapy for 1 to 2 years or life-long therapy may be required.1,10
Disseminated infection may progress to severe disease and a potentially fatal outcome, thus warranting timely recognition and accurate treatment and management. The Infectious Disease Society of America published detailed guidelines on the treatment of systemic disease.10 Management involves assessment of the extent and severity of infection and the patient’s demographics and risk factors that predispose disease severity.1,10 Symptomatic disseminated disease requires immediate treatment with Amphotericin B or an azole antifungal (Table 3, left). After initial treatment of the disseminated infection, maintenance therapy for 1 to 2 years or life-long therapy may be required.1,10
Unlike the disseminated form, primary cutaneous coccidioidomycoses self-resolves and has an excellent prognosis, generally requiring only supportive local therapy.7
Key Points
• Coccidioidomycosis is a deep cutaneous mycotic infection caused by the opportunistic dimorphic fungus Coccidioidomycosis immitis.
• Coccidioidomycosis is a “great imitator” and has a wide variety of clinical presentations ranging from single or multiple verrucous nodules, papules, ulcerations or abscesses.
• Histological examination reveals pseudoepitheliomatous hyperplasia and acanthosis overlying a granulomatous infiltrate within the dermis and/or subcutaneous tissue.
• Routine H&E, GME or PAS stains reveals organisms as large spherules containing numerous endosporules.
• Tissue culture, serology and molecular methods may be used to aid in establishing a diagnosis when visualization by direct microscopic examination is not effective.
• Like other deep fungal infections, Amphotericin B is the standard of treatment for symptomatic disseminated disease. Azoles, including itraconazole, fluconazole and ketoconazole, are additional treatment options.
Photos and Tables: Graham Library of Digital Images, Wake Forest University Department of Dermatology © 2009 Wake Forest University Dermatology
Swetha Narahari is with the Center for Dermatology Research and the Department of Dermatology at Wake Forest University School of Medicine in Winston-Salem, NC.
Dr. Feldman is with the Center for Dermatology Research and the Departments of Dermatology, Pathology and Public Health Sciences at Wake Forest University School of Medicine in Winston-Salem, NC.
Disclosure: The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories, L.P. Ms. Narahari and Dr. Feldman disclose that they have no real or apparent conflicts of interest or financial interests or arrangements with any companies or products mentioned in this article.
This ongoing feature series was taken from the 4th annual postgraduate course and workshop in medical mycology-dermatomycology, July 27-30, 1979, Newport Beach, CA.
Dr. James H. Graham was the former head of dermatopathology at the Armed Forces Institute of Pathology and the former chair of dermatology at UC Irvine. He has made available his personal library of kodachromes, slides and lectures collected throughout his career by means of a generous donation to the Wake Forest University Baptist Medical Center library. Dr. Graham’s lectures and personal images in dermatomycology are highlighted in this series to refresh the practicing clinician on deep cutaneous mycotic disease.
Coccidioidomycosis is caused by the highly infectious, dimorphic fungus Coccidioides immitis. Initially, isolated cases were thought to be caused by a protozoal infection; a fungal etiology was subsequently identified in the early 1900s and primitive cases generally resulted in disseminated, fatal disease.1 The broad clinical presentation of coccidioidomycosis was appreciated in the 1930s, when it was identified as the etiologic pathogen of “Valley fever” in the San Joaquin Valley in California.2 Cutaneous involvement is generally secondary to disseminated disease but can represent primary disease from direct inoculation. Systemic involvement, especially in immunocompromised hosts, has a poor prognosis, warranting timely diagnosis and prompt management.
Epidemiology and Pathogenesis
C. immitis is a soil-inhabiting fungus and has been isolated from contaminated vegetation. It is endemic in the southwestern United States, northern Mexico and Central and Southern America.3 Epidemics occur when soil is disrupted to a depth greater than 20 cm.4 The species exist in two phases, saprophytic and parasitic. The soil-growing filamentous mycelia form into arthroconidia, which are dispersed into the air. In the host they transform into and reside as spherules.
The organism enters the body by inhalation and generally causes a self-limited mild pulmonary disease. Dissemination may occur via hematogenous spread to the meninges, bones, lymph nodes, joints and, most commonly, the skin.2,5 Primary pulmonary infection does not show a gender or age preference. However, many genetic and co-morbid risk factors predispose an individual to systemic spread: some ethnic groups, African Americans and Filipinos, patients with decreased cellular immunity, HIV-infected persons and organ transplant recipients are at increased risk of severe disseminated disease.4,6 The Th1 cell-mediated immune system is responsible for establishing an effective response to infection. By impairing this mechanism, immunosuppressive medications like prednisone and methotrexate and newly developed biologics like TNF-alpha antagonists can predispose to severe primary infections or reactivation of latent infection.
Primary cutaneous coccidioidomycosis is very rare, with fewer than 20 case reports in the literature since 1926.7 It results from direct inoculation into the skin via contaminated foreign material and has been reported in agricultural and laboratory workers and from splinter injuries or lacerations in endemic areas.1
Clinical Presentation
 Cutaneous presentations may be divided into organism-specific or reactive reactions (Table 1, left).1 Patients with primary pulmonary infection may present with reactive erythema nodosum, erythema multiforme or a generalized morbilliform rash. San Joaquin Valley fever includes the triad of fever, erythema nodosum and arthralgias. The skin is the most common site of dissemination and the classic cutaneous finding is a verrucous papule or plaque on the nasolabial fold (Figure 1).1 Cutaneous lesions are often papules, nodules or plaques typically localized to the head and neck (Figure 2). Later, these lesions may develop ulceration, sinus tracts or abscesses. Other common areas of dissemination include the meninges and bones (Figure 3). Primary cutaneous infections present as ulcerated nodules at the site of inoculation with associated lymphadenopathy with further development of nodules along the draining lymph tracts.
Cutaneous presentations may be divided into organism-specific or reactive reactions (Table 1, left).1 Patients with primary pulmonary infection may present with reactive erythema nodosum, erythema multiforme or a generalized morbilliform rash. San Joaquin Valley fever includes the triad of fever, erythema nodosum and arthralgias. The skin is the most common site of dissemination and the classic cutaneous finding is a verrucous papule or plaque on the nasolabial fold (Figure 1).1 Cutaneous lesions are often papules, nodules or plaques typically localized to the head and neck (Figure 2). Later, these lesions may develop ulceration, sinus tracts or abscesses. Other common areas of dissemination include the meninges and bones (Figure 3). Primary cutaneous infections present as ulcerated nodules at the site of inoculation with associated lymphadenopathy with further development of nodules along the draining lymph tracts.

Figure 1: Secondary cutaneous lesion in disseminated coccidioidomycosis presenting as a verrucous plaque on the nasolabial fold.

Figure 2: Secondary cutaneous coccidioidomycosis presenting as multiple papules on the face and neck.

Figure 3: Bone involvement of the right 4th finger in a young child with disseminated coccidioidomycosis.
Histopathology
 Biopsy of suspicious secondary lesions often reveals epidermal changes that range from acanthosis to pseudoepitheliomatous hyperplasia (Figure 4, left).8 A granulomatous infiltrate composed of epithelioid cells, plasma cells and a variable number of giant cells, lymphocytes and histiocytes are seen in the dermis and/or subcutaneous adipose tissue.1,8 In the acute stage, primary cutaneous lesions demonstrate a dense inflammatory infiltrate composed of neutrophils, lymphocytes and plasma cells and later show similar changes as those seen in secondary lesions.8
Biopsy of suspicious secondary lesions often reveals epidermal changes that range from acanthosis to pseudoepitheliomatous hyperplasia (Figure 4, left).8 A granulomatous infiltrate composed of epithelioid cells, plasma cells and a variable number of giant cells, lymphocytes and histiocytes are seen in the dermis and/or subcutaneous adipose tissue.1,8 In the acute stage, primary cutaneous lesions demonstrate a dense inflammatory infiltrate composed of neutrophils, lymphocytes and plasma cells and later show similar changes as those seen in secondary lesions.8
 Visualization of organisms by routine hematoxylin and eosin stains is variable and dependent on the immune status of the host. Utilization of special stains like Gomori’s methenamine silver nitrate or periodic acid schiff may produce a higher yield of demonstrating organisms.8 Organisms are seen as spherules containing numerous endospores measuring 5 µm to 10 µm, present either within giant cells or free in the tissue (Figure 5, left).6
Visualization of organisms by routine hematoxylin and eosin stains is variable and dependent on the immune status of the host. Utilization of special stains like Gomori’s methenamine silver nitrate or periodic acid schiff may produce a higher yield of demonstrating organisms.8 Organisms are seen as spherules containing numerous endospores measuring 5 µm to 10 µm, present either within giant cells or free in the tissue (Figure 5, left).6
Differential Diagnosis
 The variable cutaneous morphology of coccidioidomycosis lesions has earned C. immitis a title as one of the “great imitators.”1,9 Lesions are generally non-specific; therefore, the clinical differential diagnosis is broad (Table 2, left). Disseminated cutaneous coccidioidomycosis should be considered in the differential diagnosis of any chronic nodular or verrucous skin lesions, especially when associated with pulmonary symptoms.9
The variable cutaneous morphology of coccidioidomycosis lesions has earned C. immitis a title as one of the “great imitators.”1,9 Lesions are generally non-specific; therefore, the clinical differential diagnosis is broad (Table 2, left). Disseminated cutaneous coccidioidomycosis should be considered in the differential diagnosis of any chronic nodular or verrucous skin lesions, especially when associated with pulmonary symptoms.9
 Histologically, the thick-walled refractile spherules are usually distinguishable from other fungal organisms by their relatively large size, ranging from 10 to 80 microns (Figure 6, left).1,9 Demonstration of spherules showing the characteristic endosporule formation differentiates them from lesions of North American blastomycosis and other deep fungal infections.
Histologically, the thick-walled refractile spherules are usually distinguishable from other fungal organisms by their relatively large size, ranging from 10 to 80 microns (Figure 6, left).1,9 Demonstration of spherules showing the characteristic endosporule formation differentiates them from lesions of North American blastomycosis and other deep fungal infections.
Diagnostic Tests
Biopsy of suspicious skin lesions and the histological demonstration of spherules and their endospores are necessary to make a correct diagnosis.9 Tissue cultures are the gold standard for organism identification, which appear as rapidly growing white colonies on standard culture media within 2 to 5 days.1,9 Qualitative and quantitative serologic tests can also be used to establish a diagnosis. Enzyme immunoassay is a highly sensitive test and provides a quick assessment of IgM and IgG coccidioidal antibodies. A positive test can be confirmed by more specific techniques, such as quantifying IgG complement-fixing antibodies by immunodiffusion or other complement fixation techniques.1 Titers generally correlate with the severity of disease and even low titers (1:2) are likely to signify a true infection.1 Molecular techniques, including in situ hybridization and polymerase chain reaction tests, are available to detect C. immitis but are less commonly used since other methods can accurately establish the diagnosis.
Treatment
 Disseminated infection may progress to severe disease and a potentially fatal outcome, thus warranting timely recognition and accurate treatment and management. The Infectious Disease Society of America published detailed guidelines on the treatment of systemic disease.10 Management involves assessment of the extent and severity of infection and the patient’s demographics and risk factors that predispose disease severity.1,10 Symptomatic disseminated disease requires immediate treatment with Amphotericin B or an azole antifungal (Table 3, left). After initial treatment of the disseminated infection, maintenance therapy for 1 to 2 years or life-long therapy may be required.1,10
Disseminated infection may progress to severe disease and a potentially fatal outcome, thus warranting timely recognition and accurate treatment and management. The Infectious Disease Society of America published detailed guidelines on the treatment of systemic disease.10 Management involves assessment of the extent and severity of infection and the patient’s demographics and risk factors that predispose disease severity.1,10 Symptomatic disseminated disease requires immediate treatment with Amphotericin B or an azole antifungal (Table 3, left). After initial treatment of the disseminated infection, maintenance therapy for 1 to 2 years or life-long therapy may be required.1,10
Unlike the disseminated form, primary cutaneous coccidioidomycoses self-resolves and has an excellent prognosis, generally requiring only supportive local therapy.7
Key Points
• Coccidioidomycosis is a deep cutaneous mycotic infection caused by the opportunistic dimorphic fungus Coccidioidomycosis immitis.
• Coccidioidomycosis is a “great imitator” and has a wide variety of clinical presentations ranging from single or multiple verrucous nodules, papules, ulcerations or abscesses.
• Histological examination reveals pseudoepitheliomatous hyperplasia and acanthosis overlying a granulomatous infiltrate within the dermis and/or subcutaneous tissue.
• Routine H&E, GME or PAS stains reveals organisms as large spherules containing numerous endosporules.
• Tissue culture, serology and molecular methods may be used to aid in establishing a diagnosis when visualization by direct microscopic examination is not effective.
• Like other deep fungal infections, Amphotericin B is the standard of treatment for symptomatic disseminated disease. Azoles, including itraconazole, fluconazole and ketoconazole, are additional treatment options.
Photos and Tables: Graham Library of Digital Images, Wake Forest University Department of Dermatology © 2009 Wake Forest University Dermatology
Swetha Narahari is with the Center for Dermatology Research and the Department of Dermatology at Wake Forest University School of Medicine in Winston-Salem, NC.
Dr. Feldman is with the Center for Dermatology Research and the Departments of Dermatology, Pathology and Public Health Sciences at Wake Forest University School of Medicine in Winston-Salem, NC.
Disclosure: The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories, L.P. Ms. Narahari and Dr. Feldman disclose that they have no real or apparent conflicts of interest or financial interests or arrangements with any companies or products mentioned in this article.
This ongoing feature series was taken from the 4th annual postgraduate course and workshop in medical mycology-dermatomycology, July 27-30, 1979, Newport Beach, CA.
Dr. James H. Graham was the former head of dermatopathology at the Armed Forces Institute of Pathology and the former chair of dermatology at UC Irvine. He has made available his personal library of kodachromes, slides and lectures collected throughout his career by means of a generous donation to the Wake Forest University Baptist Medical Center library. Dr. Graham’s lectures and personal images in dermatomycology are highlighted in this series to refresh the practicing clinician on deep cutaneous mycotic disease.
Coccidioidomycosis is caused by the highly infectious, dimorphic fungus Coccidioides immitis. Initially, isolated cases were thought to be caused by a protozoal infection; a fungal etiology was subsequently identified in the early 1900s and primitive cases generally resulted in disseminated, fatal disease.1 The broad clinical presentation of coccidioidomycosis was appreciated in the 1930s, when it was identified as the etiologic pathogen of “Valley fever” in the San Joaquin Valley in California.2 Cutaneous involvement is generally secondary to disseminated disease but can represent primary disease from direct inoculation. Systemic involvement, especially in immunocompromised hosts, has a poor prognosis, warranting timely diagnosis and prompt management.
Epidemiology and Pathogenesis
C. immitis is a soil-inhabiting fungus and has been isolated from contaminated vegetation. It is endemic in the southwestern United States, northern Mexico and Central and Southern America.3 Epidemics occur when soil is disrupted to a depth greater than 20 cm.4 The species exist in two phases, saprophytic and parasitic. The soil-growing filamentous mycelia form into arthroconidia, which are dispersed into the air. In the host they transform into and reside as spherules.
The organism enters the body by inhalation and generally causes a self-limited mild pulmonary disease. Dissemination may occur via hematogenous spread to the meninges, bones, lymph nodes, joints and, most commonly, the skin.2,5 Primary pulmonary infection does not show a gender or age preference. However, many genetic and co-morbid risk factors predispose an individual to systemic spread: some ethnic groups, African Americans and Filipinos, patients with decreased cellular immunity, HIV-infected persons and organ transplant recipients are at increased risk of severe disseminated disease.4,6 The Th1 cell-mediated immune system is responsible for establishing an effective response to infection. By impairing this mechanism, immunosuppressive medications like prednisone and methotrexate and newly developed biologics like TNF-alpha antagonists can predispose to severe primary infections or reactivation of latent infection.
Primary cutaneous coccidioidomycosis is very rare, with fewer than 20 case reports in the literature since 1926.7 It results from direct inoculation into the skin via contaminated foreign material and has been reported in agricultural and laboratory workers and from splinter injuries or lacerations in endemic areas.1
Clinical Presentation
Cutaneous presentations may be divided into organism-specific or reactive reactions (Table 1, left).1 Patients with primary pulmonary infection may present with reactive erythema nodosum, erythema multiforme or a generalized morbilliform rash. San Joaquin Valley fever includes the triad of fever, erythema nodosum and arthralgias. The skin is the most common site of dissemination and the classic cutaneous finding is a verrucous papule or plaque on the nasolabial fold (Figure 1).1 Cutaneous lesions are often papules, nodules or plaques typically localized to the head and neck (Figure 2). Later, these lesions may develop ulceration, sinus tracts or abscesses. Other common areas of dissemination include the meninges and bones (Figure 3). Primary cutaneous infections present as ulcerated nodules at the site of inoculation with associated lymphadenopathy with further development of nodules along the draining lymph tracts.
Figure 1: Secondary cutaneous lesion in disseminated coccidioidomycosis presenting as a verrucous plaque on the nasolabial fold.
Figure 2: Secondary cutaneous coccidioidomycosis presenting as multiple papules on the face and neck.
Figure 3: Bone involvement of the right 4th finger in a young child with disseminated coccidioidomycosis.
Histopathology
Biopsy of suspicious secondary lesions often reveals epidermal changes that range from acanthosis to pseudoepitheliomatous hyperplasia (Figure 4, left).8 A granulomatous infiltrate composed of epithelioid cells, plasma cells and a variable number of giant cells, lymphocytes and histiocytes are seen in the dermis and/or subcutaneous adipose tissue.1,8 In the acute stage, primary cutaneous lesions demonstrate a dense inflammatory infiltrate composed of neutrophils, lymphocytes and plasma cells and later show similar changes as those seen in secondary lesions.8
Visualization of organisms by routine hematoxylin and eosin stains is variable and dependent on the immune status of the host. Utilization of special stains like Gomori’s methenamine silver nitrate or periodic acid schiff may produce a higher yield of demonstrating organisms.8 Organisms are seen as spherules containing numerous endospores measuring 5 µm to 10 µm, present either within giant cells or free in the tissue (Figure 5, left).6
Differential Diagnosis
The variable cutaneous morphology of coccidioidomycosis lesions has earned C. immitis a title as one of the “great imitators.”1,9 Lesions are generally non-specific; therefore, the clinical differential diagnosis is broad (Table 2, left). Disseminated cutaneous coccidioidomycosis should be considered in the differential diagnosis of any chronic nodular or verrucous skin lesions, especially when associated with pulmonary symptoms.9
Histologically, the thick-walled refractile spherules are usually distinguishable from other fungal organisms by their relatively large size, ranging from 10 to 80 microns (Figure 6, left).1,9 Demonstration of spherules showing the characteristic endosporule formation differentiates them from lesions of North American blastomycosis and other deep fungal infections.
Diagnostic Tests
Biopsy of suspicious skin lesions and the histological demonstration of spherules and their endospores are necessary to make a correct diagnosis.9 Tissue cultures are the gold standard for organism identification, which appear as rapidly growing white colonies on standard culture media within 2 to 5 days.1,9 Qualitative and quantitative serologic tests can also be used to establish a diagnosis. Enzyme immunoassay is a highly sensitive test and provides a quick assessment of IgM and IgG coccidioidal antibodies. A positive test can be confirmed by more specific techniques, such as quantifying IgG complement-fixing antibodies by immunodiffusion or other complement fixation techniques.1 Titers generally correlate with the severity of disease and even low titers (1:2) are likely to signify a true infection.1 Molecular techniques, including in situ hybridization and polymerase chain reaction tests, are available to detect C. immitis but are less commonly used since other methods can accurately establish the diagnosis.
Treatment
Disseminated infection may progress to severe disease and a potentially fatal outcome, thus warranting timely recognition and accurate treatment and management. The Infectious Disease Society of America published detailed guidelines on the treatment of systemic disease.10 Management involves assessment of the extent and severity of infection and the patient’s demographics and risk factors that predispose disease severity.1,10 Symptomatic disseminated disease requires immediate treatment with Amphotericin B or an azole antifungal (Table 3, left). After initial treatment of the disseminated infection, maintenance therapy for 1 to 2 years or life-long therapy may be required.1,10
Unlike the disseminated form, primary cutaneous coccidioidomycoses self-resolves and has an excellent prognosis, generally requiring only supportive local therapy.7
Key Points
• Coccidioidomycosis is a deep cutaneous mycotic infection caused by the opportunistic dimorphic fungus Coccidioidomycosis immitis.
• Coccidioidomycosis is a “great imitator” and has a wide variety of clinical presentations ranging from single or multiple verrucous nodules, papules, ulcerations or abscesses.
• Histological examination reveals pseudoepitheliomatous hyperplasia and acanthosis overlying a granulomatous infiltrate within the dermis and/or subcutaneous tissue.
• Routine H&E, GME or PAS stains reveals organisms as large spherules containing numerous endosporules.
• Tissue culture, serology and molecular methods may be used to aid in establishing a diagnosis when visualization by direct microscopic examination is not effective.
• Like other deep fungal infections, Amphotericin B is the standard of treatment for symptomatic disseminated disease. Azoles, including itraconazole, fluconazole and ketoconazole, are additional treatment options.
Photos and Tables: Graham Library of Digital Images, Wake Forest University Department of Dermatology © 2009 Wake Forest University Dermatology
Swetha Narahari is with the Center for Dermatology Research and the Department of Dermatology at Wake Forest University School of Medicine in Winston-Salem, NC.
Dr. Feldman is with the Center for Dermatology Research and the Departments of Dermatology, Pathology and Public Health Sciences at Wake Forest University School of Medicine in Winston-Salem, NC.
Disclosure: The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories, L.P. Ms. Narahari and Dr. Feldman disclose that they have no real or apparent conflicts of interest or financial interests or arrangements with any companies or products mentioned in this article.









 Cutaneous presentations may be divided into organism-specific or reactive reactions (Table 1, left).1 Patients with primary pulmonary infection may present with reactive erythema nodosum, erythema multiforme or a generalized morbilliform rash. San Joaquin Valley fever includes the triad of fever, erythema nodosum and arthralgias. The skin is the most common site of dissemination and the classic cutaneous finding is a verrucous papule or plaque on the nasolabial fold (Figure 1).1 Cutaneous lesions are often papules, nodules or plaques typically localized to the head and neck (Figure 2). Later, these lesions may develop ulceration, sinus tracts or abscesses. Other common areas of dissemination include the meninges and bones (Figure 3). Primary cutaneous infections present as ulcerated nodules at the site of inoculation with associated lymphadenopathy with further development of nodules along the draining lymph tracts.
Cutaneous presentations may be divided into organism-specific or reactive reactions (Table 1, left).1 Patients with primary pulmonary infection may present with reactive erythema nodosum, erythema multiforme or a generalized morbilliform rash. San Joaquin Valley fever includes the triad of fever, erythema nodosum and arthralgias. The skin is the most common site of dissemination and the classic cutaneous finding is a verrucous papule or plaque on the nasolabial fold (Figure 1).1 Cutaneous lesions are often papules, nodules or plaques typically localized to the head and neck (Figure 2). Later, these lesions may develop ulceration, sinus tracts or abscesses. Other common areas of dissemination include the meninges and bones (Figure 3). Primary cutaneous infections present as ulcerated nodules at the site of inoculation with associated lymphadenopathy with further development of nodules along the draining lymph tracts.


 Biopsy of suspicious secondary lesions often reveals epidermal changes that range from acanthosis to pseudoepitheliomatous hyperplasia (Figure 4, left).8 A granulomatous infiltrate composed of epithelioid cells, plasma cells and a variable number of giant cells, lymphocytes and histiocytes are seen in the dermis and/or subcutaneous adipose tissue.1,8 In the acute stage, primary cutaneous lesions demonstrate a dense inflammatory infiltrate composed of neutrophils, lymphocytes and plasma cells and later show similar changes as those seen in secondary lesions.8
Biopsy of suspicious secondary lesions often reveals epidermal changes that range from acanthosis to pseudoepitheliomatous hyperplasia (Figure 4, left).8 A granulomatous infiltrate composed of epithelioid cells, plasma cells and a variable number of giant cells, lymphocytes and histiocytes are seen in the dermis and/or subcutaneous adipose tissue.1,8 In the acute stage, primary cutaneous lesions demonstrate a dense inflammatory infiltrate composed of neutrophils, lymphocytes and plasma cells and later show similar changes as those seen in secondary lesions.8 Visualization of organisms by routine hematoxylin and eosin stains is variable and dependent on the immune status of the host. Utilization of special stains like Gomori’s methenamine silver nitrate or periodic acid schiff may produce a higher yield of demonstrating organisms.8 Organisms are seen as spherules containing numerous endospores measuring 5 µm to 10 µm, present either within giant cells or free in the tissue (Figure 5, left).6
Visualization of organisms by routine hematoxylin and eosin stains is variable and dependent on the immune status of the host. Utilization of special stains like Gomori’s methenamine silver nitrate or periodic acid schiff may produce a higher yield of demonstrating organisms.8 Organisms are seen as spherules containing numerous endospores measuring 5 µm to 10 µm, present either within giant cells or free in the tissue (Figure 5, left).6 The variable cutaneous morphology of coccidioidomycosis lesions has earned C. immitis a title as one of the “great imitators.”1,9 Lesions are generally non-specific; therefore, the clinical differential diagnosis is broad (Table 2, left). Disseminated cutaneous coccidioidomycosis should be considered in the differential diagnosis of any chronic nodular or verrucous skin lesions, especially when associated with pulmonary symptoms.9
The variable cutaneous morphology of coccidioidomycosis lesions has earned C. immitis a title as one of the “great imitators.”1,9 Lesions are generally non-specific; therefore, the clinical differential diagnosis is broad (Table 2, left). Disseminated cutaneous coccidioidomycosis should be considered in the differential diagnosis of any chronic nodular or verrucous skin lesions, especially when associated with pulmonary symptoms.9 Histologically, the thick-walled refractile spherules are usually distinguishable from other fungal organisms by their relatively large size, ranging from 10 to 80 microns (Figure 6, left).1,9 Demonstration of spherules showing the characteristic endosporule formation differentiates them from lesions of North American blastomycosis and other deep fungal infections.
Histologically, the thick-walled refractile spherules are usually distinguishable from other fungal organisms by their relatively large size, ranging from 10 to 80 microns (Figure 6, left).1,9 Demonstration of spherules showing the characteristic endosporule formation differentiates them from lesions of North American blastomycosis and other deep fungal infections. Disseminated infection may progress to severe disease and a potentially fatal outcome, thus warranting timely recognition and accurate treatment and management. The Infectious Disease Society of America published detailed guidelines on the treatment of systemic disease.10 Management involves assessment of the extent and severity of infection and the patient’s demographics and risk factors that predispose disease severity.1,10 Symptomatic disseminated disease requires immediate treatment with Amphotericin B or an azole antifungal (Table 3, left). After initial treatment of the disseminated infection, maintenance therapy for 1 to 2 years or life-long therapy may be required.1,10
Disseminated infection may progress to severe disease and a potentially fatal outcome, thus warranting timely recognition and accurate treatment and management. The Infectious Disease Society of America published detailed guidelines on the treatment of systemic disease.10 Management involves assessment of the extent and severity of infection and the patient’s demographics and risk factors that predispose disease severity.1,10 Symptomatic disseminated disease requires immediate treatment with Amphotericin B or an azole antifungal (Table 3, left). After initial treatment of the disseminated infection, maintenance therapy for 1 to 2 years or life-long therapy may be required.1,10