


What Is This Rash on a 16-Year-Old Girl?
Case Report
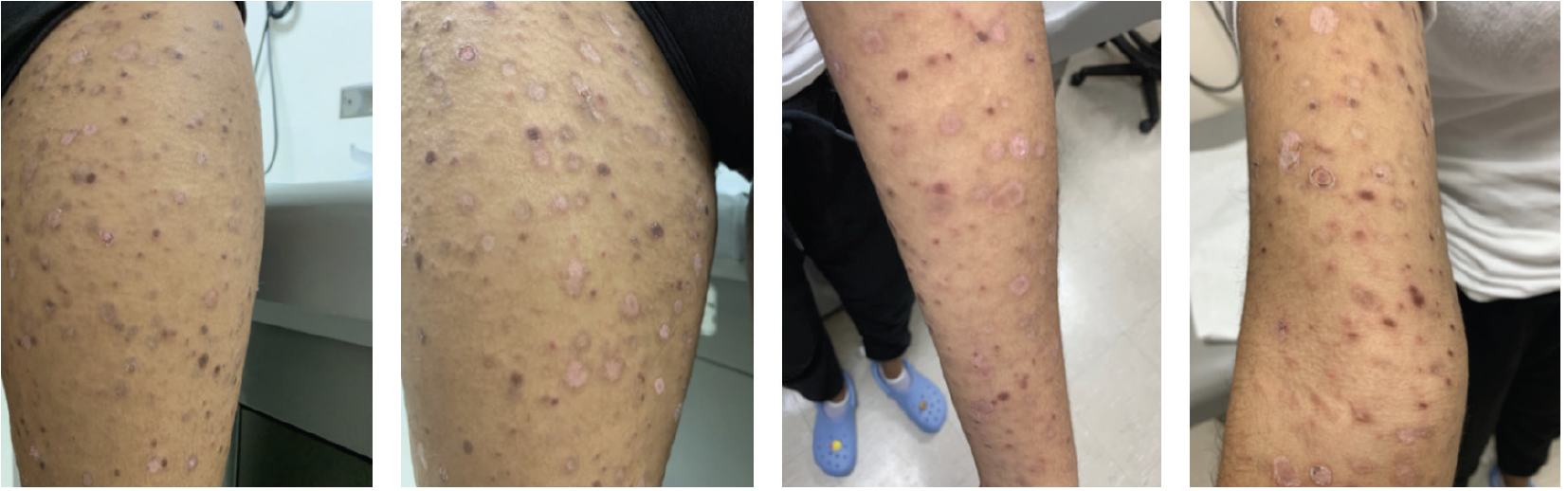
A 16-year-old, otherwise healthy, African American girl presented to the hospital 1 month after a rash started on the bilateral upper and lower extremities. Other than the rash, the patient was well. She denied any other symptoms, including joint pain, fever, chills, and night sweats. She did not take any medications and had no known allergies. On skin examination, the patient had dull pink, thin papules and plaques that were too many to count, with a hyperpigmented border. Some of the papules and plaques had a central and/or peripheral scale/crust on the face, neck, bilateral upper and lower extremities, chest, abdomen, back, and feet (Figures 1–4). A punch biopsy was performed.
What Is The Diagnosis?
Check your answer below.
Diagnosis
Pityriasis Lichenoides Chronica
Pityriasis lichenoides includes two main variants: pityriasis lichenoides and varioliformis acuta (PLEVA) and pityriasis lichenoides chronica (PLC). PLC is more prevalent in the pediatric population, but it can affect all age groups, races, and geographic regions. There is a male predominance.1 The etiology of PLC is unknown; however, it is postulated that it may be a response to foreign antigens, such as infectious agents or drugs. Lesions biopsied from patients with PLC demonstrate T-cell infiltrates; CD4+ cells, to be specific.1
Clinical Presentation and Histology
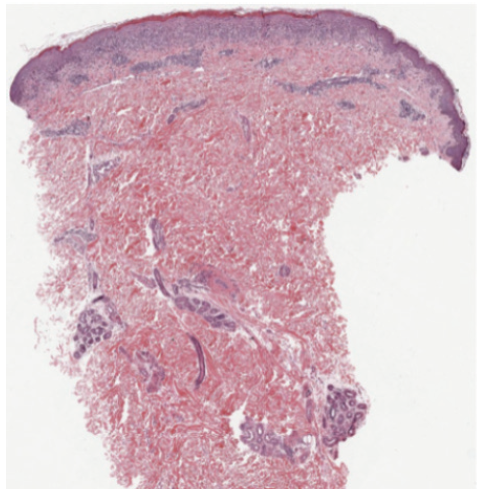
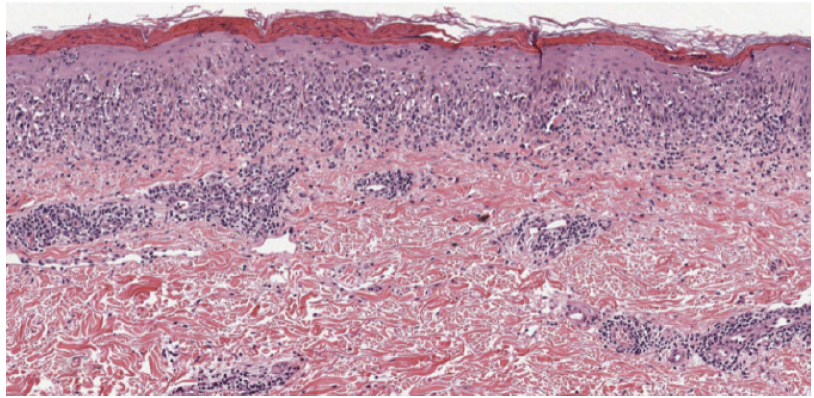
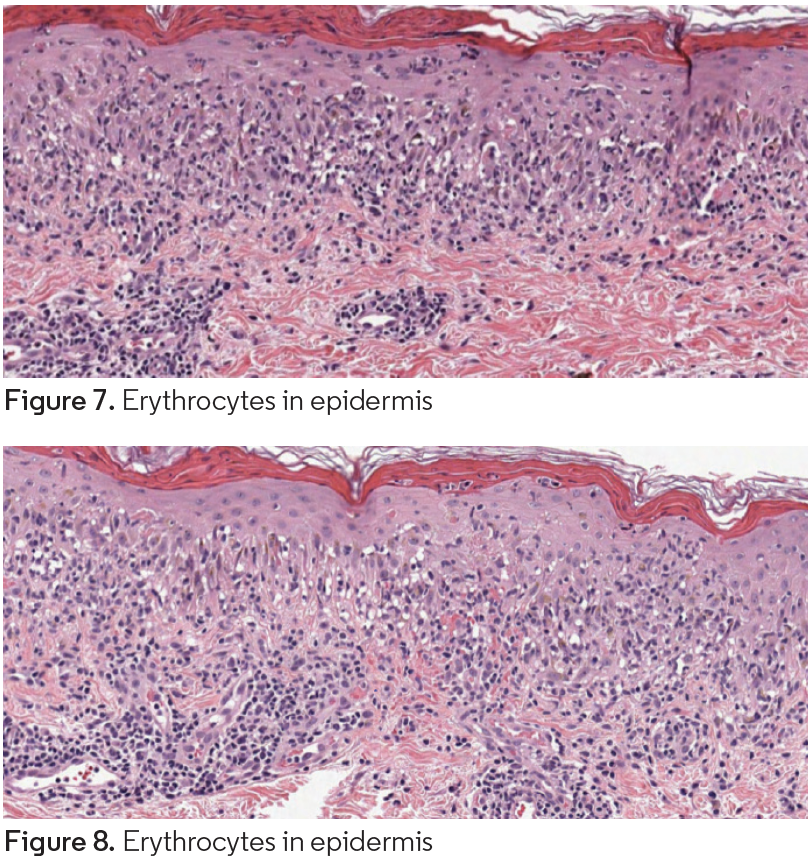
PLC presents as recurrent crops of spontaneously regressing erythematous to purpuric papules. These papules are commonly scaly as compared with the lesions in PLEVA, which are commonly crusted, ulcerated, and occasionally vesicular or pustular. The lesions often regress over weeks to months; however, patients will commonly relapse. It is hypothesized that the distribution of the lesions is more important than the acute or chronic nature. Patients with a diffuse distribution of lesions tend to have a shorter average disease course of approximately 11 months, compared with patients with a peripheral distribution who have a longer average disease course of approximately 33 months.1 Diagnosis requires histopathologic evaluation. PLC exhibits a superficial perivascular interface dermatitis. Lymphocytes predominate in the infiltrate, although neutrophils are sometimes present as well. Within the epidermis, there is focal parakeratosis and evidence of damage that ranges from edema to extensive epidermal necrosis. Frequently, there is extravasation of erythrocytes. All these changes are blunted in more chronic lesions.1
Differential Diagnosis
The differential diagnosis for PLC includes PLEVA, erythema multiforme, guttate psoriasis, lichen planus, pityriasis rosea, lymphomatoid papulosis, and papular dermatitis.
Treatment
There are no established treatment guidelines for PLC. First-line therapy often consists of topical steroids, which are rarely effective as monotherapy. Topical coal tar products, oral tetracyclines used for their anti-inflammatory properties, erythromycin, and various types of phototherapy may be considered.1 Azithromycin has also been used instead of erythromycin, particularly in children, due to an easier dosing schedule and better systemic absorption and tissue penetration.2 More extensive disease may require methotrexate; however, this is rarely used. Despite treatment, many patients continue to exhibit pigmentary alteration, either hypo- or hyperpigmentation, after the primary lesion has subsided.
Our Patient
The patient had a punch biopsy from the left thigh that was consistent with PLC (Figures 5–8). She was started on 3 courses of azithromycin over 6 weeks and referred for phototherapy. She received phototherapy 3 times weekly for approximately 1.5 months. After this course of phototherapy, she had developed no new lesions and old lesions were healing, although they did exhibit post inflammatory hyperpigmentation. She was started on doxycycline 100 mg daily.
Conclusion
More prevalent in the pediatric population, PLC is a condition that is difficult to control because there are no specific therapy guidelines, and many patients often chronically relapse. Phototherapy in combination with oral azithromycin and/or topical corticosteroids may be beneficial in the treatment of PLC.
References
- Pityriasis lichenoides et varioliformis acute and pityriasis llchenoides chronica. In: Bolognia J, Jorizzo JL, Rapini RP. Dermatology. 2nd ed. Mosby/Elsevier; 2008: 163-166.
- Geller L, Antonov NK, Lauren CT, Morel KD, Garzon MC. Pityriasis lichenoides in childhood: review of clinical presentation and treatment options. Pediatr Dermatol. 2015;32(5):579-592. doi:10.1111/pde.12581
- Zang JB, Coates SJ, Huang J, Vonderheid EC, Cohen BA. Pityriasis lichenoides: long-term follow-up study. Pediatr Dermatol. 2018;35(2):213-219. doi:10.1111/pde.13396







