 Psoriasis is a common chronic inflammatory disease that often requires long-term treatment. Characterized by cutaneous inflammation and epidermal hyperproliferation, psoriasis can have a profound impact on quality of life. In recent years, an increased understanding of psoriasis pathophysiology has led to the release of new treatment targets, including biologic therapies. The development of biologic agents has changed the treatment paradigm for dermatologists managing patients with moderate-to-severe psoriasis and psoriatic arthritis (PsA). Biologics, which are protein-based drugs made from living cells, have been shown to improve prognosis and control symptoms and also improve quality of life.
Psoriasis is a common chronic inflammatory disease that often requires long-term treatment. Characterized by cutaneous inflammation and epidermal hyperproliferation, psoriasis can have a profound impact on quality of life. In recent years, an increased understanding of psoriasis pathophysiology has led to the release of new treatment targets, including biologic therapies. The development of biologic agents has changed the treatment paradigm for dermatologists managing patients with moderate-to-severe psoriasis and psoriatic arthritis (PsA). Biologics, which are protein-based drugs made from living cells, have been shown to improve prognosis and control symptoms and also improve quality of life.
This article provides a brief overview of psoriasis and reviews the efficacy and tolerability of the biologics approved for psoriasis and PsA. Also discussed is the the burden of disease including cost, the importance of clinician and patient education and new biologics in the pipeline.
Overview of Psoriasis
Psoriasis, a disease of T cell dysregulation, is the most prevalent autoimmune disease in the United States, affecting approximately 3% of the US population. Of the individuals with psoriasis, 1.5 million US adults have moderate-to-severe psoriasis. Current published estimates of the worldwide prevalence of psoriasis range from approximately 1% to 3%.1-3 The disease, which is usually manifested as raised, well-demarcated, erythematous oval plaques with adherent silvery scales that are often painful and pruritic, is associated with comorbidities beyond skin manifestations including a higher prevalence of metabolic syndrome, cardiovascular diseases and other autoimmune diseases.4,5
The disease also significantly impacts a patient’s health-related quality of life, psychological well-being and physical and social aspects of daily living.6 For example, patients often feel stigmatized. A recent National Psoriasis Foundation-funded study of 56 participants without any serious skin problems showed that psoriasis is highly stigmatizing and carries the same level of stigma as herpes. A majority of the stigma surrounding psoriasis came down to participants’ belief that the disease was contagious.7
The causes of psoriasis are not fully understood, but a number of risk factors are recognized, including family history and environmental risk factors.8,9 Psoriasis associated with PsA — an inflammatory seronegative spondyloarthropathy — occurs in approximately 10% to 30% of psoriasis patients. In the majority of cases, joint involvement follows skin involvement, often by 10 years.3
Healthcare expenditures associated with psoriasis are significant. A systematic review of 22 studies on the direct, indirect and comorbidity costs of adult psoriasis in the United States found that the annual US cost of psoriasis is approximately $112 billion (2013 US dollars). The direct costs ranged from $51.7 billion to $63.2 billion, indirect costs ranged from $23.9 billion to $35.4 billion and medical comorbidities were estimated to contribute $36.4 billion.10
Biologics for Psoriasis
Various triggers — both internal and external — can initiate psoriatic lesion formation caused by cross-talk between the skin and the immune system. This, in turn, can culminate in a positive inflammatory feedback loop due to the persistent release of pro-inflammatory cytokines including tumor necrosis factor-alpha (TNF-α), interleukin (IL)-23 and IL-17A. Over the past decade, the role of cytokines in the pathogenesis of psoriasis have been elucidated (Table 1).4,11-15 Different from the traditional systemic drugs that impact the entire immune system, biologics target key selective immune pathways.16
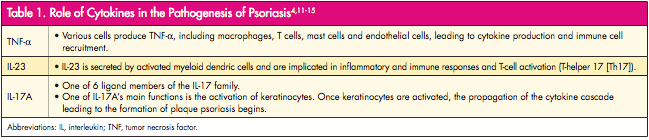
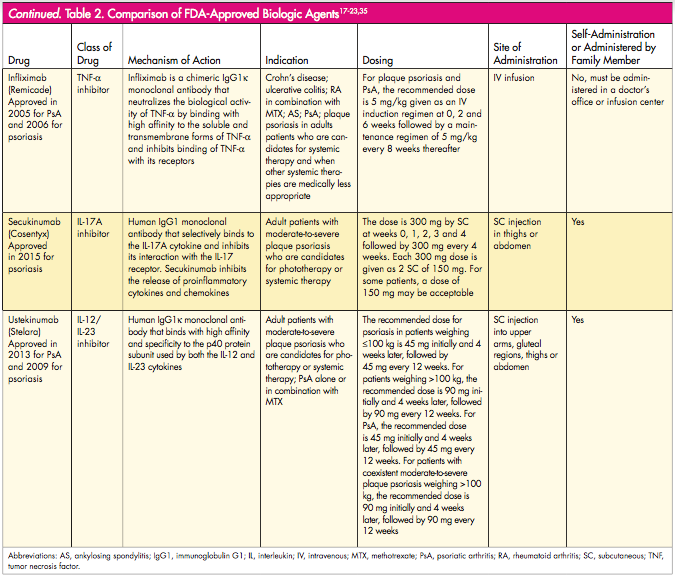
Seven biologics are FDA-approved for psoriasis, PsA or both, and more biologics are in the pipeline. These therapies belong to 1 of 2 categories: TNF-α inhibitors or the IL-12/23 and IL-17A monoclonal antibodies. TNF-α inhibitors approved for psoriasis and PsA include adalimumab (Humira, AbbVie Inc.), etanercept (Enbrel, Amgen Inc.) and infliximab (Remicade, Janssen Biotech Inc.), while the TNF-α inhibitors certolizumab pegol (Cimzia, UCB Inc.) and golimumab (Simponi, Janssen Biotech Inc.) are approved for PsA. The IL 12/23 monoclonal antibody ustekinumab (Stelara; Janssen Biotech Inc.) is approved for psoriasis and PsA, and IL-17A monoclonal antibody secukinumab (Cosentyx, Novartis Pharmaceuticals Corporation) is approved for psoriasis.17-23 Each biologic has a unique mechanism of action, dosing schedule and site and route of administration (Table 2).

Before the the first biologic for psoriasis was FDA approved, dermatologists’ treatment options consisted of topical agents, phototherapy and conventional systemic agents. Systemic psoriasis therapies (eg, methotrexate, cyclosporine and acitretin) were used when psoriasis was too extensive for topical therapy or refractory to topical therapy and phototherapy. However, these medications suppress the entire immune function, requiring routine laboratory monitoring because of the increased hepatic and renal toxicity, hematologic conditions and myelosuppresion. Systemic therapies are also contraindicated in various clinical settings (eg, pregnancy and nursing mothers).9, 24
Efficacy and Tolerability
Efficacy and tolerability are 2 of the main factors that affect the choice of biologic treatment, which are now the mainstay of systemic treatment for psoriasis. These biologic agents have demonstrated high efficacy and a favorable safety profile without evidence of cumulative organ-specific toxicity.25
The following highlights outcomes, including long-term studies, that evaluated the effectiveness and safety of the biologics approved for psoriasis and PsA.
Adalimumab
Menter et al26 reported 5-year data from ESPIRIT — the ongoing, multicenter, postmarketing, 10-year, international, observational registry evaluating the long-term safety and efficacy of adalimumab treatment in routine clinical practice. During the first 5 years of treatment, adalimumab continued to be well-tolerated in the majority of the 6,059 patients treated and no new safety signals were observed. The TNF-α inhibitor also showed increased effectiveness across the first 5 years of ESPIRIT.
Adalimumab for PsA has also been effective as shown in a post hoc analysis from ADEPT (Adalimumab Effectiveness in Psoriatic Arthritis Trial) of 152 placebo-treated and 144 adalimumab-treated patients who had evaluable radiographs at baseline and 24 weeks. At 24 weeks, approximately 5-fold reduced risk of radiographic progression was observed with adalimumab. The difference between mean change in modified total Sharp Score (mTSS) for adalimumab versus placebo was greatest for patients with a C-reactive protein ≥2.0 mg/dL (−0.5 vs 2.6, respectively).27
Certolizumab Pegol
Results from RAPID-PsA have demonstrated the efficacy and safety of certolizumab pegol versus placebo over 24 weeks. In a new study, Mease et al28 assessed this efficacy and safety data at 96 weeks with 400 mg certolizumab pegol and 200 mg certolizumab pegol dosing regimens in PsA patients with and without prior anti-TNF exposure. Outcomes measured included American College of Rheumatology (ACR) response. ACR responses were maintained to week 96: 60% of patients achieved ACR 20 at week 24, and 64% at week 96. Improvements were observed with both dose regimens. At 96 weeks, ACR 20 responses were similar in patients with and without prior anti-TNF exposure (63% and 64%, respectively). Placebo patients switching to certolizumab pegol displayed rapid clinical improvements that were maintained to week 96. The findings also showed the prevention of any clinically relevant change in structural damage, as measured by mTSS, for patients treated with certolizumab pegol. The safety profile over 96 weeks was in line with the 24-week data, with no new safety signals reported with increased exposure.
Etanercept
Papp et al29 performed a post hoc analysis on prospective efficacy and safety data for up to 4 years of etanercept use in psoriasis from a cohort of 506 patients who initiated etanercept therapy in either of 2 Phase III trials. Patients received either etanercept 25 mg twice weekly, 50 mg weekly or 50 mg twice weekly, depending on which trial therapy was started. Study endpoints included change from baseline for the static Physician Global Assessment (sPGA) and Dermatology Life Quality Index (DLQI) scores. In all, 75.9% and 27.8% maintained DLQI response (≥5-point improvement from baseline) and sPGA response (clear or almost clear) at 48 months, respectively.
Golimumab
Kavanaugh et al30 evaluated the the long-term outcomes in PsA patients who achieved or did not achieve minimal disease activity (MDA) through 5 years of golimumab treatment in GO-REVEAL (Golimumab—A Randomized Evaluation of Safety and Efficacy in Subjects with Psoriatic Arthritis Using a Human Anti-TNF Monoclonal Antibody). GO-REVEAL was a Phase III, multicenter, randomized, double-blind, placebo-controlled trial through week 24 followed by an open-label phase lasting up to 5 years that included 405 patients randomized to placebo, golimumab 50 mg or golimumab 100 mg every 4 weeks. Treatment with golimumab yielded significantly higher MDA response rates versus placebo at week 24 (28.1% vs 7.7%, respectively) and week 52 (42.4% vs 30.2%, respectively). MDA was achieved at least once by ∼50% of golimumab-treated patients overall. Among golimumab-treated patients, patient global assessment and radiographic outcomes were also observed when patients achieved persistent MDA.
Article continues on page 2
{{pagebreak}}
Infliximab
A meta-analysis of randomized, controlled studies that assessed the efficacy and safety of infliximab for the treatment of psoriasis and PsA showed that infliximab is significantly associated with symptom relief, skin lesion improvement and increase quality of life. Wang et al31 found statistically significant differences in efficacy for infliximab 3 mg/kg or 5 mg/kg group (odds ratio [OR], 13.55 and 85.45, respectively) compared with the placebo group for psoriasis vulgaris. Significant differences in efficacy between the infliximab 5 mg/kg and placebo groups during treatment for PsA was also observed (OR, 8.36).
Secukinumab
Secukinumab is most first and only FDA approved IL-17A antagonist for psoriasis. Langley et al32 assessed secukimumab in 2 Phase III, double-blind, 52-week trials, ERASURE (Efficacy of Response and Safety of Two Fixed Secukinumab Regimens in Psoriasis) and FIXTURE (Full Year Investigative Examination of Secukinumab vs Etanercept Using Two Dosing Regimens to Determine Efficacy in Psoriasis). The researchers randomly assigned 738 patients (ERASURE) and 1,306 patients (FIXTURE) to secukinumab 300 mg or 150 mg (once weekly for 5 weeks, then every 4 weeks), placebo or in the FIXTURE study only etanercept at 50 mg (twice weekly for 12 weeks, then once weekly). The primary endpoints were Psoriasis Area and Severity Index (PSAI) 75 response and a score of clear or almost clear on the Investigator’s Global Assessment (IGA) at 12 weeks.
Patients who met Psoriasis Area and Severity Index PASI 75 at week 12 was higher with each secukinumab dose versus placebo or etanercept. The rates in ERASURE were 81.6% with 300 mg secukinumab, 71.6% with 150 mg secukinumab and 4.5% with placebo; in the FIXTURE study the rates were 77.1%, 67.0% and 4.9%, respectively, and 44.0% with etanercept. Patients who achieved IGA score of clear or almost clear at 12 weeks was also higher with each secukinumab dose versus placebo and etanercept. In ERASURE, the rates were 65.3% with 300 mg secukinumab, 51.2% with 150 mg secukinumab and 2.4% with placebo; in FIXTURE, the rates were 62.5%, 51.1% and 2.8%, respectively, and 27.2% with etanercept.32
Ustekinumab
Long-term follow-up from PHOENIX 2 (Phase 3, Multicenter, Randomized, Double-blind, Placebo-controlled Trial Evaluating the Efficacy and Safety of CNTO 1275 in the Treatment of Subjects with Moderate to Severe Plaque-type Psoriasis) found that 5 years of continuous ustekinumab treatment was safe and effective.33 Patients were randomized to placebo or ustekinumab 45 mg or 90 mg at weeks 0, 4 then every 12 weeks; patients receiving placebo crossed-over at week 12. Dosing adjustments were permitted at different time points. Efficacy and safety were evaluated through weeks 244 and 264, respectively. In the overall population, the researchers found that 70% of ustekinumab-treated patients completed treatment through week 244, with more patients responding to the 45 mg and 90 mg doses, respectively: PASI 75 responses were 76.5% and 78.6%, respectively, and PASI 90 were 50.0% and 55.5%, respectively. Improved response was generally observed following dosing adjustments.
Ustekinumab 45 mg and 90 mg was also proven effective for long-term therapy in PsA, according to results at week 60 from PSUMMIT 2 (Phase 3 Multicenter, Randomized, Double-blind, Placebo-controlled Trial of Ustekinumab, a Fully Human Aanti-IL-12/23p40 Monoclonal Antibody, Administered Subcutaneously, in Subjects with Active Psoriatic Arthritis), which included patients with and without prior exposure to anti-TNF agents. The primary endpoint was ≥20% improvement in ACR at week 24. More ustekinumab-treated patients (43.8% combined for 45 mg and 90 mg) than placebo-treated patients achieved ACR 20 response week 24. Among patients previously treated with ≥1 TNF inhibitor, sustained ustekinumab efficacy was also observed at week 24 versus placebo in ACR 20 response (35.6% combined for 45 mg and 90 mg vs 14.5%, respectively).34
Adverse Events
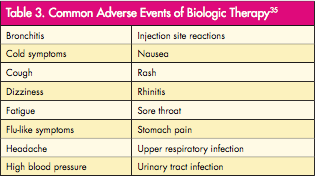
Overall, the most commonly reported adverse events (AEs) in clinical trials of biologics were mild and did not result in discontinuation of therapy (Table 3).35 In a 2-part series published in The Dermatologist36,37 on rare AEs of biologics reported in the literature, rare AEs fell into 6 categories: inflammatory skin disease, atypical infectious events, blood disorders, connective tissue disease, neurologic events and cardiac/metabolic abnormalities. Because there are AEs associated with biologic therapies, clinicians should prescreen patients before initiation and continue monitoring patients during and after treatments.38
A potential disadvantage to biologic therapy is it has to be given either by injection or intravenous infusion. Infusion can last 2 hours per session (Table 2).
Economic Burden of Biologics
Biologics for psoriasis have shown significant reductions in the number of hospital stays, use of other systemic therapies, improved PASI outcomes and increased patient satisfaction. Yet, the annual cost of these drugs is substantial. Cheng et al39 examined the cost of annual treatment paradigms for etanercept, adalimumab and ustekinumab using the average wholesale price. The cost of 1 year of induction and maintenance treatment was highest for ustekinumab ($53,909), followed by etanercept ($46,395) and adalimumab ($39,041). The sales-based cost of drugs was greatest for ustekinumab ($25,012), then adalimumab ($6,786) and etanercept ($6,629).
Cost is also an important factor for patients prescribed biologics. A survey of 106 patients at an academic medical center to discern patient attitudes toward biologics found that patients with lower income levels had increased cutbacks in personal expenses due to copayments. Among respondents, the mean annual out of pocket expense for current biologics was $557.12 per year, with a range of $0 to $7,000.40
To offset cost of therapy, the manufacturers of biologics offer programs to help determine patient eligibility and treatment cost.
Patient Preference and Education
Each individual psoriasis patient has different expectations and goals for biological treatment, which may differ from those of the clinician. Understanding the needs and expectations of patients from treatment should constitute a fundamental part of treatment with biologics.41 To better understand and align patients’ and physicians’ preferences and goals for biological treatment, a working group of psoriasis experts developed a questionnaire that can be given to patients during consultation with their dermatologist. The goal of the questionnaire is that it will offer a more structured approach when choosing a biological therapy that incorporates patients’ treatment preferences.41 When deciding on an appropriate biologic therapy, clinicians need to educate patients on the advantages and disadvantages associated with therapy so they can be involved in the decision-making process. Clinicians should also continue to be educated on the efficacy and tolerability of biologic therapy. Once a patient is started on therapy, clinicians should monitor adherence and gauge satisfaction with therapy.
In a study that assessed patient-reported treatment and dosing frequency choice with biologics, Zhang et al6 found that overall patient satisfaction with biologic treatment of psoriasis is good among patients who have previously tried or are receiving a biologic treatment. The researchers concluded that patients’ choices regarding dosing schedule and treatment satisfaction should be included among all other considerations in determining an appropriate treatment.
A separate study by Kamanger et al40 that assessed patients’ attitudes with biologics found that 62.6% of respondents were “very satisfied” with biologics, and 74.5% learned about biologics from their physician. When asked about concern that biologics medications will cause an AE, 57.5% of patients responded “not worried at all.” The survey also found that compliance rates for biologic therapy was high with 66.6% of respondents reporting “never” or “rarely” missing a dose.
Pipeline of Biologic Drugs
Many novel treatments in the pipeline promise exciting new therapeutic avenues for psoriasis and PsA that target various cytokines and regulatory molecules involved in the pathogenesis of psoriasis including inhibition of the IL-12/IL-23 pathway; inhibition of IL-17 pathway; inhibition of T cell activation in antigen-presenting cells; activation of regulatory T cells; inhibition of toll-like receptors (TLRs) 7, 8 and 9 and inhibition of granulocyte-macrophage colony-stimulating factor (GM-CSF).42
IL-17 receptor blockers have recently received FDA approval. Secukimumab was the first drug approved in this class in January 2015 for psoriasis. Brodalumab and ixekizumab are 2 other agents in this class that show promise. In a Phase III study, 661 patients received brodalumab 210 mg or 140 mg or placebo. At week 12, PASI 75 was observed in 83% of the 210 mg group versus 60% of the 140 mg group; PASI 100 was observed in 42% of the 210 mg group versus 23% of the 140 mg group. Results of a Phase II trial of ixekizumab (N=142) found that PSAI 75 were significantly improved versus placebo (150 mg, 82.1%; 75 mg, 82.8% and 25 mg, 76.7% vs 7.7% with placebo).42 Amgen Inc. had initially partnered with AstraZeneca in developing brodalumab, but announced their withdrawal from the project earlier this year following the observation of suicidal behavior and ideation observed in some subjects taking the medication. The impact of these findings on further medication development is not yet clear.
New drugs that specifically target IL-23 pathway such as guselkumab and tildrakizumab are in Phase II and III studies for psoriasis.42 Results from a Phase II study of BI 655066 — another agent that targets the IL-23 pathway — were recently presented at the 24th European Academy of Dermatology and Venereology. The head-to-head study evaluated the efficacy and safety of BI 655066 versus ustekinumab in 166 patients with moderate-to-severe-plaque psoriasis and found that 39% more patients maintained clear or almost clear skin (PASI 90) on BI 655066 after 9 months compared with ustekinumab. Nearly triple the percentage of patients maintained completely clear skin (PASI 100) on BI 655066 after 9 months versus ustekinumab (69% vs 30%, respectively). Additionally, clear skin or almost clear skin (PASI 90) was achieved faster and maintained for more than 2 months longer with BI 655066 compared with ustekinumab.43
Other therapies in development include abatacept, a fusion protein designed to inhibit T cell activation by binding receptors for CD80 and CD86 in antigen-presenting cells, that is in Phase III studies for psoriasis and PsA. Tregalizumab, a monoclonal antibody that activates regulatory T cells, is in Phase II studies for psoriasis. IMO-8400 is unique in that it treats psoriasis by targeting TLRs 7, 8 and 9; Phase II studies are underway. Namilumab, a GM-CSF inhibitor, is in Phase II studies for psoriasis.42
Conclusion
The proven efficacy and safety of biologics has added to the armamentarium of treatment options for patients suffering from psoriasis and PsA. As more biologic therapies enter the marketplace, the opportunity for improved prognosis and symptom control will benefit patients and improve their quality of life. Efficacy and safety, patient comorbidities, patient preference and quality life need to be taken into consideration when dermatologists are prescribing treatment. Continuing education on current and future medications is also needed so dermatologists and other clinicians properly manage patients living with psoriasis.
References
1. National Psoriasis Foundation Web site. Psoriasis statistics. https://www.pso riasis.org/research/science-of-psoriasis/statistics. Accessed November 17, 2015.
2. National Psoriasis Foundation. The Psoriasis and Psoriatic Arthritis Pocket Guide: Treatment Options and Patient Management. 3rd ed. Portland, OR; 2009.
3. Van de Kerkhof PC, Reich K, Kavanaugh A, et al. J Eur Acad Dermatol Venereol. 2015;29(10):2002-2010.
4. Nestle FO, Kaplan DH, Barker J. Psoriasis. N Engl J Med. 2009;36(15):496-509.
5. Feldman SR, Zhao Y, Shi L, Tran ME. Economic and comorbidity burden among patients with moderate-to-severe psoriasis. J Mang Care Spec Pharm. 2015;21(10):874-888.
6. Zhang M, Brenneman SK, Carter CT, et al. Patient-reported treatment satisfaction and choice of dosing frequency with biologic treatment
for moderate to severe plaque psoriasis. Patient Pref Adherence. 2015;8:777-784.
7. Donigan JM, Pascoe VL, Kimball AB. Psoriasis and herpes simplex virus are highly stigmatizing compared with other common dermatologic conditions: A survey-based study. J Am Acad Dermatol. 2015;73(3):525-526.
8. Parisi R, Symmons DR, Griffiths CE, Ashcroft DM. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol. 2013;133(2):377-385.
9. Menter A, Gottlieb A, Feldman SR, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 1. Overview of psoriasis and guidelines of care for the treatment of psoriasis with biologics. J Am Acad Dermatol. 2008;58(5):826-850.
10. Brezinski EA, Dhillon JS, Armstrong AW. Economic burden of psoriasis in the United States: A systematic review. JAMA Dermatol. 2015;151(6):651-658.
11. Gaffen SL. Structure and signaling in the IL-17 receptor family. Nat Rev Immunol. 2009;9(8):556-567.
12. Lin AM, Rubin CJ, Khandpur R, et al. Mast cells and neutrophils release IL-17 through extracellular trap formation in psoriasis. J Immunol. 2011;187(1):490-500.
13. Tracey D, Klareskog L, Sasso EH, Salfeld JG, Tak PP. Tumor necrosis factor antagonist mechanisms of action: a comprehensive review. Pharmacol Ther. 2008;117(2):244-279.
14. Lee E, Trepicchio WL, Oestreicher JL, et al. Increased expression of interleukin 23 p19 and p40 in lesional skin of patients with psoriasis vulgaris. J Exp Med. 2004;199(1):125-130.
15. Awasthi A, Kuchroo VK. Th17 cells: from precursors to players in inflammation and infection. Int Immunol. 2009;21(5):489-498.
16. National Psoriasis Foundation. Moderate to Severe Psoriasis: Biologic Drugs. https://www.psoriasis.org/about-psoriasis/treatments/biologics. Accessed November 16, 2015.
17. Humira [prescribing information]. North Chicago, IL: AbbVie Inc; 2015.
18. Cimzia [prescribing information]. Smyrna, GA: UCB Inc; 2013.
19. Enbrel [prescribing information]. Thousand Oaks, CA: Amgen Inc; 2015.
20. Simponi [prescribing information]. Horsham, PA: Janssen Biotech Inc; 2013.
21. Remicade [prescribing information]. Horsham, PA: Janssen Biotech Inc; 2015.
22. Cosentyx [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2015.
23. Stelara. [prescribing information]. Horsham, PA: Janssen Biotech Inc; 2014.
24. Menter A, Korman NJ, Elmets CA. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 4. Guidelines of care for the management and treatment of psoriasis with traditional systemic agents. J Am Acad Dermatol. 2009;61(3):451-485.
25. Mansouri Y, Goldenberg G. Biologic safety in psoriasis: review of long-term safety data. J Clin Aesthet Dermatol. 2015;8(2):30-42.
26. Menter A, Thaçi D, Papp KA, et al. Five-year analysis from the ESPRIT 10-year postmarketing surveillance registry of adalimumab treatment for moderate to severe psoriasis. J Am Acad Dermatol. 2015;73(3):410-419.
27. Gladman DD, Mease PJ, Choy EH, Ritchlin CT, Perodok RJ, Sasso EH. Risk factors for radiographic progression in psoriatic arthritis: subanalysis of the randomized controlled trial ADEPT. Arthritis Res Ther. 2010;12(3):R113.
28. Mease P, Deodhar A, Fleischmann R, et al. Effect of certolizumab pegol over 96 weeks in patients with psoriatic arthritis with and without prior antitumour necrosis factor exposure. RMD Open. 2015;1(1):e000119.
29. Papp KA, Poulin Y, Bissonnette R, et al. Assessment of the long-term safety and effectiveness of etanercept for the treatment of psoriasis in an adult population. J Am Acad Dermatol. 2012;66(2):e33-45.
30. Kavanaugh A, van der Heijde D, Beutler A, et al. Patients with psoriatic arthritis who achieve minimal disease activity in response to golimumab therapy demonstrate less radiographic progression: Results through 5 years of the randomized, placebo-controlled, GO-REVEAL study. Arthritis Care Res. Published online ahead of print March 16, 2015.
31. Wang J, Zhan Q, Zhang L. A systematic review on the efficacy and safety of infliximab in patients with psoriasis. Hum Vaccin Immunother. Published online ahead of print November 3, 2015.
32. Langley RG, Elewsku BE, Lebwohl M, et al. Secukinumab in plaque psoriasis--results of two phase 3 trials. N Engl J Med. 2014;371(4):326-338.
33. Langley RG, Lebwohol M, Krueger GG, et al. Long-term efficacy and safety of ustekinumab, with and without dosing adjustment, in patients with moderate-to-severe psoriasis: results from the PHOENIX 2 study through 5 years of follow-up. Br J Dermatol. 2015;172(5):1371-1383.
34. Ritchlin C, Rahman P, Kavanaugh A, et al. Efficacy and safety of the anti-IL-12/23 p40 monoclonal antibody, ustekinumab, in patients with active psoriatic arthritis despite conventional non-biological and biological anti-tumour necrosis factor therapy: 6-month and 1-year results of the phase 3, multicentre, double-blind, placebo-controlled, randomised PSUMMIT 2 trial. Ann Rheum Dis. 2014;73(6):990-999.
35. National Psoriasis Foundations. Biologic Drugs: Fact Sheets. https://www.psoriasis.org/about-psoriasis/treatments/biologics/resources. Accessed November 16, 2015.
36. Townsend M, Stober BE. Rare side effects of biologics: part 1. The Dermatologist. 2013;21(11):28-32.
37. Townsend M, Stober BE. Rare side effects of biologics: part 2. The Dermatologist. 2013;21(12):30-34.
38. Levy LL, Solomon SM, Emer JJ. Biologics in the treatment of psoriasis and emerging new therapies in the pipeline. Psoriasis: Targets and Therapy. 2012;2:29-43.
39. Cheng J, Feldman SR. The cost of biologics for psoriasis is increasing. Drug Context. 2014;3:212266.
40. Kamangar F, Isip L, Bhutani T, et al. How psoriasis patients perceive, obtain, and use biologic agents: Survey from an academic medical center. J Dermatolog Treat. 2013;24(1):13-24.
41. Strohal R, Prinz JC, Girolomoni G, Nast A. A patient-centered approach to biological treatment decision making for psoriasis: an expert consensus. J Eur Acad Dermatol Venereol. Published online ahead of print September 14, 2015.
42. Feely MA, Smith BL, Weinberg JM. Novel psoriasis therapies and patient outcomes, part 2: biologic treatments. Cutis. 2015;95(5):282-290.
43. Boehringer Ingelheim’s investigational biologic cleared skin better, faster and for longer than ustekinumab in phase II psoriasis study [news release]. Ridgefield, CT: Boehringer Ingelheim GmbH; October 8, 2015. https://www.boehringer-ingelheim.com/news/news_releases/press_releases/2015/08_oktober_2015_immunology.html. Accessed November 19, 2015.
 Psoriasis is a common chronic inflammatory disease that often requires long-term treatment. Characterized by cutaneous inflammation and epidermal hyperproliferation, psoriasis can have a profound impact on quality of life. In recent years, an increased understanding of psoriasis pathophysiology has led to the release of new treatment targets, including biologic therapies. The development of biologic agents has changed the treatment paradigm for dermatologists managing patients with moderate-to-severe psoriasis and psoriatic arthritis (PsA). Biologics, which are protein-based drugs made from living cells, have been shown to improve prognosis and control symptoms and also improve quality of life.
Psoriasis is a common chronic inflammatory disease that often requires long-term treatment. Characterized by cutaneous inflammation and epidermal hyperproliferation, psoriasis can have a profound impact on quality of life. In recent years, an increased understanding of psoriasis pathophysiology has led to the release of new treatment targets, including biologic therapies. The development of biologic agents has changed the treatment paradigm for dermatologists managing patients with moderate-to-severe psoriasis and psoriatic arthritis (PsA). Biologics, which are protein-based drugs made from living cells, have been shown to improve prognosis and control symptoms and also improve quality of life.
This article provides a brief overview of psoriasis and reviews the efficacy and tolerability of the biologics approved for psoriasis and PsA. Also discussed is the the burden of disease including cost, the importance of clinician and patient education and new biologics in the pipeline.
Overview of Psoriasis
Psoriasis, a disease of T cell dysregulation, is the most prevalent autoimmune disease in the United States, affecting approximately 3% of the US population. Of the individuals with psoriasis, 1.5 million US adults have moderate-to-severe psoriasis. Current published estimates of the worldwide prevalence of psoriasis range from approximately 1% to 3%.1-3 The disease, which is usually manifested as raised, well-demarcated, erythematous oval plaques with adherent silvery scales that are often painful and pruritic, is associated with comorbidities beyond skin manifestations including a higher prevalence of metabolic syndrome, cardiovascular diseases and other autoimmune diseases.4,5
The disease also significantly impacts a patient’s health-related quality of life, psychological well-being and physical and social aspects of daily living.6 For example, patients often feel stigmatized. A recent National Psoriasis Foundation-funded study of 56 participants without any serious skin problems showed that psoriasis is highly stigmatizing and carries the same level of stigma as herpes. A majority of the stigma surrounding psoriasis came down to participants’ belief that the disease was contagious.7
The causes of psoriasis are not fully understood, but a number of risk factors are recognized, including family history and environmental risk factors.8,9 Psoriasis associated with PsA — an inflammatory seronegative spondyloarthropathy — occurs in approximately 10% to 30% of psoriasis patients. In the majority of cases, joint involvement follows skin involvement, often by 10 years.3
Healthcare expenditures associated with psoriasis are significant. A systematic review of 22 studies on the direct, indirect and comorbidity costs of adult psoriasis in the United States found that the annual US cost of psoriasis is approximately $112 billion (2013 US dollars). The direct costs ranged from $51.7 billion to $63.2 billion, indirect costs ranged from $23.9 billion to $35.4 billion and medical comorbidities were estimated to contribute $36.4 billion.10
Biologics for Psoriasis
Various triggers — both internal and external — can initiate psoriatic lesion formation caused by cross-talk between the skin and the immune system. This, in turn, can culminate in a positive inflammatory feedback loop due to the persistent release of pro-inflammatory cytokines including tumor necrosis factor-alpha (TNF-α), interleukin (IL)-23 and IL-17A. Over the past decade, the role of cytokines in the pathogenesis of psoriasis have been elucidated (Table 1).4,11-15 Different from the traditional systemic drugs that impact the entire immune system, biologics target key selective immune pathways.16

Seven biologics are FDA-approved for psoriasis, PsA or both, and more biologics are in the pipeline. These therapies belong to 1 of 2 categories: TNF-α inhibitors or the IL-12/23 and IL-17A monoclonal antibodies. TNF-α inhibitors approved for psoriasis and PsA include adalimumab (Humira, AbbVie Inc.), etanercept (Enbrel, Amgen Inc.) and infliximab (Remicade, Janssen Biotech Inc.), while the TNF-α inhibitors certolizumab pegol (Cimzia, UCB Inc.) and golimumab (Simponi, Janssen Biotech Inc.) are approved for PsA. The IL 12/23 monoclonal antibody ustekinumab (Stelara; Janssen Biotech Inc.) is approved for psoriasis and PsA, and IL-17A monoclonal antibody secukinumab (Cosentyx, Novartis Pharmaceuticals Corporation) is approved for psoriasis.17-23 Each biologic has a unique mechanism of action, dosing schedule and site and route of administration (Table 2).


Before the the first biologic for psoriasis was FDA approved, dermatologists’ treatment options consisted of topical agents, phototherapy and conventional systemic agents. Systemic psoriasis therapies (eg, methotrexate, cyclosporine and acitretin) were used when psoriasis was too extensive for topical therapy or refractory to topical therapy and phototherapy. However, these medications suppress the entire immune function, requiring routine laboratory monitoring because of the increased hepatic and renal toxicity, hematologic conditions and myelosuppresion. Systemic therapies are also contraindicated in various clinical settings (eg, pregnancy and nursing mothers).9, 24
Efficacy and Tolerability
Efficacy and tolerability are 2 of the main factors that affect the choice of biologic treatment, which are now the mainstay of systemic treatment for psoriasis. These biologic agents have demonstrated high efficacy and a favorable safety profile without evidence of cumulative organ-specific toxicity.25
The following highlights outcomes, including long-term studies, that evaluated the effectiveness and safety of the biologics approved for psoriasis and PsA.
Adalimumab
Menter et al26 reported 5-year data from ESPIRIT — the ongoing, multicenter, postmarketing, 10-year, international, observational registry evaluating the long-term safety and efficacy of adalimumab treatment in routine clinical practice. During the first 5 years of treatment, adalimumab continued to be well-tolerated in the majority of the 6,059 patients treated and no new safety signals were observed. The TNF-α inhibitor also showed increased effectiveness across the first 5 years of ESPIRIT.
Adalimumab for PsA has also been effective as shown in a post hoc analysis from ADEPT (Adalimumab Effectiveness in Psoriatic Arthritis Trial) of 152 placebo-treated and 144 adalimumab-treated patients who had evaluable radiographs at baseline and 24 weeks. At 24 weeks, approximately 5-fold reduced risk of radiographic progression was observed with adalimumab. The difference between mean change in modified total Sharp Score (mTSS) for adalimumab versus placebo was greatest for patients with a C-reactive protein ≥2.0 mg/dL (−0.5 vs 2.6, respectively).27
Certolizumab Pegol
Results from RAPID-PsA have demonstrated the efficacy and safety of certolizumab pegol versus placebo over 24 weeks. In a new study, Mease et al28 assessed this efficacy and safety data at 96 weeks with 400 mg certolizumab pegol and 200 mg certolizumab pegol dosing regimens in PsA patients with and without prior anti-TNF exposure. Outcomes measured included American College of Rheumatology (ACR) response. ACR responses were maintained to week 96: 60% of patients achieved ACR 20 at week 24, and 64% at week 96. Improvements were observed with both dose regimens. At 96 weeks, ACR 20 responses were similar in patients with and without prior anti-TNF exposure (63% and 64%, respectively). Placebo patients switching to certolizumab pegol displayed rapid clinical improvements that were maintained to week 96. The findings also showed the prevention of any clinically relevant change in structural damage, as measured by mTSS, for patients treated with certolizumab pegol. The safety profile over 96 weeks was in line with the 24-week data, with no new safety signals reported with increased exposure.
Etanercept
Papp et al29 performed a post hoc analysis on prospective efficacy and safety data for up to 4 years of etanercept use in psoriasis from a cohort of 506 patients who initiated etanercept therapy in either of 2 Phase III trials. Patients received either etanercept 25 mg twice weekly, 50 mg weekly or 50 mg twice weekly, depending on which trial therapy was started. Study endpoints included change from baseline for the static Physician Global Assessment (sPGA) and Dermatology Life Quality Index (DLQI) scores. In all, 75.9% and 27.8% maintained DLQI response (≥5-point improvement from baseline) and sPGA response (clear or almost clear) at 48 months, respectively.
Golimumab
Kavanaugh et al30 evaluated the the long-term outcomes in PsA patients who achieved or did not achieve minimal disease activity (MDA) through 5 years of golimumab treatment in GO-REVEAL (Golimumab—A Randomized Evaluation of Safety and Efficacy in Subjects with Psoriatic Arthritis Using a Human Anti-TNF Monoclonal Antibody). GO-REVEAL was a Phase III, multicenter, randomized, double-blind, placebo-controlled trial through week 24 followed by an open-label phase lasting up to 5 years that included 405 patients randomized to placebo, golimumab 50 mg or golimumab 100 mg every 4 weeks. Treatment with golimumab yielded significantly higher MDA response rates versus placebo at week 24 (28.1% vs 7.7%, respectively) and week 52 (42.4% vs 30.2%, respectively). MDA was achieved at least once by ∼50% of golimumab-treated patients overall. Among golimumab-treated patients, patient global assessment and radiographic outcomes were also observed when patients achieved persistent MDA.
Article continues on page 2
{{pagebreak}}
Infliximab
A meta-analysis of randomized, controlled studies that assessed the efficacy and safety of infliximab for the treatment of psoriasis and PsA showed that infliximab is significantly associated with symptom relief, skin lesion improvement and increase quality of life. Wang et al31 found statistically significant differences in efficacy for infliximab 3 mg/kg or 5 mg/kg group (odds ratio [OR], 13.55 and 85.45, respectively) compared with the placebo group for psoriasis vulgaris. Significant differences in efficacy between the infliximab 5 mg/kg and placebo groups during treatment for PsA was also observed (OR, 8.36).
Secukinumab
Secukinumab is most first and only FDA approved IL-17A antagonist for psoriasis. Langley et al32 assessed secukimumab in 2 Phase III, double-blind, 52-week trials, ERASURE (Efficacy of Response and Safety of Two Fixed Secukinumab Regimens in Psoriasis) and FIXTURE (Full Year Investigative Examination of Secukinumab vs Etanercept Using Two Dosing Regimens to Determine Efficacy in Psoriasis). The researchers randomly assigned 738 patients (ERASURE) and 1,306 patients (FIXTURE) to secukinumab 300 mg or 150 mg (once weekly for 5 weeks, then every 4 weeks), placebo or in the FIXTURE study only etanercept at 50 mg (twice weekly for 12 weeks, then once weekly). The primary endpoints were Psoriasis Area and Severity Index (PSAI) 75 response and a score of clear or almost clear on the Investigator’s Global Assessment (IGA) at 12 weeks.
Patients who met Psoriasis Area and Severity Index PASI 75 at week 12 was higher with each secukinumab dose versus placebo or etanercept. The rates in ERASURE were 81.6% with 300 mg secukinumab, 71.6% with 150 mg secukinumab and 4.5% with placebo; in the FIXTURE study the rates were 77.1%, 67.0% and 4.9%, respectively, and 44.0% with etanercept. Patients who achieved IGA score of clear or almost clear at 12 weeks was also higher with each secukinumab dose versus placebo and etanercept. In ERASURE, the rates were 65.3% with 300 mg secukinumab, 51.2% with 150 mg secukinumab and 2.4% with placebo; in FIXTURE, the rates were 62.5%, 51.1% and 2.8%, respectively, and 27.2% with etanercept.32
Ustekinumab
Long-term follow-up from PHOENIX 2 (Phase 3, Multicenter, Randomized, Double-blind, Placebo-controlled Trial Evaluating the Efficacy and Safety of CNTO 1275 in the Treatment of Subjects with Moderate to Severe Plaque-type Psoriasis) found that 5 years of continuous ustekinumab treatment was safe and effective.33 Patients were randomized to placebo or ustekinumab 45 mg or 90 mg at weeks 0, 4 then every 12 weeks; patients receiving placebo crossed-over at week 12. Dosing adjustments were permitted at different time points. Efficacy and safety were evaluated through weeks 244 and 264, respectively. In the overall population, the researchers found that 70% of ustekinumab-treated patients completed treatment through week 244, with more patients responding to the 45 mg and 90 mg doses, respectively: PASI 75 responses were 76.5% and 78.6%, respectively, and PASI 90 were 50.0% and 55.5%, respectively. Improved response was generally observed following dosing adjustments.
Ustekinumab 45 mg and 90 mg was also proven effective for long-term therapy in PsA, according to results at week 60 from PSUMMIT 2 (Phase 3 Multicenter, Randomized, Double-blind, Placebo-controlled Trial of Ustekinumab, a Fully Human Aanti-IL-12/23p40 Monoclonal Antibody, Administered Subcutaneously, in Subjects with Active Psoriatic Arthritis), which included patients with and without prior exposure to anti-TNF agents. The primary endpoint was ≥20% improvement in ACR at week 24. More ustekinumab-treated patients (43.8% combined for 45 mg and 90 mg) than placebo-treated patients achieved ACR 20 response week 24. Among patients previously treated with ≥1 TNF inhibitor, sustained ustekinumab efficacy was also observed at week 24 versus placebo in ACR 20 response (35.6% combined for 45 mg and 90 mg vs 14.5%, respectively).34
Adverse Events
Overall, the most commonly reported adverse events (AEs) in clinical trials of biologics were mild and did not result in discontinuation of therapy (Table 3).35 In a 2-part series published in The Dermatologist36,37 on rare AEs of biologics reported in the literature, rare AEs fell into 6 categories: inflammatory skin disease, atypical infectious events, blood disorders, connective tissue disease, neurologic events and cardiac/metabolic abnormalities. Because there are AEs associated with biologic therapies, clinicians should prescreen patients before initiation and continue monitoring patients during and after treatments.38

A potential disadvantage to biologic therapy is it has to be given either by injection or intravenous infusion. Infusion can last 2 hours per session (Table 2).
Economic Burden of Biologics
Biologics for psoriasis have shown significant reductions in the number of hospital stays, use of other systemic therapies, improved PASI outcomes and increased patient satisfaction. Yet, the annual cost of these drugs is substantial. Cheng et al39 examined the cost of annual treatment paradigms for etanercept, adalimumab and ustekinumab using the average wholesale price. The cost of 1 year of induction and maintenance treatment was highest for ustekinumab ($53,909), followed by etanercept ($46,395) and adalimumab ($39,041). The sales-based cost of drugs was greatest for ustekinumab ($25,012), then adalimumab ($6,786) and etanercept ($6,629).
Cost is also an important factor for patients prescribed biologics. A survey of 106 patients at an academic medical center to discern patient attitudes toward biologics found that patients with lower income levels had increased cutbacks in personal expenses due to copayments. Among respondents, the mean annual out of pocket expense for current biologics was $557.12 per year, with a range of $0 to $7,000.40
To offset cost of therapy, the manufacturers of biologics offer programs to help determine patient eligibility and treatment cost.
Patient Preference and Education
Each individual psoriasis patient has different expectations and goals for biological treatment, which may differ from those of the clinician. Understanding the needs and expectations of patients from treatment should constitute a fundamental part of treatment with biologics.41 To better understand and align patients’ and physicians’ preferences and goals for biological treatment, a working group of psoriasis experts developed a questionnaire that can be given to patients during consultation with their dermatologist. The goal of the questionnaire is that it will offer a more structured approach when choosing a biological therapy that incorporates patients’ treatment preferences.41 When deciding on an appropriate biologic therapy, clinicians need to educate patients on the advantages and disadvantages associated with therapy so they can be involved in the decision-making process. Clinicians should also continue to be educated on the efficacy and tolerability of biologic therapy. Once a patient is started on therapy, clinicians should monitor adherence and gauge satisfaction with therapy.
In a study that assessed patient-reported treatment and dosing frequency choice with biologics, Zhang et al6 found that overall patient satisfaction with biologic treatment of psoriasis is good among patients who have previously tried or are receiving a biologic treatment. The researchers concluded that patients’ choices regarding dosing schedule and treatment satisfaction should be included among all other considerations in determining an appropriate treatment.
A separate study by Kamanger et al40 that assessed patients’ attitudes with biologics found that 62.6% of respondents were “very satisfied” with biologics, and 74.5% learned about biologics from their physician. When asked about concern that biologics medications will cause an AE, 57.5% of patients responded “not worried at all.” The survey also found that compliance rates for biologic therapy was high with 66.6% of respondents reporting “never” or “rarely” missing a dose.
Pipeline of Biologic Drugs
Many novel treatments in the pipeline promise exciting new therapeutic avenues for psoriasis and PsA that target various cytokines and regulatory molecules involved in the pathogenesis of psoriasis including inhibition of the IL-12/IL-23 pathway; inhibition of IL-17 pathway; inhibition of T cell activation in antigen-presenting cells; activation of regulatory T cells; inhibition of toll-like receptors (TLRs) 7, 8 and 9 and inhibition of granulocyte-macrophage colony-stimulating factor (GM-CSF).42
IL-17 receptor blockers have recently received FDA approval. Secukimumab was the first drug approved in this class in January 2015 for psoriasis. Brodalumab and ixekizumab are 2 other agents in this class that show promise. In a Phase III study, 661 patients received brodalumab 210 mg or 140 mg or placebo. At week 12, PASI 75 was observed in 83% of the 210 mg group versus 60% of the 140 mg group; PASI 100 was observed in 42% of the 210 mg group versus 23% of the 140 mg group. Results of a Phase II trial of ixekizumab (N=142) found that PSAI 75 were significantly improved versus placebo (150 mg, 82.1%; 75 mg, 82.8% and 25 mg, 76.7% vs 7.7% with placebo).42 Amgen Inc. had initially partnered with AstraZeneca in developing brodalumab, but announced their withdrawal from the project earlier this year following the observation of suicidal behavior and ideation observed in some subjects taking the medication. The impact of these findings on further medication development is not yet clear.
New drugs that specifically target IL-23 pathway such as guselkumab and tildrakizumab are in Phase II and III studies for psoriasis.42 Results from a Phase II study of BI 655066 — another agent that targets the IL-23 pathway — were recently presented at the 24th European Academy of Dermatology and Venereology. The head-to-head study evaluated the efficacy and safety of BI 655066 versus ustekinumab in 166 patients with moderate-to-severe-plaque psoriasis and found that 39% more patients maintained clear or almost clear skin (PASI 90) on BI 655066 after 9 months compared with ustekinumab. Nearly triple the percentage of patients maintained completely clear skin (PASI 100) on BI 655066 after 9 months versus ustekinumab (69% vs 30%, respectively). Additionally, clear skin or almost clear skin (PASI 90) was achieved faster and maintained for more than 2 months longer with BI 655066 compared with ustekinumab.43
Other therapies in development include abatacept, a fusion protein designed to inhibit T cell activation by binding receptors for CD80 and CD86 in antigen-presenting cells, that is in Phase III studies for psoriasis and PsA. Tregalizumab, a monoclonal antibody that activates regulatory T cells, is in Phase II studies for psoriasis. IMO-8400 is unique in that it treats psoriasis by targeting TLRs 7, 8 and 9; Phase II studies are underway. Namilumab, a GM-CSF inhibitor, is in Phase II studies for psoriasis.42
Conclusion
The proven efficacy and safety of biologics has added to the armamentarium of treatment options for patients suffering from psoriasis and PsA. As more biologic therapies enter the marketplace, the opportunity for improved prognosis and symptom control will benefit patients and improve their quality of life. Efficacy and safety, patient comorbidities, patient preference and quality life need to be taken into consideration when dermatologists are prescribing treatment. Continuing education on current and future medications is also needed so dermatologists and other clinicians properly manage patients living with psoriasis.
References
1. National Psoriasis Foundation Web site. Psoriasis statistics. https://www.pso riasis.org/research/science-of-psoriasis/statistics. Accessed November 17, 2015.
2. National Psoriasis Foundation. The Psoriasis and Psoriatic Arthritis Pocket Guide: Treatment Options and Patient Management. 3rd ed. Portland, OR; 2009.
3. Van de Kerkhof PC, Reich K, Kavanaugh A, et al. J Eur Acad Dermatol Venereol. 2015;29(10):2002-2010.
4. Nestle FO, Kaplan DH, Barker J. Psoriasis. N Engl J Med. 2009;36(15):496-509.
5. Feldman SR, Zhao Y, Shi L, Tran ME. Economic and comorbidity burden among patients with moderate-to-severe psoriasis. J Mang Care Spec Pharm. 2015;21(10):874-888.
6. Zhang M, Brenneman SK, Carter CT, et al. Patient-reported treatment satisfaction and choice of dosing frequency with biologic treatment
for moderate to severe plaque psoriasis. Patient Pref Adherence. 2015;8:777-784.
7. Donigan JM, Pascoe VL, Kimball AB. Psoriasis and herpes simplex virus are highly stigmatizing compared with other common dermatologic conditions: A survey-based study. J Am Acad Dermatol. 2015;73(3):525-526.
8. Parisi R, Symmons DR, Griffiths CE, Ashcroft DM. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol. 2013;133(2):377-385.
9. Menter A, Gottlieb A, Feldman SR, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 1. Overview of psoriasis and guidelines of care for the treatment of psoriasis with biologics. J Am Acad Dermatol. 2008;58(5):826-850.
10. Brezinski EA, Dhillon JS, Armstrong AW. Economic burden of psoriasis in the United States: A systematic review. JAMA Dermatol. 2015;151(6):651-658.
11. Gaffen SL. Structure and signaling in the IL-17 receptor family. Nat Rev Immunol. 2009;9(8):556-567.
12. Lin AM, Rubin CJ, Khandpur R, et al. Mast cells and neutrophils release IL-17 through extracellular trap formation in psoriasis. J Immunol. 2011;187(1):490-500.
13. Tracey D, Klareskog L, Sasso EH, Salfeld JG, Tak PP. Tumor necrosis factor antagonist mechanisms of action: a comprehensive review. Pharmacol Ther. 2008;117(2):244-279.
14. Lee E, Trepicchio WL, Oestreicher JL, et al. Increased expression of interleukin 23 p19 and p40 in lesional skin of patients with psoriasis vulgaris. J Exp Med. 2004;199(1):125-130.
15. Awasthi A, Kuchroo VK. Th17 cells: from precursors to players in inflammation and infection. Int Immunol. 2009;21(5):489-498.
16. National Psoriasis Foundation. Moderate to Severe Psoriasis: Biologic Drugs. https://www.psoriasis.org/about-psoriasis/treatments/biologics. Accessed November 16, 2015.
17. Humira [prescribing information]. North Chicago, IL: AbbVie Inc; 2015.
18. Cimzia [prescribing information]. Smyrna, GA: UCB Inc; 2013.
19. Enbrel [prescribing information]. Thousand Oaks, CA: Amgen Inc; 2015.
20. Simponi [prescribing information]. Horsham, PA: Janssen Biotech Inc; 2013.
21. Remicade [prescribing information]. Horsham, PA: Janssen Biotech Inc; 2015.
22. Cosentyx [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2015.
23. Stelara. [prescribing information]. Horsham, PA: Janssen Biotech Inc; 2014.
24. Menter A, Korman NJ, Elmets CA. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 4. Guidelines of care for the management and treatment of psoriasis with traditional systemic agents. J Am Acad Dermatol. 2009;61(3):451-485.
25. Mansouri Y, Goldenberg G. Biologic safety in psoriasis: review of long-term safety data. J Clin Aesthet Dermatol. 2015;8(2):30-42.
26. Menter A, Thaçi D, Papp KA, et al. Five-year analysis from the ESPRIT 10-year postmarketing surveillance registry of adalimumab treatment for moderate to severe psoriasis. J Am Acad Dermatol. 2015;73(3):410-419.
27. Gladman DD, Mease PJ, Choy EH, Ritchlin CT, Perodok RJ, Sasso EH. Risk factors for radiographic progression in psoriatic arthritis: subanalysis of the randomized controlled trial ADEPT. Arthritis Res Ther. 2010;12(3):R113.
28. Mease P, Deodhar A, Fleischmann R, et al. Effect of certolizumab pegol over 96 weeks in patients with psoriatic arthritis with and without prior antitumour necrosis factor exposure. RMD Open. 2015;1(1):e000119.
29. Papp KA, Poulin Y, Bissonnette R, et al. Assessment of the long-term safety and effectiveness of etanercept for the treatment of psoriasis in an adult population. J Am Acad Dermatol. 2012;66(2):e33-45.
30. Kavanaugh A, van der Heijde D, Beutler A, et al. Patients with psoriatic arthritis who achieve minimal disease activity in response to golimumab therapy demonstrate less radiographic progression: Results through 5 years of the randomized, placebo-controlled, GO-REVEAL study. Arthritis Care Res. Published online ahead of print March 16, 2015.
31. Wang J, Zhan Q, Zhang L. A systematic review on the efficacy and safety of infliximab in patients with psoriasis. Hum Vaccin Immunother. Published online ahead of print November 3, 2015.
32. Langley RG, Elewsku BE, Lebwohl M, et al. Secukinumab in plaque psoriasis--results of two phase 3 trials. N Engl J Med. 2014;371(4):326-338.
33. Langley RG, Lebwohol M, Krueger GG, et al. Long-term efficacy and safety of ustekinumab, with and without dosing adjustment, in patients with moderate-to-severe psoriasis: results from the PHOENIX 2 study through 5 years of follow-up. Br J Dermatol. 2015;172(5):1371-1383.
34. Ritchlin C, Rahman P, Kavanaugh A, et al. Efficacy and safety of the anti-IL-12/23 p40 monoclonal antibody, ustekinumab, in patients with active psoriatic arthritis despite conventional non-biological and biological anti-tumour necrosis factor therapy: 6-month and 1-year results of the phase 3, multicentre, double-blind, placebo-controlled, randomised PSUMMIT 2 trial. Ann Rheum Dis. 2014;73(6):990-999.
35. National Psoriasis Foundations. Biologic Drugs: Fact Sheets. https://www.psoriasis.org/about-psoriasis/treatments/biologics/resources. Accessed November 16, 2015.
36. Townsend M, Stober BE. Rare side effects of biologics: part 1. The Dermatologist. 2013;21(11):28-32.
37. Townsend M, Stober BE. Rare side effects of biologics: part 2. The Dermatologist. 2013;21(12):30-34.
38. Levy LL, Solomon SM, Emer JJ. Biologics in the treatment of psoriasis and emerging new therapies in the pipeline. Psoriasis: Targets and Therapy. 2012;2:29-43.
39. Cheng J, Feldman SR. The cost of biologics for psoriasis is increasing. Drug Context. 2014;3:212266.
40. Kamangar F, Isip L, Bhutani T, et al. How psoriasis patients perceive, obtain, and use biologic agents: Survey from an academic medical center. J Dermatolog Treat. 2013;24(1):13-24.
41. Strohal R, Prinz JC, Girolomoni G, Nast A. A patient-centered approach to biological treatment decision making for psoriasis: an expert consensus. J Eur Acad Dermatol Venereol. Published online ahead of print September 14, 2015.
42. Feely MA, Smith BL, Weinberg JM. Novel psoriasis therapies and patient outcomes, part 2: biologic treatments. Cutis. 2015;95(5):282-290.
43. Boehringer Ingelheim’s investigational biologic cleared skin better, faster and for longer than ustekinumab in phase II psoriasis study [news release]. Ridgefield, CT: Boehringer Ingelheim GmbH; October 8, 2015. https://www.boehringer-ingelheim.com/news/news_releases/press_releases/2015/08_oktober_2015_immunology.html. Accessed November 19, 2015.
Psoriasis is a common chronic inflammatory disease that often requires long-term treatment. Characterized by cutaneous inflammation and epidermal hyperproliferation, psoriasis can have a profound impact on quality of life. In recent years, an increased understanding of psoriasis pathophysiology has led to the release of new treatment targets, including biologic therapies. The development of biologic agents has changed the treatment paradigm for dermatologists managing patients with moderate-to-severe psoriasis and psoriatic arthritis (PsA). Biologics, which are protein-based drugs made from living cells, have been shown to improve prognosis and control symptoms and also improve quality of life.
This article provides a brief overview of psoriasis and reviews the efficacy and tolerability of the biologics approved for psoriasis and PsA. Also discussed is the the burden of disease including cost, the importance of clinician and patient education and new biologics in the pipeline.
Overview of Psoriasis
Psoriasis, a disease of T cell dysregulation, is the most prevalent autoimmune disease in the United States, affecting approximately 3% of the US population. Of the individuals with psoriasis, 1.5 million US adults have moderate-to-severe psoriasis. Current published estimates of the worldwide prevalence of psoriasis range from approximately 1% to 3%.1-3 The disease, which is usually manifested as raised, well-demarcated, erythematous oval plaques with adherent silvery scales that are often painful and pruritic, is associated with comorbidities beyond skin manifestations including a higher prevalence of metabolic syndrome, cardiovascular diseases and other autoimmune diseases.4,5
The disease also significantly impacts a patient’s health-related quality of life, psychological well-being and physical and social aspects of daily living.6 For example, patients often feel stigmatized. A recent National Psoriasis Foundation-funded study of 56 participants without any serious skin problems showed that psoriasis is highly stigmatizing and carries the same level of stigma as herpes. A majority of the stigma surrounding psoriasis came down to participants’ belief that the disease was contagious.7
The causes of psoriasis are not fully understood, but a number of risk factors are recognized, including family history and environmental risk factors.8,9 Psoriasis associated with PsA — an inflammatory seronegative spondyloarthropathy — occurs in approximately 10% to 30% of psoriasis patients. In the majority of cases, joint involvement follows skin involvement, often by 10 years.3
Healthcare expenditures associated with psoriasis are significant. A systematic review of 22 studies on the direct, indirect and comorbidity costs of adult psoriasis in the United States found that the annual US cost of psoriasis is approximately $112 billion (2013 US dollars). The direct costs ranged from $51.7 billion to $63.2 billion, indirect costs ranged from $23.9 billion to $35.4 billion and medical comorbidities were estimated to contribute $36.4 billion.10
Biologics for Psoriasis
Various triggers — both internal and external — can initiate psoriatic lesion formation caused by cross-talk between the skin and the immune system. This, in turn, can culminate in a positive inflammatory feedback loop due to the persistent release of pro-inflammatory cytokines including tumor necrosis factor-alpha (TNF-α), interleukin (IL)-23 and IL-17A. Over the past decade, the role of cytokines in the pathogenesis of psoriasis have been elucidated (Table 1).4,11-15 Different from the traditional systemic drugs that impact the entire immune system, biologics target key selective immune pathways.16
Seven biologics are FDA-approved for psoriasis, PsA or both, and more biologics are in the pipeline. These therapies belong to 1 of 2 categories: TNF-α inhibitors or the IL-12/23 and IL-17A monoclonal antibodies. TNF-α inhibitors approved for psoriasis and PsA include adalimumab (Humira, AbbVie Inc.), etanercept (Enbrel, Amgen Inc.) and infliximab (Remicade, Janssen Biotech Inc.), while the TNF-α inhibitors certolizumab pegol (Cimzia, UCB Inc.) and golimumab (Simponi, Janssen Biotech Inc.) are approved for PsA. The IL 12/23 monoclonal antibody ustekinumab (Stelara; Janssen Biotech Inc.) is approved for psoriasis and PsA, and IL-17A monoclonal antibody secukinumab (Cosentyx, Novartis Pharmaceuticals Corporation) is approved for psoriasis.17-23 Each biologic has a unique mechanism of action, dosing schedule and site and route of administration (Table 2).
Before the the first biologic for psoriasis was FDA approved, dermatologists’ treatment options consisted of topical agents, phototherapy and conventional systemic agents. Systemic psoriasis therapies (eg, methotrexate, cyclosporine and acitretin) were used when psoriasis was too extensive for topical therapy or refractory to topical therapy and phototherapy. However, these medications suppress the entire immune function, requiring routine laboratory monitoring because of the increased hepatic and renal toxicity, hematologic conditions and myelosuppresion. Systemic therapies are also contraindicated in various clinical settings (eg, pregnancy and nursing mothers).9, 24
Efficacy and Tolerability
Efficacy and tolerability are 2 of the main factors that affect the choice of biologic treatment, which are now the mainstay of systemic treatment for psoriasis. These biologic agents have demonstrated high efficacy and a favorable safety profile without evidence of cumulative organ-specific toxicity.25
The following highlights outcomes, including long-term studies, that evaluated the effectiveness and safety of the biologics approved for psoriasis and PsA.
Adalimumab
Menter et al26 reported 5-year data from ESPIRIT — the ongoing, multicenter, postmarketing, 10-year, international, observational registry evaluating the long-term safety and efficacy of adalimumab treatment in routine clinical practice. During the first 5 years of treatment, adalimumab continued to be well-tolerated in the majority of the 6,059 patients treated and no new safety signals were observed. The TNF-α inhibitor also showed increased effectiveness across the first 5 years of ESPIRIT.
Adalimumab for PsA has also been effective as shown in a post hoc analysis from ADEPT (Adalimumab Effectiveness in Psoriatic Arthritis Trial) of 152 placebo-treated and 144 adalimumab-treated patients who had evaluable radiographs at baseline and 24 weeks. At 24 weeks, approximately 5-fold reduced risk of radiographic progression was observed with adalimumab. The difference between mean change in modified total Sharp Score (mTSS) for adalimumab versus placebo was greatest for patients with a C-reactive protein ≥2.0 mg/dL (−0.5 vs 2.6, respectively).27
Certolizumab Pegol
Results from RAPID-PsA have demonstrated the efficacy and safety of certolizumab pegol versus placebo over 24 weeks. In a new study, Mease et al28 assessed this efficacy and safety data at 96 weeks with 400 mg certolizumab pegol and 200 mg certolizumab pegol dosing regimens in PsA patients with and without prior anti-TNF exposure. Outcomes measured included American College of Rheumatology (ACR) response. ACR responses were maintained to week 96: 60% of patients achieved ACR 20 at week 24, and 64% at week 96. Improvements were observed with both dose regimens. At 96 weeks, ACR 20 responses were similar in patients with and without prior anti-TNF exposure (63% and 64%, respectively). Placebo patients switching to certolizumab pegol displayed rapid clinical improvements that were maintained to week 96. The findings also showed the prevention of any clinically relevant change in structural damage, as measured by mTSS, for patients treated with certolizumab pegol. The safety profile over 96 weeks was in line with the 24-week data, with no new safety signals reported with increased exposure.
Etanercept
Papp et al29 performed a post hoc analysis on prospective efficacy and safety data for up to 4 years of etanercept use in psoriasis from a cohort of 506 patients who initiated etanercept therapy in either of 2 Phase III trials. Patients received either etanercept 25 mg twice weekly, 50 mg weekly or 50 mg twice weekly, depending on which trial therapy was started. Study endpoints included change from baseline for the static Physician Global Assessment (sPGA) and Dermatology Life Quality Index (DLQI) scores. In all, 75.9% and 27.8% maintained DLQI response (≥5-point improvement from baseline) and sPGA response (clear or almost clear) at 48 months, respectively.
Golimumab
Kavanaugh et al30 evaluated the the long-term outcomes in PsA patients who achieved or did not achieve minimal disease activity (MDA) through 5 years of golimumab treatment in GO-REVEAL (Golimumab—A Randomized Evaluation of Safety and Efficacy in Subjects with Psoriatic Arthritis Using a Human Anti-TNF Monoclonal Antibody). GO-REVEAL was a Phase III, multicenter, randomized, double-blind, placebo-controlled trial through week 24 followed by an open-label phase lasting up to 5 years that included 405 patients randomized to placebo, golimumab 50 mg or golimumab 100 mg every 4 weeks. Treatment with golimumab yielded significantly higher MDA response rates versus placebo at week 24 (28.1% vs 7.7%, respectively) and week 52 (42.4% vs 30.2%, respectively). MDA was achieved at least once by ∼50% of golimumab-treated patients overall. Among golimumab-treated patients, patient global assessment and radiographic outcomes were also observed when patients achieved persistent MDA.
Article continues on page 2
{{pagebreak}}
Infliximab
A meta-analysis of randomized, controlled studies that assessed the efficacy and safety of infliximab for the treatment of psoriasis and PsA showed that infliximab is significantly associated with symptom relief, skin lesion improvement and increase quality of life. Wang et al31 found statistically significant differences in efficacy for infliximab 3 mg/kg or 5 mg/kg group (odds ratio [OR], 13.55 and 85.45, respectively) compared with the placebo group for psoriasis vulgaris. Significant differences in efficacy between the infliximab 5 mg/kg and placebo groups during treatment for PsA was also observed (OR, 8.36).
Secukinumab
Secukinumab is most first and only FDA approved IL-17A antagonist for psoriasis. Langley et al32 assessed secukimumab in 2 Phase III, double-blind, 52-week trials, ERASURE (Efficacy of Response and Safety of Two Fixed Secukinumab Regimens in Psoriasis) and FIXTURE (Full Year Investigative Examination of Secukinumab vs Etanercept Using Two Dosing Regimens to Determine Efficacy in Psoriasis). The researchers randomly assigned 738 patients (ERASURE) and 1,306 patients (FIXTURE) to secukinumab 300 mg or 150 mg (once weekly for 5 weeks, then every 4 weeks), placebo or in the FIXTURE study only etanercept at 50 mg (twice weekly for 12 weeks, then once weekly). The primary endpoints were Psoriasis Area and Severity Index (PSAI) 75 response and a score of clear or almost clear on the Investigator’s Global Assessment (IGA) at 12 weeks.
Patients who met Psoriasis Area and Severity Index PASI 75 at week 12 was higher with each secukinumab dose versus placebo or etanercept. The rates in ERASURE were 81.6% with 300 mg secukinumab, 71.6% with 150 mg secukinumab and 4.5% with placebo; in the FIXTURE study the rates were 77.1%, 67.0% and 4.9%, respectively, and 44.0% with etanercept. Patients who achieved IGA score of clear or almost clear at 12 weeks was also higher with each secukinumab dose versus placebo and etanercept. In ERASURE, the rates were 65.3% with 300 mg secukinumab, 51.2% with 150 mg secukinumab and 2.4% with placebo; in FIXTURE, the rates were 62.5%, 51.1% and 2.8%, respectively, and 27.2% with etanercept.32
Ustekinumab
Long-term follow-up from PHOENIX 2 (Phase 3, Multicenter, Randomized, Double-blind, Placebo-controlled Trial Evaluating the Efficacy and Safety of CNTO 1275 in the Treatment of Subjects with Moderate to Severe Plaque-type Psoriasis) found that 5 years of continuous ustekinumab treatment was safe and effective.33 Patients were randomized to placebo or ustekinumab 45 mg or 90 mg at weeks 0, 4 then every 12 weeks; patients receiving placebo crossed-over at week 12. Dosing adjustments were permitted at different time points. Efficacy and safety were evaluated through weeks 244 and 264, respectively. In the overall population, the researchers found that 70% of ustekinumab-treated patients completed treatment through week 244, with more patients responding to the 45 mg and 90 mg doses, respectively: PASI 75 responses were 76.5% and 78.6%, respectively, and PASI 90 were 50.0% and 55.5%, respectively. Improved response was generally observed following dosing adjustments.
Ustekinumab 45 mg and 90 mg was also proven effective for long-term therapy in PsA, according to results at week 60 from PSUMMIT 2 (Phase 3 Multicenter, Randomized, Double-blind, Placebo-controlled Trial of Ustekinumab, a Fully Human Aanti-IL-12/23p40 Monoclonal Antibody, Administered Subcutaneously, in Subjects with Active Psoriatic Arthritis), which included patients with and without prior exposure to anti-TNF agents. The primary endpoint was ≥20% improvement in ACR at week 24. More ustekinumab-treated patients (43.8% combined for 45 mg and 90 mg) than placebo-treated patients achieved ACR 20 response week 24. Among patients previously treated with ≥1 TNF inhibitor, sustained ustekinumab efficacy was also observed at week 24 versus placebo in ACR 20 response (35.6% combined for 45 mg and 90 mg vs 14.5%, respectively).34
Adverse Events
Overall, the most commonly reported adverse events (AEs) in clinical trials of biologics were mild and did not result in discontinuation of therapy (Table 3).35 In a 2-part series published in The Dermatologist36,37 on rare AEs of biologics reported in the literature, rare AEs fell into 6 categories: inflammatory skin disease, atypical infectious events, blood disorders, connective tissue disease, neurologic events and cardiac/metabolic abnormalities. Because there are AEs associated with biologic therapies, clinicians should prescreen patients before initiation and continue monitoring patients during and after treatments.38
A potential disadvantage to biologic therapy is it has to be given either by injection or intravenous infusion. Infusion can last 2 hours per session (Table 2).
Economic Burden of Biologics
Biologics for psoriasis have shown significant reductions in the number of hospital stays, use of other systemic therapies, improved PASI outcomes and increased patient satisfaction. Yet, the annual cost of these drugs is substantial. Cheng et al39 examined the cost of annual treatment paradigms for etanercept, adalimumab and ustekinumab using the average wholesale price. The cost of 1 year of induction and maintenance treatment was highest for ustekinumab ($53,909), followed by etanercept ($46,395) and adalimumab ($39,041). The sales-based cost of drugs was greatest for ustekinumab ($25,012), then adalimumab ($6,786) and etanercept ($6,629).
Cost is also an important factor for patients prescribed biologics. A survey of 106 patients at an academic medical center to discern patient attitudes toward biologics found that patients with lower income levels had increased cutbacks in personal expenses due to copayments. Among respondents, the mean annual out of pocket expense for current biologics was $557.12 per year, with a range of $0 to $7,000.40
To offset cost of therapy, the manufacturers of biologics offer programs to help determine patient eligibility and treatment cost.
Patient Preference and Education
Each individual psoriasis patient has different expectations and goals for biological treatment, which may differ from those of the clinician. Understanding the needs and expectations of patients from treatment should constitute a fundamental part of treatment with biologics.41 To better understand and align patients’ and physicians’ preferences and goals for biological treatment, a working group of psoriasis experts developed a questionnaire that can be given to patients during consultation with their dermatologist. The goal of the questionnaire is that it will offer a more structured approach when choosing a biological therapy that incorporates patients’ treatment preferences.41 When deciding on an appropriate biologic therapy, clinicians need to educate patients on the advantages and disadvantages associated with therapy so they can be involved in the decision-making process. Clinicians should also continue to be educated on the efficacy and tolerability of biologic therapy. Once a patient is started on therapy, clinicians should monitor adherence and gauge satisfaction with therapy.
In a study that assessed patient-reported treatment and dosing frequency choice with biologics, Zhang et al6 found that overall patient satisfaction with biologic treatment of psoriasis is good among patients who have previously tried or are receiving a biologic treatment. The researchers concluded that patients’ choices regarding dosing schedule and treatment satisfaction should be included among all other considerations in determining an appropriate treatment.
A separate study by Kamanger et al40 that assessed patients’ attitudes with biologics found that 62.6% of respondents were “very satisfied” with biologics, and 74.5% learned about biologics from their physician. When asked about concern that biologics medications will cause an AE, 57.5% of patients responded “not worried at all.” The survey also found that compliance rates for biologic therapy was high with 66.6% of respondents reporting “never” or “rarely” missing a dose.
Pipeline of Biologic Drugs
Many novel treatments in the pipeline promise exciting new therapeutic avenues for psoriasis and PsA that target various cytokines and regulatory molecules involved in the pathogenesis of psoriasis including inhibition of the IL-12/IL-23 pathway; inhibition of IL-17 pathway; inhibition of T cell activation in antigen-presenting cells; activation of regulatory T cells; inhibition of toll-like receptors (TLRs) 7, 8 and 9 and inhibition of granulocyte-macrophage colony-stimulating factor (GM-CSF).42
IL-17 receptor blockers have recently received FDA approval. Secukimumab was the first drug approved in this class in January 2015 for psoriasis. Brodalumab and ixekizumab are 2 other agents in this class that show promise. In a Phase III study, 661 patients received brodalumab 210 mg or 140 mg or placebo. At week 12, PASI 75 was observed in 83% of the 210 mg group versus 60% of the 140 mg group; PASI 100 was observed in 42% of the 210 mg group versus 23% of the 140 mg group. Results of a Phase II trial of ixekizumab (N=142) found that PSAI 75 were significantly improved versus placebo (150 mg, 82.1%; 75 mg, 82.8% and 25 mg, 76.7% vs 7.7% with placebo).42 Amgen Inc. had initially partnered with AstraZeneca in developing brodalumab, but announced their withdrawal from the project earlier this year following the observation of suicidal behavior and ideation observed in some subjects taking the medication. The impact of these findings on further medication development is not yet clear.
New drugs that specifically target IL-23 pathway such as guselkumab and tildrakizumab are in Phase II and III studies for psoriasis.42 Results from a Phase II study of BI 655066 — another agent that targets the IL-23 pathway — were recently presented at the 24th European Academy of Dermatology and Venereology. The head-to-head study evaluated the efficacy and safety of BI 655066 versus ustekinumab in 166 patients with moderate-to-severe-plaque psoriasis and found that 39% more patients maintained clear or almost clear skin (PASI 90) on BI 655066 after 9 months compared with ustekinumab. Nearly triple the percentage of patients maintained completely clear skin (PASI 100) on BI 655066 after 9 months versus ustekinumab (69% vs 30%, respectively). Additionally, clear skin or almost clear skin (PASI 90) was achieved faster and maintained for more than 2 months longer with BI 655066 compared with ustekinumab.43
Other therapies in development include abatacept, a fusion protein designed to inhibit T cell activation by binding receptors for CD80 and CD86 in antigen-presenting cells, that is in Phase III studies for psoriasis and PsA. Tregalizumab, a monoclonal antibody that activates regulatory T cells, is in Phase II studies for psoriasis. IMO-8400 is unique in that it treats psoriasis by targeting TLRs 7, 8 and 9; Phase II studies are underway. Namilumab, a GM-CSF inhibitor, is in Phase II studies for psoriasis.42
Conclusion
The proven efficacy and safety of biologics has added to the armamentarium of treatment options for patients suffering from psoriasis and PsA. As more biologic therapies enter the marketplace, the opportunity for improved prognosis and symptom control will benefit patients and improve their quality of life. Efficacy and safety, patient comorbidities, patient preference and quality life need to be taken into consideration when dermatologists are prescribing treatment. Continuing education on current and future medications is also needed so dermatologists and other clinicians properly manage patients living with psoriasis.
References
1. National Psoriasis Foundation Web site. Psoriasis statistics. https://www.pso riasis.org/research/science-of-psoriasis/statistics. Accessed November 17, 2015.
2. National Psoriasis Foundation. The Psoriasis and Psoriatic Arthritis Pocket Guide: Treatment Options and Patient Management. 3rd ed. Portland, OR; 2009.
3. Van de Kerkhof PC, Reich K, Kavanaugh A, et al. J Eur Acad Dermatol Venereol. 2015;29(10):2002-2010.
4. Nestle FO, Kaplan DH, Barker J. Psoriasis. N Engl J Med. 2009;36(15):496-509.
5. Feldman SR, Zhao Y, Shi L, Tran ME. Economic and comorbidity burden among patients with moderate-to-severe psoriasis. J Mang Care Spec Pharm. 2015;21(10):874-888.
6. Zhang M, Brenneman SK, Carter CT, et al. Patient-reported treatment satisfaction and choice of dosing frequency with biologic treatment
for moderate to severe plaque psoriasis. Patient Pref Adherence. 2015;8:777-784.
7. Donigan JM, Pascoe VL, Kimball AB. Psoriasis and herpes simplex virus are highly stigmatizing compared with other common dermatologic conditions: A survey-based study. J Am Acad Dermatol. 2015;73(3):525-526.
8. Parisi R, Symmons DR, Griffiths CE, Ashcroft DM. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol. 2013;133(2):377-385.
9. Menter A, Gottlieb A, Feldman SR, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 1. Overview of psoriasis and guidelines of care for the treatment of psoriasis with biologics. J Am Acad Dermatol. 2008;58(5):826-850.
10. Brezinski EA, Dhillon JS, Armstrong AW. Economic burden of psoriasis in the United States: A systematic review. JAMA Dermatol. 2015;151(6):651-658.
11. Gaffen SL. Structure and signaling in the IL-17 receptor family. Nat Rev Immunol. 2009;9(8):556-567.
12. Lin AM, Rubin CJ, Khandpur R, et al. Mast cells and neutrophils release IL-17 through extracellular trap formation in psoriasis. J Immunol. 2011;187(1):490-500.
13. Tracey D, Klareskog L, Sasso EH, Salfeld JG, Tak PP. Tumor necrosis factor antagonist mechanisms of action: a comprehensive review. Pharmacol Ther. 2008;117(2):244-279.
14. Lee E, Trepicchio WL, Oestreicher JL, et al. Increased expression of interleukin 23 p19 and p40 in lesional skin of patients with psoriasis vulgaris. J Exp Med. 2004;199(1):125-130.
15. Awasthi A, Kuchroo VK. Th17 cells: from precursors to players in inflammation and infection. Int Immunol. 2009;21(5):489-498.
16. National Psoriasis Foundation. Moderate to Severe Psoriasis: Biologic Drugs. https://www.psoriasis.org/about-psoriasis/treatments/biologics. Accessed November 16, 2015.
17. Humira [prescribing information]. North Chicago, IL: AbbVie Inc; 2015.
18. Cimzia [prescribing information]. Smyrna, GA: UCB Inc; 2013.
19. Enbrel [prescribing information]. Thousand Oaks, CA: Amgen Inc; 2015.
20. Simponi [prescribing information]. Horsham, PA: Janssen Biotech Inc; 2013.
21. Remicade [prescribing information]. Horsham, PA: Janssen Biotech Inc; 2015.
22. Cosentyx [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2015.
23. Stelara. [prescribing information]. Horsham, PA: Janssen Biotech Inc; 2014.
24. Menter A, Korman NJ, Elmets CA. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 4. Guidelines of care for the management and treatment of psoriasis with traditional systemic agents. J Am Acad Dermatol. 2009;61(3):451-485.
25. Mansouri Y, Goldenberg G. Biologic safety in psoriasis: review of long-term safety data. J Clin Aesthet Dermatol. 2015;8(2):30-42.
26. Menter A, Thaçi D, Papp KA, et al. Five-year analysis from the ESPRIT 10-year postmarketing surveillance registry of adalimumab treatment for moderate to severe psoriasis. J Am Acad Dermatol. 2015;73(3):410-419.
27. Gladman DD, Mease PJ, Choy EH, Ritchlin CT, Perodok RJ, Sasso EH. Risk factors for radiographic progression in psoriatic arthritis: subanalysis of the randomized controlled trial ADEPT. Arthritis Res Ther. 2010;12(3):R113.
28. Mease P, Deodhar A, Fleischmann R, et al. Effect of certolizumab pegol over 96 weeks in patients with psoriatic arthritis with and without prior antitumour necrosis factor exposure. RMD Open. 2015;1(1):e000119.
29. Papp KA, Poulin Y, Bissonnette R, et al. Assessment of the long-term safety and effectiveness of etanercept for the treatment of psoriasis in an adult population. J Am Acad Dermatol. 2012;66(2):e33-45.
30. Kavanaugh A, van der Heijde D, Beutler A, et al. Patients with psoriatic arthritis who achieve minimal disease activity in response to golimumab therapy demonstrate less radiographic progression: Results through 5 years of the randomized, placebo-controlled, GO-REVEAL study. Arthritis Care Res. Published online ahead of print March 16, 2015.
31. Wang J, Zhan Q, Zhang L. A systematic review on the efficacy and safety of infliximab in patients with psoriasis. Hum Vaccin Immunother. Published online ahead of print November 3, 2015.
32. Langley RG, Elewsku BE, Lebwohl M, et al. Secukinumab in plaque psoriasis--results of two phase 3 trials. N Engl J Med. 2014;371(4):326-338.
33. Langley RG, Lebwohol M, Krueger GG, et al. Long-term efficacy and safety of ustekinumab, with and without dosing adjustment, in patients with moderate-to-severe psoriasis: results from the PHOENIX 2 study through 5 years of follow-up. Br J Dermatol. 2015;172(5):1371-1383.
34. Ritchlin C, Rahman P, Kavanaugh A, et al. Efficacy and safety of the anti-IL-12/23 p40 monoclonal antibody, ustekinumab, in patients with active psoriatic arthritis despite conventional non-biological and biological anti-tumour necrosis factor therapy: 6-month and 1-year results of the phase 3, multicentre, double-blind, placebo-controlled, randomised PSUMMIT 2 trial. Ann Rheum Dis. 2014;73(6):990-999.
35. National Psoriasis Foundations. Biologic Drugs: Fact Sheets. https://www.psoriasis.org/about-psoriasis/treatments/biologics/resources. Accessed November 16, 2015.
36. Townsend M, Stober BE. Rare side effects of biologics: part 1. The Dermatologist. 2013;21(11):28-32.
37. Townsend M, Stober BE. Rare side effects of biologics: part 2. The Dermatologist. 2013;21(12):30-34.
38. Levy LL, Solomon SM, Emer JJ. Biologics in the treatment of psoriasis and emerging new therapies in the pipeline. Psoriasis: Targets and Therapy. 2012;2:29-43.
39. Cheng J, Feldman SR. The cost of biologics for psoriasis is increasing. Drug Context. 2014;3:212266.
40. Kamangar F, Isip L, Bhutani T, et al. How psoriasis patients perceive, obtain, and use biologic agents: Survey from an academic medical center. J Dermatolog Treat. 2013;24(1):13-24.
41. Strohal R, Prinz JC, Girolomoni G, Nast A. A patient-centered approach to biological treatment decision making for psoriasis: an expert consensus. J Eur Acad Dermatol Venereol. Published online ahead of print September 14, 2015.
42. Feely MA, Smith BL, Weinberg JM. Novel psoriasis therapies and patient outcomes, part 2: biologic treatments. Cutis. 2015;95(5):282-290.
43. Boehringer Ingelheim’s investigational biologic cleared skin better, faster and for longer than ustekinumab in phase II psoriasis study [news release]. Ridgefield, CT: Boehringer Ingelheim GmbH; October 8, 2015. https://www.boehringer-ingelheim.com/news/news_releases/press_releases/2015/08_oktober_2015_immunology.html. Accessed November 19, 2015.










