Atopic Dermatitis in Patients With Skin of Color
Introduction
Atopic dermatitis (AD), or eczema, is a chronic inflammatory disease characterized by itchy, xerotic lesions. The 2012 National Health Interview Survey reported a prevalence of 12% among children in the United States, with a greater prevalence in patients with skin of color (persons of African, Asian, Hispanic/Latino, Middle Eastern, and/or Native American ancestry).1 Previous reports from the 2003 National Survey of Children’s Health indicate AD prevalence affected 16% of black children compared with 9.7% of white children (overall prevalence 10.7%).2
Additional epidemiologic studies, such as Henderson et al,3 confirm these findings. In this study, clinicians reviewed pediatric dermatology visits over a 10-year period to evaluate racial disparities across diagnoses. According to their report, the most common diagnoses were consistent (acne, dermatitis, warts) among all race/ethnicities, yet the disease prevalence differed, with unspecified dermatitis constituting 29% of office visits in black patients, 29.1% in Asian patients, and 13.1% in white patients.3 Racial disparities in AD prevalence have been observed in other studies.4-7
Pathogenesis
AD is a common skin condition generally associated with other atopic disorders (allergic rhinitis, asthma).8 The precise pathogenesis of the disease remains unclear; however, the central premise of disease lies in the dysfunction of the skin barrier. AD pathogenesis is now thought to be a multifactorial disease process involving epidermal permeability, environmental factors, neural network, and immune response.9, 10
Recent breakthroughs in AD research have demonstrated racial differences in genetic factors contributing to AD disease and progression. For example, studies have shown a lower value of ceramide-to-cholesterol ratio among black patients (0.8) compared with Asians (2.1) and white patients (1.7), as well as elevated transepidermal water loss across normal black skin, not just affected patients with AD.11,12 These findings, which contribute to barrier disruption, may explain the higher rates of AD among patients with skin of color, particularly black patients.
The most recent breakthrough in AD research in patients with skin of color is the identification of genetic defects in filaggrin and its variants, which are associated with more persistent disease.13, 14 These genetic defects and reported differences in neural pathways may explain why patients with skin of color present to dermatologists with characteristically different reports of itch from other races.15
Disease States
The clinical presentation of AD differs according to stage (acute and chronic) and age.16 Infants may present with generalized or localized disease, often confined to the cheeks and extensor surfaces, sparing the genital region.16
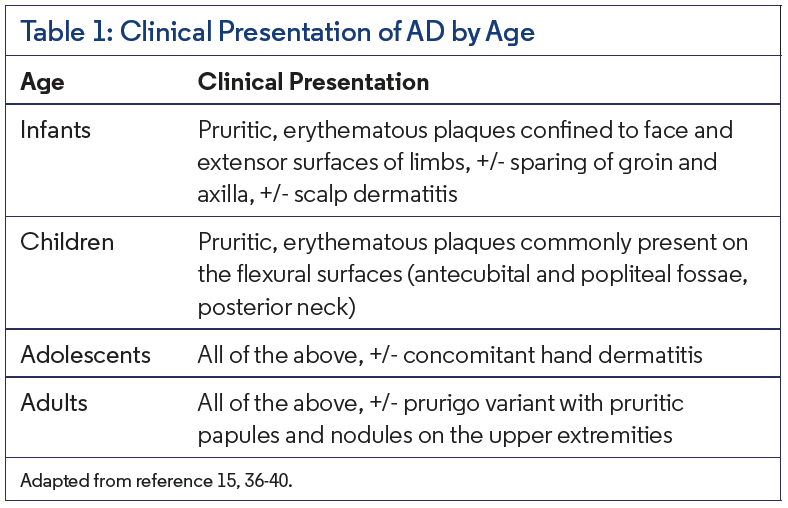
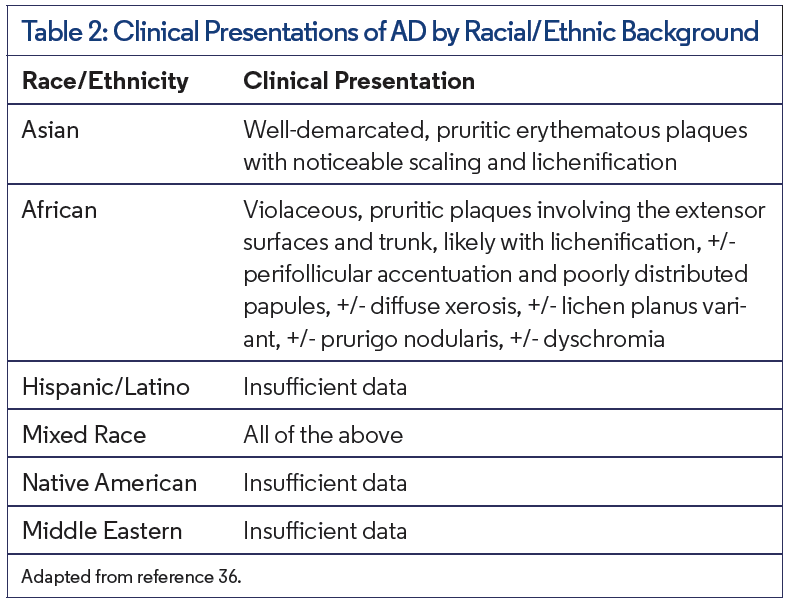
The most common findings in children, adolescents, and adults include flexural dermatitis of the antecubital and popliteal fossae and the prurigo variant with pruritic papules and nodules (Table 1).16 In patients with skin of color, AD may have an atypical clinical presentation given the varied skin types present. Active AD in black patients may present as scattered papular lesions on the extensors and trunk with annular configuration.15 However, lesions on the flexural regions are still possible in this group. Chronic AD may be characterized by prurigo nodularis and lichenification (Table 2).15
In patients with fair skin types, practitioners can depend on erythema, chronic and/or recurrent pruritus, and flexural dermatitis as reliable indicators of active disease. In dark-skinned patients, it can be difficult to assess for erythema. In this patient population, it may be best if providers rely on patient reports of reddened skin or evidence of post-inflammatory hyperpigmentation (PIH) rather than erythema.15
Other Considerations
Patients with skin of color are more likely to present to a dermatologist with concerns regarding dyschromia from eczema. Persistent hypopigmentation is commonly seen in dark-skinned patients with a history of severe, long-standing AD.15, 17 In many cases, PIH is the primary concern. In 1983, Halder et al identified the trend of patients with skin of color pursuing dermatologic care for pigment changes.18
This patient preference to address PIH along with atopic disease control may present a particular challenge to the dermatologist who may not understand the cultural concerns that can impact management. In patients of African descent, there may be use of over-the-counter products promoted for dry skin, such as cocoa butter, shea butter, oils, and other “organic” options, as therapeutic treatment for AD. Patients may continue to use these topical therapies in addition to their prescription topical medications, further aggravating their skin and complicating care. For all patients with AD, but particularly patients with skin of color, it is imperative that providers discuss the patient’s skin care regimen.
Treatments
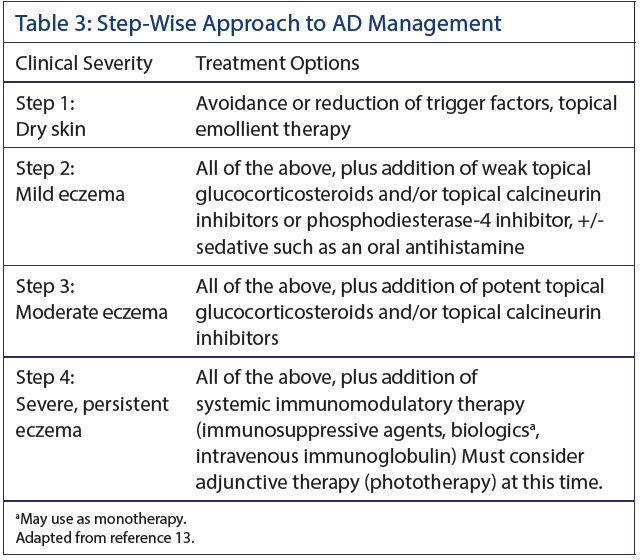
Successful treatment of AD requires several different approaches regardless of race/ethnicity (Table 3).15 Yet, a clear understanding of cultural practices and preferences may play an important role in disease management. Studies show that patient preferences for vehicle or certain drugs may differ across demographics.4,19 For example, Hispanic patients may prefer home remedies or complementary and alternative medicine as treatment options.4, 20, 21 This is an important consideration when establishing a therapeutic regimen for AD in patients with skin of color. Studies have also shown a lower adherence to medication among adult black patients diagnosed with AD, despite higher disease severity.4, 22, 23 These findings suggest any of the following: a mistrust of treatment, misunderstanding of treatment or severity in disease course, lack of trust in provider, and/or frustration with treatment regimen. At the very least, the findings support the idea of patient preferences strongly affecting medication adherence, and therefore treatment success.
Treatment of mild eczema involves the use of hydrating emollients, topical corticosteroids, or calcineurin inhibitors, and avoiding any known provocation factors.15, 24 Topical corticosteroids are frequently used as first-line therapy in AD. There is a risk of hypopigmentation from long-term steroid use. However, hypopigmentation in dark-skinned patients with AD is more likely to be associated with post-inflammatory changes from their disease rather than from steroid use.15 Topical calcineurin inhibitors are often used as monotherapy in maintenance therapy.24 Eichenfield et al25 evaluated the efficacy of pimecrolimus among children and infants with AD and found that the race/ethnicity of the patient had no effect on treatment outcome. Those patients diagnosed with mild eczema may also benefit from oral sedatives such as antihistamines or antidepressants (doxepin) to help minimize pruritus, especially at bedtime.
In moderate disease states, patients are typically started on higher potency topical steroids and/or topical calcineurin inhibitors. These patients may also benefit from adjunct therapy, such as antimicrobial agents for bacterial infection, bleach baths for prevention of microbial colonization, and UV light (narrowband UV-B).24 Fitzpatrick skin type may influence the efficacy of phototherapy as demonstrated in Ravnbak et al26 and Jacobe et al.27 Ravnbak et al found that an increased dose of narrowband UV-B is required in patients with darker skin types,26 while Mok et al demonstrated standard dose narrowband UV-B and UV-A/narrowband UV-B are effective therapies in Asian pediatric populations.28
Lastly, practitioners should consider topical crisaborole (Eucrisa), a phosphodiesterase-4 inhibitor, for use in patients with skin of color and mild or moderate AD. Studies have shown crisaborole to be an effective treatment option, with higher proportions of black and Hispanic patients attaining clear to almost clear disease with crisaborole compared with vehicle.2,29, 30
In patients presenting with severe, persistent eczema the management can be particularly challenging. Systemic medications, such as methotrexate, azathioprine, and cyclosporine, are often used in this patient group. Methotrexate is an effective therapeutic option. However, some patients may experience adverse side effects with use. Black patients, in particular, have an increased risk of alopecia with use of methotrexate. This is likely a consequence of genetic polymorphisms observed in those of African descent, which are responsible for methotrexate toxicity.31 Azathioprine has been shown to improve severe AD.15, 32 Metabolism of azathioprine is affected by thiopurine methyltransferase enzyme (TPMT) activity. TPMT deficiency is prevalent among blacks, thus placing this population at risk for severe toxicity if treated with conventional dosages of azathioprine.33,34 Providers should obtain a TPMT level prior to initiating therapy with azathioprine and utilize ongoing blood monitoring. Cyclosporine can be prescribed for short-term use in severe, recalcitrant AD.15 Oral bioavailability of cyclosporine in blacks is 20% to 50% lower than in whites, requiring a higher dosage to maintain adequate concentrations.35
Additional off-label therapies for severe AD include mycophenolate mofetil or dapsone.15 Given the risk for hemolytic anemia with dapsone use in glucose-6-phosphate dehydrogenase (G6PD) deficient patients, it is recommended that providers obtain a serum G6PD level prior to starting dapsone and monitor blood counts.15
The newest treatment option for moderate to severe AD is dupilumab (Dupixent), a monoclonal antibody that was recently approved by the FDA for use in adults and children aged 12 years and older. Studies demonstrate significant improvement in severity and symptoms of AD, with comparable results among all races and ethnicities.36
Affiliations and Disclosures
Dr De Souza is a clinical research fellow in the dermatology department at Wake Forest Baptist Medical Center in Winston-Salem, NC.
Dr McMichael, Hair and Scalp Section Editor, is professor and chair of the department of dermatology at Wake Forest Baptist Medical Center.
Disclosures: Dr De Souza reports no relevant financial relationships. Dr McMichael has received grants from Allergan and Proctor & Gamble. She is a consultant for Aclaris, Allergan, Bioniz, Cassiopea, Covance, eResearch Technology, Inc, Galderma, Guthey Renker, Incyte, Johnson & Johnson, Merck & Co, Inc, Merz Pharmaceuticals, Pfizer, Proctor & Gamble, and Samumed. She receives royalties from Informa Healthcare and UpToDate and also has conducted research for Cassiopea and Samumed.
References
- Strom MA, Silverberg JI. Utilization of preventive health care in adults and children with eczema. Am J Prevent Med. 2016;50(2):e33-e44. doi:10.1016/j.amepre.2015.07.029
- Shaw TE, Currie GP, Koudelka CW, Simpson EL. Eczema prevalence in the United States: Data from the 2003 National Survey of Children’s Health. J Invest Dermatol. 2011;131(1):67-73. doi:10.1038/jid.2010.251
- Henderson MD, Abboud J, Cogan CM. Skin‐of‐color epidemiology: A report of the most common skin conditions by race. Pediatr Dermatol. 2012;29(5):584-589. doi:10.1111/j.1525-1470.2012.01775.x
- Davis SA, Narahari S, Feldman SR, Huang W, Pichardo-Geisinger RO, McMichael AJ. Top dermatologic conditions in patients of color: An analysis of nationally representative data. J Drugs Dermatol. 2012;11(4):466-473.
- Davis LR, Marten RH, Sarkany I. Atopic eczema in European and Negro West Indian infants in London. Br J Dermatol. 1961;73(11):410-414.
- Schachner L, Ling NS, Press S. A statistical analysis of a pediatric dermatology clinic. Pediatr Dermatol. 1983;1(2):157-164.
- Williams HC, Pembroke AC, Forsdyke H, Boodoo G, Hay RJ, Burney PG. London-born black Caribbean children are at increased risk of atopic dermatitis. J Am Acad Dermatol. 1995;32(2):212-21
- Akdis CA, Akdis M, Bieber T, et al. Diagnosis and treatment of atopic dermatitis in children and adults: European Academy of Allergology and Clinical Immunology/American Academy of Allergy, Asthma and Immunology/PRACTALL Consensus Report. J Allergy Clin Immunol. 2006;118(1):152-169.
- Mollanazar NK, Smith PK, Yosipovitch G. Mediators of chronic pruritus in atopic dermatitis: getting the itch out? Clin Rev Allergy Immunol. 2016;51(3):263-292.
- Peng W, Novak N. Pathogenesis of atopic dermatitis. Clin Exp Allergy. 2015;45(3):566-574. doi:1111/cea.12495
- Jungersted JM1, Høgh JK, Hellgren LI, Jemec GB, Agner T. Ethnicity and stratum corneum ceramides. Br J Dermatol. 2010;163(6):1169–1173. doi:10.1111/j.1365-2133.2010.10080.x.
- Proksch E, Fölster-Holst R, Bräutigam M, Sepehrmanesh M, Pfeiffer S, Jensen JM. Role of the epidermal barrier in atopic dermatitis. J Dtsch Dermatol Ges. 2009;7(10):899–910. doi:10.1111/j.1610-0387.2009.07157.x
- Palmer CN, Irvine AD, Terron-Kwiatkowski, et al. A common loss‐of‐function variants of the epidermal barrier protein filaggrin are a major predisposing factor for atopic dermatitis. Nat Genet. 2006;38(4):441-446. doi:10.1038/ng1767
- Margolis DJ, Mitra N, Gochnauer H, et al. Uncommon filaggrin variants are associated with persistent atopic dermatitis in African Americans. J Invest Dermatol. 2018;138(7):1501-1506. doi:10.1016/j.jid.2018.01.029
- Vachiramon V, Tey HL, Thompson AE, Yosipovitch G. Atopic dermatitis in African American children: Addressing unmet needs of a common disease. Pediatr Dermatol. 2012;29(4):395-402. doi:10.1111/j.1525-1470.2012.01740.x
- Werfel T, Schwerk N, Hansen G, Kapp A. The diagnosis and graded therapy of atopic dermatitis. Dtsch Arztebl Int. 2014;111(29-30):509-520. doi:10.3238/arztebl.2014.0509
- Ortonne J. Vitiligo and other disorders of hypopigmentation. In: Bolognia JL, Jorizzo JL, Rapini RP, et al, eds. Dermatology. 2nd ed. London, England: Mosby Elsevier; 2008:913-938.
- Halder RM, Grimes PE, McLaurin CI, Kress MA, Kenney JA. Incidence of common dermatoses in a predominantly black dermatologic practice. Cutis. 1983;32(4):388-390.
- Ransford HE, Carrillo FR, Rivera Y. Health care-seeking among Latino immigrants: blocked access, use of traditional medicine, and the role of religion. J Health Care Poor Underserved. 2010;21(3):862-878. doi:10.1353/hpu.0.0348
- Ou HT, Feldman SR, Balkrishnan R. Understanding and improving treatment adherence in pediatric patients. Semin Cutan Med Surg. 2010;29(2):137-140. doi:10.1016/j.sder.2010.03.012
- Horii KA, Simon SD, Liu DY, Sharma V. Atopic dermatitis in children in the United States, 1997-2004: Visit trends, patient and provider characteristics, and prescribing patterns. Pediatrics. 2007;120(3):e527-e534. doi:10.1542/peds.2007-0289
- Fisher EJ, Adams BB. African American and Caucasian patients’ vehicle preference for the scalp. J Am Acad Dermatol. 2008;58(2 suppl):S46-S47. doi:10.1016/j.jaad.2006.05.020
- Feldman SR, Vallejos QM, Quandt SA, et al. Health care utilization among migrant Latino farmworkers: the case of skin disease. J Rural Health. 2009;25(1):98-103. doi:10.1111/j.1748-0361.2009.00205.x
- Ring J, Alomar A, Bieber T, et al. Guidelines for treatment of atopic eczema (atopic dermatitis) part I. J Eur Acad Dermatol Venereol. 2012;26(8):1045-1060. doi:10.1111/j.1468-3083.2012.04635.x
- Eichenfield LF, Lucky AW, Langley RG, et al. Use of pimecrolimus cream 1% (Elidel) in the treatment of atopic dermatitis in infants and children: The effects of ethnic origin and baseline disease severity on treatment outcome. Int J Dermatol. 2005;44(1):70-75. doi:10.1111/j.1365-4632.2004.02234.x
- Ravnbak MH, Wulf HC. Pigmentation after single and multiple UV‐exposures depending on UV‐spectrum. Arch Dermatol Res. 2007;299(1):25-32. doi:10.1007/s00403-006-0728-3
- Jacobe HT, Cayce R, Nguyen J. UVA1 phototherapy is effective in darker skin: A review of 101 patients of Fitzpatrick skin types I-V. Br J Dermatol. 2008;159(3):691-696. doi:10.1111/j.1365-2133.2008.08672.x
- Mok ZR, Koh MJ, Chong WS. Is phototherapy useful in the treatment of atopic dermatitis in Asian children? A 5‐year report from Singapore. Pediatr Dermatol. 2014;31(6)698-702. doi:10.1111/pde.12405
- Gold Stein LF, Eichenfield LF. Topical therapy for atopic dermatitis: New and investigational agents. Semin Cutan Med Surg. 2016;35(4S):S99-S102. doi:10.12788/j.sder.2017.050
- Callender VD, Alexis AF, Stein Gold LF, et al. Efficacy and safety of crisaborole ointment, 2%, for treatment of mild to moderate atopic dermatitis across racial and ethnic groups. Presented at: 2017 Academy of Dermatology and Venereology Congress; Sept 13-17, 2017; Geneva, Switzerland. Poster P0270.
- Ranganathan P, Culverhouse R, Marsh S, et al. Methotrexate (MTX) pathway gene polymorphisms and their effects on MTX toxicity in Caucasian and African American patients with rheumatoid arthritis. J Rheumatol. 2008;35(4):572–579.
- Meggitt SJ, Gray JC, Reynolds NJ. Azathioprine dosed by thiopurine methyltransferase activity for moderate‐to‐severe atopic eczema: A double‐blind, randomised controlled trial. Lancet. 2006;367(9513):839-846.
- Escousse A, Rifle G, Sgro C, Mousson C, Zanetta G, Chevet D. Azathioprine toxicity, 6‐mercaptopurine accumulation and the “poor” 6‐thiopurine methylator phenotype. Eur J Clin Pharmacol. 1995;48(3-4):309-310.
- McLeod HL, Lin JS, Scott EP, Pui CH, Evans WE. Thiopurine methyltransferase activity in American white subjects and black subjects. Clin Pharmacol Ther. 1994;55(1):15-20.
- Dirks NL, Huth B, Yates CR, Meibohm B. Pharmacokinetics of immunosuppressants: A perspective on ethnic differences. Int J Clin Pharmacol Ther. 2004;42(12):701-718.
- Kaufman, Bridget P, Guttman‐Yassky E, and Alexis AF. Atopic dermatitis in diverse racial and ethnic groups—Variations in epidemiology, genetics, clinical presentation and treatment. Exp Dermatol. 2018;27(4):340-357.
- Pugliarello S1, Cozzi A, Gisondi P, Girolomoni G. Phenotypes of atopic dermatitis. J Dtsch Dermatol Ges. 2011;9(1):12–20. doi:10.1111/j.1610-0387.2010.07508.x
- Tanaka M, Aiba S, Matsumura N, Aoyama H, Tagami H. Prurigo nodularis consists of two distinct forms: early‐onset atopic and late‐onset non‐atopic. Dermatology. 1995;190(4):269–276.
- Hanifin J, Rajka G. Diagnostic features of atopic dermatitis. Acta Derm Venereol. 1980;92(Suppl):44–47.
- Bieber T. Atopic dermatitis. N Engl J Med. 2008;358(14):1483–1494. doi:10.1056/NEJMra074081