PATIENT PRESENTATION

A 58-year-old man presented with an asymptomatic lesion that had been present for 2 years on his right lateral distal leg. Cutaneous examination showed a 2-mm annular hyperkeratotic plaque with central atrophy and raised borders, as shown in the image above. The patient had a history of bone marrow transplant to treat acute myeloid leukemia.
WHAT IS YOUR DIAGNOSIS?
Diagnosis: Porokeratosis of Mibelli
 Mibelli and Respighi first described porokeratosis of Mibelli in 1893.1 The condition was initially assumed to involve hyperkeratosis of the eccrine ostia, and the disease was subsequently mislabeled “porokeratosis.”2 It is now commonly referred to as porokeratosis of Mibelli. Five clinical variants are currently recognized: porokeratosis of Mibelli (classic type), disseminated superficial porokeratosis and disseminated superficial actinic porokeratosis, porokeratosis palmaris et plantaris disseminate, linear porokeratosis, and punctate porokeratosis (Table 1).3-25
Mibelli and Respighi first described porokeratosis of Mibelli in 1893.1 The condition was initially assumed to involve hyperkeratosis of the eccrine ostia, and the disease was subsequently mislabeled “porokeratosis.”2 It is now commonly referred to as porokeratosis of Mibelli. Five clinical variants are currently recognized: porokeratosis of Mibelli (classic type), disseminated superficial porokeratosis and disseminated superficial actinic porokeratosis, porokeratosis palmaris et plantaris disseminate, linear porokeratosis, and punctate porokeratosis (Table 1).3-25
Epidemiology
The onset of porokeratosis of Mibelli typically occurs during childhood, especially if it is hereditary.3 Porokeratosis of Mibelli is more commonly observed (2.17:1.00) in men than in women.3 Caucasians, particularly Italians, are at higher risk to present with the disease.2 Darker skin types rarely present with porokeratosis of Mibelli.3
Clinical Characteristics
Porokeratosis of Mibelli typically appears in early childhood, although onset can occur at any age.5 A solitary or small number of plaques of variable size (up to 20 cm in diameter) typically present unilaterally on limbs, as well as the palms and soles.3 Several cases report lesions on the face, genitals and mucous membranes.2,3 Giant forms have been described and may mimic findings of psoriasis.9 These lesions typically display a highly raised peripheral border of up to 1 cm.2
The lesion initially appears as an asymptomatic papule that spreads slowly in a centrifugal manner, yielding a hypopigmented atrophic central section with anhidrosis and alopecia.2 An “M-shaped” border, often appearing as two adjacent raised edges, can be viewed in radial cross section.2,10 It eventually presents as an oval or circular plaque with a well-demarcated margin.8 A fissure circumscribing the hyperkeratotic border serves as a clinical hallmark for diagnosis.8
Differential Diagnosis
Porokeratosis of Mibelli is a rare disorder of keratinization for which several similarly appearing conditions may be considered in the differential diagnosis. Psoriasis plaques may mimic or coexist in patients with porokeratosis of Mibelli.9 Gene expression profiling of the cornoid lamella in porokeratosis of Mibelli shares several similarities with psoriasis, including significantly comparable levels of S-100 calcium-binding proteins and gap junction proteins.9 Elastosis perforans serpinginosa, lichen planus, lichen sclerosus atrophicus, linear verrucous epidermal nevus, plaque stage of cutaneous T-cell lymphoma and punctate keratoderma may also be considered in the differential diagnosis for porokeratosis.18,19
Histopathology
All variants of porokeratosis display a characteristic cornoid lamella, a tightly packed column of parakeratosis presenting within an indentation of the epidermis.1,3 The column of parakeratosis typically extends through the orthokeratotic stratum corneum.5 The granular layer is centrally diminished or absent and keratinocytes are dyskeratotic.7 The epidermis is atrophic, with vacuolar change commonly exhibited in the keratinocytes at the base of the cornoid lamella.8 The subjacent papillary dermis may present with a perivascular inflammatory infiltrate.1,2
Associated Conditions
Several conditions have been associated with porokeratosis of Mibelli. Many patients have developed porokeratosis of Mibelli following bone marrow transplantation;11,12 immunosuppressive therapy following each respective bone marrow transplant has been reported to initiate the onset of porokeratosis.12 One group of investigators noted that 10.68% of patients who underwent organ transplantation with immunosuppressive treatments subsequently developed porokeratosis.12 In addition to organ transplantation, other methods of immunosuppression, including electron beam radiation, corticosteroids and chemotherapy, have been associated with porokeratosis.11,13,14
Additionally, porokeratosis has been reported in several patients as a possible result of paraneoplastic syndrome. Porokeratosis, particularly disseminated superficial porokeratosis, developed prior to a diagnosis of solid organ malignancies, suggesting a paraneoplastic manifestation of the cutaneous disease.15,16 The lesions appeared in patients affected by hepatocellular carcinoma, cholangiocarcinoma and ovarian adenocarcinoma.15,16 Recent studies associate the pathogenic linkage between each respective carcinoma and the porokeratosis with p53 gene product overexpression.15,16
Recently, a 66-year-old male with a hyperkeratotic variant of porokeratosis of Mibelli who presented with associated dermal amyloid deposits was described.17 The hyperkeratotic lesions appeared as multiple brownish verrucous plaques on the gluteal region and left toe.17 Several patients have been described with either the hyperkeratotic variant of porokeratosis of Mibelli or whose porokeratosis was associated with dermal amyloid deposits; however, very few individuals have been reported in whom both abnormalities are present. The relationship between these two entities has yet to be determined.17
Pathogensis
The etiology of porokeratosis is unknown. It is thought to be a genodermatosis inherited sporadically or in an autosomal dominant fashion with variable penetrance.1,4 It has been postulated that the epidermis contains abnormal keratinocyte clones, produced by either improper maturation of keratinocytes or by an acceleration of epidermopoiesis, which migrate centrifugally to form the distinctive cornoid lamella.1,3 Disruption of loricrin expression beneath the cornoid lamella signifies abnormal regulation of terminal differentiation.3,15 Instability of region p12-14 of chromosome 3 may be involved with the defective terminal differentiation in porokeratosis of Mibelli.3,5
In addition to genetics, environmental factors play a role in the development of porokeratosis of Mibelli. Phenotypic expression of the mutant keratinocyte clones are elicited by several trigger factors, including trauma, immunosuppression, irradiation and infective agents.1,2,6 Several cases were reported after organ transplants, including bone marrow, heart, kidney, liver and lung transplants.6
Malignant transformation is a potential complication of porokeratosis.2 Malignancies include Bowen’s disease, squamous cell carcinoma and basal cell carcinoma.2 Findings of increased chromosomal instability in fibroblasts from unaffected areas and peripheral blood lymphocytes suggest an increased susceptibility to general malignancy.3 The increased oncogenic potential is attributed to overexpression of p53 in the keratinocytes near the cornoid lamella.3 Overexpression of the p53 gene product may be responsible for early keratinocyte apoptosis, further complementing the defective regulation of keratinocyte terminal differentiation.15
Treatment
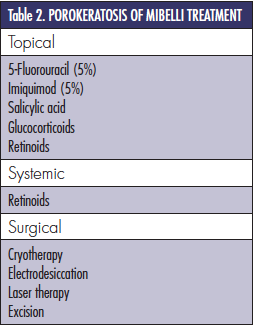
 Several treatment modalities are available for the management of porokeratosis of Mibelli (Table 2). Therapeutic intervention depends on lesion size and location, as well as the aesthetic desires of the patient.9 Protection from sunlight, moisturizers and supported immune status may sufficiently suppress the disease. However, periodic observation and/or further treatment may be recommended due to the potential risk of malignant transformation.3,20 Topical therapies include 5-fluorouracil, imiquimod, salicylic acid, glucocorticoids and retinoids.3 Additional options include destruction of the lesion with cryotherapy, electrodissection, laser ablation and/or surgical excision.3,19-20
Several treatment modalities are available for the management of porokeratosis of Mibelli (Table 2). Therapeutic intervention depends on lesion size and location, as well as the aesthetic desires of the patient.9 Protection from sunlight, moisturizers and supported immune status may sufficiently suppress the disease. However, periodic observation and/or further treatment may be recommended due to the potential risk of malignant transformation.3,20 Topical therapies include 5-fluorouracil, imiquimod, salicylic acid, glucocorticoids and retinoids.3 Additional options include destruction of the lesion with cryotherapy, electrodissection, laser ablation and/or surgical excision.3,19-20
Salicylic acid has been demonstrated to inhibit the progression of porokeratosis lesions, but relapses have been noted after cessation of treatment.3 Glucocorticoids have also shown success as a topical treatment, but may contribute to further immunosuppression and possible malignant transformation.3 Topical and systemic utilization of retinoids have yielded recent reports of success.3 If there are no contraindications, systemic retinoids may be the preferred method of treatment, as they are not only able to terminate carcinogenesis but also to diminish cytological atypia.3 Yet, retinoids may contribute to immunosuppression in these patients, reducing their long-term use.3
Topical 5-fluorouracil is an effective therapy currently employed against several porokeratosis variants.3,21 Its method of action inhibits the formation of thymidylic acid, thereby hindering the rate-limiting step of DNA synthesis in rapidly dividing cells.21 A novel treatment has combined topical fluorouracil and photodynamic therapy with aminolevulinic acid with promising results.21 However, in some patients, severe dermatitis and scarring after fluorouracil have been reported.22
Porokeratosis of Mibelli has also been managed using topical imiquimod.20-21,23-24 Imiquimod is a novel immune response modifier that functions by inducing cytokine production for innate and acquired cellular immune response.20-21 Imiquimod 5% cream combined with keralytic therapy has been an efficacious treatment, particularly in immunocompromised patients.23 Researchers recently reported the successful use of both topical imiquimod 5% with topical 5-fluorouracil 5%.7 Local skin inflammation with erthyema, edema, ulceration, dryness and scab formation may occur when treating with imiquimod cream.24 Preliminary results did not show significant scarring.23
Destructive treatments are another option available for treating porokeratosis of Mibelli. Cryotherapy, electrodesiccation, laser therapy and surgical excision have all shown varying levels of success.3,19-20 These modalities may be preferred in patients with one to few porokeratosis lesions.3 Surgical excision should be considered if there is biopsy confirmation that cutaneous malignancy has developed; indeed, surgical removal may also be favored when dealing with recalcitrant lesions.3 Further studies are needed to determine the significance of non-invasive therapies in comparison with surgical treatments in reducing the incidence of malignancy.3
Summary
Porokeratosis of Mibelli is a rare disorder of keratinization, presenting with one or more annular plaques with central atrophy and raised keratotic borders. There are several clinical variants, with each form exhibiting a common histopathologic characteristic cornoid lamella. The lesions should be carefully monitored periodically in order to detect potential malignant transformation into Bowen’s disease, squamous cell carcinoma or basal cell carcinoma. There are multiple treatment options available.
Patient Management

 Figure 2. Distant (left) and closer (right) views show complete resolution of porokeratosis of Mibelli following treatment with topical 5-fluorouracil. There are erythematous excoriation sites of recent arthropod assaults.
Figure 2. Distant (left) and closer (right) views show complete resolution of porokeratosis of Mibelli following treatment with topical 5-fluorouracil. There are erythematous excoriation sites of recent arthropod assaults.
Our patient illustrates the successful treatment of porokeratosis of Mibelli of the right lateral calf in a 58-year-old man with topical fluorouracil 5% (Efudex 5%). He exhibited complete resolution of the lesion within 2 months of twice daily treatment and has shown no recurrence after 1 year (Figure 2). We will continue to monitor his condition and ensure that there is no recurrence of lesions.
Mr. Anzalone is with the University of Texas Medical School in Houston, TX.
Dr. Cohen is with the University of Houston Health Center, and the departments of dermatology at both the University of Texas Health Science Center Medical School and the University of Texas MD Anderson Cancer Center in Houston, TX.
Disclosure: The authors have no conflicts of interest or financial disclosures to report.
PATIENT PRESENTATION

A 58-year-old man presented with an asymptomatic lesion that had been present for 2 years on his right lateral distal leg. Cutaneous examination showed a 2-mm annular hyperkeratotic plaque with central atrophy and raised borders, as shown in the image above. The patient had a history of bone marrow transplant to treat acute myeloid leukemia.
WHAT IS YOUR DIAGNOSIS?
Diagnosis: Porokeratosis of Mibelli
 Mibelli and Respighi first described porokeratosis of Mibelli in 1893.1 The condition was initially assumed to involve hyperkeratosis of the eccrine ostia, and the disease was subsequently mislabeled “porokeratosis.”2 It is now commonly referred to as porokeratosis of Mibelli. Five clinical variants are currently recognized: porokeratosis of Mibelli (classic type), disseminated superficial porokeratosis and disseminated superficial actinic porokeratosis, porokeratosis palmaris et plantaris disseminate, linear porokeratosis, and punctate porokeratosis (Table 1).3-25
Mibelli and Respighi first described porokeratosis of Mibelli in 1893.1 The condition was initially assumed to involve hyperkeratosis of the eccrine ostia, and the disease was subsequently mislabeled “porokeratosis.”2 It is now commonly referred to as porokeratosis of Mibelli. Five clinical variants are currently recognized: porokeratosis of Mibelli (classic type), disseminated superficial porokeratosis and disseminated superficial actinic porokeratosis, porokeratosis palmaris et plantaris disseminate, linear porokeratosis, and punctate porokeratosis (Table 1).3-25
Epidemiology
The onset of porokeratosis of Mibelli typically occurs during childhood, especially if it is hereditary.3 Porokeratosis of Mibelli is more commonly observed (2.17:1.00) in men than in women.3 Caucasians, particularly Italians, are at higher risk to present with the disease.2 Darker skin types rarely present with porokeratosis of Mibelli.3
Clinical Characteristics
Porokeratosis of Mibelli typically appears in early childhood, although onset can occur at any age.5 A solitary or small number of plaques of variable size (up to 20 cm in diameter) typically present unilaterally on limbs, as well as the palms and soles.3 Several cases report lesions on the face, genitals and mucous membranes.2,3 Giant forms have been described and may mimic findings of psoriasis.9 These lesions typically display a highly raised peripheral border of up to 1 cm.2
The lesion initially appears as an asymptomatic papule that spreads slowly in a centrifugal manner, yielding a hypopigmented atrophic central section with anhidrosis and alopecia.2 An “M-shaped” border, often appearing as two adjacent raised edges, can be viewed in radial cross section.2,10 It eventually presents as an oval or circular plaque with a well-demarcated margin.8 A fissure circumscribing the hyperkeratotic border serves as a clinical hallmark for diagnosis.8
Differential Diagnosis
Porokeratosis of Mibelli is a rare disorder of keratinization for which several similarly appearing conditions may be considered in the differential diagnosis. Psoriasis plaques may mimic or coexist in patients with porokeratosis of Mibelli.9 Gene expression profiling of the cornoid lamella in porokeratosis of Mibelli shares several similarities with psoriasis, including significantly comparable levels of S-100 calcium-binding proteins and gap junction proteins.9 Elastosis perforans serpinginosa, lichen planus, lichen sclerosus atrophicus, linear verrucous epidermal nevus, plaque stage of cutaneous T-cell lymphoma and punctate keratoderma may also be considered in the differential diagnosis for porokeratosis.18,19
Histopathology
All variants of porokeratosis display a characteristic cornoid lamella, a tightly packed column of parakeratosis presenting within an indentation of the epidermis.1,3 The column of parakeratosis typically extends through the orthokeratotic stratum corneum.5 The granular layer is centrally diminished or absent and keratinocytes are dyskeratotic.7 The epidermis is atrophic, with vacuolar change commonly exhibited in the keratinocytes at the base of the cornoid lamella.8 The subjacent papillary dermis may present with a perivascular inflammatory infiltrate.1,2
Associated Conditions
Several conditions have been associated with porokeratosis of Mibelli. Many patients have developed porokeratosis of Mibelli following bone marrow transplantation;11,12 immunosuppressive therapy following each respective bone marrow transplant has been reported to initiate the onset of porokeratosis.12 One group of investigators noted that 10.68% of patients who underwent organ transplantation with immunosuppressive treatments subsequently developed porokeratosis.12 In addition to organ transplantation, other methods of immunosuppression, including electron beam radiation, corticosteroids and chemotherapy, have been associated with porokeratosis.11,13,14
Additionally, porokeratosis has been reported in several patients as a possible result of paraneoplastic syndrome. Porokeratosis, particularly disseminated superficial porokeratosis, developed prior to a diagnosis of solid organ malignancies, suggesting a paraneoplastic manifestation of the cutaneous disease.15,16 The lesions appeared in patients affected by hepatocellular carcinoma, cholangiocarcinoma and ovarian adenocarcinoma.15,16 Recent studies associate the pathogenic linkage between each respective carcinoma and the porokeratosis with p53 gene product overexpression.15,16
Recently, a 66-year-old male with a hyperkeratotic variant of porokeratosis of Mibelli who presented with associated dermal amyloid deposits was described.17 The hyperkeratotic lesions appeared as multiple brownish verrucous plaques on the gluteal region and left toe.17 Several patients have been described with either the hyperkeratotic variant of porokeratosis of Mibelli or whose porokeratosis was associated with dermal amyloid deposits; however, very few individuals have been reported in whom both abnormalities are present. The relationship between these two entities has yet to be determined.17
Pathogensis
The etiology of porokeratosis is unknown. It is thought to be a genodermatosis inherited sporadically or in an autosomal dominant fashion with variable penetrance.1,4 It has been postulated that the epidermis contains abnormal keratinocyte clones, produced by either improper maturation of keratinocytes or by an acceleration of epidermopoiesis, which migrate centrifugally to form the distinctive cornoid lamella.1,3 Disruption of loricrin expression beneath the cornoid lamella signifies abnormal regulation of terminal differentiation.3,15 Instability of region p12-14 of chromosome 3 may be involved with the defective terminal differentiation in porokeratosis of Mibelli.3,5
In addition to genetics, environmental factors play a role in the development of porokeratosis of Mibelli. Phenotypic expression of the mutant keratinocyte clones are elicited by several trigger factors, including trauma, immunosuppression, irradiation and infective agents.1,2,6 Several cases were reported after organ transplants, including bone marrow, heart, kidney, liver and lung transplants.6
Malignant transformation is a potential complication of porokeratosis.2 Malignancies include Bowen’s disease, squamous cell carcinoma and basal cell carcinoma.2 Findings of increased chromosomal instability in fibroblasts from unaffected areas and peripheral blood lymphocytes suggest an increased susceptibility to general malignancy.3 The increased oncogenic potential is attributed to overexpression of p53 in the keratinocytes near the cornoid lamella.3 Overexpression of the p53 gene product may be responsible for early keratinocyte apoptosis, further complementing the defective regulation of keratinocyte terminal differentiation.15
Treatment
 Several treatment modalities are available for the management of porokeratosis of Mibelli (Table 2). Therapeutic intervention depends on lesion size and location, as well as the aesthetic desires of the patient.9 Protection from sunlight, moisturizers and supported immune status may sufficiently suppress the disease. However, periodic observation and/or further treatment may be recommended due to the potential risk of malignant transformation.3,20 Topical therapies include 5-fluorouracil, imiquimod, salicylic acid, glucocorticoids and retinoids.3 Additional options include destruction of the lesion with cryotherapy, electrodissection, laser ablation and/or surgical excision.3,19-20
Several treatment modalities are available for the management of porokeratosis of Mibelli (Table 2). Therapeutic intervention depends on lesion size and location, as well as the aesthetic desires of the patient.9 Protection from sunlight, moisturizers and supported immune status may sufficiently suppress the disease. However, periodic observation and/or further treatment may be recommended due to the potential risk of malignant transformation.3,20 Topical therapies include 5-fluorouracil, imiquimod, salicylic acid, glucocorticoids and retinoids.3 Additional options include destruction of the lesion with cryotherapy, electrodissection, laser ablation and/or surgical excision.3,19-20
Salicylic acid has been demonstrated to inhibit the progression of porokeratosis lesions, but relapses have been noted after cessation of treatment.3 Glucocorticoids have also shown success as a topical treatment, but may contribute to further immunosuppression and possible malignant transformation.3 Topical and systemic utilization of retinoids have yielded recent reports of success.3 If there are no contraindications, systemic retinoids may be the preferred method of treatment, as they are not only able to terminate carcinogenesis but also to diminish cytological atypia.3 Yet, retinoids may contribute to immunosuppression in these patients, reducing their long-term use.3
Topical 5-fluorouracil is an effective therapy currently employed against several porokeratosis variants.3,21 Its method of action inhibits the formation of thymidylic acid, thereby hindering the rate-limiting step of DNA synthesis in rapidly dividing cells.21 A novel treatment has combined topical fluorouracil and photodynamic therapy with aminolevulinic acid with promising results.21 However, in some patients, severe dermatitis and scarring after fluorouracil have been reported.22
Porokeratosis of Mibelli has also been managed using topical imiquimod.20-21,23-24 Imiquimod is a novel immune response modifier that functions by inducing cytokine production for innate and acquired cellular immune response.20-21 Imiquimod 5% cream combined with keralytic therapy has been an efficacious treatment, particularly in immunocompromised patients.23 Researchers recently reported the successful use of both topical imiquimod 5% with topical 5-fluorouracil 5%.7 Local skin inflammation with erthyema, edema, ulceration, dryness and scab formation may occur when treating with imiquimod cream.24 Preliminary results did not show significant scarring.23
Destructive treatments are another option available for treating porokeratosis of Mibelli. Cryotherapy, electrodesiccation, laser therapy and surgical excision have all shown varying levels of success.3,19-20 These modalities may be preferred in patients with one to few porokeratosis lesions.3 Surgical excision should be considered if there is biopsy confirmation that cutaneous malignancy has developed; indeed, surgical removal may also be favored when dealing with recalcitrant lesions.3 Further studies are needed to determine the significance of non-invasive therapies in comparison with surgical treatments in reducing the incidence of malignancy.3
Summary
Porokeratosis of Mibelli is a rare disorder of keratinization, presenting with one or more annular plaques with central atrophy and raised keratotic borders. There are several clinical variants, with each form exhibiting a common histopathologic characteristic cornoid lamella. The lesions should be carefully monitored periodically in order to detect potential malignant transformation into Bowen’s disease, squamous cell carcinoma or basal cell carcinoma. There are multiple treatment options available.
Patient Management

 Figure 2. Distant (left) and closer (right) views show complete resolution of porokeratosis of Mibelli following treatment with topical 5-fluorouracil. There are erythematous excoriation sites of recent arthropod assaults.
Figure 2. Distant (left) and closer (right) views show complete resolution of porokeratosis of Mibelli following treatment with topical 5-fluorouracil. There are erythematous excoriation sites of recent arthropod assaults.
Our patient illustrates the successful treatment of porokeratosis of Mibelli of the right lateral calf in a 58-year-old man with topical fluorouracil 5% (Efudex 5%). He exhibited complete resolution of the lesion within 2 months of twice daily treatment and has shown no recurrence after 1 year (Figure 2). We will continue to monitor his condition and ensure that there is no recurrence of lesions.
Mr. Anzalone is with the University of Texas Medical School in Houston, TX.
Dr. Cohen is with the University of Houston Health Center, and the departments of dermatology at both the University of Texas Health Science Center Medical School and the University of Texas MD Anderson Cancer Center in Houston, TX.
Disclosure: The authors have no conflicts of interest or financial disclosures to report.
PATIENT PRESENTATION
A 58-year-old man presented with an asymptomatic lesion that had been present for 2 years on his right lateral distal leg. Cutaneous examination showed a 2-mm annular hyperkeratotic plaque with central atrophy and raised borders, as shown in the image above. The patient had a history of bone marrow transplant to treat acute myeloid leukemia.
WHAT IS YOUR DIAGNOSIS?
Diagnosis: Porokeratosis of Mibelli
Mibelli and Respighi first described porokeratosis of Mibelli in 1893.1 The condition was initially assumed to involve hyperkeratosis of the eccrine ostia, and the disease was subsequently mislabeled “porokeratosis.”2 It is now commonly referred to as porokeratosis of Mibelli. Five clinical variants are currently recognized: porokeratosis of Mibelli (classic type), disseminated superficial porokeratosis and disseminated superficial actinic porokeratosis, porokeratosis palmaris et plantaris disseminate, linear porokeratosis, and punctate porokeratosis (Table 1).3-25
Epidemiology
The onset of porokeratosis of Mibelli typically occurs during childhood, especially if it is hereditary.3 Porokeratosis of Mibelli is more commonly observed (2.17:1.00) in men than in women.3 Caucasians, particularly Italians, are at higher risk to present with the disease.2 Darker skin types rarely present with porokeratosis of Mibelli.3
Clinical Characteristics
Porokeratosis of Mibelli typically appears in early childhood, although onset can occur at any age.5 A solitary or small number of plaques of variable size (up to 20 cm in diameter) typically present unilaterally on limbs, as well as the palms and soles.3 Several cases report lesions on the face, genitals and mucous membranes.2,3 Giant forms have been described and may mimic findings of psoriasis.9 These lesions typically display a highly raised peripheral border of up to 1 cm.2
The lesion initially appears as an asymptomatic papule that spreads slowly in a centrifugal manner, yielding a hypopigmented atrophic central section with anhidrosis and alopecia.2 An “M-shaped” border, often appearing as two adjacent raised edges, can be viewed in radial cross section.2,10 It eventually presents as an oval or circular plaque with a well-demarcated margin.8 A fissure circumscribing the hyperkeratotic border serves as a clinical hallmark for diagnosis.8
Differential Diagnosis
Porokeratosis of Mibelli is a rare disorder of keratinization for which several similarly appearing conditions may be considered in the differential diagnosis. Psoriasis plaques may mimic or coexist in patients with porokeratosis of Mibelli.9 Gene expression profiling of the cornoid lamella in porokeratosis of Mibelli shares several similarities with psoriasis, including significantly comparable levels of S-100 calcium-binding proteins and gap junction proteins.9 Elastosis perforans serpinginosa, lichen planus, lichen sclerosus atrophicus, linear verrucous epidermal nevus, plaque stage of cutaneous T-cell lymphoma and punctate keratoderma may also be considered in the differential diagnosis for porokeratosis.18,19
Histopathology
All variants of porokeratosis display a characteristic cornoid lamella, a tightly packed column of parakeratosis presenting within an indentation of the epidermis.1,3 The column of parakeratosis typically extends through the orthokeratotic stratum corneum.5 The granular layer is centrally diminished or absent and keratinocytes are dyskeratotic.7 The epidermis is atrophic, with vacuolar change commonly exhibited in the keratinocytes at the base of the cornoid lamella.8 The subjacent papillary dermis may present with a perivascular inflammatory infiltrate.1,2
Associated Conditions
Several conditions have been associated with porokeratosis of Mibelli. Many patients have developed porokeratosis of Mibelli following bone marrow transplantation;11,12 immunosuppressive therapy following each respective bone marrow transplant has been reported to initiate the onset of porokeratosis.12 One group of investigators noted that 10.68% of patients who underwent organ transplantation with immunosuppressive treatments subsequently developed porokeratosis.12 In addition to organ transplantation, other methods of immunosuppression, including electron beam radiation, corticosteroids and chemotherapy, have been associated with porokeratosis.11,13,14
Additionally, porokeratosis has been reported in several patients as a possible result of paraneoplastic syndrome. Porokeratosis, particularly disseminated superficial porokeratosis, developed prior to a diagnosis of solid organ malignancies, suggesting a paraneoplastic manifestation of the cutaneous disease.15,16 The lesions appeared in patients affected by hepatocellular carcinoma, cholangiocarcinoma and ovarian adenocarcinoma.15,16 Recent studies associate the pathogenic linkage between each respective carcinoma and the porokeratosis with p53 gene product overexpression.15,16
Recently, a 66-year-old male with a hyperkeratotic variant of porokeratosis of Mibelli who presented with associated dermal amyloid deposits was described.17 The hyperkeratotic lesions appeared as multiple brownish verrucous plaques on the gluteal region and left toe.17 Several patients have been described with either the hyperkeratotic variant of porokeratosis of Mibelli or whose porokeratosis was associated with dermal amyloid deposits; however, very few individuals have been reported in whom both abnormalities are present. The relationship between these two entities has yet to be determined.17
Pathogensis
The etiology of porokeratosis is unknown. It is thought to be a genodermatosis inherited sporadically or in an autosomal dominant fashion with variable penetrance.1,4 It has been postulated that the epidermis contains abnormal keratinocyte clones, produced by either improper maturation of keratinocytes or by an acceleration of epidermopoiesis, which migrate centrifugally to form the distinctive cornoid lamella.1,3 Disruption of loricrin expression beneath the cornoid lamella signifies abnormal regulation of terminal differentiation.3,15 Instability of region p12-14 of chromosome 3 may be involved with the defective terminal differentiation in porokeratosis of Mibelli.3,5
In addition to genetics, environmental factors play a role in the development of porokeratosis of Mibelli. Phenotypic expression of the mutant keratinocyte clones are elicited by several trigger factors, including trauma, immunosuppression, irradiation and infective agents.1,2,6 Several cases were reported after organ transplants, including bone marrow, heart, kidney, liver and lung transplants.6
Malignant transformation is a potential complication of porokeratosis.2 Malignancies include Bowen’s disease, squamous cell carcinoma and basal cell carcinoma.2 Findings of increased chromosomal instability in fibroblasts from unaffected areas and peripheral blood lymphocytes suggest an increased susceptibility to general malignancy.3 The increased oncogenic potential is attributed to overexpression of p53 in the keratinocytes near the cornoid lamella.3 Overexpression of the p53 gene product may be responsible for early keratinocyte apoptosis, further complementing the defective regulation of keratinocyte terminal differentiation.15
Treatment
Several treatment modalities are available for the management of porokeratosis of Mibelli (Table 2). Therapeutic intervention depends on lesion size and location, as well as the aesthetic desires of the patient.9 Protection from sunlight, moisturizers and supported immune status may sufficiently suppress the disease. However, periodic observation and/or further treatment may be recommended due to the potential risk of malignant transformation.3,20 Topical therapies include 5-fluorouracil, imiquimod, salicylic acid, glucocorticoids and retinoids.3 Additional options include destruction of the lesion with cryotherapy, electrodissection, laser ablation and/or surgical excision.3,19-20
Salicylic acid has been demonstrated to inhibit the progression of porokeratosis lesions, but relapses have been noted after cessation of treatment.3 Glucocorticoids have also shown success as a topical treatment, but may contribute to further immunosuppression and possible malignant transformation.3 Topical and systemic utilization of retinoids have yielded recent reports of success.3 If there are no contraindications, systemic retinoids may be the preferred method of treatment, as they are not only able to terminate carcinogenesis but also to diminish cytological atypia.3 Yet, retinoids may contribute to immunosuppression in these patients, reducing their long-term use.3
Topical 5-fluorouracil is an effective therapy currently employed against several porokeratosis variants.3,21 Its method of action inhibits the formation of thymidylic acid, thereby hindering the rate-limiting step of DNA synthesis in rapidly dividing cells.21 A novel treatment has combined topical fluorouracil and photodynamic therapy with aminolevulinic acid with promising results.21 However, in some patients, severe dermatitis and scarring after fluorouracil have been reported.22
Porokeratosis of Mibelli has also been managed using topical imiquimod.20-21,23-24 Imiquimod is a novel immune response modifier that functions by inducing cytokine production for innate and acquired cellular immune response.20-21 Imiquimod 5% cream combined with keralytic therapy has been an efficacious treatment, particularly in immunocompromised patients.23 Researchers recently reported the successful use of both topical imiquimod 5% with topical 5-fluorouracil 5%.7 Local skin inflammation with erthyema, edema, ulceration, dryness and scab formation may occur when treating with imiquimod cream.24 Preliminary results did not show significant scarring.23
Destructive treatments are another option available for treating porokeratosis of Mibelli. Cryotherapy, electrodesiccation, laser therapy and surgical excision have all shown varying levels of success.3,19-20 These modalities may be preferred in patients with one to few porokeratosis lesions.3 Surgical excision should be considered if there is biopsy confirmation that cutaneous malignancy has developed; indeed, surgical removal may also be favored when dealing with recalcitrant lesions.3 Further studies are needed to determine the significance of non-invasive therapies in comparison with surgical treatments in reducing the incidence of malignancy.3
Summary
Porokeratosis of Mibelli is a rare disorder of keratinization, presenting with one or more annular plaques with central atrophy and raised keratotic borders. There are several clinical variants, with each form exhibiting a common histopathologic characteristic cornoid lamella. The lesions should be carefully monitored periodically in order to detect potential malignant transformation into Bowen’s disease, squamous cell carcinoma or basal cell carcinoma. There are multiple treatment options available.
Patient Management
Figure 2. Distant (left) and closer (right) views show complete resolution of porokeratosis of Mibelli following treatment with topical 5-fluorouracil. There are erythematous excoriation sites of recent arthropod assaults.
Our patient illustrates the successful treatment of porokeratosis of Mibelli of the right lateral calf in a 58-year-old man with topical fluorouracil 5% (Efudex 5%). He exhibited complete resolution of the lesion within 2 months of twice daily treatment and has shown no recurrence after 1 year (Figure 2). We will continue to monitor his condition and ensure that there is no recurrence of lesions.
Mr. Anzalone is with the University of Texas Medical School in Houston, TX.
Dr. Cohen is with the University of Houston Health Center, and the departments of dermatology at both the University of Texas Health Science Center Medical School and the University of Texas MD Anderson Cancer Center in Houston, TX.
Disclosure: The authors have no conflicts of interest or financial disclosures to report.








 Mibelli and Respighi first described porokeratosis of Mibelli in 1893.1 The condition was initially assumed to involve hyperkeratosis of the eccrine ostia, and the disease was subsequently mislabeled “porokeratosis.”2 It is now commonly referred to as porokeratosis of Mibelli. Five clinical variants are currently recognized: porokeratosis of Mibelli (classic type), disseminated superficial porokeratosis and disseminated superficial actinic porokeratosis, porokeratosis palmaris et plantaris disseminate, linear porokeratosis, and punctate porokeratosis (Table 1).3-25
Mibelli and Respighi first described porokeratosis of Mibelli in 1893.1 The condition was initially assumed to involve hyperkeratosis of the eccrine ostia, and the disease was subsequently mislabeled “porokeratosis.”2 It is now commonly referred to as porokeratosis of Mibelli. Five clinical variants are currently recognized: porokeratosis of Mibelli (classic type), disseminated superficial porokeratosis and disseminated superficial actinic porokeratosis, porokeratosis palmaris et plantaris disseminate, linear porokeratosis, and punctate porokeratosis (Table 1).3-25 Several treatment modalities are available for the management of porokeratosis of Mibelli (Table 2). Therapeutic intervention depends on lesion size and location, as well as the aesthetic desires of the patient.9 Protection from sunlight, moisturizers and supported immune status may sufficiently suppress the disease. However, periodic observation and/or further treatment may be recommended due to the potential risk of malignant transformation.3,20 Topical therapies include 5-fluorouracil, imiquimod, salicylic acid, glucocorticoids and retinoids.3 Additional options include destruction of the lesion with cryotherapy, electrodissection, laser ablation and/or surgical excision.3,19-20
Several treatment modalities are available for the management of porokeratosis of Mibelli (Table 2). Therapeutic intervention depends on lesion size and location, as well as the aesthetic desires of the patient.9 Protection from sunlight, moisturizers and supported immune status may sufficiently suppress the disease. However, periodic observation and/or further treatment may be recommended due to the potential risk of malignant transformation.3,20 Topical therapies include 5-fluorouracil, imiquimod, salicylic acid, glucocorticoids and retinoids.3 Additional options include destruction of the lesion with cryotherapy, electrodissection, laser ablation and/or surgical excision.3,19-20
 Figure 2. Distant (left) and closer (right) views show complete resolution of porokeratosis of Mibelli following treatment with topical 5-fluorouracil. There are erythematous excoriation sites of recent arthropod assaults.
Figure 2. Distant (left) and closer (right) views show complete resolution of porokeratosis of Mibelli following treatment with topical 5-fluorouracil. There are erythematous excoriation sites of recent arthropod assaults.