


Spongiotic Dermatitis: Differential Diagnosis and Elusive Etiology
Spongiotic dermatitis is a histologic diagnosis that comprises a broad rubric of many different entities. Although extremely common, few diagnoses are more frustrating for dermatologists.1 Pathologists will attest that this diagnosis can only be made with certainty via biopsy. However, most dermatopathologists also find spongiotic dermatitis frustrating because making the diagnosis from a histopathologic standpoint often entails additional workup and an unsatisfying final line diagnosis that is more of a differential than a definitive diagnosis.

It is a rare day when I do not see at least 1 patient with a clinical presentation consistent with spongiotic dermatitis. As a dermatologist, I have come to embrace this diagnosis. It has humbled me far too many times to recount, but I now take comfort in knowing that even if the etiology eludes us, sometimes it is satisfying enough to simply provide reassurance to the patient that their rash will almost always be self-limited and generally resolve without sequelae. Moreover, the signs and symptoms of spongiotic dermatitis are usually responsive to treatment.
Etiology
Owing to its ubiquity, the clinical presentation of spongiotic dermatitis remains one of the most variable in the dermatology clinic. Sometimes it is focal and sometimes, widespread. It is usually pruritic but certainly not always. At times the diagnosis is a slam dunk, such as when the patient says, “I was gardening last week and came in contact with poison ivy. This happens every spring.” Obviously, no biopsy or further diagnostic workup is necessary for this patient. And then there are those cases of spongiotic dermatitis that are not so straightforward. These are frustrating for both the patient and the provider. Does the patient have a lifelong history of atopic dermatitis? If that is the case, then the current presentation could simply be an acute fl are of their existing disease. Or this could be contact dermatitis as seen in the first example but in a patient with atopic dermatitis. Did the patient start a new medication or is he or she allergic to a particular food?
Indeed, contact dermatitis is the most common reason for a patient’s spongiotic dermatitis presentation, but proving that and subsequently identifying the allergen can be challenging. Is the patient’s rash the result of a viral infection—COVID-19 perhaps?2 Or maybe this presentation of apparent spongiotic dermatitis is due to the COVID-19 vaccine.3 Sometimes spongiotic dermatitis presents when there is an active infection elsewhere on the body. This is known as an id reaction, as seen in scabies.4 Additionally, there are chronic and acute cutaneous infections, such as dermatophytosis, that present exactly as spongiotic dermatitis.
In some cases, clinically determining that spongiotic dermatitis is superficial and primarily of an epidermal nature is not apparent. In other words, is the rash emanating from deeper inside the skin, known as a dermal hypersensitivity reaction? Although quite different from a histologic standpoint, but often similar clinically, spongiotic dermatitis can easily be confused with a dermal hypersensitivity reaction. In and of itself, dermal hypersensitivity reaction is a source of confusion.5 Like spongiotic dermatitis, precisely identifying the source of a dermal hypersensitivity reaction can leave clinicians and patients alike absolutely fl ummoxed. Some of the most notable causes of dermal hypersensitivity reaction are adverse drug reaction and food allergy, but clinicians also need to consider connective tissue disease, malignancy, and a plethora of other possible culprits.
Histology
When looking at the skin biopsy, spongiosis is the finding of keratinocytes in the stratum spinosum with their tight junctions slightly splayed apart—the sine qua non of the diagnosis. Splaying may be seen to such a degree that frank vesiculation is observed. I refer to this as florid spongiotic dermatitis, a finding normally seen in hand eczema or dyshidrotic eczema (pompholyx). If eosinophils are also present, which commonly occurs, the possibility of contact dermatitis is increased. However, a whole host of additional possibilities should be considered in the setting of eosinophilic spongiotic dermatitis, including bullous pemphigoid (or the urticarial phase of bullous pemphigoid), pemphigus (vulgaris and foliaceus), arthropod assault (bug/insect bite), herpes gestationis, scabies (or other parasitic infestation), and incontinentia pigmenti (in the appropriate setting).
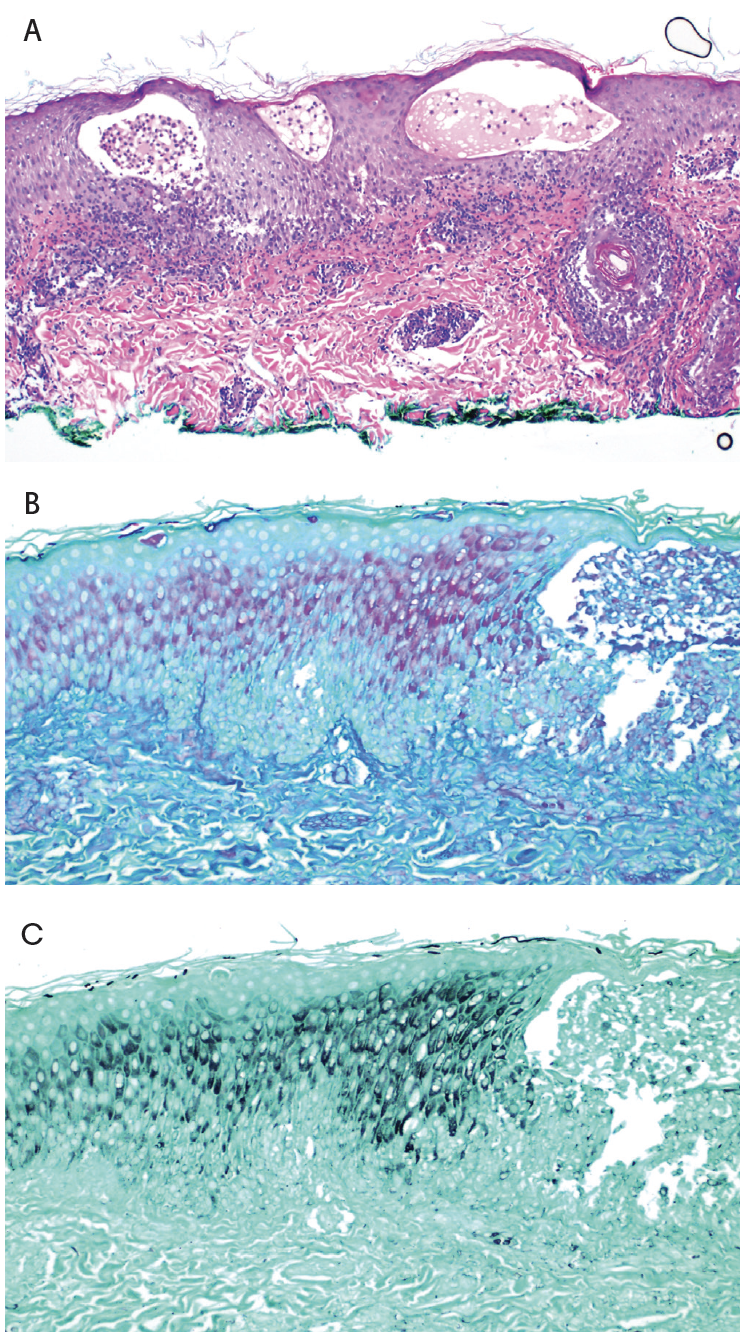
Because of this broad differential, there is a tendency for some clinicians to discount the result of the biopsy and deem it unhelpful, especially in the setting of a frustrated patient with an enigmatic rash. The clinician’s frustration may increase further after a confirmed histologic diagnosis of spongiotic dermatitis. Often, the only added piece of evidence to the dermatologist’s workup is that a periodic acid–Schiff (PAS) stain was performed and found to be negative, which usually, but not always, indicates the absence of dermatophytosis (tinea infection). Figure 1 shows a case of florid spongiotic dermatitis where special stains (PAS and Gomori methenamine silver) were used to confirm the diagnosis of dermatophytosis. Instead of frustration, this is where I embrace the diagnosis and am grateful that the histology did not show evidence of mycosis fungoides or some other rare but more serious mimicker of spongiotic dermatitis. And I am even more thankful to learn that it is not a vexing dermal hypersensitivity reaction, which is usually more difficult to manage and even more elusive in its etiology.
Compassionate Care
Unfortunately, due to long wait times in dermatology, it occurs all too frequently that the rash has already resolved by the time of the patient’s appointment. Provide reassurance and spend some time validating their concerns, as well as making a bona fide effort to help them determine the cause. Working up a suspected diagnosis of spongiotic dermatitis should always be accompanied by an abundance of patience and compassion.
References
1. Cohen JN, Bowman S, Laszik ZG, North JP. Clinicopathologic overlap of psoriasis, eczema, and psoriasiform dermatoses: a retrospective study of T helper type 2 and 17 subsets, interleukin 36, and beta-defensin 2 in spongiotic psoriasiform dermatitis, sebopsoriasis, and tumor necrosis factor alpha inhibitor-associated dermatitis. J Am Acad Dermatol. 2020;82(2):430-439. doi:10.1016/j.jaad.2019.08.023
2. Seike I, Kanamori H, Oshima K, Aoyagi T. Maculopapular rash in Japanese patients with COVID-19. Intern Med. 2022;61(7):1113-1114. doi:10.2169/internalmedicine. 8491-21
3. Zafar M, Ewnetu B, Ahmed S, Iqbal U, Whitehead M. COVID-19 vaccination-induced rash: does the choice of vaccine matter? Cureus. 2021;13(6):e15490. doi:10.7759/cureus.15490
4. Bertoli MJ, Schwartz RA, Janniger CK. Autoeczematization: a strange id reaction of the skin. Cutis. 2021;108(3):163-166. doi:10.12788/cutis.0342
5. LeBoit PE. The last refuge of scoundrels. Am J Dermatopathol. 2004;26(6):516-517. doi:10.1097/00000372-200412000-00016









