While sclerotherapy has long been considered the gold standard first-line treatment for small leg veins, with the new longer-pulsed 1064 nm Nd:Yag lasers and improved skill with their use, many clinicians will consider laser earlier in the leg vein treatment algorithm.
While sclerotherapy has long been considered the gold standard first-line treatment for small leg veins, with the new longer-pulsed 1064 nm Nd:Yag lasers and improved skill with their use, many clinicians will consider laser earlier in the leg vein treatment algorithm.
The Nd:Yag laser is the current laser of choice for treating leg veins. A recent comparison of treatment of lower extremity telangiectasias in 57 women with foam 0.5% polidocanol sclerotherapy (Asclera, Merz Aesthetics, Inc.) versus Nd:Yag laser found that both treatments result in >70% clearance. The only significant difference was in pain perception, which was greater with laser.1 Patients were treated in 2 sessions at 6-week intervals and anesthesia was not used. One leg was randomly assigned to treatment with laser, while the other received sclerotherapy. Investigators were blinded, and patients were evaluated at 6 months.1 Tips on anesthesia and patient comfort with laser leg vein treatment is discussed later in the article.
Choosing the Patient
Laser treatment of leg veins is most effective for small, superficial red or blue veins (<0.5 mm) and telangiectatic mats, any veins too small for the 32-gauge sclerotherapy needle and for needle phobic patients.2 Patients with numerous nodular varicose and spider veins tend to be poor candidates for laser leg vein treatment because of their high risk of harboring deeper venous reflux disease. These patients should receive further evaluation with ultrasound and possible treatment with endovenous laser ablation or radiofrequency laser ablation or ambulatory phlebectomy.

Prior to treatment, patients should be advised to avoid blood thinners, tanning, artificial tanners and sun exposure.
3 In addition, just as with sclerotherapy treatment, to reduce the risk of thrombosis patients should discontinue oral contraceptives prior to laser vein treatment.
4 When planning your patient’s leg vein treatment, whether it is with laser or not, it is important to identify risk factors for failed treatment. See Table for a list of poor candidates for laser leg vein treatment.
Choosing the Device: 1064 nm Nd:Yag
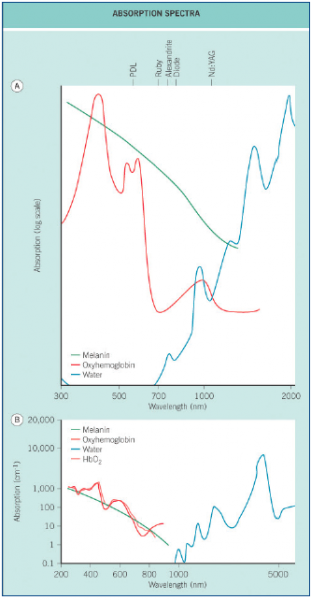
The 1064 nm Nd:Yag laser is the leading laser for small leg vein treatment. The short pulse duration of the original pulsed dye lasers failed to coagulate the deeper thicker veins as well as the Nd:Yag. In addition, the shorter pulse pulsed dye lasers produced a significant amount of purpura at the site of treatment, sometimes leaving stripes, circles and honeycomb patterns depending on the size and location of the vessel. Even with the long pulsed dye laser, the melanin absorption competes too much with the hemoglobin absorption resulting in a significantly higher risk of post-inflammatory hyperpigmentation (PIH)4 (Figure 1).
Figure 1. Various Absorption rates (from Dermatology with permission from Elsevier).
It is crucial to provide adequate epidermal cooling when a pulsed dye laser is used to treat veins. The longer wavelength of 1064 nm allows for deeper, adequate skin penetration (3 mm) to the veins (Figure 2). The longer pulse duration allows for slower heating and coagulation of the vessel with less purpura and less damage to the surrounding skin. The Nd:Yag is unlikely to be absorbed by melanin, which lowers the risk of epidermal damage even in darker skin types.4
Figure 2. Depth of penetration by various lasers (from Dermatology with permission from Elsevier).2,8
While a larger spot size is preferred for improved penetrance and less scatter, this is most important for treating larger and deeper veins. With the 1064 nm Nd:Yag laser, it is critical to not stack pulses and accumulate too much heat or there is significant risk to overheating the surrounding tissues, resulting in blisters and scars. Effective and safe vessel coagulation can be achieved with pulses spaced 1 mm apart.4
In addition to the risk of stacking excessive heat and causing surrounding tissue damage, another disadvantage of the Nd:Yag laser compared to sclerotherapy with polidocanol is the pain felt by the patient. Topical (eg, betacaine, tetracaine, lidocaine mix) anesthesia and epidermal cooling with air or ice is routine in my practice when treating veins with the Nd:Yag.
After topical anesthesia cream application is complete (45- 90 minutes) and removed, I prefer to use an ice cube popsicle stick and hold it for 3 seconds prior to firing the laser. The endpoint of laser treatment is immediate blanching of the vein (not the skin) or cease of blood flow with no epidermal change. This can be verified with compression and release and watching for residual flow. If there is no blanching, but flow seems to have ceased, then treatment is usually adequate.
Technique
Because oxygenated blood is targeted best by 500 nm to 600 nm lasers and deoxygenated by 800 nm to 1,100 nm, one may think that it would be best to employ the 2 different wavelengths for a more thorough leg vein treatment. The versatility of the 1064 nm Nd:Yag has eliminated the need for treatment with the 2 lasers. By modifying the spot size and pulse duration depending on the color of vein, both red and blue can be treated effectively.4 For red and superficial veins, treat with a smaller spot size and shorter pulse duration and relatively higher fluence (2-3 mm, 15-20 ms and 250-300J/cm2 Cynergy laser, Cynosure).
For blue, deeper veins, treat with a larger spot size and longer pulse duration with a moderate fluence (4 mm, 50 ms and 200J/cm2 Cynergy laser, Cynosure). It is crucial to begin with 1 pulse and look for your endpoints (Figure 3).
Figures 3A-C. Before and after treatment with 1064 nm Nd:Yag Cynergy laser at 8 weeks.
Other Devices
The KTP laser is useful and very efficacious only for small, superficial telangiectasias in patients with non-tanned Fitzpatrick skin types I-III. Pulse stacking should be avoided as with the Yag laser.
A recent study looked at the 532 nm KTP (Excel V, Cutera) using a 5 mm spot, 13 to 15J/cm2 and 40 ms pulse duration in treating 79 sites on 25 women. Physicians assessing improvement were blinded and reported a median improvement of 2.5 (5-point scale) at 12 weeks with minimal discomfort.5 PIH was reported in 2% of treatment sites. In summary, the KTP is mainly limited by its absorption of melanin and consequent increased risk of PIH when compared to the 1064 nm Nd:Yag.
Long-pulsed alexandrite and diode lasers may also be used successfully to treat leg veins, though they will not penetrate as deep as the 1064 nm, and may absorb more melanin versus the Nd:Yag.4
A recent study compared the indocyanine green-augmented diode laser (810 nm) to the 1064 nm Nd:Yag in a prospective, randomized, controlled trial to treat small telangiectatic leg veins in 29 study participants.6 For the study, 2 blinded investigators evaluated the patients at 3 months. Both investigators’ and participants’ assessments found significantly better clearance at 3 months with the diode laser versus the Nd:Yag; however, the diode laser was rated more painful.
In summary, while the diode laser may be as effective as the Nd:Yag with small telangiectatic leg veins, it may be more painful, and is unlikely to penetrate deep enough compared to the Nd:Yag for some larger or deeper veins.
Intense pulse light (515 nm-1,200 nm) may be used because it permits target of both superficial and deeper vessels. However, it is not safe in darker skin types because of risk of melanin absorption and consequent blistering.
Treatment Pearls
When there are deeper reticular veins, it is not a good idea to limit your treatment to laser or begin your treatment with laser. Try to assess for deeper reticular varicose veins that may be connected to a superficial vein and treat that deeper reticular vein with sclerotherapy prior to attempting laser treatment of the smaller superficial vein. Larger reticular veins are best treated first with foam sclerotherapy and then remaining superficial veins can be treated with laser. Polidocanol was FDA approved in 2010 and carries the advantages of being less allergenic than sodium tetradecyl sulfate injection (Sotradecol, AngioDynamics) and many physicians report that patients experience less pain and a lower risk for skin ulceration than other sclerosants. Laser treatments may need to be repeated and should be spaced 8 weeks apart if treating some larger diameter veins. If only small superficial red veins were treated, then 4 weeks follow-up is usually adequate. Some veins may gradually resorb over many weeks. It is good to advise patients about this, so they do not have unrealistic expectations about immediate results.
Though some physicians have reported that no compression is needed after laser treatment, I prefer to recommend 3 weeks of compression when many veins are treated and if the patient tends to stand or sit a lot. For best results, combine sclerotherapy treatment with laser treatment in the same day, and apply compression immediately after completion while patient is still on the table.
A recent study compared treatment of spider leg veins less than 1.5 mm in skin type IV patients with polidocanol foam versus either Nd:Yag (low-fluence pulsed) laser alone or with polidocanol foam followed by Nd:Yag (low-fluence pulsed) laser.7 Efficacy of combination treatment proved safe and satisfactory in 96% of patients using low-fluence laser pulses with a total cumulative energy in the 3 cm venous segment; and the Nd:Yag laser was safe in these darker skin types.
Dr. Stolman, a board-certified dermatologist and dermatologic surgeon specializing in lasers and other skin treatment devices, is on the faculty at of the University of Utah School of Medicine, department of dermatology, in Salt Lake City, UT.
Disclosure: The author reports no relevant financial relationships.
References
1. Parlar B, Blazek C, Cazzaniga S, et al. Treatment of lower extremity telangiectasias in women by foam sclerotherapy vs. Nd:YAG laser: a prospective, comparative, randomized, open-label trial. J Eur Acad Dermatol Venereol. Published online ahead of print July 28, 2014.
2. Meesters AA, Pitassi LH, Campos V, Wokerstorfer A, Dierickx CC. Transcutaneous laser treatment of leg veins. Lasers Med Sci. 2014;29(2):481-492.
3. Hirsch RJ, Anderson RR. Principles of laser skin interactions. In: Bolognia JL, Jorizzo JL, Rapini RP, eds. Dermatology. Maryland Heights, MO: Mosby; 2003:2148. 4.Hsu TS. An overview of therapy for leg veins. In: Alam M, Nguyen TH, eds. Procedures in Cosmetic Dermatology Series: Treatment of Leg Veins. Philadelphia, PA: Elsevier; 2006:48-70.
5. Bogle MA, Sadick NS. Laser surgery. In: Alam M, Nguyen TH, eds. Procedures in Cosmetic Dermatology Series: Treatment of Leg Veins. Philadelphia, PA: Elsevier; 2006:48-70.
6. Bernstein EF, Noyaner-Turley A, Renton B. Treatment of spider veins of the lower extremity with a novel 532 nm KTP laser. Lasers Surg Med. 2014;46(2):81-88.
7. Klein A, Buschmann M, Babilas P, Landthaler M, Baumler W. Indocyanine green-augmented diode laser therapy vs. long-pulsed Nd:Yag (1064 nm) laser treatment of telangiectatic leg veins: a randomized controlled trial. Br J Dermatol. 2013;169(2):365-673.
8. Moreno-Morega J, Hernandez E, Royo J, et al. Optimal and safe treatment of spider leg veins measuring less than 1.5 mm on skin type IV patients, using repeated low-fluence Nd:YAG laser pulses after polidocanol injection. Lasers Med Sci. 2013;28(3):925-933.
 While sclerotherapy has long been considered the gold standard first-line treatment for small leg veins, with the new longer-pulsed 1064 nm Nd:Yag lasers and improved skill with their use, many clinicians will consider laser earlier in the leg vein treatment algorithm.
While sclerotherapy has long been considered the gold standard first-line treatment for small leg veins, with the new longer-pulsed 1064 nm Nd:Yag lasers and improved skill with their use, many clinicians will consider laser earlier in the leg vein treatment algorithm.
The Nd:Yag laser is the current laser of choice for treating leg veins. A recent comparison of treatment of lower extremity telangiectasias in 57 women with foam 0.5% polidocanol sclerotherapy (Asclera, Merz Aesthetics, Inc.) versus Nd:Yag laser found that both treatments result in >70% clearance. The only significant difference was in pain perception, which was greater with laser.1 Patients were treated in 2 sessions at 6-week intervals and anesthesia was not used. One leg was randomly assigned to treatment with laser, while the other received sclerotherapy. Investigators were blinded, and patients were evaluated at 6 months.1 Tips on anesthesia and patient comfort with laser leg vein treatment is discussed later in the article.
Choosing the Patient
Laser treatment of leg veins is most effective for small, superficial red or blue veins (<0.5 mm) and telangiectatic mats, any veins too small for the 32-gauge sclerotherapy needle and for needle phobic patients.2 Patients with numerous nodular varicose and spider veins tend to be poor candidates for laser leg vein treatment because of their high risk of harboring deeper venous reflux disease. These patients should receive further evaluation with ultrasound and possible treatment with endovenous laser ablation or radiofrequency laser ablation or ambulatory phlebectomy.

Prior to treatment, patients should be advised to avoid blood thinners, tanning, artificial tanners and sun exposure.
3 In addition, just as with sclerotherapy treatment, to reduce the risk of thrombosis patients should discontinue oral contraceptives prior to laser vein treatment.
4 When planning your patient’s leg vein treatment, whether it is with laser or not, it is important to identify risk factors for failed treatment. See Table for a list of poor candidates for laser leg vein treatment.
Choosing the Device: 1064 nm Nd:Yag
The 1064 nm Nd:Yag laser is the leading laser for small leg vein treatment. The short pulse duration of the original pulsed dye lasers failed to coagulate the deeper thicker veins as well as the Nd:Yag. In addition, the shorter pulse pulsed dye lasers produced a significant amount of purpura at the site of treatment, sometimes leaving stripes, circles and honeycomb patterns depending on the size and location of the vessel. Even with the long pulsed dye laser, the melanin absorption competes too much with the hemoglobin absorption resulting in a significantly higher risk of post-inflammatory hyperpigmentation (PIH)4 (Figure 1).
Figure 1. Various Absorption rates (from Dermatology with permission from Elsevier).
It is crucial to provide adequate epidermal cooling when a pulsed dye laser is used to treat veins. The longer wavelength of 1064 nm allows for deeper, adequate skin penetration (3 mm) to the veins (Figure 2). The longer pulse duration allows for slower heating and coagulation of the vessel with less purpura and less damage to the surrounding skin. The Nd:Yag is unlikely to be absorbed by melanin, which lowers the risk of epidermal damage even in darker skin types.4
Figure 2. Depth of penetration by various lasers (from Dermatology with permission from Elsevier).2,8
While a larger spot size is preferred for improved penetrance and less scatter, this is most important for treating larger and deeper veins. With the 1064 nm Nd:Yag laser, it is critical to not stack pulses and accumulate too much heat or there is significant risk to overheating the surrounding tissues, resulting in blisters and scars. Effective and safe vessel coagulation can be achieved with pulses spaced 1 mm apart.4
In addition to the risk of stacking excessive heat and causing surrounding tissue damage, another disadvantage of the Nd:Yag laser compared to sclerotherapy with polidocanol is the pain felt by the patient. Topical (eg, betacaine, tetracaine, lidocaine mix) anesthesia and epidermal cooling with air or ice is routine in my practice when treating veins with the Nd:Yag.
After topical anesthesia cream application is complete (45- 90 minutes) and removed, I prefer to use an ice cube popsicle stick and hold it for 3 seconds prior to firing the laser. The endpoint of laser treatment is immediate blanching of the vein (not the skin) or cease of blood flow with no epidermal change. This can be verified with compression and release and watching for residual flow. If there is no blanching, but flow seems to have ceased, then treatment is usually adequate.
Technique
Because oxygenated blood is targeted best by 500 nm to 600 nm lasers and deoxygenated by 800 nm to 1,100 nm, one may think that it would be best to employ the 2 different wavelengths for a more thorough leg vein treatment. The versatility of the 1064 nm Nd:Yag has eliminated the need for treatment with the 2 lasers. By modifying the spot size and pulse duration depending on the color of vein, both red and blue can be treated effectively.4 For red and superficial veins, treat with a smaller spot size and shorter pulse duration and relatively higher fluence (2-3 mm, 15-20 ms and 250-300J/cm2 Cynergy laser, Cynosure).
For blue, deeper veins, treat with a larger spot size and longer pulse duration with a moderate fluence (4 mm, 50 ms and 200J/cm2 Cynergy laser, Cynosure). It is crucial to begin with 1 pulse and look for your endpoints (Figure 3).
Figures 3A-C. Before and after treatment with 1064 nm Nd:Yag Cynergy laser at 8 weeks.
Other Devices
The KTP laser is useful and very efficacious only for small, superficial telangiectasias in patients with non-tanned Fitzpatrick skin types I-III. Pulse stacking should be avoided as with the Yag laser.
A recent study looked at the 532 nm KTP (Excel V, Cutera) using a 5 mm spot, 13 to 15J/cm2 and 40 ms pulse duration in treating 79 sites on 25 women. Physicians assessing improvement were blinded and reported a median improvement of 2.5 (5-point scale) at 12 weeks with minimal discomfort.5 PIH was reported in 2% of treatment sites. In summary, the KTP is mainly limited by its absorption of melanin and consequent increased risk of PIH when compared to the 1064 nm Nd:Yag.
Long-pulsed alexandrite and diode lasers may also be used successfully to treat leg veins, though they will not penetrate as deep as the 1064 nm, and may absorb more melanin versus the Nd:Yag.4
A recent study compared the indocyanine green-augmented diode laser (810 nm) to the 1064 nm Nd:Yag in a prospective, randomized, controlled trial to treat small telangiectatic leg veins in 29 study participants.6 For the study, 2 blinded investigators evaluated the patients at 3 months. Both investigators’ and participants’ assessments found significantly better clearance at 3 months with the diode laser versus the Nd:Yag; however, the diode laser was rated more painful.
In summary, while the diode laser may be as effective as the Nd:Yag with small telangiectatic leg veins, it may be more painful, and is unlikely to penetrate deep enough compared to the Nd:Yag for some larger or deeper veins.
Intense pulse light (515 nm-1,200 nm) may be used because it permits target of both superficial and deeper vessels. However, it is not safe in darker skin types because of risk of melanin absorption and consequent blistering.
Treatment Pearls
When there are deeper reticular veins, it is not a good idea to limit your treatment to laser or begin your treatment with laser. Try to assess for deeper reticular varicose veins that may be connected to a superficial vein and treat that deeper reticular vein with sclerotherapy prior to attempting laser treatment of the smaller superficial vein. Larger reticular veins are best treated first with foam sclerotherapy and then remaining superficial veins can be treated with laser. Polidocanol was FDA approved in 2010 and carries the advantages of being less allergenic than sodium tetradecyl sulfate injection (Sotradecol, AngioDynamics) and many physicians report that patients experience less pain and a lower risk for skin ulceration than other sclerosants. Laser treatments may need to be repeated and should be spaced 8 weeks apart if treating some larger diameter veins. If only small superficial red veins were treated, then 4 weeks follow-up is usually adequate. Some veins may gradually resorb over many weeks. It is good to advise patients about this, so they do not have unrealistic expectations about immediate results.
Though some physicians have reported that no compression is needed after laser treatment, I prefer to recommend 3 weeks of compression when many veins are treated and if the patient tends to stand or sit a lot. For best results, combine sclerotherapy treatment with laser treatment in the same day, and apply compression immediately after completion while patient is still on the table.
A recent study compared treatment of spider leg veins less than 1.5 mm in skin type IV patients with polidocanol foam versus either Nd:Yag (low-fluence pulsed) laser alone or with polidocanol foam followed by Nd:Yag (low-fluence pulsed) laser.7 Efficacy of combination treatment proved safe and satisfactory in 96% of patients using low-fluence laser pulses with a total cumulative energy in the 3 cm venous segment; and the Nd:Yag laser was safe in these darker skin types.
Dr. Stolman, a board-certified dermatologist and dermatologic surgeon specializing in lasers and other skin treatment devices, is on the faculty at of the University of Utah School of Medicine, department of dermatology, in Salt Lake City, UT.
Disclosure: The author reports no relevant financial relationships.
References
1. Parlar B, Blazek C, Cazzaniga S, et al. Treatment of lower extremity telangiectasias in women by foam sclerotherapy vs. Nd:YAG laser: a prospective, comparative, randomized, open-label trial. J Eur Acad Dermatol Venereol. Published online ahead of print July 28, 2014.
2. Meesters AA, Pitassi LH, Campos V, Wokerstorfer A, Dierickx CC. Transcutaneous laser treatment of leg veins. Lasers Med Sci. 2014;29(2):481-492.
3. Hirsch RJ, Anderson RR. Principles of laser skin interactions. In: Bolognia JL, Jorizzo JL, Rapini RP, eds. Dermatology. Maryland Heights, MO: Mosby; 2003:2148. 4.Hsu TS. An overview of therapy for leg veins. In: Alam M, Nguyen TH, eds. Procedures in Cosmetic Dermatology Series: Treatment of Leg Veins. Philadelphia, PA: Elsevier; 2006:48-70.
5. Bogle MA, Sadick NS. Laser surgery. In: Alam M, Nguyen TH, eds. Procedures in Cosmetic Dermatology Series: Treatment of Leg Veins. Philadelphia, PA: Elsevier; 2006:48-70.
6. Bernstein EF, Noyaner-Turley A, Renton B. Treatment of spider veins of the lower extremity with a novel 532 nm KTP laser. Lasers Surg Med. 2014;46(2):81-88.
7. Klein A, Buschmann M, Babilas P, Landthaler M, Baumler W. Indocyanine green-augmented diode laser therapy vs. long-pulsed Nd:Yag (1064 nm) laser treatment of telangiectatic leg veins: a randomized controlled trial. Br J Dermatol. 2013;169(2):365-673.
8. Moreno-Morega J, Hernandez E, Royo J, et al. Optimal and safe treatment of spider leg veins measuring less than 1.5 mm on skin type IV patients, using repeated low-fluence Nd:YAG laser pulses after polidocanol injection. Lasers Med Sci. 2013;28(3):925-933.
While sclerotherapy has long been considered the gold standard first-line treatment for small leg veins, with the new longer-pulsed 1064 nm Nd:Yag lasers and improved skill with their use, many clinicians will consider laser earlier in the leg vein treatment algorithm.
The Nd:Yag laser is the current laser of choice for treating leg veins. A recent comparison of treatment of lower extremity telangiectasias in 57 women with foam 0.5% polidocanol sclerotherapy (Asclera, Merz Aesthetics, Inc.) versus Nd:Yag laser found that both treatments result in >70% clearance. The only significant difference was in pain perception, which was greater with laser.1 Patients were treated in 2 sessions at 6-week intervals and anesthesia was not used. One leg was randomly assigned to treatment with laser, while the other received sclerotherapy. Investigators were blinded, and patients were evaluated at 6 months.1 Tips on anesthesia and patient comfort with laser leg vein treatment is discussed later in the article.
Choosing the Patient
Laser treatment of leg veins is most effective for small, superficial red or blue veins (<0.5 mm) and telangiectatic mats, any veins too small for the 32-gauge sclerotherapy needle and for needle phobic patients.2 Patients with numerous nodular varicose and spider veins tend to be poor candidates for laser leg vein treatment because of their high risk of harboring deeper venous reflux disease. These patients should receive further evaluation with ultrasound and possible treatment with endovenous laser ablation or radiofrequency laser ablation or ambulatory phlebectomy.
Prior to treatment, patients should be advised to avoid blood thinners, tanning, artificial tanners and sun exposure.
3 In addition, just as with sclerotherapy treatment, to reduce the risk of thrombosis patients should discontinue oral contraceptives prior to laser vein treatment.
4 When planning your patient’s leg vein treatment, whether it is with laser or not, it is important to identify risk factors for failed treatment. See Table for a list of poor candidates for laser leg vein treatment.
Choosing the Device: 1064 nm Nd:Yag
The 1064 nm Nd:Yag laser is the leading laser for small leg vein treatment. The short pulse duration of the original pulsed dye lasers failed to coagulate the deeper thicker veins as well as the Nd:Yag. In addition, the shorter pulse pulsed dye lasers produced a significant amount of purpura at the site of treatment, sometimes leaving stripes, circles and honeycomb patterns depending on the size and location of the vessel. Even with the long pulsed dye laser, the melanin absorption competes too much with the hemoglobin absorption resulting in a significantly higher risk of post-inflammatory hyperpigmentation (PIH)4 (Figure 1).
Figure 1. Various Absorption rates (from Dermatology with permission from Elsevier).
It is crucial to provide adequate epidermal cooling when a pulsed dye laser is used to treat veins. The longer wavelength of 1064 nm allows for deeper, adequate skin penetration (3 mm) to the veins (Figure 2). The longer pulse duration allows for slower heating and coagulation of the vessel with less purpura and less damage to the surrounding skin. The Nd:Yag is unlikely to be absorbed by melanin, which lowers the risk of epidermal damage even in darker skin types.4
Figure 2. Depth of penetration by various lasers (from Dermatology with permission from Elsevier).2,8
While a larger spot size is preferred for improved penetrance and less scatter, this is most important for treating larger and deeper veins. With the 1064 nm Nd:Yag laser, it is critical to not stack pulses and accumulate too much heat or there is significant risk to overheating the surrounding tissues, resulting in blisters and scars. Effective and safe vessel coagulation can be achieved with pulses spaced 1 mm apart.4
In addition to the risk of stacking excessive heat and causing surrounding tissue damage, another disadvantage of the Nd:Yag laser compared to sclerotherapy with polidocanol is the pain felt by the patient. Topical (eg, betacaine, tetracaine, lidocaine mix) anesthesia and epidermal cooling with air or ice is routine in my practice when treating veins with the Nd:Yag.
After topical anesthesia cream application is complete (45- 90 minutes) and removed, I prefer to use an ice cube popsicle stick and hold it for 3 seconds prior to firing the laser. The endpoint of laser treatment is immediate blanching of the vein (not the skin) or cease of blood flow with no epidermal change. This can be verified with compression and release and watching for residual flow. If there is no blanching, but flow seems to have ceased, then treatment is usually adequate.
Technique
Because oxygenated blood is targeted best by 500 nm to 600 nm lasers and deoxygenated by 800 nm to 1,100 nm, one may think that it would be best to employ the 2 different wavelengths for a more thorough leg vein treatment. The versatility of the 1064 nm Nd:Yag has eliminated the need for treatment with the 2 lasers. By modifying the spot size and pulse duration depending on the color of vein, both red and blue can be treated effectively.4 For red and superficial veins, treat with a smaller spot size and shorter pulse duration and relatively higher fluence (2-3 mm, 15-20 ms and 250-300J/cm2 Cynergy laser, Cynosure).
For blue, deeper veins, treat with a larger spot size and longer pulse duration with a moderate fluence (4 mm, 50 ms and 200J/cm2 Cynergy laser, Cynosure). It is crucial to begin with 1 pulse and look for your endpoints (Figure 3).
Figures 3A-C. Before and after treatment with 1064 nm Nd:Yag Cynergy laser at 8 weeks.
Other Devices
The KTP laser is useful and very efficacious only for small, superficial telangiectasias in patients with non-tanned Fitzpatrick skin types I-III. Pulse stacking should be avoided as with the Yag laser.
A recent study looked at the 532 nm KTP (Excel V, Cutera) using a 5 mm spot, 13 to 15J/cm2 and 40 ms pulse duration in treating 79 sites on 25 women. Physicians assessing improvement were blinded and reported a median improvement of 2.5 (5-point scale) at 12 weeks with minimal discomfort.5 PIH was reported in 2% of treatment sites. In summary, the KTP is mainly limited by its absorption of melanin and consequent increased risk of PIH when compared to the 1064 nm Nd:Yag.
Long-pulsed alexandrite and diode lasers may also be used successfully to treat leg veins, though they will not penetrate as deep as the 1064 nm, and may absorb more melanin versus the Nd:Yag.4
A recent study compared the indocyanine green-augmented diode laser (810 nm) to the 1064 nm Nd:Yag in a prospective, randomized, controlled trial to treat small telangiectatic leg veins in 29 study participants.6 For the study, 2 blinded investigators evaluated the patients at 3 months. Both investigators’ and participants’ assessments found significantly better clearance at 3 months with the diode laser versus the Nd:Yag; however, the diode laser was rated more painful.
In summary, while the diode laser may be as effective as the Nd:Yag with small telangiectatic leg veins, it may be more painful, and is unlikely to penetrate deep enough compared to the Nd:Yag for some larger or deeper veins.
Intense pulse light (515 nm-1,200 nm) may be used because it permits target of both superficial and deeper vessels. However, it is not safe in darker skin types because of risk of melanin absorption and consequent blistering.
Treatment Pearls
When there are deeper reticular veins, it is not a good idea to limit your treatment to laser or begin your treatment with laser. Try to assess for deeper reticular varicose veins that may be connected to a superficial vein and treat that deeper reticular vein with sclerotherapy prior to attempting laser treatment of the smaller superficial vein. Larger reticular veins are best treated first with foam sclerotherapy and then remaining superficial veins can be treated with laser. Polidocanol was FDA approved in 2010 and carries the advantages of being less allergenic than sodium tetradecyl sulfate injection (Sotradecol, AngioDynamics) and many physicians report that patients experience less pain and a lower risk for skin ulceration than other sclerosants. Laser treatments may need to be repeated and should be spaced 8 weeks apart if treating some larger diameter veins. If only small superficial red veins were treated, then 4 weeks follow-up is usually adequate. Some veins may gradually resorb over many weeks. It is good to advise patients about this, so they do not have unrealistic expectations about immediate results.
Though some physicians have reported that no compression is needed after laser treatment, I prefer to recommend 3 weeks of compression when many veins are treated and if the patient tends to stand or sit a lot. For best results, combine sclerotherapy treatment with laser treatment in the same day, and apply compression immediately after completion while patient is still on the table.
A recent study compared treatment of spider leg veins less than 1.5 mm in skin type IV patients with polidocanol foam versus either Nd:Yag (low-fluence pulsed) laser alone or with polidocanol foam followed by Nd:Yag (low-fluence pulsed) laser.7 Efficacy of combination treatment proved safe and satisfactory in 96% of patients using low-fluence laser pulses with a total cumulative energy in the 3 cm venous segment; and the Nd:Yag laser was safe in these darker skin types.
Dr. Stolman, a board-certified dermatologist and dermatologic surgeon specializing in lasers and other skin treatment devices, is on the faculty at of the University of Utah School of Medicine, department of dermatology, in Salt Lake City, UT.
Disclosure: The author reports no relevant financial relationships.
References
1. Parlar B, Blazek C, Cazzaniga S, et al. Treatment of lower extremity telangiectasias in women by foam sclerotherapy vs. Nd:YAG laser: a prospective, comparative, randomized, open-label trial. J Eur Acad Dermatol Venereol. Published online ahead of print July 28, 2014.
2. Meesters AA, Pitassi LH, Campos V, Wokerstorfer A, Dierickx CC. Transcutaneous laser treatment of leg veins. Lasers Med Sci. 2014;29(2):481-492.
3. Hirsch RJ, Anderson RR. Principles of laser skin interactions. In: Bolognia JL, Jorizzo JL, Rapini RP, eds. Dermatology. Maryland Heights, MO: Mosby; 2003:2148. 4.Hsu TS. An overview of therapy for leg veins. In: Alam M, Nguyen TH, eds. Procedures in Cosmetic Dermatology Series: Treatment of Leg Veins. Philadelphia, PA: Elsevier; 2006:48-70.
5. Bogle MA, Sadick NS. Laser surgery. In: Alam M, Nguyen TH, eds. Procedures in Cosmetic Dermatology Series: Treatment of Leg Veins. Philadelphia, PA: Elsevier; 2006:48-70.
6. Bernstein EF, Noyaner-Turley A, Renton B. Treatment of spider veins of the lower extremity with a novel 532 nm KTP laser. Lasers Surg Med. 2014;46(2):81-88.
7. Klein A, Buschmann M, Babilas P, Landthaler M, Baumler W. Indocyanine green-augmented diode laser therapy vs. long-pulsed Nd:Yag (1064 nm) laser treatment of telangiectatic leg veins: a randomized controlled trial. Br J Dermatol. 2013;169(2):365-673.
8. Moreno-Morega J, Hernandez E, Royo J, et al. Optimal and safe treatment of spider leg veins measuring less than 1.5 mm on skin type IV patients, using repeated low-fluence Nd:YAG laser pulses after polidocanol injection. Lasers Med Sci. 2013;28(3):925-933.