


Tackling the Impossible: Psoriasis Treatment Algorithm Guided by Patients’ Preferences
The various presentations of psoriasis can make choosing from among the numerous treatment options overwhelming for patients and physicians. Treatment algorithms can help guide the decision.
Psoriasis remains one of the most common chronic inflammatory skin diseases, with worldwide prevalence ranging from 0.5% to 11.4% in adults. Psoriasis occurs in various clinical forms, including chronic plaque, guttate, pustular, erythrodermic, inverse, and nail psoriasis.1 The spectrum of manifestation ranges from asymptomatic to disabling and rarely life-threatening, with treatments ranging from observation to systemic and biologic therapy.
The various presentations of psoriasis can make choosing from among the numerous treatment options overwhelming for patients and physicians. Treatment algorithms can help guide the decision. This article describes psoriasis treatment algorithms based not only on the severity of the disease and widely accepted guidelines, but also on patients’ preferences for efficacy, price, and safety.
Initial Steps For All Patients
The first step in psoriasis management is addressing patients’ psychosocial needs, including the need to understand their disease. Initial counseling starts by providing patient education materials on how to manage symptoms and increase quality of life (QoL).
Referring patients to the National Psoriasis Foundation (NPF) provides not only basic patient education about psoriasis, but also a place for patients to connect with other patients. The American Academy of Dermatology also developed extensive 6-part guidelines on initial management of psoriasis patients. Psychosocial impact and evaluation of joints’ involvement should be a part of initial counseling.
Screening for Psoriatic Arthritis
Psoriatic arthritis (PsA) is common in patients with psoriasis and tends to begin years after psoriasis starts. Dermatologists can screen for early PsA. Asking patients about joint stiffness, joint
pain, or back pain is a sensitive way of identifying possible PsA. When there is suspected arthritis, physical examination should include a complete musculoskeletal examination including evaluation of range of motion and gait; x-ray evaluation of joints may also be warranted.
Therefore, if the dermatologist is not prepared to perform such a physical examination and order the radiological examinations, a suspicion of joint involvement may merit a referral to a rheumatologist. Dermatologists and rheumatologists should collaborate in choosing the ideal treatments for patients with psoriasis and PsA.
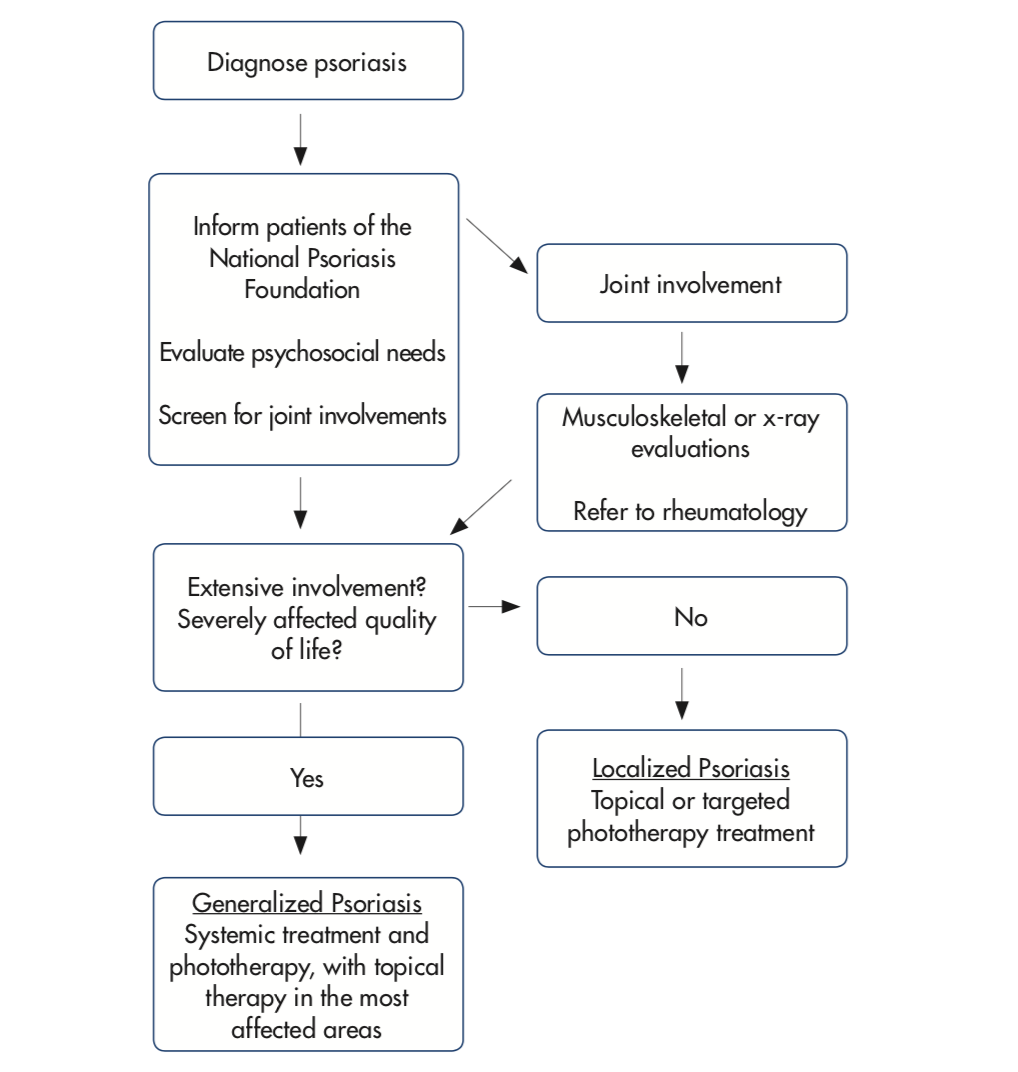
Figure 1. Initial psoriasis assessment and counseling.
Categorization of Patients
The initial categorization for treatment purposes classifies patients into limited or extensive psoriasis, depending on whether or not it is feasible to apply topical treatments to all affected areas. Assessments on body surface area involvement and QoL help determine the treatment algorithm (Figure 1).
Choosing the Therapies
Guiding factors (Table 1) when choosing treatment modalities include treatment characteristics that affect adherence, efficacy, side effect profiles, and cost; adherence is especially important for topical treatments.
Physicians and patients classically select treatments that strike a balance between these factors. However, patients often weigh these factors differently than the physician would. This guideline recommends medication selection guided by patients’ preference of which factor they find to be most important. As head-to-head comparisons of psoriasis treatments are sparse, this algorithm is largely opinion-based.
Localized Psoriasis
Algorithms for localized psoriasis depend on the specific areas of the body that are affected (Figure 2). Patients in this category typically use topical corticosteroids as first-line therapy.1 Synergistic combination treatment allows for lower exposure to each of its components.
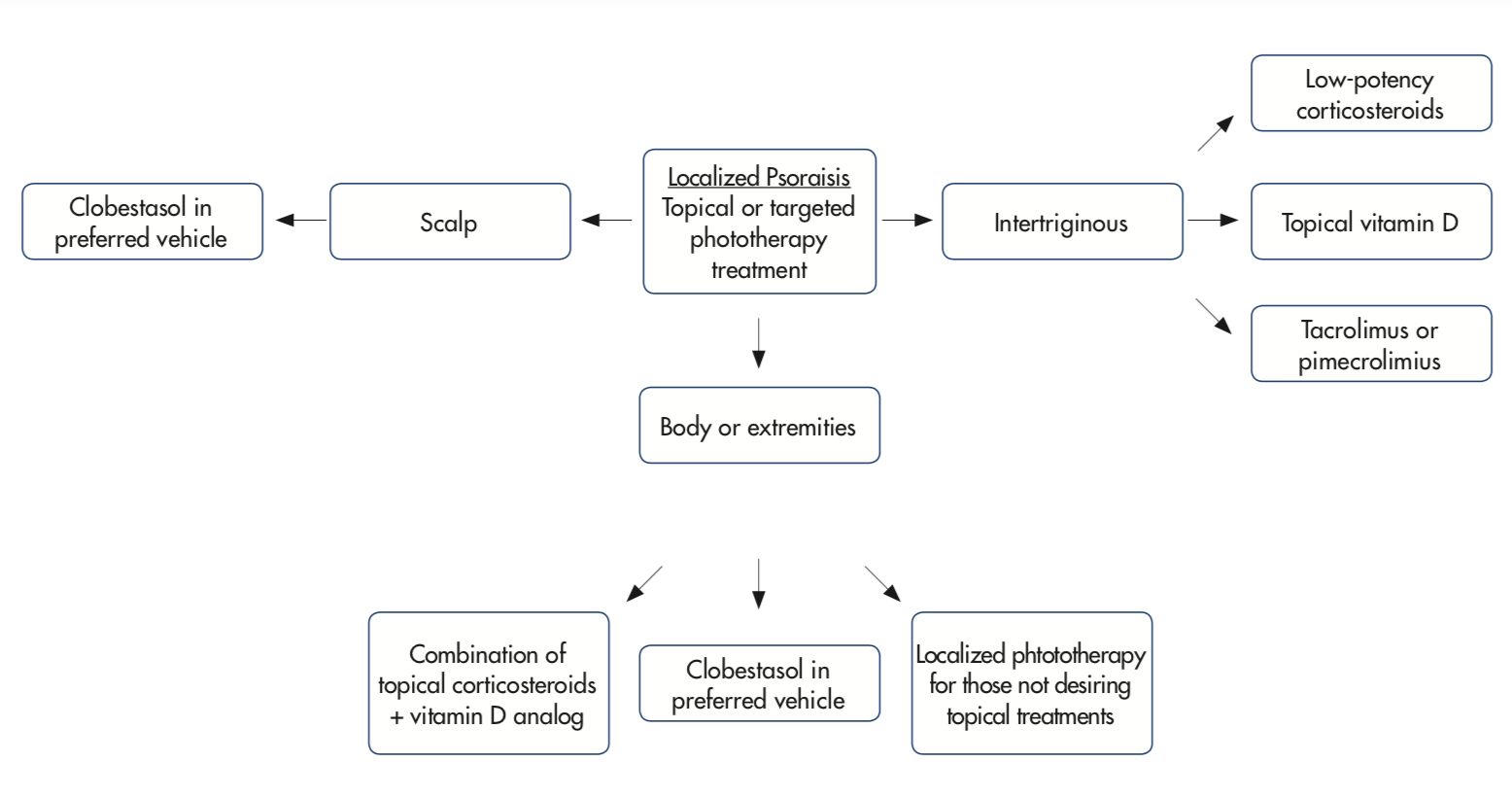
Figure 2. Treatment options for localized psoriasis based on location.
Caution should be taken when prescribing multiple treatments as this makes adherence more difficult. When multiple medications are prescribed, patients are more likely to not fill all the prescriptions; and when multiple prescriptions are filled, patients are less likely to apply all of them.
Involvement of functional or sensitive areas may warrant adjunctive systemic or phototherapy treatment. If response is not robust, consider escalation of medication potency, adjunctive therapy, and the possibility of poor adherence to treatment. For example, higher potency topical corticosteroids or combination with another topical may increase the efficacy of planned treatment. Combination treatment with phototherapy is also common.
Topical corticosteroids of high potency are typically avoided in face and intertriginous areas; however, they are encouraged for scalp or other body areas. If patients have involvement of both types of areas, multiple prescriptions may be given, but in order to promote better adherence, it may be appropriate to choose just 1 treatment strong enough for the most resistant areas with just short-term use on the more sensitive region.
Moderate to Severe Psoriasis
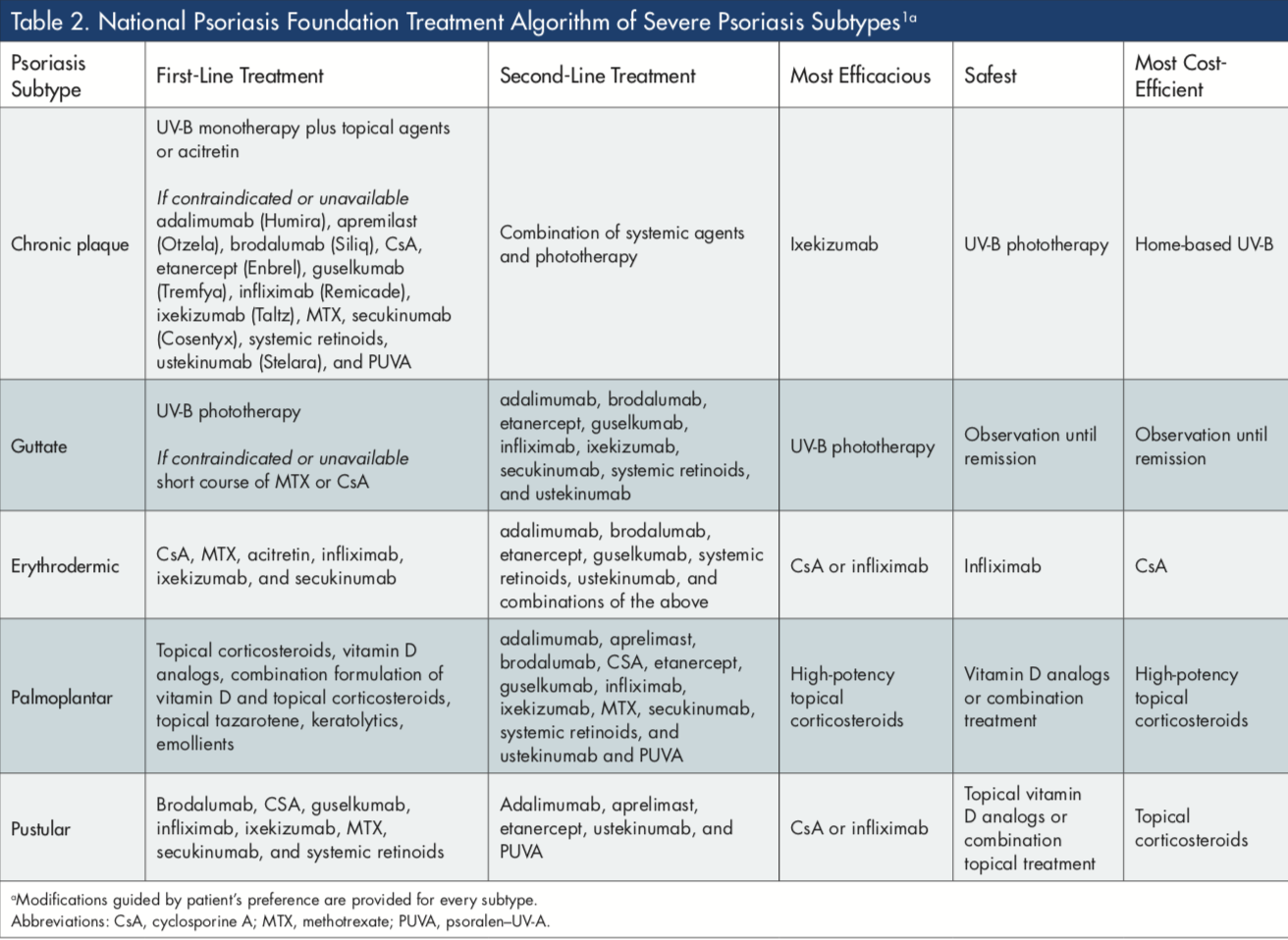
A guideline for generalized chronic plaque psoriasis also must address efficacy, side effect profiles, and cost (Figure 3). The NPF has also published treatment approaches (modified in Table 2).1 Phototherapy is often a good first-line option for extensive psoriasis. If patients cannot access phototherapy in the office, home phototherapy may provide a low cost, accessible UV treatment options.
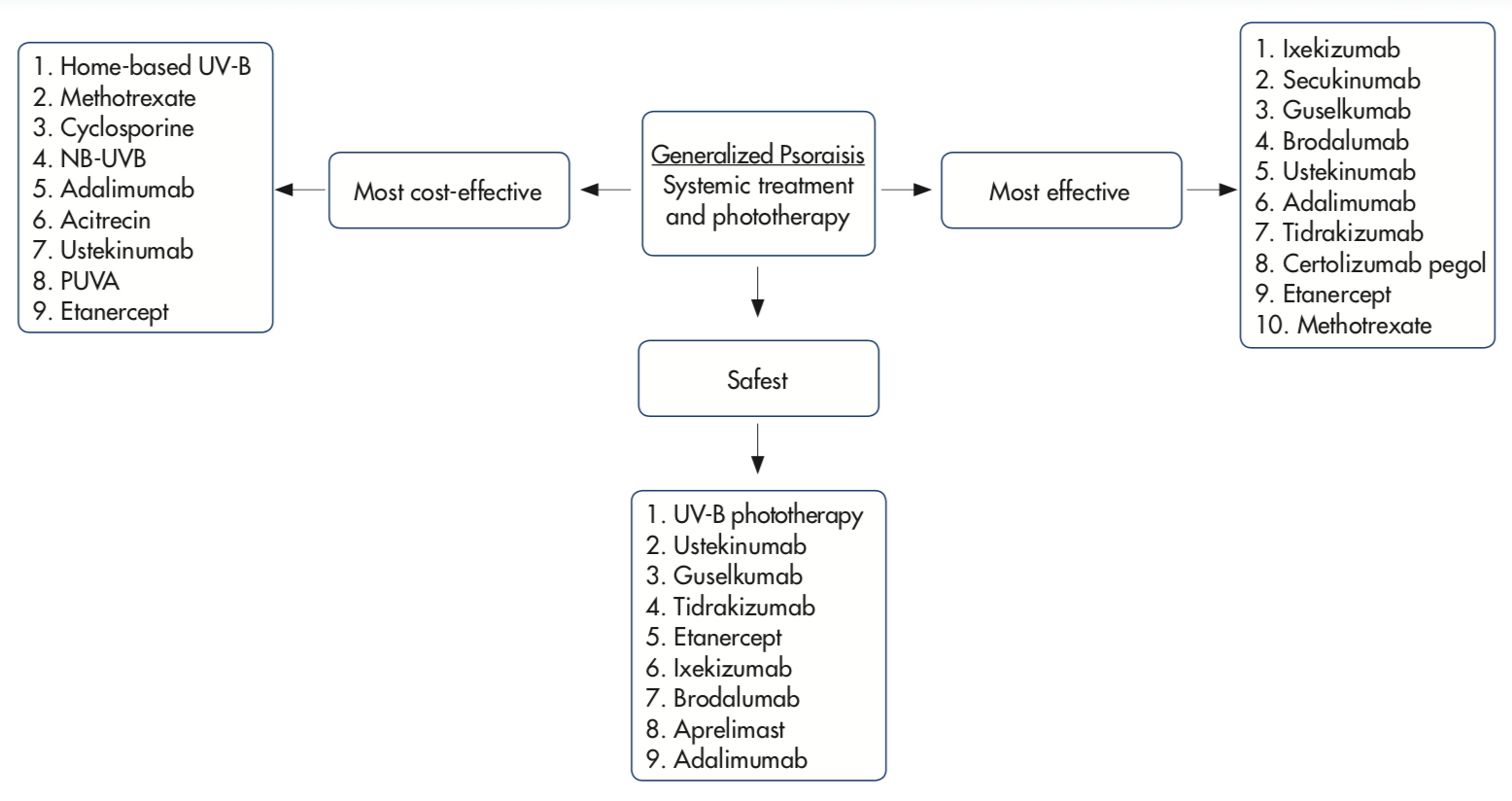
Figure 3. Treatment algorithm for generalized or severe psoriasis based on efficacy, side effect profiles, and cost.
When phototherapy is contraindicated or not effective for generalized chronic plaque psoriasis, systemic treatments can be chosen based on the patient’s preference. IL-17 pathway inhibitors are good options for patients seeking the most effective treatment and ustekinumab (Stelara) for patients looking for something that has a long track record of safety. Many of the treatments are so similar in efficacy and safety (for example, secukinumab [Cosentyx] and ixekizumab [Taltz]) that, unless a patient has a particular preference for the particular dosing regimen, a coin flip may be good as any other reason to choose between them.
Those who failed the second-line biologic agents should be re-counseled regarding modifiable life factors (ie, alcohol, smoking, and obesity) and escalate or optimize adjunctive therapies (switch to subcutaneous methotrexate from oral, initiate topical and phototherapy).2
Psoriatic Arthritis
Because the majority of patients present with cutaneous manifestations of psoriasis 10 years prior to PsA, early screening questions for joint involvement are warranted. If PsA is diagnosed or even suspected, patients should undergo complete joint examination, imaging, and laboratory tests for inflammation markers often necessitating referral to a rheumatologist. In the event when rheumatologists are inaccessible, dermatologists may be required to offer care for the joint involvement.
Involvement of joints does not necessarily affect the treatment choice for skin involvement. The presence of mild PsA may be treated with nonsteroidal anti-inflammatory agents and physical therapy and not require use of a biologic. Moreover, systemic anti-inflammatory medications that improve psoriasis are likely to be effective for joint involvement, too, even if those systemic medications do not have FDA-approved indications for treatment of PsA.
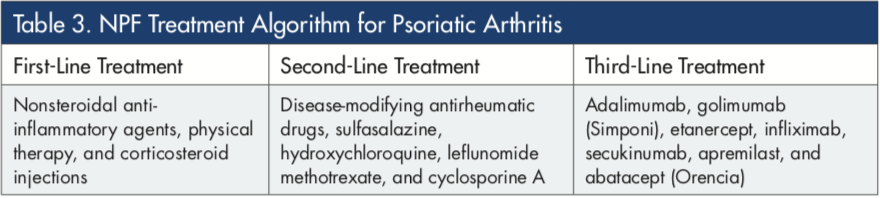
A number of medications may be minimized if patients report improvement of PsA with medications prescribed for psoriasis by dermatologists; this may help patients and physicians to have stable treatment plans. Therapy can be escalated to disease-modifying antirheumatic drugs (DMARDs) and/or biologic treatments if the disease is refractory (Table 3)1. Although the absolute costs of DMARDs are less costly, the efficacy and safety of biologic agents make them cost-effective and possibly superior to DMARDs.3
Mr Tjahjono is a medical student at the Mayo Clinic School of Medicine in Rochester, MN.
Dr Cline is with the Center for Dermatology Research at Wake Forest School of Medicine in Winston-Salem, NC.
Dr Feldman is with the Center for Dermatology Research, Department of Dermatology, and Department of Pathology and Department of Public Health Sciences at Wake Forest School of Medicine, in Winston-Salem, NC.
Disclosure: Mr Tjahjono and Dr Cline report no relevant financial relationships.
Dr. Feldman received research, speaking and/or consulting support from a variety of companies including Galderma, GSK/Stiefel, Almirall, Leo Pharma, Boehringer Ingelheim, Mylan, Celgene, Pfizer, Ortho Dermatology, Abbvie, Samsung, Janssen, Lilly, Menlo, Merck, Novartis, Regeneron, Sanofi, Novan, Qurient, National Biological Corporation, Caremark, Advance Medical, Sun Pharma, Suncare Research, Informa, UpToDate, and National Psoriasis Foundation. He is founder and majority owner of www.DrScore.com and founder and part owner of Causa Research, a company dedicated to enhancing patients’ adherence to treatment.
References
1. Voorhees AV, Feldman S, Lebwohl M, Mandelin A, Ritchlin C. The Psoriasis and Psoriatic Arthritis Pocket Guide: Treatment Algorithms and Management Options. 4th ed. Portland, OR: National Psoriasis Foundation; 2017. https://www.psoriasis.org/sites/default/files/npf_pocketguide_2017.pdf. Accessed June 25, 2018.
2. Smith CH, Jabbar-Lopez ZK, Yiu ZZ, et al. British Association of Dermatologists guidelines for biologic therapy for psoriasis 2017. Br J Dermatol. 2017;177(3):628-636.
3. D’Angiolella LS, Cortesi PA, Lafranconi A, et al. Cost and cost effectiveness of treatments for psoriatic arthritis: A systematic literature review. Pharmacoeconomics. 2018;36(5):567-589.









