
In the October 2015 issue of The Dermatologist, dermatologic procedures with 10-day global periods were discussed. This article (Part 5 in the series) will discuss procedures with 90-day global periods, as well as proper coding of some other miscellaneous procedures.
Procedures with 90-day global periods are considered major procedures and for the most part are performed in a hospital or outpatient surgery center. There are a few procedures performed in dermatology that are associated with 90-day global periods. It is important to note that the total global period of a 90-day procedure is actually 92 days, as the day prior to the procedure and the day of the procedure are included, along with the 90 days following the procedure. Most 90-day procedures in dermatology are complex repairs of skin excisions or Mohs excisions. These include complex linear repairs, any type of flap repair including rotational, transposition and interpolation, and both split-thickness and full-thickness skin grafts (Table 1).
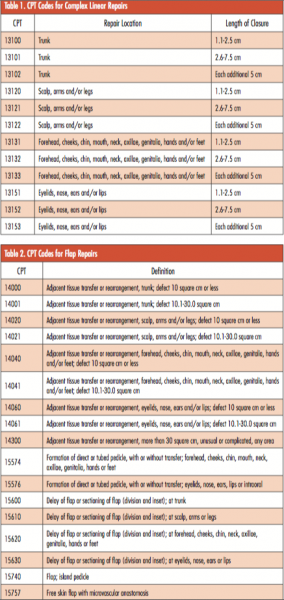 Similar to other procedures, these Current Procedural Terminology (CPT) codes include supplies, suture removal visits and postoperative complications within the 90-day global period. Complex linear repairs are defined as needing retention sutures to anchor tissue in place, extensive undermining, stents, debridement or scar revision. The phrase “extensive undermining” is not specifically defined by the CPT guidelines; therefore, it is up to the physician to determine what qualifies as extensive undermining. For complex linear repairs, there are CPT codes used to indicate extra closure lengths beyond 7.5 cm. These codes should be submitted in addition to the primary repair CPT code. For each additional 5 cm beyond the primary CPT code, a quantity modifier should be used. For example, a complex linear repair on the trunk that is 17 cm in length, would require CPT code 13101 and 13102 + 2 in order to bill for the entire length of the closure. Note that secondary intention closure of a surgical defect is CPT code 13160 and has a global period of zero days.
Similar to other procedures, these Current Procedural Terminology (CPT) codes include supplies, suture removal visits and postoperative complications within the 90-day global period. Complex linear repairs are defined as needing retention sutures to anchor tissue in place, extensive undermining, stents, debridement or scar revision. The phrase “extensive undermining” is not specifically defined by the CPT guidelines; therefore, it is up to the physician to determine what qualifies as extensive undermining. For complex linear repairs, there are CPT codes used to indicate extra closure lengths beyond 7.5 cm. These codes should be submitted in addition to the primary repair CPT code. For each additional 5 cm beyond the primary CPT code, a quantity modifier should be used. For example, a complex linear repair on the trunk that is 17 cm in length, would require CPT code 13101 and 13102 + 2 in order to bill for the entire length of the closure. Note that secondary intention closure of a surgical defect is CPT code 13160 and has a global period of zero days.
Repair flaps are used to rotate or move tissue into a surgical defect and by definition require extensive undermining (Table 2). Flaps are mostly used in Mohs surgery cases or head and neck excisions. The CPT code for a flap is determined by the anatomic location and the tissue square. The tissue square size is obtained by measuring the length and width of both the excision defect and the area of the undermined flap. Skin graft repairs take skin from a distant body site and graft them onto a surgical defect (Table 3). Full-thickness grafts use skin down to subcutaneous fat, split-thickness grafts use epidermis and part of the dermis, and composite grafts include skin and cartilage. Xenografts use non-human skin as graft skin, such as a porcine graft. The repair of the donor site in full-thickness skin grafts is included within the repair code and should not be billed separately.
Lip wedge excisions are involved procedures that usually require 3-layered closure of mucosa, muscle and skin. Due to their complexity, these procedures are associated with a 90-day global period (Table 4).


Miscellaneous Procedures
Several other procedures can be performed by dermatologists that have not yet been described. Phototherapy is considered a procedure, and does not have to be performed by a physician. Different CPT codes exist for different types of phototherapy based on whether the patient receives UVA or UVB, and UV laser treatment coding is determined by total area treated (Table 5).

Now that onabotulinumtoxinA (Botox, Allergan Inc.) is FDA approved for treatment of hyperhidrosis some insurance companies will reimburse for axillary injections. This typically will not be reimbursed without prior authorization and documentation of previously failed treatments. The CPT code for chemical denervation of eccrine glands is 64650. A J code is also submitted which account for the quantity of botulinum toxin used, and a quantity modifier is needed as well. The J code J0585 codes for 1 unit of botulinum toxin, so if 50 units are administered then the quantity modifier 50 would go after the J code.
 Photodynamic therapy is used for treatment of actinic skin damage and is coded using CPT code 96567. This code is defined as photodynamic therapy by external application of light to destroy premalignant and/or malignant lesions of the skin and adjacent mucosa by activation of photosensitive drug(s), each phototherapy exposure session. This CPT code also requires a J code J7803 which reimburses for aminolevulinic acid HCl for topical administration, 20%, single-unit dosage form (Levulan Kerastick, DUSA Pharmaceuticals Inc.). For Medicare, Evaluation and Management (E/M) services are not permitted to be reported on the same date of service that photodynamic therapy (CPT 96567) is performed. You may report an E/M code if an unrelated condition is treated or evaluated during the same visit as photodynamic therapy. This will require a secondary diagnosis on the claim related to the E/M visit and the appropriate modifier.
Photodynamic therapy is used for treatment of actinic skin damage and is coded using CPT code 96567. This code is defined as photodynamic therapy by external application of light to destroy premalignant and/or malignant lesions of the skin and adjacent mucosa by activation of photosensitive drug(s), each phototherapy exposure session. This CPT code also requires a J code J7803 which reimburses for aminolevulinic acid HCl for topical administration, 20%, single-unit dosage form (Levulan Kerastick, DUSA Pharmaceuticals Inc.). For Medicare, Evaluation and Management (E/M) services are not permitted to be reported on the same date of service that photodynamic therapy (CPT 96567) is performed. You may report an E/M code if an unrelated condition is treated or evaluated during the same visit as photodynamic therapy. This will require a secondary diagnosis on the claim related to the E/M visit and the appropriate modifier.
Dermabrasion may be covered by some insurance companies as third- or fourth-line treatment for keloids, acne or scarring if patients have demonstrated at least 6 months of failing first- and second-line treatments (Table 6). The provider should obtain prior authorization for this procedure prior to submitting a claim.
In rare instances, chemical peels may be covered by insurance companies for actinic damage or other medical reasons (Table 7). Acne surgery is defined as marsupialization, opening or removal of multiple milia, comedones, cysts, pustules and is associated with CPT code 10040. Sclerotherapy sometimes can be reimbursed procedures if varicosities are associated with pain and if patients have failed more conservative measures (Table 8).
Most of the CPT codes for nail procedures listed in Table 9 would be more commonly used by podiatrists or orthopedic surgeons, but dermatologists sometimes perform procedures on the nail unit.
The next article in this series will discuss E/M and CPT modifiers needed for proper billing and reimbursement.
Dr. Strowd is assistant professor of dermatology at Wake Forest School of Medicine in Winston-Salem, NC.
Disclosure: The author reports no relevant financial relationships.

In the October 2015 issue of The Dermatologist, dermatologic procedures with 10-day global periods were discussed. This article (Part 5 in the series) will discuss procedures with 90-day global periods, as well as proper coding of some other miscellaneous procedures.
Procedures with 90-day global periods are considered major procedures and for the most part are performed in a hospital or outpatient surgery center. There are a few procedures performed in dermatology that are associated with 90-day global periods. It is important to note that the total global period of a 90-day procedure is actually 92 days, as the day prior to the procedure and the day of the procedure are included, along with the 90 days following the procedure. Most 90-day procedures in dermatology are complex repairs of skin excisions or Mohs excisions. These include complex linear repairs, any type of flap repair including rotational, transposition and interpolation, and both split-thickness and full-thickness skin grafts (Table 1).
 Similar to other procedures, these Current Procedural Terminology (CPT) codes include supplies, suture removal visits and postoperative complications within the 90-day global period. Complex linear repairs are defined as needing retention sutures to anchor tissue in place, extensive undermining, stents, debridement or scar revision. The phrase “extensive undermining” is not specifically defined by the CPT guidelines; therefore, it is up to the physician to determine what qualifies as extensive undermining. For complex linear repairs, there are CPT codes used to indicate extra closure lengths beyond 7.5 cm. These codes should be submitted in addition to the primary repair CPT code. For each additional 5 cm beyond the primary CPT code, a quantity modifier should be used. For example, a complex linear repair on the trunk that is 17 cm in length, would require CPT code 13101 and 13102 + 2 in order to bill for the entire length of the closure. Note that secondary intention closure of a surgical defect is CPT code 13160 and has a global period of zero days.
Similar to other procedures, these Current Procedural Terminology (CPT) codes include supplies, suture removal visits and postoperative complications within the 90-day global period. Complex linear repairs are defined as needing retention sutures to anchor tissue in place, extensive undermining, stents, debridement or scar revision. The phrase “extensive undermining” is not specifically defined by the CPT guidelines; therefore, it is up to the physician to determine what qualifies as extensive undermining. For complex linear repairs, there are CPT codes used to indicate extra closure lengths beyond 7.5 cm. These codes should be submitted in addition to the primary repair CPT code. For each additional 5 cm beyond the primary CPT code, a quantity modifier should be used. For example, a complex linear repair on the trunk that is 17 cm in length, would require CPT code 13101 and 13102 + 2 in order to bill for the entire length of the closure. Note that secondary intention closure of a surgical defect is CPT code 13160 and has a global period of zero days.
Repair flaps are used to rotate or move tissue into a surgical defect and by definition require extensive undermining (Table 2). Flaps are mostly used in Mohs surgery cases or head and neck excisions. The CPT code for a flap is determined by the anatomic location and the tissue square. The tissue square size is obtained by measuring the length and width of both the excision defect and the area of the undermined flap. Skin graft repairs take skin from a distant body site and graft them onto a surgical defect (Table 3). Full-thickness grafts use skin down to subcutaneous fat, split-thickness grafts use epidermis and part of the dermis, and composite grafts include skin and cartilage. Xenografts use non-human skin as graft skin, such as a porcine graft. The repair of the donor site in full-thickness skin grafts is included within the repair code and should not be billed separately.
Lip wedge excisions are involved procedures that usually require 3-layered closure of mucosa, muscle and skin. Due to their complexity, these procedures are associated with a 90-day global period (Table 4).


Miscellaneous Procedures
Several other procedures can be performed by dermatologists that have not yet been described. Phototherapy is considered a procedure, and does not have to be performed by a physician. Different CPT codes exist for different types of phototherapy based on whether the patient receives UVA or UVB, and UV laser treatment coding is determined by total area treated (Table 5).

Now that onabotulinumtoxinA (Botox, Allergan Inc.) is FDA approved for treatment of hyperhidrosis some insurance companies will reimburse for axillary injections. This typically will not be reimbursed without prior authorization and documentation of previously failed treatments. The CPT code for chemical denervation of eccrine glands is 64650. A J code is also submitted which account for the quantity of botulinum toxin used, and a quantity modifier is needed as well. The J code J0585 codes for 1 unit of botulinum toxin, so if 50 units are administered then the quantity modifier 50 would go after the J code.
 Photodynamic therapy is used for treatment of actinic skin damage and is coded using CPT code 96567. This code is defined as photodynamic therapy by external application of light to destroy premalignant and/or malignant lesions of the skin and adjacent mucosa by activation of photosensitive drug(s), each phototherapy exposure session. This CPT code also requires a J code J7803 which reimburses for aminolevulinic acid HCl for topical administration, 20%, single-unit dosage form (Levulan Kerastick, DUSA Pharmaceuticals Inc.). For Medicare, Evaluation and Management (E/M) services are not permitted to be reported on the same date of service that photodynamic therapy (CPT 96567) is performed. You may report an E/M code if an unrelated condition is treated or evaluated during the same visit as photodynamic therapy. This will require a secondary diagnosis on the claim related to the E/M visit and the appropriate modifier.
Photodynamic therapy is used for treatment of actinic skin damage and is coded using CPT code 96567. This code is defined as photodynamic therapy by external application of light to destroy premalignant and/or malignant lesions of the skin and adjacent mucosa by activation of photosensitive drug(s), each phototherapy exposure session. This CPT code also requires a J code J7803 which reimburses for aminolevulinic acid HCl for topical administration, 20%, single-unit dosage form (Levulan Kerastick, DUSA Pharmaceuticals Inc.). For Medicare, Evaluation and Management (E/M) services are not permitted to be reported on the same date of service that photodynamic therapy (CPT 96567) is performed. You may report an E/M code if an unrelated condition is treated or evaluated during the same visit as photodynamic therapy. This will require a secondary diagnosis on the claim related to the E/M visit and the appropriate modifier.
Dermabrasion may be covered by some insurance companies as third- or fourth-line treatment for keloids, acne or scarring if patients have demonstrated at least 6 months of failing first- and second-line treatments (Table 6). The provider should obtain prior authorization for this procedure prior to submitting a claim.
In rare instances, chemical peels may be covered by insurance companies for actinic damage or other medical reasons (Table 7). Acne surgery is defined as marsupialization, opening or removal of multiple milia, comedones, cysts, pustules and is associated with CPT code 10040. Sclerotherapy sometimes can be reimbursed procedures if varicosities are associated with pain and if patients have failed more conservative measures (Table 8).
Most of the CPT codes for nail procedures listed in Table 9 would be more commonly used by podiatrists or orthopedic surgeons, but dermatologists sometimes perform procedures on the nail unit.
The next article in this series will discuss E/M and CPT modifiers needed for proper billing and reimbursement.
Dr. Strowd is assistant professor of dermatology at Wake Forest School of Medicine in Winston-Salem, NC.
Disclosure: The author reports no relevant financial relationships.
In the October 2015 issue of The Dermatologist, dermatologic procedures with 10-day global periods were discussed. This article (Part 5 in the series) will discuss procedures with 90-day global periods, as well as proper coding of some other miscellaneous procedures.
Procedures with 90-day global periods are considered major procedures and for the most part are performed in a hospital or outpatient surgery center. There are a few procedures performed in dermatology that are associated with 90-day global periods. It is important to note that the total global period of a 90-day procedure is actually 92 days, as the day prior to the procedure and the day of the procedure are included, along with the 90 days following the procedure. Most 90-day procedures in dermatology are complex repairs of skin excisions or Mohs excisions. These include complex linear repairs, any type of flap repair including rotational, transposition and interpolation, and both split-thickness and full-thickness skin grafts (Table 1).
Similar to other procedures, these Current Procedural Terminology (CPT) codes include supplies, suture removal visits and postoperative complications within the 90-day global period. Complex linear repairs are defined as needing retention sutures to anchor tissue in place, extensive undermining, stents, debridement or scar revision. The phrase “extensive undermining” is not specifically defined by the CPT guidelines; therefore, it is up to the physician to determine what qualifies as extensive undermining. For complex linear repairs, there are CPT codes used to indicate extra closure lengths beyond 7.5 cm. These codes should be submitted in addition to the primary repair CPT code. For each additional 5 cm beyond the primary CPT code, a quantity modifier should be used. For example, a complex linear repair on the trunk that is 17 cm in length, would require CPT code 13101 and 13102 + 2 in order to bill for the entire length of the closure. Note that secondary intention closure of a surgical defect is CPT code 13160 and has a global period of zero days.
Repair flaps are used to rotate or move tissue into a surgical defect and by definition require extensive undermining (Table 2). Flaps are mostly used in Mohs surgery cases or head and neck excisions. The CPT code for a flap is determined by the anatomic location and the tissue square. The tissue square size is obtained by measuring the length and width of both the excision defect and the area of the undermined flap. Skin graft repairs take skin from a distant body site and graft them onto a surgical defect (Table 3). Full-thickness grafts use skin down to subcutaneous fat, split-thickness grafts use epidermis and part of the dermis, and composite grafts include skin and cartilage. Xenografts use non-human skin as graft skin, such as a porcine graft. The repair of the donor site in full-thickness skin grafts is included within the repair code and should not be billed separately.
Lip wedge excisions are involved procedures that usually require 3-layered closure of mucosa, muscle and skin. Due to their complexity, these procedures are associated with a 90-day global period (Table 4).
Miscellaneous Procedures
Several other procedures can be performed by dermatologists that have not yet been described. Phototherapy is considered a procedure, and does not have to be performed by a physician. Different CPT codes exist for different types of phototherapy based on whether the patient receives UVA or UVB, and UV laser treatment coding is determined by total area treated (Table 5).
Now that onabotulinumtoxinA (Botox, Allergan Inc.) is FDA approved for treatment of hyperhidrosis some insurance companies will reimburse for axillary injections. This typically will not be reimbursed without prior authorization and documentation of previously failed treatments. The CPT code for chemical denervation of eccrine glands is 64650. A J code is also submitted which account for the quantity of botulinum toxin used, and a quantity modifier is needed as well. The J code J0585 codes for 1 unit of botulinum toxin, so if 50 units are administered then the quantity modifier 50 would go after the J code.
Photodynamic therapy is used for treatment of actinic skin damage and is coded using CPT code 96567. This code is defined as photodynamic therapy by external application of light to destroy premalignant and/or malignant lesions of the skin and adjacent mucosa by activation of photosensitive drug(s), each phototherapy exposure session. This CPT code also requires a J code J7803 which reimburses for aminolevulinic acid HCl for topical administration, 20%, single-unit dosage form (Levulan Kerastick, DUSA Pharmaceuticals Inc.). For Medicare, Evaluation and Management (E/M) services are not permitted to be reported on the same date of service that photodynamic therapy (CPT 96567) is performed. You may report an E/M code if an unrelated condition is treated or evaluated during the same visit as photodynamic therapy. This will require a secondary diagnosis on the claim related to the E/M visit and the appropriate modifier.
Dermabrasion may be covered by some insurance companies as third- or fourth-line treatment for keloids, acne or scarring if patients have demonstrated at least 6 months of failing first- and second-line treatments (Table 6). The provider should obtain prior authorization for this procedure prior to submitting a claim.
In rare instances, chemical peels may be covered by insurance companies for actinic damage or other medical reasons (Table 7). Acne surgery is defined as marsupialization, opening or removal of multiple milia, comedones, cysts, pustules and is associated with CPT code 10040. Sclerotherapy sometimes can be reimbursed procedures if varicosities are associated with pain and if patients have failed more conservative measures (Table 8).
Most of the CPT codes for nail procedures listed in Table 9 would be more commonly used by podiatrists or orthopedic surgeons, but dermatologists sometimes perform procedures on the nail unit.
The next article in this series will discuss E/M and CPT modifiers needed for proper billing and reimbursement.
Dr. Strowd is assistant professor of dermatology at Wake Forest School of Medicine in Winston-Salem, NC.
Disclosure: The author reports no relevant financial relationships.












