


What Is This Tender Nodule in the Umbilicus?
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of The Dermatologist or HMP Global, their employees, and affiliates.
Case Report

A 32-year-old-woman was referred to the dermatology clinic for evaluation of an umbilical lesion. The lesion was present for a few years and associated with stabbing umbilical pain and clear discharge around the time of her menstrual cycle. She had a history of endometriosis and previously underwent laparoscopic surgery for treatment. She also had a surgical history of 2 cesarean sections and a laparoscopic appendectomy. The patient’s primary care physician recommended thorough hygiene of the area and prescribed nystatin cream, which did not alleviate her symptoms. On exam, a rm, 6-mm, pinkbrown, bilobed, exophytic papule was present on the inferolateral umbilicus. The lesion had a rubbery texture and was firmly adhered to the underlying skin (Figure 1). Circular scars around the umbilicus from her prior laparoscopic surgeries were also noted. Close-up view utilizing a dermatoscope revealed a glistening surface with a central indentation and fine peripheral scale (Figure 2).
What’s Your Diagnosis?
Continue below for the answer.
Diagnosis:
Cutaneous Endometriosis
Endometriosis is the implantation of endometrial tissue into extrauterine sites. Cutaneous endometriosis is a rare form of the disease that occurs when ectopic endometrial tissue is implanted in the skin, representing 0.5% to 1% of all cases of endometriosis.1 It is an uncommon manifestation of endometriosis often misdiagnosed due to its rarity. Endometriosis is due to reflux of menstrual secretions, hematogenous or lymphatic spread, or induction/transformation of progenitor cell lines.2 Due to the lack of a diagnostic algorithm, the average delay to diagnosis for those with “simple/classic” endometriosis is 4 to 11 years.3
Clinical Presentation
The classic triad of cutaneous endometriosis is an abdominal mass associated with cyclical pain and discharge and a history of abdominal surgery.4 It usually presents as a single lesion in women between the ages of 20 and 45 years, with an average size of 2 to 3 cm.4 Lesions often arise in scars from gynecologic surgery and can vary in color from flesh-colored to red or blue.5 It is speculated that laparoscopic instrumentation of the abdomen can lead to transplantation of endometrial tissue from the uterus to the abdominal wall or subcutis during surgical trocar removal, which then leads to cutaneous endometriosis.6 Trocars are often inserted within, and surrounding, the umbilicus during laparoscopic gynecologic surgery, which likely explains the umbilical localization of endometrial tissue in this case.7
Although endometriosis itself is relatively common and affects 10% to 15% of women of childbearing age, cutaneous endometriosis is rare and represents less than 1% of overall cases of endometriosis.4 It is further subdivided into primary and secondary types. In primary cutaneous endometriosis, patients have no surgical history. In secondary cutaneous endometriosis, patients have a history of abdominal surgery. Most cases are secondary in nature although, interestingly, most patients do not have a history of endometriosis at the time they are diagnosed.4 The most common location for cutaneous endometriosis to occur is the umbilicus, which is referred to as a Villar nodule, named after the first person to describe the entity.8,9
Histopathology
Histology reveals endometrial glands with apocrine-like secretion in a myxoid stroma.5 Extravasated erythrocytes and hemosiderin may also be seen.5
Differential Diagnosis
The differential diagnosis is wide and includes scar, umbilical hernia, omphalitis, pyogenic granuloma, Sister Mary Joseph nodule, squamous cell carcinoma, and melanoma, among others. One study revealed that the initial diagnosis is incorrect in most cases, with fibroma, incisional hernia, granuloma, chronic omphalitis, or neuropathic pain being the most frequent initial diagnosis.4 Given that many patients have a history of abdominal surgery, the general surgery department is most frequently initially consulted (79% of cases), followed by gynecology (21% of cases).4 Most patients who are evaluated by general surgical practitioners undergo fine needle aspiration to obtain a diagnosis, outlining the important role that dermatologists can play in obtaining an expedient diagnosis via shave biopsy in these patients.4
Treatment
Treatments include hormonal therapy to shrink endometrial tissue, surgical excision, or hysterectomy.10
Our Patient
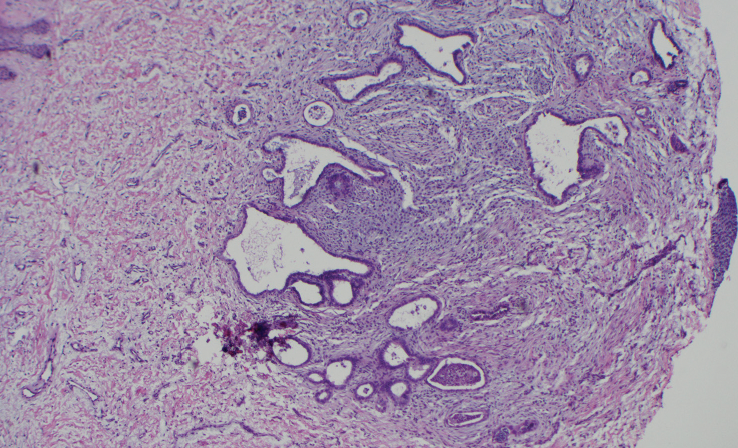
A shave biopsy of the lesion was performed, which showed a deep dermal nodule composed of apocrine glands in a myxoid stroma consistent with a diagnosis of cutaneous endometriosis (Figure 3 and Figure 4). The patient’s symptoms greatly improved following biopsy, and she was treated with a contraceptive implant by her primary care physician, which led to further symptomatic relief. She has not required further surgical intervention for her endometriosis and has not developed any new cutaneous lesions.
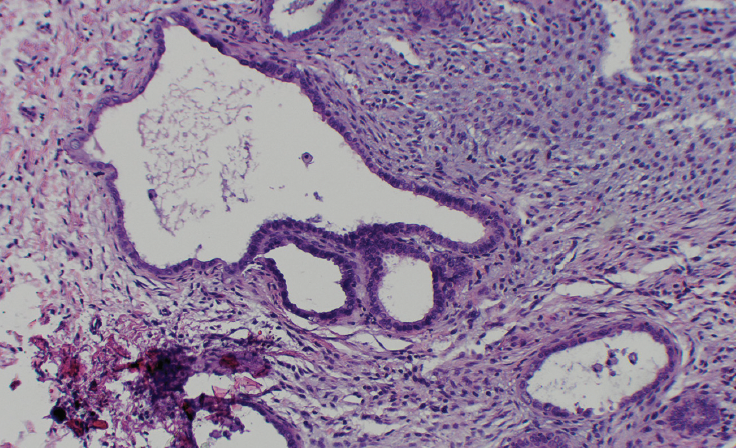
with active secretion, H&E stain, 400x magnification.
Conclusion
Given its rarity as an entity, cutaneous endometriosis is often misdiagnosed initially, which leads to a delay in diagnosis and treatment. Cutaneous endometriosis should be on the differential diagnosis for any female patient presenting with cyclically painful cutaneous lesions, particularly if they have a history of abdominal surgery. Untreated cutaneous endometriosis can have a significant impact on a patient’s quality of life, highlighting the important diagnostic role dermatologists can play in recognizing and diagnosing this condition.
Acknowledgments
Dr Pruneda is a PGY4 resident in the department of dermatology at Texas Tech University Health Sciences Center in Lubbock, TX. Kush Maheshwari is a fourth-year medical student at Baylor College of Medicine in Houston, TX. Dr Tarbox is an associate professior in the department of dermatology at Texas Tech University Health Sciences Center in Lubbock, TX.
References
1. Jaime TJ, Jaime TJ, Ormiga P, Leal F, Nogueira OM, Rodrigues, N. Umbilical endometriosis: report of a case and its dermoscopic features. An Bras Dermatol. 2013;88(1):121-124. doi:10.1590/S0365-05962013000100019
2. Burney RO, Giudice LC. Pathogenesis and pathophysiology of endometriosis. Fertil Steril. 2012;98(3):511-519. doi:10.1016/j.fertnstert.2012.06.029
3. Agarwal SK, Chapron C, Giudice LC, et al. Clinical diagnosis of endometriosis: a call to action. Am J Obstet Gynecol. 2019;220(4):354.e1-354.e12. doi:10.1016/j.ajog.2018.12.039
4. Lopez-Soto A, Sanchez-Zapata MI, Martinez-Cendan JP, Ortiz Reina S, Bernal Mañas CM, Remezal Solano M. Cutaneous endometriosis: presentation of 33 cases and literature review. Eur J Obstet Gynecol Reprod Biol. 2018;221:58-63. doi:10.1016/j.ejogrb.2017.11.024
5. Rapini RP. Miscellaneous remnants and neoplasms. In: Rapini RP. Practical Dermatopathology. 3rd ed. Elsevier; 2021.
6. Jubanyik K, Comite F. Extrapelvic endometriosis. Obstet Gynecol Clin North Am. 1997;24(2):411-440. doi:10.1016/s0889-8545(05)70311-9
7. Alkatout I, Mettler L, Maass N, Noé GK, Elessawy M. Abdominal anatomy in the context of port placement and trocars. J Turk Ger Gynecol Assoc. 2015;16(4):241-251. doi:10.5152/jtgga.2015.0148
8. Loh SH, Lew BL, Sim WY. Primary cutaneous endometriosis of umbilicus. Ann Dermatol. 2017;29(5):621-625. doi:10.5021/ad.2017.29.5.621
9. Victory R, Diamond MP, Johns DA. Villar’s nodule: a case report and systematic literature review of endometriosis externa of the umbilicus. J Minim Invasive Gynecol. 2007;14(1):23-32. doi:10.1016/j.jmig.2006.07.014
10. Zondervan KT, Becker CM, Koga K, Missmer SA, Taylor RN, Viganò P. Endometriosis. Nat Rev Dis Primers. 2018;4(1):9. doi:10.1038/s41572-018-0008-5








