

Endovascular Management of Chronic Inferior Vena Cava and Iliac Vein Obstruction
Abstract
Chronic iliac vein and inferior vena cava (IVC) occlusion or stenosis due to deep vein thrombosis or non-thrombotic conditions is an important cause of venous outflow obstruction and may lead to post-thrombotic syndrome and chronic venous insufficiency, resulting in significant disability. Diagnosis requires a high clinical suspicion and intravascular ultrasound plays an important role. Percutaneous angioplasty and stenting has become the preferred treatment for IVC and iliac vein obstruction, providing symptom relief and clinical improvement with encouraging early and intermediate outcomes. IVC filter occlusion may contribute to venous outflow obstruction and is not a contraindication to percutaneous treatment.
VASCULAR DISEASE MANAGEMENT 2012;9(3):E33–E38
____________________________________________
Until recently, treatment of lower extremity venous insufficiency and post-thrombotic syndrome focused on compression therapy and surgical interventions such as vein stripping, ablation, and phlebectomy aimed at addressing superficial vein reflux. However, venous outflow obstruction from occlusion, stenosis, or compression of the inferior vena cava (IVC) and iliac veins is an important and treatable cause of venous hypertension and chronic venous insufficiency (CVI) in many patients. Chronic venous outflow obstruction caused by deep vein thrombosis (DVT) results in a collection of symptoms called post-thrombotic syndrome (PTS) that includes chronic lower extremity edema, pain, and skin changes. Over 5% of the U.S. population is affected by PTS, which is a substantial cause of disability and reduced quality of life. Non-thrombotic processes caused by compression (ie, May-Thurner Syndrome, tumors, retroperitoneal fibrosis) may be equally important causes of symptomatic venous outflow obstruction.
Irrespective of the cause of venous outflow obstruction, endovascular intervention with percutaneous angioplasty and stenting has become the treatment method of choice. Percutaneous techniques are now preferred over surgical bypass because the percutaneous approach is safe with consequent low morbidity, affords good patency rates, and provides consistent and reliable clinical improvement in the majority of patients. The diagnosis and endovascular treatment of venous outflow obstruction due to chronic IVC and iliac vein occlusions is the focus of this review.
Post-Thrombotic (Secondary) Obstruction
Chronic iliac vein obstruction and occlusion are well known consequences of acute iliofemoral DVT. Although endovascular treatment of acute DVT is becoming more widely practiced, a majority of patients with acute DVT are managed with an initial course of heparin followed by 3-6 months of oral anticoagulant therapy. DVT can lead to PTS through 2 primary mechanisms: 1) persistent iliofemoral obstruction or occlusion and 2) valvular incompetence. Though early recanalization of thrombus may occur,1 70%-80% of patients with thrombosed iliac veins will have persistent partial obstruction or occlusion.2 Following the acute insult, DVTs can lead to dilation of the venous system and valve destruction in the deep and superficial system. Though valvular destruction is not attributed to thrombus itself,1 early recanalization is associated with preservation of valve integrity. Protection against both persistent obstruction and valvular incompetence is the basis for early treatment of acute proximal lower extremity DVT with catheter-directed lytic therapy and percutaneous mechanical thrombectomy.1,3 The integrity of popliteal vein valves is particularly important in preventing post-thrombotic syndrome and leg ulceration.4 In addition to causing valvular incompetence, persistent obstruction is also known to have a detrimental effect on the calf-muscle pump function, further predisposing patients to ambulatory venous hypertension.2,5
These hemodynamic effects lead to the development of PTS in 28%-40% of patients who have acute DVT,6,7 a constellation of symptoms that may manifest slowly many years following the initial DVT. Persistent obstruction is sufficient to cause venous claudication, which may occur in as many as 44% of patients following acute iliofemoral DVT.8 Valvular incompetence is a larger contributor to ambulatory venous hypertension leading to the development of leg swelling and skin changes.2,3 Venous ulceration occurs in up to 15% of patients 5 years after acute DVT. The incidence and severity of PTS is affected by the location of the DVT and patients are more likely to develop PTS after a proximal or extensive lower extremity DVT. Moreover, patients with PTS have significantly diminished quality of life.8
Primary Disease
Primary (non-thrombotic) causes of obstruction such as external compression of the left common iliac vein by the right common iliac artery (May-Thurner syndrome) and intraluminal webs or bands are increasingly being found as contributing or causative factors in chronic venous disease (CVD). Evidence of anatomic compression may be present in up to 66% of the population9 and may lead to symptoms (May-Thurner syndrome) in a smaller proportion. Anatomic compression is a known risk factor for the development of iliofemoral DVT.10 Primary obstructing lesions, in the absence of DVT, were previously thought to be responsible for only 1%-5% of cases of CVD.10 However, a recent study utilizing intravascular ultrasound (IVUS) showed that of 938 limbs with CVD and proximal obstruction, 53% could be attributed to primary non-thrombotic lesions such as external compression or intravascular web, 40% were post-thrombotic, and 7% were a combination.11 Iliac vein obstruction can also be seen in patients with retroperitoneal fibrosis, pelvic tumors, or following radiation therapy.12,13 Overall, primary non-thrombotic lesions may be at least as important as post-thrombotic lesions in the development of iliac vein obstruction.
In both post-thrombotic and primary disease, a distinct proximal obstructing lesion that contributes to CVD can be identified. Prior to the recognition of the prevalence of these lesions, the most significant factor leading to the development of CVI was thought to be valvular incompetence. However, proximal obstruction has been found to contribute to a significant proportion of cases of CVI,11 offering a target for endovascular intervention.
Inferior Vena Cava Obstruction
Patients with IVC obstruction may have chronic symptoms but also may present with no symptoms or only mild symptoms due to the rich collateral network of veins that develops to bypass the obstructed IVC. IVC occlusions or stenoses are typically infrarenal and are rarely limited to the IVC alone. Distal extension into the common iliac vein or further is present in >90% of patients. As a result, 2/3 of patients experience unilateral limb symptoms and 1/3 experience bilateral limb symptoms.14 Thrombosis of an indwelling IVC filter is a common cause of IVC occlusion and represents a unique therapeutic challenge that is becoming more common as IVC filter placement becomes more common.
Diagnosis
A high clinical suspicion is vital in selecting patients with CVD who should have further testing for proximal obstruction. On presentation, patients should be evaluated on the Clinical, Etiologic, Anatomical, and Pathophysiological (CEAP) classification system15,16 to grade the severity of CVD. Aspects of a patient’s history that should prompt further evaluation for a proximal obstructing lesion include history of DVT, presence of severe symptoms not explained by superficial reflux alone, venous claudication, or unexplained lower extremity pain and swelling, especially when the thigh is involved. Other clues on physical exam include the presence of groin, suprapubic, or abdominal wall varices.
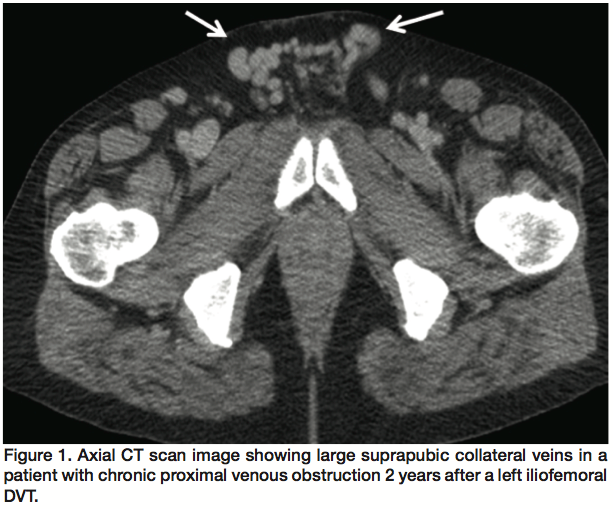
There is no single, reliable non-invasive test to diagnose hemodynamically significant proximal venous obstruction. Venous duplex ultrasonography is useful in evaluating the lower extremities but up to 1/4 of patients with CVD symptoms show little or no ultrasound abnormalities below the groin.17 This subset of patients in particular requires evaluation of the iliac veins and IVC where ultrasound is less reliable, especially in obese patients or due to overlying bowel gas. Computed tomography (CT) scans and magnetic resonance venography scans can be obtained to look for vascular asymmetry, presence of collateral veins, or masses (Figure 1). Though these studies can be very helpful,18 the lack of these findings does not rule out a flow-obstructing lesion. If a CT scan is obtained, delayed venous phase images should be requested for the most helpful diagnostic information.
Transfemoral venography is the historical gold standard and may be able to visualize iliofemoral occlusion or stenosis. Other suggestive features of stenosis on venography are filling of prominent collateral veins, though the absence of collaterals does not rule out obstruction. Contrast thinning or flattening (“pancaking”) may also be seen in areas of vein compression. However, due to the supine position of the patient, many lesions can be missed, resulting in a sensitivity of roughly 50%17 for transfemoral venography. Degree of stenosis can be underestimated by up to 30%.19 Intraluminal webs or bands may give a cribiform appearance with multiple small channels, but can often be obscured by contrast and underappreciated.
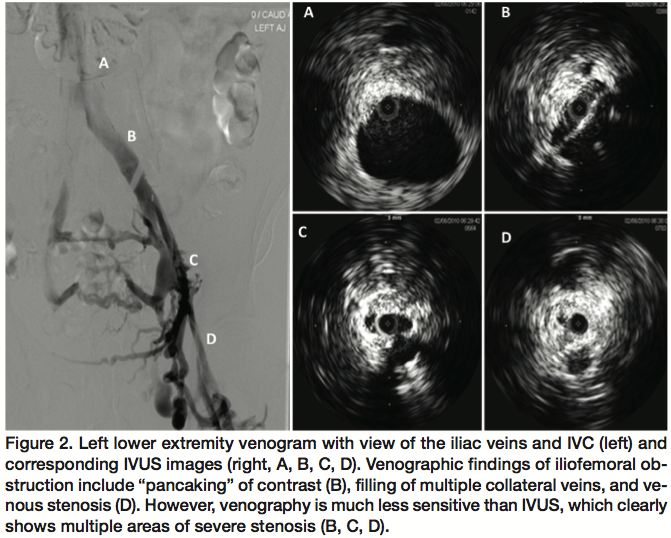
IVUS can reveal intraluminal and mural details not seen with venography and can also show the echogenicity of thrombus, which may correlate with its age (Figure 2). When compared to IVUS, venography has a sensitivity of 45% and negative predictive value of 49% in the assessment of >70% stenosis.19 With a diagnostic sensitivity of >90%, IVUS has become the method of choice in the diagnosis of iliocaval obstruction and furthermore allows for endovenous intervention during the same procedure.17 However, IVUS remains an invasive procedure and requires 9 Fr sheath access. Therefore, IVUS is usually reserved for instances when there is a high index of clinical suspicion for proximal venous obstruction or when non-invasive imaging is inconclusive in patients who are being considered for intervention.
Indications for Treatment
Patients who have severe CVD, indicated by a CEAP >3 (ie, edema, skin changes, active ulceration) and who have failed conservative therapy are candidates for endovascular intervention. Patients with venous claudication alone may also be candidates as this is highly suggestive of proximal venous obstruction. In 5%-10% of CVD patients, venous pain may be the sole manifestation of their disease. Consequently, some CEAP 0-2 patients may be considered candidates if they have significant venous pain.12,17 Patients should be appropriate candidates for general anesthesia and endovascular intervention.
Technique
Some physicians prefer to use general anesthesia when the potential for iliocaval stent placement exists because stent placement and dilatation can be painful,17 however we commonly perform these procedures under local anesthesia and sedation. We prefer to position the patient supine and to access the ipsilateral femoral vein at the level of the mid-thigh under ultrasound guidance.20 If the extent of thrombus precludes this approach, the patient can be positioned prone and the popliteal vein accessed. Access via the common femoral vein or great saphenous vein is generally avoided since this limits evaluation and treatment of occlusive disease involving the femoral vein. Jugular vein access may be used for treatment of IVC lesions, but evaluation and treatment of distal disease is also more difficult from this approach. An initial transfemoral venogram is obtained to evaluate the vascular anatomy; stenosis >60% is considered hemodynamically significant. IVUS is used routinely to evaluate the intramural and luminal anatomy as well as the characteristics of any apparent thrombus. Extrinsic compression of the iliac vein and intraluminal webs/bands are reliably well visualized with IVUS.
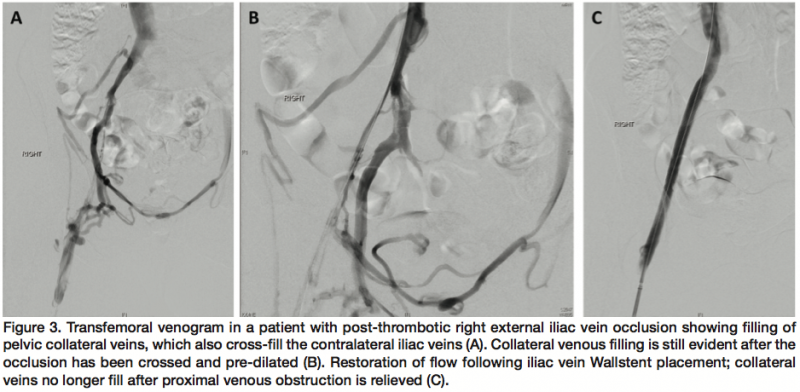
In contrast to arterial techniques, endovenous intervention utilizes torqueable, pushable catheters in combination with stiff glide wires. Stiff glide wires with supporting catheters are typically manipulated until an appropriate channel is entered, at which point the wire can be looped and advanced.20 In cases of iliofemoral occlusion, dilation should not be attempted until the lesion is crossed. Otherwise, a cavity will be created, which wires will tend to curl in rather than advance.21 Once the lesion is crossed, we recommend pre-dilation to allow stent delivery. Repeated dilation at anatomic choke points may be necessary.21 Stents are mandatory in the treatment of iliac vein and IVC occlusion (Figure 3). We typically employ 12-16 mm Wallstents (Boston Scientific) in the iliac vein. If stenting in the common iliac vein, the most proximal stent should extend 3-4 cm into the IVC to avoid distal stent migration with time.5,12,17 “Kissing” iliac stents are not necessary as contralateral iliac vein flow is rarely affected, though contralateral iliac thrombosis has been reported.12 It is essential to stent across the entire area of disease, avoiding skip areas, which may become stenotic if left untreated. Stenting across the inguinal ligament into the common femoral vein is acceptable in order to treat the entire area of disease and has not been associated with increased rate of complications.17 We recommend overlapping stents by >2 cm to prevent separation with dilation.22 Dilation should be repeated following stent placement, but not until all stents are in place.21 Primary non-thrombotic processes are easily crossed and 12-16 mm Wallstents should also always be employed in their treatment.11 Repeat transfemoral venography should show brisk flow through the stent and a decrease in the amount of collateral venous flow. We also recommend completion IVUS to assess for stent expansion and apposition.
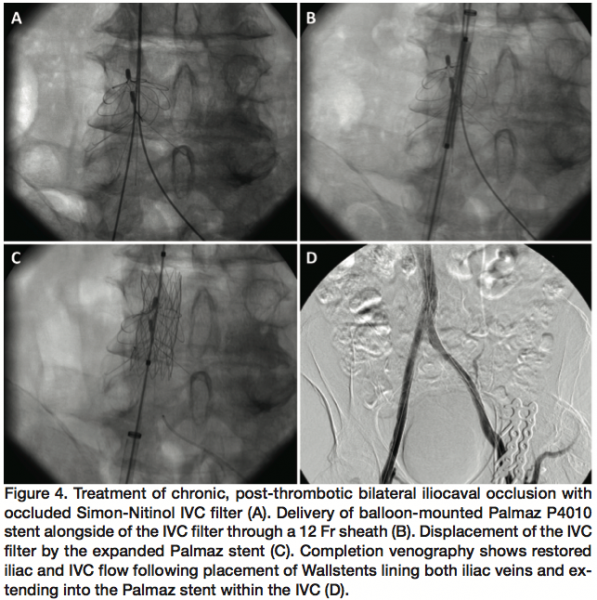
For IVC occlusions or stenosis, we typically employ 18-24 mm Wallstents. Again, the entire diseased segment should be covered. In the event that the occlusion is caused by a thrombosed IVC filter, a wire should be used to cross the thrombosis between the vessel wall and IVC filter, or through the filter itself. Pre-dilatation up to 16-18 atm can be safely attempted to displace or fracture the IVC filter. A Wallstent can then be deployed through the newly created flow channel.14,23 We have also used Palmaz P4010 or P3110 balloon expandable stents (Cordis) to displace occluded IVC filters and reestablish a flow channel, usually in combination with Wallstents (Figure 4).
While thrombolysis and mechanical thrombectomy have a central role in the interventional treatment of acute DVT, these modalities have little to no role in the management of chronic iliac and caval occlusions. An exception may be a small subset of patients with “acute-on-chronic” proximal DVT, where pharmomechanical catheter-directed thrombolysis should be employed to eliminate the acute thrombus component prior to stent placement. Patients with an acute exacerbation of symptoms may have acute thrombus present, which is confirmed by easy passage of the guidewire across an occlusion and venography, showing filling defects.
Anticoagulation
While the use of intraoperative heparin is widely accepted, postoperative anticoagulation and antiplatelet regimens differ.5,21 We give intravenous heparin during our intervention and recommend anticoagulation with warfarin for 6 months following the placement of iliofemoral or IVC stents. We do not recommend additional antiplatelet agents following venous stent placement as any thrombus that forms is typically platelet-poor. If a patient is already being treated with warfarin at the time of presentation, it is not discontinued prior to stent placement. All patients with chronic iliocaval obstruction due to thrombus should undergo medical workup for hypercoagulability including antithrombin 3, protein C and S deficiencies, anticardiolipin antibody, lupus anticoagulant, prothrombin, MTHFR, and factor V Leiden gene mutations as well as a screen for hyperhomocysteinemia.21 If a hypercoagulable state is identified, lifelong anticoagulation is recommended.
Outcomes
A number of centers have reported small series of patients who have undergone iliocaval stent placement for post-thrombotic and/or primary occlusion. Reported primary patency rates for stents placed for post-thrombotic occlusion are variable, ranging from 61%-83% at 1-year follow-up24,25 and 67% at 2-years follow-up. In a larger series of 982 lesions, which included all etiologies of iliocaval obstructions, primary patency rates following stenting of primary non-thrombotic occlusion were reported to be 79% compared to 57% for post-thrombotic occlusions at 72 months follow-up.12 Stents placed for primary disease have consistently superior patency rates. Other studies have similarly shown that iliac stenting is safe and affords relatively good intermediate-term patency rates.26-31
In one of the largest studies to date, 870 patients with 982 chronic nonmalignant obstructive lesions of the iliocaval veins were stented with no mortality (<30 days). At 72 months follow-up, cumulative primary, primary-assisted, and secondary patency rates were 79%, 100%, and 100% for primary non-thrombotic obstruction, respectively, and 57%, 80%, and 86% for post-thrombotic obstructions, respectively. Stent occlusion occurred in 23 limbs at a median of 13 months postoperatively for an overall rate of 3%. The “kissing” iliac stent technique was not utilized and contralateral iliac vein thrombosis occurred in 1% of limbs (11 of 982). The cumulative rate of severe in-stent restenosis was 5% of limbs. Restenosis occurred more frequently in post-thrombotic occlusion (10%) when compared to primary non-thrombotic occlusion (1%, P=0.0253).12
Despite these promising intermediate results, longer-term results are not widely available. In a recently published study, 89 patients were treated endovascularly for iliocaval obstructive lesions (52 primary, 35 secondary, 2 congenital). Though the median follow-up was 38 months, the authors report primary, primary-assisted, and secondary patency rates of 83%, 89%, and 93% at 3 and 10-years follow-up, respectively.22
Chronic total occlusions of the iliac veins present a particular challenge for endovascular therapy and patients have typically been treated by venovenous bypass. In a report of 167 post-thrombotic total iliac occlusions, a technical success rate of 83% was achieved. During the 48-month follow-up period, 39 out of 139 stented limbs (28%) occluded. Seventeen of these patients had patency restored but 7 later re-occluded. The 4-year secondary stent patency was 66%.21
The treatment of chronic IVC obstructions has similarly encouraging outcomes. In a cohort of 97 patients with chronic symptoms (99 limbs), technical success was achieved in 100% of stenotic lesions and 66% of occlusions (14 out of 21). Cumulative primary and primary-assisted stent patency rates at 2 years were 58% and 82%, respectively. Four stents occluded during the follow-up period.14
When IVC obstructions are due to IVC filter thrombosis, displacing or fracturing the filter is recommended for stent placement. In a group of 25 patients with an obstructed IVC filter, the filter was displaced sideways or remodeled and an IVC stent was placed. In this group, 12% had postoperative thrombotic occlusion of their stent. At 54-month follow-up, primary and secondary patency rates in this group were 32% and 42%, repectively.23
Clinical studies have shown that a number of hemodynamic factors improve after iliocaval stent placement. In 16 patients (23 limbs) who underwent iliocaval stent placement, venous claudication was eliminated in all who were affected preoperatively (15 patients). Furthermore, there were improvements in calf muscle pump function, venous outflow, and CEAP status. However, venous reflux was noted to increase.5 It has also been shown that leg swelling and venous pain improve following stenting. An ulcer-healing rate of 62% at 2-years follow-up has been reported in a cohort of 304 limbs.32 Clinical results are excellent even when looking at patients with deep venous reflux as a significant component of their CVD, a group previously thought to be less responsive to treatment of an obstructive lesion.33 Quality of life significantly improves following stent placement as well.8
Conclusion
Most chronic iliofemoral vein and IVC occlusions can be percutaneously recanalized with low morbidity. Endovascular intervention is appropriate in selected patients with chronic venous insufficiency and significant symptoms. CT venography, MR venography, and IVUS should play an increasing role in the evaluation of patients with severe chronic venous insufficiency as these modalities are likely to identify patients who would benefit from endovascular intervention. The presence of an occluded IVC filter is not a contraindication to percutaneous revascularization. Intermediate primary patency rates are promising but long-term data is needed to assess the durability of this procedure. Development of large diameter stents specifically designed for treating proximal venous occlusive disease in the future may facilitate treatment and further improve outcomes.
References
- Killewich LA, Bedford GR, Beach KW, Strandness DE Jr. Spontaneous lysis of deep venous thrombi: rate and outcome. J Vasc Surg. 1989;9(1):89-97.
- Akesson H, Brudin L, Dahlström JA, Eklöf B, Ohlin P, Plate G. Venous function assessed during a 5 year period after acute ilio-femoral venous thrombosis treated with anticoagulation. Eur J Vasc Surg. 1990;4(1):43-48.
- Meissner MH, Manzo RA, Bergelin RO, Markel A, Strandness DE Jr. Deep venous insufficiency: the relationship between lysis and subsequent reflux. J Vasc Surg. 1993;18(4):596-605; discussion 606-608.
- Shull KC, Nicolaides AN, Fernandes é Fernandes J, et al. Significance of popliteal reflux in relation to ambulatory venous pressure and ulceration. Arch Surg. 1979;114(11):1304-1306.
- Delis KT, Bjarnason H, Wennberg PW, Rooke TW, Gloviczki P. Successful iliac vein and inferior vena cava stenting ameliorates venous claudication and improves venous outflow, calf muscle pump function, and clinical status in post-thrombotic syndrome. Ann Surg. 2007;245(1):130-139.
- Prandoni P, Lensing AW, Cogo A, et al. The long-term clinical course of acute deep venous thrombosis. Ann Intern Med. 1996;125(1):1-7.
- Kahn SR, Shrier I, Julian JA, et al. Determinants and time course of the postthrombotic syndrome after acute deep venous thrombosis. Ann Intern Med. 2008;149(10):698-707.
- Delis KT, Bountouroglou D, Mansfield AO. Venous claudication in iliofemoral thrombosis: long-term effects on venous hemodynamics, clinical status, and quality of life. Ann Surg. 2004;239(1):118-126.
- Kibbe MR, Ujiki M, Goodwin AL, Eskandari M, Yao J, Matsumura J. Iliac vein compression in an asymptomatic patient population. J Vasc Surg. 2004;39(5):937-943.
- Taheri SA, Williams J, Powell S, et al. Iliocaval compression syndrome. Am J Surg. 1987;154(2):169-172.
- Raju S, Neglén P. High prevalence of nonthrombotic iliac vein lesions in chronic venous disease: a permissive role in pathogenicity. J Vasc Surg. 2006;44(1):136-43; discussion 144.
- Neglén P, Hollis KC, Olivier J, Raju S. Stenting of the venous outflow in chronic venous disease: long-term stent-related outcome, clinical, and hemodynamic result. J Vasc Surg. 2007;46(5):979-990.
- Hartung O, Alimi YS, Di Mauro P, Portier F, Juhan C. Endovascular treatment of iliocaval occlusion caused by retroperitoneal fibrosis: late results in two cases. J Vasc Surg. 2002;36(4):849-852.
- Raju S, Hollis K, Neglén P. Obstructive lesions of the inferior vena cava: clinical features and endovenous treatment. J Vasc Surg. 2006;44(4):820-827.
- Bergan JJ, Schmid-Schönbein GW, Smith PD, Nicolaides AN, Boisseau MR, Eklof B. Chronic venous disease. N Engl J Med. 2006;355(5):488-498.
- Kistner RL, Eklof B, Masuda EM. Diagnosis of chronic venous disease of the lower extremities: the "CEAP" classification. Mayo Clin Proc. 1996;71(4):338-345.
- Raju S. Endovenous treatment of patients with iliac-caval venous obstruction. J Cardiovasc Surg (Torino). 2008;49(1):27-33.
- Marston W, Fish D, Unger J, Keagy B. Incidence of and risk factors for iliocaval venous obstruction in patients with active or healed venous leg ulcers. J Vasc Surg. 2011;53(5):1303-1308.
- Neglén P, Raju S. Intravascular ultrasound scan evaluation of the obstructed vein. J Vasc Surg. 2002;35(4):694-700.
- Raju S, McAllister S, Neglén P. Recanalization of totally occluded iliac and adjacent venous segments. J Vasc Surg. 2002;36(5):903-911.
- Raju S, Neglén P. Percutaneous recanalization of total occlusions of the iliac vein. J Vasc Surg. 2009;50(2):360-368.
- Hartung O, Loundou AD, Barthelemy P, Arnoux D, Boufi M, Alimi YS. Endovascular management of chronic disabling ilio-caval obstructive lesions: long-term results. Eur J Vasc Endovasc Surg. 2009;38(1):118-124.
- Neglén P, Oglesbee M, Olivier J, Raju S. Stenting of chronically obstructed inferior vena cava filters. J Vasc Surg. 2011;54(1):153-161.
- Wahlgren CM, Wahlberg E, Olofsson P. Endovascular treatment in postthrombotic syndrome. Vasc Endovascular Surg. 2010;44(5):356-360.
- AbuRahma AF, Perkins SE, Wulu JT, Ng HK. Iliofemoral deep vein thrombosis: conventional therapy versus lysis and percutaneous transluminal angioplasty and stenting. Ann Surg. 2001;233(6):752-760.
- O'Sullivan GJ, Semba CP, Bittner CA, et al. Endovascular management of iliac vein compression (May-Thurner) syndrome. J Vasc Interv Radiol. 2000;11(7):823-836.
- Knipp BS, Ferguson E, Williams DM, et al. Factors associated with outcome after interventional treatment of symptomatic iliac vein compression syndrome. J Vasc Surg. 2007;46(4):743-749.
- Oguzkurt L, Tercan F, Ozkan U, Gulcan O. Iliac vein compression syndrome: outcome of endovascular treatment with long-term follow-up. Eur J Radiol. 2008;68(3):487-492.
- Lamont JP, Pearl GJ, Patetsios P, et al. Prospective evaluation of endoluminal venous stents in the treatment of the May-Thurner syndrome. Ann Vasc Surg. 2002;16(1):61-64.
- Hartung O, Otero A, Boufi M, et al. Mid-term results of endovascular treatment for symptomatic chronic nonmalignant iliocaval venous occlusive disease. J Vasc Surg. 2005;42(6):1138-1144; discussion 1144.
- Hurst DR, Forauer AR, Bloom JR, Greenfield LJ, Wakefield TW, Williams DM. Diagnosis and endovascular treatment of iliocaval compression syndrome. J Vasc Surg. 2001;34(1):106-113.
- Raju S, Owen S Jr, Neglén P. The clinical impact of iliac venous stents in the management of chronic venous insufficiency. J Vasc Surg. 2002;35(1):8-15.
- Raju S, Darcey R, Neglén P. Unexpected major role for venous stenting in deep reflux disease. J Vasc Surg. 2010;51(2):401-408; discussion 408.
____________________________________________
From the Division of Vascular and Endovascular Surgery, New York Presbyterian Hospital, Weill Cornell Medical College, New York, New York.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted September 6, 2011, provisional acceptance given September 13, 2011, final version accepted October 11, 2012.
Address for correspondence: Darren B. Schneider, MD, New York Presbyterian Hospital, Weill-Cornell Medical Center, Division of Vascular and Endovascular Surgery, 525 East 68th Street, New York, New York, 10065, USA. Email: doj9016@gmail.com

