 Actinomycosis is a chronic, granulomatous soft tissue invasion and inflammation accompanied by the formation of external sinus tracts that typically discharge diagnostic sulfur granules.1 Caused by the branching, gram-positive, non-acid fast, anaerobic organism Actinomyces, it was first identified in humans in 1878 by James Israel.1 In 1891, it was first successfully cultured by Wolff and Israel.1,2 Although several species including A. naeslundii, A. viscosus and A. odontolyticus have been recognized as etiologies, the most common causative organism is A. israeili.3 Non-virulent, endogenous, commensal residents of the gastrointestinal tract, oropharyncx and female genitalia, these organisms require penetration of mucosal barriers to initiate infection.4 Thus, cutaneous involvement is often secondary to local trauma, disruption of microbial flora or dissemination from visceral sites. Primary cutaneous involvement is considered rare.3 Infection can spread extensively, causing significant morbidity, so a high index of suspicion is required for recognition and treatment.
Actinomycosis is a chronic, granulomatous soft tissue invasion and inflammation accompanied by the formation of external sinus tracts that typically discharge diagnostic sulfur granules.1 Caused by the branching, gram-positive, non-acid fast, anaerobic organism Actinomyces, it was first identified in humans in 1878 by James Israel.1 In 1891, it was first successfully cultured by Wolff and Israel.1,2 Although several species including A. naeslundii, A. viscosus and A. odontolyticus have been recognized as etiologies, the most common causative organism is A. israeili.3 Non-virulent, endogenous, commensal residents of the gastrointestinal tract, oropharyncx and female genitalia, these organisms require penetration of mucosal barriers to initiate infection.4 Thus, cutaneous involvement is often secondary to local trauma, disruption of microbial flora or dissemination from visceral sites. Primary cutaneous involvement is considered rare.3 Infection can spread extensively, causing significant morbidity, so a high index of suspicion is required for recognition and treatment.
Epidemiology and pathogenesis
Actinomycosis is an inhabitant of the normal oral, gastrointestinal and female reproductive flora. Therefore, the orocervicofacial, thoracic and abdomenopelvic areas are those most typically affected.4 Unlike several other fungi that cause cutaneous involvement, it is not found in external environmental reservoirs such as soil or straw.5 It occurs worldwide, but has a higher incidence in farm workers of rural tropical regions.3 Those with lower socioeconomic status and poor dental hygiene are more likely to become infected, and statistically men are more susceptible than women by 3:1.4
In order to initiate infection, this normally nonvirulent organism requires a portal of entry beyond mucosal barriers, an anaerobic or microaerophillic environment and/or an immunosuppressed host. Penetration is often accomplished via localized tissue injury whether it is through carious teeth, gum disease, surgery involving one of the endogenous sites, human bites, intramuscular injections, puncture wounds or compound fractures.3-5 The anaerobic organism proliferates upon implantation in deep tissues where oxygen is scarce.4 A mixed bacterial infection allows for further migration by destroying over-vascularized regions leading to devitalized tissues with decreased oxygen supply.4,6 Although actinomycosis has certainly been identified in those with intact immunity, immunosuppressed individuals are more susceptible to infection. Thus, those with HIV infection, diabetes mellitus, acute lymphocytic leukemia, undergoing chemotherapy or taking corticosteroids are of increased risk.5 The proliferation of Actinomyces proceeds in a progressive, insidious manner without consideration for tissue planes, and may disseminate via hematogenous spread to bones and/or the central nervous system.6
Clinical Presentation
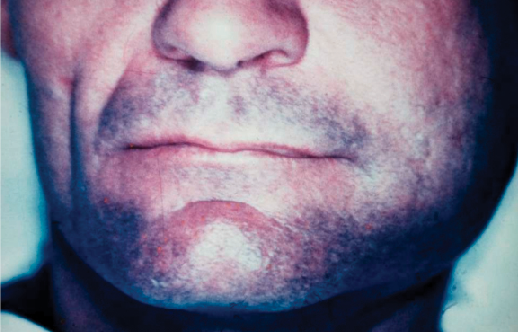
Figure 1. Actinomycosis of left jaw with subcutaneous cellulitis.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
Cutaneous involvement manifests as an intense suppurative and granulomatous inflammation that first may present as a nodular lesion, sometimes with surrounding cellulitis (Figure 1). The infection often progress so that nodules evolve into abscesses and sinus tracts (Figure 2). The most common clinical forms of actinomycosis is cervicofacial, producing the characteristic “lumpy jaw” from which “sulfur granules” are typically discharged.4 Less commonly, thoracic, abdominal or pelvic actinomycosis may occur. Regardless of the location of distribution, the classic clinical picture involves purulent foci with a dense, fibrotic periphery that penetrate into adjacent structures with the development of fistulae and sinus tracts (Figure 3). These sinus tracts drain and may spontaneously open and close.5

Figure 2. Cervicofacial actinomycosis with abscess and draining sinus tract.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology

Figure 3. Cervicofacial actinomycosis with fistulization.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
Histopathology
A biopsy of a secondary abscess reveals a central area of histiocytic and polymorphonuclear neutrophilic infiltration containing lobulated, granular colonies with surrounding granulation tissue (Figure 4). Diagnostic basophilic sulfur granules range from 0.1-2.0 mm in size with peripherally radiating, elongated eosinophilic clubs (Figure 5). This is referred to as the Splendore-Hoeppli phenomenon.5 Actinomyces appear as branching, non-acid fast, gram-positive filaments solidified with fragments of tissue exudates, similar to a grain of sulfur.1 Although only positive in less than a quarter of cases, culture of organisms provides a definitive diagnosis.5 At 37°C, with an enriched and anaerobic media, successful culture shows glossy, white nodular colonies.3
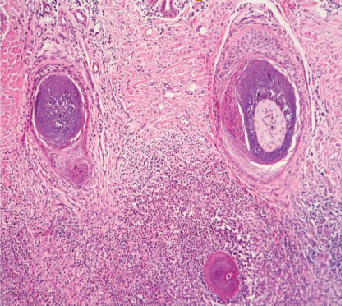
Figure 4. Histology showing actinomycoses sulfur granules with surrounding inflammation.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology

Figure 5. Basophilic sulfur granules with surrounding eosinophilic filaments—the Splendore-Hoeppli phenomenon.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
Differential Diagnosis
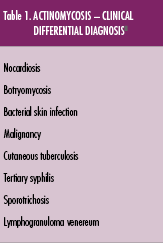
Because cutaneous actinomycosis is so rare, a high degree of clinical suspicion and histopathological evaluation is required to differentiate the illness from other mimickers. It may be confused with other chronic inflammatory skin diseases such as malignancy, cutaneous tuberculosis, tertiary syphilis, sporotrichosis, lymphogranuloma venereum, nocardiosis and botryomycosis (Table 1).3
Histologically, the gram-positive, non-acid-fast branching granules of actinomycoses are distinguishable from the granules of nocardiosis that are gram-positive and partially acid-fast positive. Botryomycosis granules consist of nonfilamentous cocci or bacilli that can be gram-positive or gram-negative.2,5
Diagnostic Tests
Biopsy of suspicious skin lesions and the histological demonstration of sulfur granules are necessary to make a correct diagnosis. Culture of the organism is the gold standard for identification. Organisms appear as glossy, white colonies on enriched, anaerobic culture media within 4 days.1,3 The granules of Actinomyces are Grocott silver, gram-positive, and periodicacid-Schiff stain positive, while Ziehl-Neelsen stain negative.7 Other serologic tests may be used to further narrow the differential diagnosis. For example, Mantoux and Quantiferon Gold test may be used to rule out cutaneous tuberculosis.8
Treatment
In general, the prognosis of cutaneous actinomycosis is a favorable one.2 However, the high success rate of treatment is dependent upon timely recognition and proper management. This involves a thorough history and physical examination to allow for adequate evaluation of the infection’s severity and the patient’s risk factors that may predispose to disease acquisition and/or progression. Depending on the severity, surgical excision or debridement may be indicated. Long-term, high-dose penicillin is the mainstay of actinomycosis treatment to completely eliminate the organism and prevent recurrence.1-3,5,7 Nevertheless, dosage strengths, duration and modalities are variable as there is, as of yet, no professional society treatment guideline statement for actinomycosis.3,5 Alternative antibiotics include tetracycline-class drugs, imipenem, chloramphenicol, macrolides, clindamycin, ceftriaxone and trimethoprim/sulfamethoxazole. Used as monotherapy, the efficaciousness of these remains debatable, but has been quite promising when used in combination with penicillins.1,5 There has also been some reported success using hyperbaric oxygen.2,5
Key Points
• Actinomycosis is a suppurative, cellulitic, granulomatous soft tissue infection most commonly caused by the endogenous, gram-positive, branching organism A. israeili.
• The typical clinical presentation consists of a central abscess with fistualization and sinus tracts that typically discharge sulfur granules.
• Histological examination reveals basophilic sulfur granules with an eosinophilic periphery, along with granulomatous inflammatory infiltrate.
• Culture, staining and direct microscopic evaluation are diagnostic techniques utilized to provide a definitive diagnosis.
• High-dose, long-term penicillins are the treatments of choice, after surgical excision if it is indicated. Other antibiotics and/or hyperbaric oxygen may be used alternatively or in conjunction with penicillins.
Ms. Snyder, MS, is with the Center for Dermatology Research, and the departments of Dermatology at Wake Forest University School of Medicine in Winston-Salem, NC.
Mr. Al-Dabagh is a 4th year medical student at Case Western Reserve University School of Medicine in Cleveland, OH.
Dr. Feldman is with the Center for Dermatology Research and the Departments of Dermatology, Pathology and Public Health Sciences at Wake Forest University School of Medicine in Winston-Salem, NC.
Disclosures: The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories, L.P. Dr. Feldman is a consultant and speaker for Galderma, Stiefel/GlaxoSmithKline, Abbott Labs, Warner Chilcott, Janssen, Amgen, Photomedex, Genentech, BiogenIdec and Bristol Myers Squibb. Dr. Feldman has received grants from Galderma, Astellas, Abbott Labs, Warner Chilcott, Janssen, Amgen, Photomedex, Genentech, BiogenIdec, Coria/Valeant, Pharmaderm, Ortho Pharmaceuticals, Aventis Pharmaceuticals, Roche Dermatology, 3M, Bristol-Myers Squibb, Stiefel/GlaxoSmithKline, Novartis, Medicis, Leo, HanAll Pharmaceuticals, Celgene, Basilea and Anacor and has received stock options from Photomedex. He is owner of www.DrScore.com and a founder of Causa Research.
Ms. Snyder and Mr. Al-Dabagh have no conflicts to disclose.
References
1. Patil D, Siddaramappa B, Manjunathswamy BS, et al. Primary cutaneous actinomycosis. Int J Dermatol. 2008;47(12):1271-1273.
2. Al-Niaimi F, Patel A, Blessing K, Fox R, Burden AD. Cutaneous actinomycosis presenting as chronic mastitis. Clin Exp Dermatol. 2010; 35(2):149-151.
3. Romano C, Massai L, De Aloe G, Schurfeld K, Miracco C. A case of primary cutaneous actinomycosis. Acta Derm Venereol. 2002;82(2):144-145.
4. Metgud SC. Primary cutaneous actinomycosis: a rare soft tissue infection. Indian J Med Microbiol. 2008;26(2):184-186.
5. Cocuroccia B, Gubinelli E, Fazio M, Girolomoni G. Primary cutaneous actinomycosis of the forehead. J Eur Acad Dermatol Venereol. 2003;17(3):331-333.
6. Magdeburg R, Grobholz R, Dornschneider G, Post S, Bussen D. Perianal abscess caused by Actinomyces: report of a case. Tech Coloproctol. 2008;12(4):347-349.
7. Ghaninejad H, Hasibi M, Moslehi H, Hashemi P, Rashidi A. Primary cutaneous actinomycosis of the elbow with an exceptionally long incubation period. Int J Dermatol. 2008;47(3):304-305.
8. Tomb RR, Stephan F, Haddad A, Choucairt J. Cutaneous granular bacteriosis, a rarely diagnosed infection of the head and the neck. Clin Exp Dermatol. 2009;34(8):887-889.
 Actinomycosis is a chronic, granulomatous soft tissue invasion and inflammation accompanied by the formation of external sinus tracts that typically discharge diagnostic sulfur granules.1 Caused by the branching, gram-positive, non-acid fast, anaerobic organism Actinomyces, it was first identified in humans in 1878 by James Israel.1 In 1891, it was first successfully cultured by Wolff and Israel.1,2 Although several species including A. naeslundii, A. viscosus and A. odontolyticus have been recognized as etiologies, the most common causative organism is A. israeili.3 Non-virulent, endogenous, commensal residents of the gastrointestinal tract, oropharyncx and female genitalia, these organisms require penetration of mucosal barriers to initiate infection.4 Thus, cutaneous involvement is often secondary to local trauma, disruption of microbial flora or dissemination from visceral sites. Primary cutaneous involvement is considered rare.3 Infection can spread extensively, causing significant morbidity, so a high index of suspicion is required for recognition and treatment.
Actinomycosis is a chronic, granulomatous soft tissue invasion and inflammation accompanied by the formation of external sinus tracts that typically discharge diagnostic sulfur granules.1 Caused by the branching, gram-positive, non-acid fast, anaerobic organism Actinomyces, it was first identified in humans in 1878 by James Israel.1 In 1891, it was first successfully cultured by Wolff and Israel.1,2 Although several species including A. naeslundii, A. viscosus and A. odontolyticus have been recognized as etiologies, the most common causative organism is A. israeili.3 Non-virulent, endogenous, commensal residents of the gastrointestinal tract, oropharyncx and female genitalia, these organisms require penetration of mucosal barriers to initiate infection.4 Thus, cutaneous involvement is often secondary to local trauma, disruption of microbial flora or dissemination from visceral sites. Primary cutaneous involvement is considered rare.3 Infection can spread extensively, causing significant morbidity, so a high index of suspicion is required for recognition and treatment.
Epidemiology and pathogenesis
Actinomycosis is an inhabitant of the normal oral, gastrointestinal and female reproductive flora. Therefore, the orocervicofacial, thoracic and abdomenopelvic areas are those most typically affected.4 Unlike several other fungi that cause cutaneous involvement, it is not found in external environmental reservoirs such as soil or straw.5 It occurs worldwide, but has a higher incidence in farm workers of rural tropical regions.3 Those with lower socioeconomic status and poor dental hygiene are more likely to become infected, and statistically men are more susceptible than women by 3:1.4
In order to initiate infection, this normally nonvirulent organism requires a portal of entry beyond mucosal barriers, an anaerobic or microaerophillic environment and/or an immunosuppressed host. Penetration is often accomplished via localized tissue injury whether it is through carious teeth, gum disease, surgery involving one of the endogenous sites, human bites, intramuscular injections, puncture wounds or compound fractures.3-5 The anaerobic organism proliferates upon implantation in deep tissues where oxygen is scarce.4 A mixed bacterial infection allows for further migration by destroying over-vascularized regions leading to devitalized tissues with decreased oxygen supply.4,6 Although actinomycosis has certainly been identified in those with intact immunity, immunosuppressed individuals are more susceptible to infection. Thus, those with HIV infection, diabetes mellitus, acute lymphocytic leukemia, undergoing chemotherapy or taking corticosteroids are of increased risk.5 The proliferation of Actinomyces proceeds in a progressive, insidious manner without consideration for tissue planes, and may disseminate via hematogenous spread to bones and/or the central nervous system.6
Clinical Presentation

Figure 1. Actinomycosis of left jaw with subcutaneous cellulitis.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
Cutaneous involvement manifests as an intense suppurative and granulomatous inflammation that first may present as a nodular lesion, sometimes with surrounding cellulitis (Figure 1). The infection often progress so that nodules evolve into abscesses and sinus tracts (Figure 2). The most common clinical forms of actinomycosis is cervicofacial, producing the characteristic “lumpy jaw” from which “sulfur granules” are typically discharged.4 Less commonly, thoracic, abdominal or pelvic actinomycosis may occur. Regardless of the location of distribution, the classic clinical picture involves purulent foci with a dense, fibrotic periphery that penetrate into adjacent structures with the development of fistulae and sinus tracts (Figure 3). These sinus tracts drain and may spontaneously open and close.5

Figure 2. Cervicofacial actinomycosis with abscess and draining sinus tract.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology

Figure 3. Cervicofacial actinomycosis with fistulization.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
Histopathology
A biopsy of a secondary abscess reveals a central area of histiocytic and polymorphonuclear neutrophilic infiltration containing lobulated, granular colonies with surrounding granulation tissue (Figure 4). Diagnostic basophilic sulfur granules range from 0.1-2.0 mm in size with peripherally radiating, elongated eosinophilic clubs (Figure 5). This is referred to as the Splendore-Hoeppli phenomenon.5 Actinomyces appear as branching, non-acid fast, gram-positive filaments solidified with fragments of tissue exudates, similar to a grain of sulfur.1 Although only positive in less than a quarter of cases, culture of organisms provides a definitive diagnosis.5 At 37°C, with an enriched and anaerobic media, successful culture shows glossy, white nodular colonies.3

Figure 4. Histology showing actinomycoses sulfur granules with surrounding inflammation.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology

Figure 5. Basophilic sulfur granules with surrounding eosinophilic filaments—the Splendore-Hoeppli phenomenon.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
Differential Diagnosis
Because cutaneous actinomycosis is so rare, a high degree of clinical suspicion and histopathological evaluation is required to differentiate the illness from other mimickers. It may be confused with other chronic inflammatory skin diseases such as malignancy, cutaneous tuberculosis, tertiary syphilis, sporotrichosis, lymphogranuloma venereum, nocardiosis and botryomycosis (Table 1).3

Histologically, the gram-positive, non-acid-fast branching granules of actinomycoses are distinguishable from the granules of nocardiosis that are gram-positive and partially acid-fast positive. Botryomycosis granules consist of nonfilamentous cocci or bacilli that can be gram-positive or gram-negative.2,5
Diagnostic Tests
Biopsy of suspicious skin lesions and the histological demonstration of sulfur granules are necessary to make a correct diagnosis. Culture of the organism is the gold standard for identification. Organisms appear as glossy, white colonies on enriched, anaerobic culture media within 4 days.1,3 The granules of Actinomyces are Grocott silver, gram-positive, and periodicacid-Schiff stain positive, while Ziehl-Neelsen stain negative.7 Other serologic tests may be used to further narrow the differential diagnosis. For example, Mantoux and Quantiferon Gold test may be used to rule out cutaneous tuberculosis.8
Treatment
In general, the prognosis of cutaneous actinomycosis is a favorable one.2 However, the high success rate of treatment is dependent upon timely recognition and proper management. This involves a thorough history and physical examination to allow for adequate evaluation of the infection’s severity and the patient’s risk factors that may predispose to disease acquisition and/or progression. Depending on the severity, surgical excision or debridement may be indicated. Long-term, high-dose penicillin is the mainstay of actinomycosis treatment to completely eliminate the organism and prevent recurrence.1-3,5,7 Nevertheless, dosage strengths, duration and modalities are variable as there is, as of yet, no professional society treatment guideline statement for actinomycosis.3,5 Alternative antibiotics include tetracycline-class drugs, imipenem, chloramphenicol, macrolides, clindamycin, ceftriaxone and trimethoprim/sulfamethoxazole. Used as monotherapy, the efficaciousness of these remains debatable, but has been quite promising when used in combination with penicillins.1,5 There has also been some reported success using hyperbaric oxygen.2,5
Key Points
• Actinomycosis is a suppurative, cellulitic, granulomatous soft tissue infection most commonly caused by the endogenous, gram-positive, branching organism A. israeili.
• The typical clinical presentation consists of a central abscess with fistualization and sinus tracts that typically discharge sulfur granules.
• Histological examination reveals basophilic sulfur granules with an eosinophilic periphery, along with granulomatous inflammatory infiltrate.
• Culture, staining and direct microscopic evaluation are diagnostic techniques utilized to provide a definitive diagnosis.
• High-dose, long-term penicillins are the treatments of choice, after surgical excision if it is indicated. Other antibiotics and/or hyperbaric oxygen may be used alternatively or in conjunction with penicillins.
Ms. Snyder, MS, is with the Center for Dermatology Research, and the departments of Dermatology at Wake Forest University School of Medicine in Winston-Salem, NC.
Mr. Al-Dabagh is a 4th year medical student at Case Western Reserve University School of Medicine in Cleveland, OH.
Dr. Feldman is with the Center for Dermatology Research and the Departments of Dermatology, Pathology and Public Health Sciences at Wake Forest University School of Medicine in Winston-Salem, NC.
Disclosures: The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories, L.P. Dr. Feldman is a consultant and speaker for Galderma, Stiefel/GlaxoSmithKline, Abbott Labs, Warner Chilcott, Janssen, Amgen, Photomedex, Genentech, BiogenIdec and Bristol Myers Squibb. Dr. Feldman has received grants from Galderma, Astellas, Abbott Labs, Warner Chilcott, Janssen, Amgen, Photomedex, Genentech, BiogenIdec, Coria/Valeant, Pharmaderm, Ortho Pharmaceuticals, Aventis Pharmaceuticals, Roche Dermatology, 3M, Bristol-Myers Squibb, Stiefel/GlaxoSmithKline, Novartis, Medicis, Leo, HanAll Pharmaceuticals, Celgene, Basilea and Anacor and has received stock options from Photomedex. He is owner of www.DrScore.com and a founder of Causa Research.
Ms. Snyder and Mr. Al-Dabagh have no conflicts to disclose.
References
1. Patil D, Siddaramappa B, Manjunathswamy BS, et al. Primary cutaneous actinomycosis. Int J Dermatol. 2008;47(12):1271-1273.
2. Al-Niaimi F, Patel A, Blessing K, Fox R, Burden AD. Cutaneous actinomycosis presenting as chronic mastitis. Clin Exp Dermatol. 2010; 35(2):149-151.
3. Romano C, Massai L, De Aloe G, Schurfeld K, Miracco C. A case of primary cutaneous actinomycosis. Acta Derm Venereol. 2002;82(2):144-145.
4. Metgud SC. Primary cutaneous actinomycosis: a rare soft tissue infection. Indian J Med Microbiol. 2008;26(2):184-186.
5. Cocuroccia B, Gubinelli E, Fazio M, Girolomoni G. Primary cutaneous actinomycosis of the forehead. J Eur Acad Dermatol Venereol. 2003;17(3):331-333.
6. Magdeburg R, Grobholz R, Dornschneider G, Post S, Bussen D. Perianal abscess caused by Actinomyces: report of a case. Tech Coloproctol. 2008;12(4):347-349.
7. Ghaninejad H, Hasibi M, Moslehi H, Hashemi P, Rashidi A. Primary cutaneous actinomycosis of the elbow with an exceptionally long incubation period. Int J Dermatol. 2008;47(3):304-305.
8. Tomb RR, Stephan F, Haddad A, Choucairt J. Cutaneous granular bacteriosis, a rarely diagnosed infection of the head and the neck. Clin Exp Dermatol. 2009;34(8):887-889.
Actinomycosis is a chronic, granulomatous soft tissue invasion and inflammation accompanied by the formation of external sinus tracts that typically discharge diagnostic sulfur granules.1 Caused by the branching, gram-positive, non-acid fast, anaerobic organism Actinomyces, it was first identified in humans in 1878 by James Israel.1 In 1891, it was first successfully cultured by Wolff and Israel.1,2 Although several species including A. naeslundii, A. viscosus and A. odontolyticus have been recognized as etiologies, the most common causative organism is A. israeili.3 Non-virulent, endogenous, commensal residents of the gastrointestinal tract, oropharyncx and female genitalia, these organisms require penetration of mucosal barriers to initiate infection.4 Thus, cutaneous involvement is often secondary to local trauma, disruption of microbial flora or dissemination from visceral sites. Primary cutaneous involvement is considered rare.3 Infection can spread extensively, causing significant morbidity, so a high index of suspicion is required for recognition and treatment.
Epidemiology and pathogenesis
Actinomycosis is an inhabitant of the normal oral, gastrointestinal and female reproductive flora. Therefore, the orocervicofacial, thoracic and abdomenopelvic areas are those most typically affected.4 Unlike several other fungi that cause cutaneous involvement, it is not found in external environmental reservoirs such as soil or straw.5 It occurs worldwide, but has a higher incidence in farm workers of rural tropical regions.3 Those with lower socioeconomic status and poor dental hygiene are more likely to become infected, and statistically men are more susceptible than women by 3:1.4
In order to initiate infection, this normally nonvirulent organism requires a portal of entry beyond mucosal barriers, an anaerobic or microaerophillic environment and/or an immunosuppressed host. Penetration is often accomplished via localized tissue injury whether it is through carious teeth, gum disease, surgery involving one of the endogenous sites, human bites, intramuscular injections, puncture wounds or compound fractures.3-5 The anaerobic organism proliferates upon implantation in deep tissues where oxygen is scarce.4 A mixed bacterial infection allows for further migration by destroying over-vascularized regions leading to devitalized tissues with decreased oxygen supply.4,6 Although actinomycosis has certainly been identified in those with intact immunity, immunosuppressed individuals are more susceptible to infection. Thus, those with HIV infection, diabetes mellitus, acute lymphocytic leukemia, undergoing chemotherapy or taking corticosteroids are of increased risk.5 The proliferation of Actinomyces proceeds in a progressive, insidious manner without consideration for tissue planes, and may disseminate via hematogenous spread to bones and/or the central nervous system.6
Clinical Presentation
Figure 1. Actinomycosis of left jaw with subcutaneous cellulitis.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
Cutaneous involvement manifests as an intense suppurative and granulomatous inflammation that first may present as a nodular lesion, sometimes with surrounding cellulitis (Figure 1). The infection often progress so that nodules evolve into abscesses and sinus tracts (Figure 2). The most common clinical forms of actinomycosis is cervicofacial, producing the characteristic “lumpy jaw” from which “sulfur granules” are typically discharged.4 Less commonly, thoracic, abdominal or pelvic actinomycosis may occur. Regardless of the location of distribution, the classic clinical picture involves purulent foci with a dense, fibrotic periphery that penetrate into adjacent structures with the development of fistulae and sinus tracts (Figure 3). These sinus tracts drain and may spontaneously open and close.5
Figure 2. Cervicofacial actinomycosis with abscess and draining sinus tract.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
Figure 3. Cervicofacial actinomycosis with fistulization.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
Histopathology
A biopsy of a secondary abscess reveals a central area of histiocytic and polymorphonuclear neutrophilic infiltration containing lobulated, granular colonies with surrounding granulation tissue (Figure 4). Diagnostic basophilic sulfur granules range from 0.1-2.0 mm in size with peripherally radiating, elongated eosinophilic clubs (Figure 5). This is referred to as the Splendore-Hoeppli phenomenon.5 Actinomyces appear as branching, non-acid fast, gram-positive filaments solidified with fragments of tissue exudates, similar to a grain of sulfur.1 Although only positive in less than a quarter of cases, culture of organisms provides a definitive diagnosis.5 At 37°C, with an enriched and anaerobic media, successful culture shows glossy, white nodular colonies.3
Figure 4. Histology showing actinomycoses sulfur granules with surrounding inflammation.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
Figure 5. Basophilic sulfur granules with surrounding eosinophilic filaments—the Splendore-Hoeppli phenomenon.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
Differential Diagnosis
Because cutaneous actinomycosis is so rare, a high degree of clinical suspicion and histopathological evaluation is required to differentiate the illness from other mimickers. It may be confused with other chronic inflammatory skin diseases such as malignancy, cutaneous tuberculosis, tertiary syphilis, sporotrichosis, lymphogranuloma venereum, nocardiosis and botryomycosis (Table 1).3
Histologically, the gram-positive, non-acid-fast branching granules of actinomycoses are distinguishable from the granules of nocardiosis that are gram-positive and partially acid-fast positive. Botryomycosis granules consist of nonfilamentous cocci or bacilli that can be gram-positive or gram-negative.2,5
Diagnostic Tests
Biopsy of suspicious skin lesions and the histological demonstration of sulfur granules are necessary to make a correct diagnosis. Culture of the organism is the gold standard for identification. Organisms appear as glossy, white colonies on enriched, anaerobic culture media within 4 days.1,3 The granules of Actinomyces are Grocott silver, gram-positive, and periodicacid-Schiff stain positive, while Ziehl-Neelsen stain negative.7 Other serologic tests may be used to further narrow the differential diagnosis. For example, Mantoux and Quantiferon Gold test may be used to rule out cutaneous tuberculosis.8
Treatment
In general, the prognosis of cutaneous actinomycosis is a favorable one.2 However, the high success rate of treatment is dependent upon timely recognition and proper management. This involves a thorough history and physical examination to allow for adequate evaluation of the infection’s severity and the patient’s risk factors that may predispose to disease acquisition and/or progression. Depending on the severity, surgical excision or debridement may be indicated. Long-term, high-dose penicillin is the mainstay of actinomycosis treatment to completely eliminate the organism and prevent recurrence.1-3,5,7 Nevertheless, dosage strengths, duration and modalities are variable as there is, as of yet, no professional society treatment guideline statement for actinomycosis.3,5 Alternative antibiotics include tetracycline-class drugs, imipenem, chloramphenicol, macrolides, clindamycin, ceftriaxone and trimethoprim/sulfamethoxazole. Used as monotherapy, the efficaciousness of these remains debatable, but has been quite promising when used in combination with penicillins.1,5 There has also been some reported success using hyperbaric oxygen.2,5
Key Points
• Actinomycosis is a suppurative, cellulitic, granulomatous soft tissue infection most commonly caused by the endogenous, gram-positive, branching organism A. israeili.
• The typical clinical presentation consists of a central abscess with fistualization and sinus tracts that typically discharge sulfur granules.
• Histological examination reveals basophilic sulfur granules with an eosinophilic periphery, along with granulomatous inflammatory infiltrate.
• Culture, staining and direct microscopic evaluation are diagnostic techniques utilized to provide a definitive diagnosis.
• High-dose, long-term penicillins are the treatments of choice, after surgical excision if it is indicated. Other antibiotics and/or hyperbaric oxygen may be used alternatively or in conjunction with penicillins.
Ms. Snyder, MS, is with the Center for Dermatology Research, and the departments of Dermatology at Wake Forest University School of Medicine in Winston-Salem, NC.
Mr. Al-Dabagh is a 4th year medical student at Case Western Reserve University School of Medicine in Cleveland, OH.
Dr. Feldman is with the Center for Dermatology Research and the Departments of Dermatology, Pathology and Public Health Sciences at Wake Forest University School of Medicine in Winston-Salem, NC.
Disclosures: The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories, L.P. Dr. Feldman is a consultant and speaker for Galderma, Stiefel/GlaxoSmithKline, Abbott Labs, Warner Chilcott, Janssen, Amgen, Photomedex, Genentech, BiogenIdec and Bristol Myers Squibb. Dr. Feldman has received grants from Galderma, Astellas, Abbott Labs, Warner Chilcott, Janssen, Amgen, Photomedex, Genentech, BiogenIdec, Coria/Valeant, Pharmaderm, Ortho Pharmaceuticals, Aventis Pharmaceuticals, Roche Dermatology, 3M, Bristol-Myers Squibb, Stiefel/GlaxoSmithKline, Novartis, Medicis, Leo, HanAll Pharmaceuticals, Celgene, Basilea and Anacor and has received stock options from Photomedex. He is owner of www.DrScore.com and a founder of Causa Research.
Ms. Snyder and Mr. Al-Dabagh have no conflicts to disclose.
References
1. Patil D, Siddaramappa B, Manjunathswamy BS, et al. Primary cutaneous actinomycosis. Int J Dermatol. 2008;47(12):1271-1273.
2. Al-Niaimi F, Patel A, Blessing K, Fox R, Burden AD. Cutaneous actinomycosis presenting as chronic mastitis. Clin Exp Dermatol. 2010; 35(2):149-151.
3. Romano C, Massai L, De Aloe G, Schurfeld K, Miracco C. A case of primary cutaneous actinomycosis. Acta Derm Venereol. 2002;82(2):144-145.
4. Metgud SC. Primary cutaneous actinomycosis: a rare soft tissue infection. Indian J Med Microbiol. 2008;26(2):184-186.
5. Cocuroccia B, Gubinelli E, Fazio M, Girolomoni G. Primary cutaneous actinomycosis of the forehead. J Eur Acad Dermatol Venereol. 2003;17(3):331-333.
6. Magdeburg R, Grobholz R, Dornschneider G, Post S, Bussen D. Perianal abscess caused by Actinomyces: report of a case. Tech Coloproctol. 2008;12(4):347-349.
7. Ghaninejad H, Hasibi M, Moslehi H, Hashemi P, Rashidi A. Primary cutaneous actinomycosis of the elbow with an exceptionally long incubation period. Int J Dermatol. 2008;47(3):304-305.
8. Tomb RR, Stephan F, Haddad A, Choucairt J. Cutaneous granular bacteriosis, a rarely diagnosed infection of the head and the neck. Clin Exp Dermatol. 2009;34(8):887-889.











