


Unilateral Renal Artery Stenosis with Unusual Etiology in a Young Male Patient
VASCULAR DISEASE MANAGEMENT 2021;18(11):E209-E211
Abstract
Fibromuscular dysplasia (FMD) is commonly seen in young to middle-aged women involving medium-sized arteries with a classical beaded string appearance on angiogram. We present an unusual case of FMD in a young male patient with refractory hypertension and no apparent risk factors who presented with unifocal and unilateral renal artery stenosis with aneurysmal post-stenotic dilation.
Introduction
Renal artery stenosis (RAS) is a blockage or narrowing of one or both renal arteries. Common etiologies of RAS include atherosclerosis, fibromuscular dysplasia (FMD), thrombosis, embolism, renovascular hypertension, acute or chronic renal kidney injury, and external compression. In this case report, we discuss an unusual etiology of RAS with post-stenotic aneurysmal dilation in a young male patient with no apparent risk factors.
Procedure
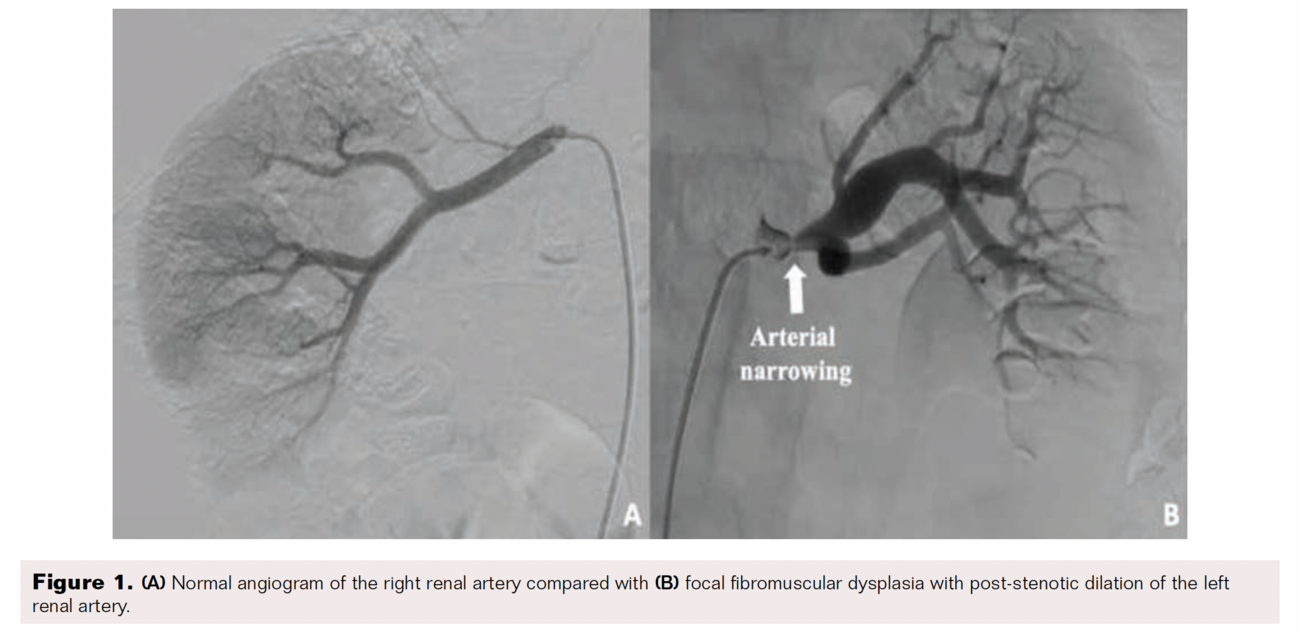
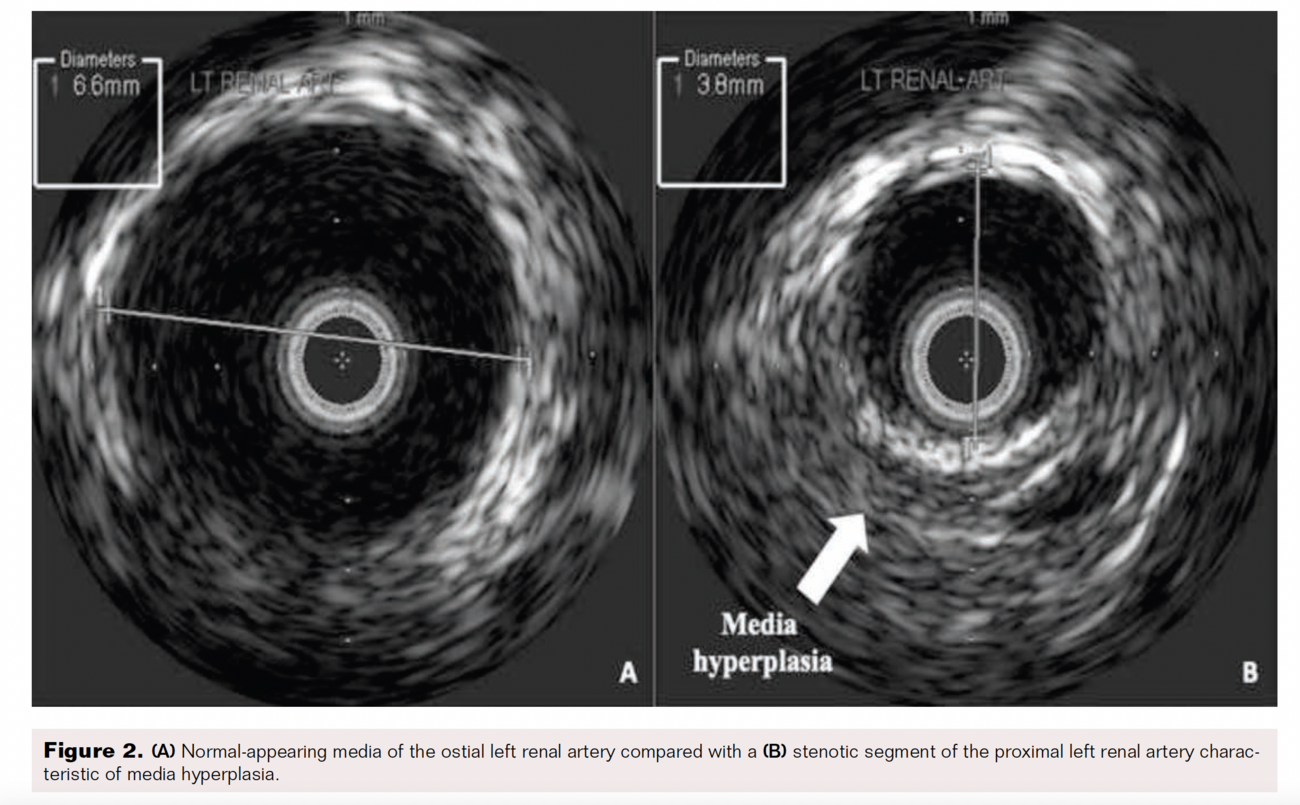
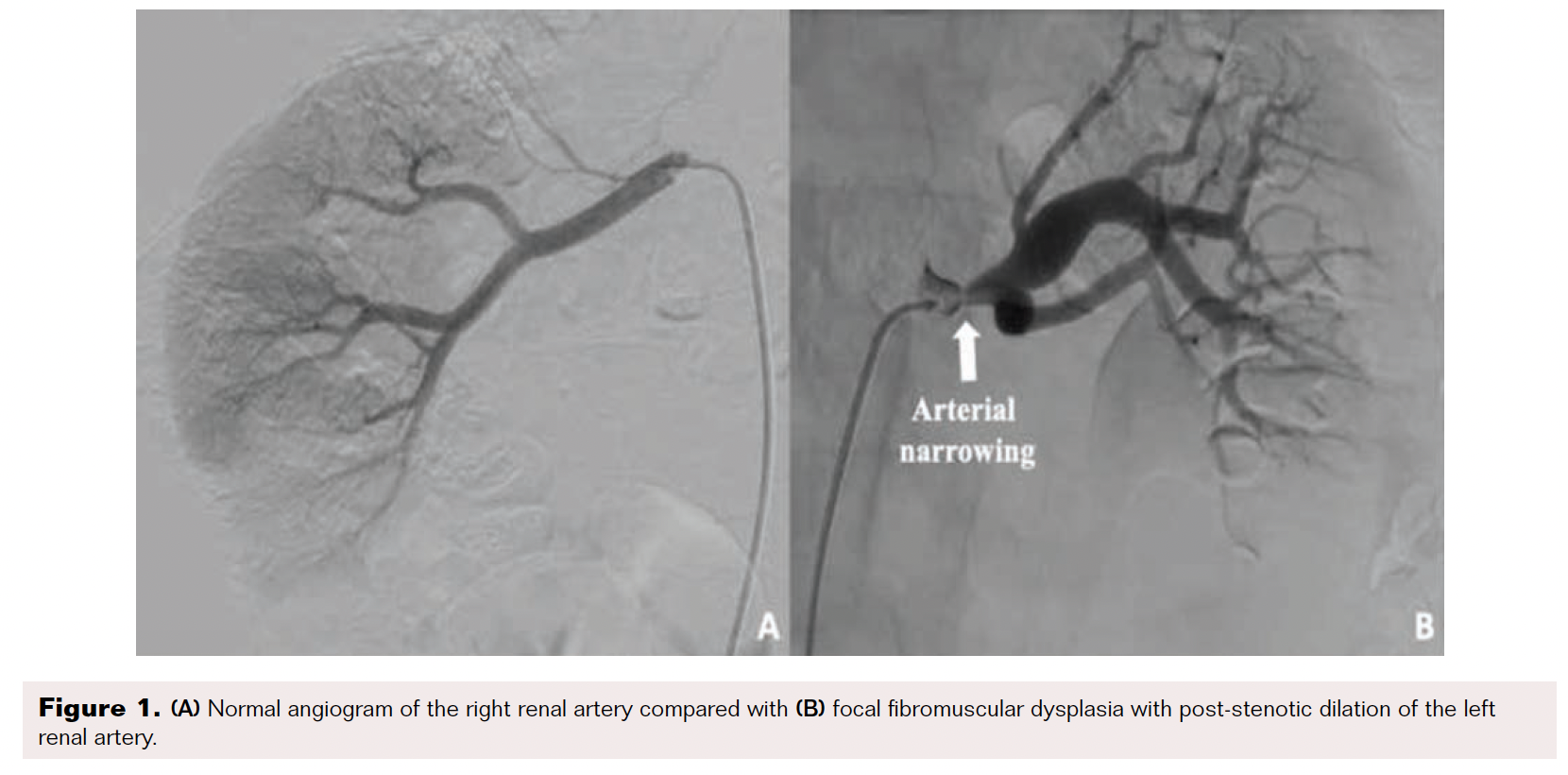
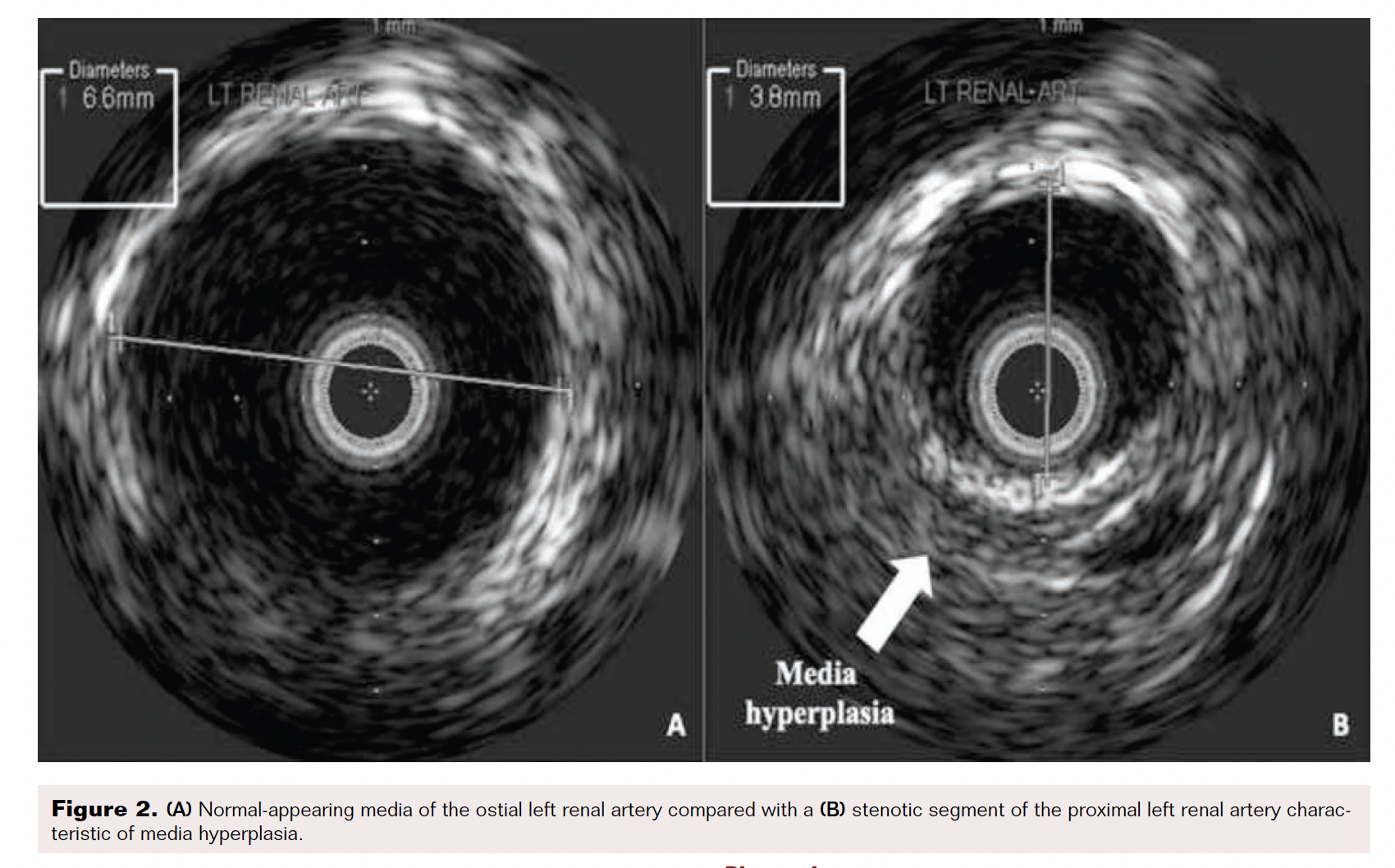
A 22-year-old man presented to the clinic with a new onset of elevated blood pressure ranging 130-150/80-90 mmHg. He denied a family history of hypertension, recent over-the-counter decongestant use, tobacco or illicit drug use, excessive alcohol intake, or a history of sleep apnea. His first elevated blood pressure was incidentally found 2 months earlier when he tested positive for SARS-CoV-2 and once more while donating blood plasma. The patient otherwise had no symptoms. He was started on amlodipine 10 mg once daily and telmisartan 80 mg once daily. At the 1-month follow-up, he continued to have unresolved hypertension, so chlorthalidone 25 mg once daily was added. His lab work showed renin activity elevated at 20 ng/mL/h with normal aldosterone. His metanephrine and thyroid-stimulating hormone/thyroxine levels were normal. His basic metabolic panel (BMP) showed elevated creatinine at 1.4 mg/dL and decreased sodium at 133 mmol/L but was otherwise unremarkable. A renal ultrasound Doppler revealed a normal proximal left main renal artery peak velocity at 105 cm/s; however, the mid-left main renal artery peak velocity was elevated at 312 cm/s, suggesting RAS. A computed tomography (CT) angiogram of the abdomen and pelvis showed smooth tapered narrowing at the proximal left renal artery, with peak narrowing measuring 2 to 2.5 mm in diameter approximately 8 mm distal to the ostium and at least moderate distal post-stenotic dilation. The remainder of the arteries, including an accessory artery to the right kidney, appeared to be normal bilaterally. The patient subsequently underwent angiography, which found discrete 80% stenosis in the left proximal renal artery and severe post-stenotic aneurysmal dilation (Figure 1). The right renal artery angiography was normal. Intravascular ultrasound showed no atherosclerotic plaque, web plexus, or calcification in the left renal artery (Figure 2). Balloon angioplasty of the left renal artery was performed using a 0.014" Hi-Torque All-Star guidewire (Abbott) and a 6 mm Viatrac balloon (Abbott) at 7 atm max pressure. An I.V. ultrasound was done using an Eagle Eye Platinum catheter (Philips). Post-intervention residual stenosis was noted at 20%. The patient was placed on aspirin 81 mg daily and clopidogrel 75 mg daily for 3 months. On a subsequent follow-up, the patient showed significant blood pressure improvement, and his medications were gradually stopped. His blood pressure normalized to 115–120/80 mmHg, and repeat lab values showed an unremarkable BMP and urinalysis.
Discussion
RAS is the largest cause of secondary hypertension, accounting for 25% to 35% of the disease.1 It is associated with worsening renal insufficiency, refractory heart failure, and flash pulmonary edema. Management of RAS depends on the etiology of the stenosis, with atherosclerosis (90%) and FMD (< 10%) accounting for most cases.2
FMD is a non-inflammatory and non-atherosclerotic vascular disease, most commonly impacting women ages 20 to 60, but may also present in children, men, and older adults.3 It typically impacts medium-sized vessels of the body, most commonly the renal arteries, vertebral arteries, and carotid arteries, but can also involve the mesenteric, external iliac, and brachial arteries.4 Although the cause of FMD is unknown, risk factors of FMD include genetics, smoking, hormonal factors, and disorders of the vasa vasorum.2 The clinical presentation of FMD depends on the arteries involved. When the renal arteries are involved, refractory hypertension may be present. Likewise, when the carotid arteries are involved, patients present with headaches, tinnitus, transient ischemic attacks, or strokes. FMD may also be found incidentally in asymptomatic patients on imaging for other clinical indications.
Diagnosis is made via CT angiography, and treatment with angioplasty generally yields favorable results. FMD typically presents in the medial and distal portion of the renal artery, where it is divided into multifocal/unifocal or tubular subtypes. The hallmark characteristic of the more common multifocal type is a “string of beads” appearance of the artery, suggesting fibrotic accumulations in the vessels followed by dilation or aneurysms of the arteries. The less common focal subtype appears as a single, smooth narrowing of the artery.
In the 2020 European/International FMD Registry and Initiative study with more than 1,000 FMD patients, a focal vs multifocal FMD subgroup analysis revealed that individuals with focal FMD were younger at diagnosis (39 ± 16 years vs 49 ± 15 years), presented earlier with hypertension (32 ± 15 years vs 39 ± 15 years), were more frequently male (31% vs 14%), and less likely to have multivessel involvement (16% vs 41%) and bilateral renal FMD (21% vs 41%).5 These findings support previously published data by Savard et al, where focal FMD was more common in men, diagnosed 20 years earlier than in women, less frequently involved bilateral vessels, and presented with higher blood pressures compared with multifocal FMD patients.6
Hypertension in multifocal FMD is managed with an average of two antihypertensive drugs.6 However, such is not the case with unifocal FMD, where revascularization with angioplasty results in better outcomes and dramatic improvements in blood pressure compared with multifocal FMD.7 In contrast, atherosclerotic RAS does not always respond well to angioplasty, with variable cure rates.8,9 Because the pathogenesis of FMD is different from atherosclerotic RAS, stent placement during angioplasty is not useful in FMD, whereas it shows superior results in the latter.9 Stent placement is typically used in FMD in the scenario of dissection during an angioplasty.10
Conclusion
Our patient falls in the smaller subset of patients with focal FMD. He is a young man with a single-vessel, unilateral renal artery involvement and an early presentation of severe hypertension. As seen in this case, it is important to recognize and identify the less common subtypes of FMD when treating and managing patients with hypertension.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript accepted September 1, 2021.
Address for correspondence: Gurpreet Baweja, MD, 1300 W. Terrell Ave., Suite 500, Fort Worth, TX 76104; Email: gurpreetbaweja@texashealth.org
REFERENCES
1. Benjamin MM, Fazel P, Filardo G, Choi JW, Stoler RC. Prevalence of and risk factors of renal artery stenosis in patients with resistant hypertension. Am J Cardiol. 2014;113:687-690.
2. Safian RD, Textor SC. Renal-artery stenosis. N Engl J Med. 2001;344:431-442.
3. Olin JW, Sealove BA. Diagnosis, management, and future developments of fibromuscular dysplasia. J Vasc Surg. 2011;53:826-836.
4. Slovut DP, Olin JW. Fibromuscular dysplasia. N Engl J Med. 2004;350:1862-1871.
5. Pappaccogli M, Di Monaco S, Warchoł-Celińska E, et al. The European/International Fibromuscular Dysplasia Registry and Initiative (FEIRI)—clinical phenotypes and their predictors based on a cohort of 1000 patients. Cardiovasc Res. 2021;117:950-959.
6. Savard S, Steichen O, Azarine A, Azizi M, Jeunemaitre X, Plouin PF. Association between 2 angiographic subtypes of renal artery fibromuscular dysplasia and clinical characteristics. Circulation. 2012;126:3062-3069.
7. Lüscher TF, Keller HM, Imhof HG, et al. Fibromuscular hyperplasia: extension of the disease and therapeutic outcome. Results of the University Hospital Zurich Cooperative Study on Fibromuscular Hyperplasia. Nephron 1986;44:109-114.
8. Burket MW, Cooper CJ, Kennedy DJ, et al. Renal artery angioplasty and stent placement: predictors of a favorable outcome. Am Heart J. 2000;139:64-71.
9. Watson PS, Hadjipetrou P, Cox SV, Piemonte TC, Eisenhauer AC. Effect of renal artery stenting on renal function and size in patients with atherosclerotic renovascular disease. Circulation. 2000;102:1671-1677.
10. Gornik HL, Persu A, Adlam D, et al. First International Consensus on the diagnosis and management of fibromuscular dysplasia. Vasc Med 2019;24:164-189.

