


Excimer Laser Atherectomy for Chronic Femoropopliteal Artery Occlusion Following Failed Femoropopliteal Bypass
VASCULAR DISEASE MANAGEMENT 2018;15(7):E67-E71
Abstract
Late prosthetic graft occlusions are a known complication of femoropopliteal bypass surgery. Patients with critical limb ischemia (CLI) necessitate immediate treatment to restore blood flow to the affected limb. We present a case of a 63-yearold patient originally treated with femoropopliteal bypass surgery using a polytetrafluoroethylene (PTFE) graft for chronic total occlusion (CTO) of the left superficial femoral artery (SFA), based on the TransAtlantic Inter-Society Consensus II guidelines (TASC II). The patient was subsequently admitted for CLI of left lower extremity due to occlusion of the prosthetic graft. Because of a high repeat operative risk secondary to multiple comorbidities and poor distal runoff, endovascular intervention was recommended. Excimer laser atherectomy (ELA) along with balloon angioplasty and stenting were used to achieve target-vessel revascularization. Following the procedure, the patient’s ischemic pain resolved completely. This case demonstrates promising results from an endovascular-first strategy with ELA for the treatment of TASC II C and D lesions following failed bypass surgery.
Peripheral artery disease (PAD) is a common manifestation of systemic atherosclerosis and is associated with significant long-term cardiovascular morbidity and mortality. The prevalence of PAD has increased significantly over the past several decades due to increased life expectancy along with the epidemic of other cardiovascular risk factors such as diabetes, and it is estimated to soon affect ≥30% of elderly patients.1,2
Patients with critical limb ischemia (CLI) are at high risk for major amputation and death within the first year after diagnosis.3 Such patients very frequently also suffer from other major comorbidities such as renal failure and diabetes mellitus.4 The current TASC II guidelines suggest an endovascular procedure as the treatment of choice for femoropopliteal occlusive lesions up to 10 cm long and surgical therapy for chronic total occlusions of the common femoral artery and SFA >20 cm.5 Long-term follow-up has demonstrated that nearly 50% of vascular reconstructions are subject restenosis or occlusion.6,7 The 5-year patency rate of the superficial femoral and popliteal artery bypass grafts have been reported to range between 50% to 70%.8,9
A significant complication of infrainguinal bypass is late prosthetic graft occlusions, often presenting as critical ischemia. Late graft occlusion should be treated only if the patient’s symptoms are severe enough to warrant intervention. Edwards et al suggested that late graft occlusions could be treated by establishing a new bypass with autogenous vein, which provides superior results and durability.10
Current TASC II guidelines recommend an “endovascular first” approach in patients with CLI, based on the potential risks and the anticipated success rate of interventional treatment options.11 Endovascular treatment techniques and devices have continued to improve, and endovascular treatment of PAD has exceeded surgery, with more TASC II grade C and D being addressed by an endovascular approach. A number of adjunctive techniques and devices have been developed to treat these more complex lesions. Among them, Excimer laser atherectomy (ELA) has been shown to be an effective treatment for CLI. Wissgott et al have reported recanalization rates of 90% with ELA.12
Case Report
We report here the case of a patient who presented with CLI due to occlusion of both native SFAs and bilateral prosthetic grafts. Excimer Laser Atherectomy (ELA) was used as the primary modality to revascularize this patient. Informed written consent was obtained from the patient prior to the creation of this case report.
This patient was a 63-year-old Asian man admitted to our institution with 3 days of Rutherford category 4 ischemic rest pain of left lower limb. Prior to presentation, the patient had been experiencing bilateral lower extremity intermittent claudication for approximately 8 years.
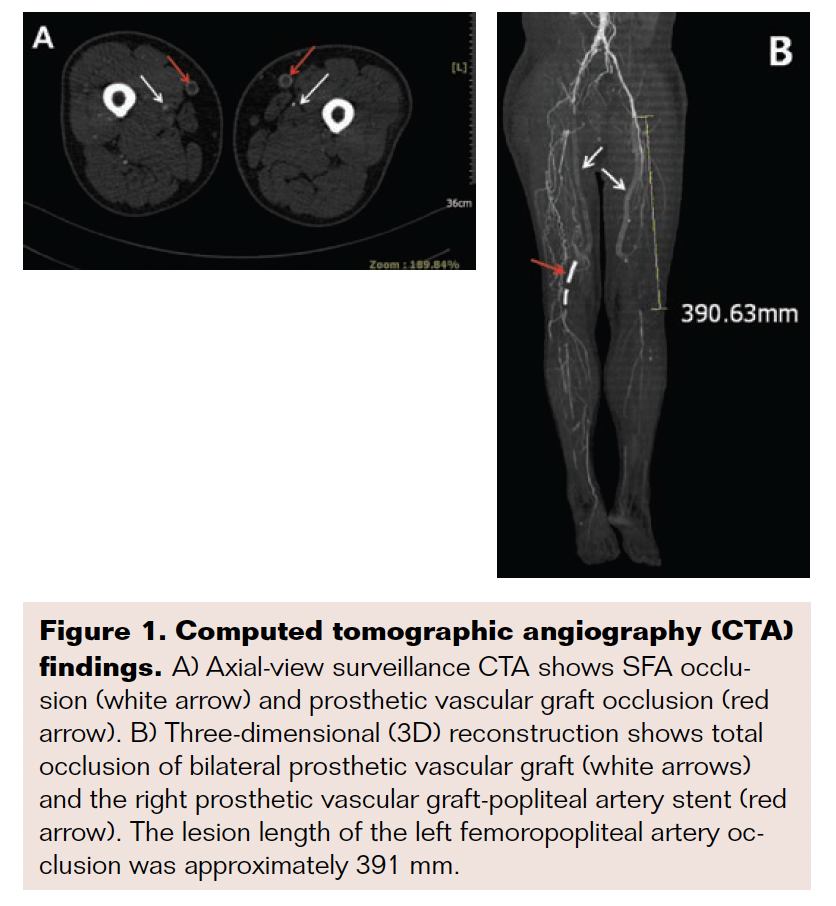 Past medical history included hypertension and coronary heart disease. Additional history included cerebral infarction and hypothyroidism controlled with levothyroxine. His major cardiovascular risk factor was smoking for 40 years (60 cigarettes/day). Past surgical history included cholecystectomy, bilateral femoropopliteal artery bypass grafting with polytetrafluroethylene (PTFE) and subsequent right-sided graft stenting 7 years ago. Physical examination revealed weak bilateral common femoral artery (CFA) pulses. Bilateral popliteal artery, posterior tibial artery, and dorsalis pedis artery pulses were absent. Laboratory test results were unremarkable except for an increase in the homocysteine (23.9 μmol/L) and triglyceride (3.41 mmol/L) value. Bilateral ankle-brachial index (ABI) was severely reduced at 0. Computed tomographic angiography (CTA) demonstrated severe stenosis of the left external iliac artery (EIA), occlusion of the right iliac and femoral arteries, and long total occlusion of both SFAs. There was also bilateral prosthetic vascular graft occlusion, as well as occlusion of the right graft stent. The posterior tibial artery (PTA) and the peroneal artery (PA) were partially occluded, and the anterior tibial artery (ATA) was totally occluded (Figure 1). Due to the history of failed bypass surgeries and multiple medical comorbidities, as well as the complexity of the lesions, the decision was made to revascularize the left leg with ELA rather than open surgical repair.
Past medical history included hypertension and coronary heart disease. Additional history included cerebral infarction and hypothyroidism controlled with levothyroxine. His major cardiovascular risk factor was smoking for 40 years (60 cigarettes/day). Past surgical history included cholecystectomy, bilateral femoropopliteal artery bypass grafting with polytetrafluroethylene (PTFE) and subsequent right-sided graft stenting 7 years ago. Physical examination revealed weak bilateral common femoral artery (CFA) pulses. Bilateral popliteal artery, posterior tibial artery, and dorsalis pedis artery pulses were absent. Laboratory test results were unremarkable except for an increase in the homocysteine (23.9 μmol/L) and triglyceride (3.41 mmol/L) value. Bilateral ankle-brachial index (ABI) was severely reduced at 0. Computed tomographic angiography (CTA) demonstrated severe stenosis of the left external iliac artery (EIA), occlusion of the right iliac and femoral arteries, and long total occlusion of both SFAs. There was also bilateral prosthetic vascular graft occlusion, as well as occlusion of the right graft stent. The posterior tibial artery (PTA) and the peroneal artery (PA) were partially occluded, and the anterior tibial artery (ATA) was totally occluded (Figure 1). Due to the history of failed bypass surgeries and multiple medical comorbidities, as well as the complexity of the lesions, the decision was made to revascularize the left leg with ELA rather than open surgical repair.
Procedural Details
An endovascular approach was planned under local anesthesia. Preplanned procedural steps included: 1) Transbrachial arterial access of left arm with reconstruction of the right iliofemoral artery blood flow. 2) Trans profunda femoral arterial access of right limb followed by reconstruction of the left iliac artery. 3) Left femoropopliteal artery intervention with ELA. Procedural details are as follows:
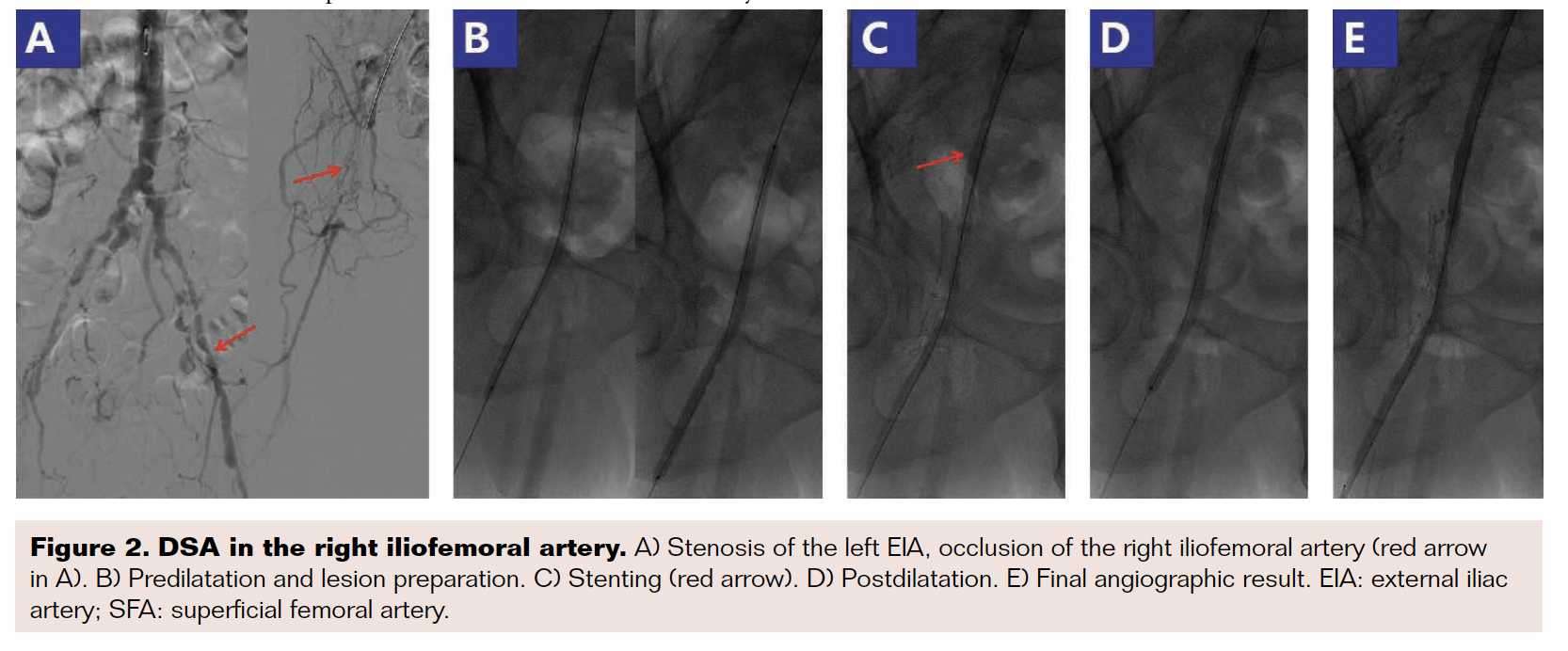 Left brachial arterial access was obtained with a 5F micropuncture kit (Cook Medical). A 0.035-inch × 150 cm Radiofocus angled soft hydrophilic guidewire (Terumo Medical) as well as a 5F pigtail catheter (Cordis) were then positioned at the infra-renal level for baseline aortoiliac angiography (Figure 2A). The pigtail catheter was then exchanged for a 6F × 90 cm Flexor Raabe Sheath (Cook Medical) with a 0.035-inch × 260 cm Radiofocus angled stiff hydrophilic guidewire (Terumo Medical). Several unsuccessful attempts were made to cross the intensely fibrous proximal cap of the right iliac occlusion using a 4F MPA catheter (Cordis), including using the stiff end of a 0.035" stiff hydrophilic guidewire. This system was then exchanged for a 0.035" Quick-Cross Support Catheter (Spectranetics) combined with a 0.035" stiff hydrophilic guidewire, which allowed for successful penetration of the proximal cap. After lesion crossing and confirmation of position in the true lumen, a 0.035" × 300 cm Supracore guidewire (Abbott Vascular) was advanced into the right profunda femoral artery. Pressure-only balloon angioplasty (POBA) was then performed using a 4.0 mm × 150 mm Pacific balloon (Medtronic Vascular) and 5.0 mm × 150 mm Admiral balloon (Medtronic Vascular) in the right iliofemoral artery (Figure 2B). An 8.0 mm × 80 mm Complete SE (Medtronic Vascular) self-expanding nitinol stent was placed in the right EIA and post-dilatated with a 6.0 mm × 150 mm Admiral balloon (Medtronic Vascular, Minneapolis, MN) (Figures 2C and D).
Left brachial arterial access was obtained with a 5F micropuncture kit (Cook Medical). A 0.035-inch × 150 cm Radiofocus angled soft hydrophilic guidewire (Terumo Medical) as well as a 5F pigtail catheter (Cordis) were then positioned at the infra-renal level for baseline aortoiliac angiography (Figure 2A). The pigtail catheter was then exchanged for a 6F × 90 cm Flexor Raabe Sheath (Cook Medical) with a 0.035-inch × 260 cm Radiofocus angled stiff hydrophilic guidewire (Terumo Medical). Several unsuccessful attempts were made to cross the intensely fibrous proximal cap of the right iliac occlusion using a 4F MPA catheter (Cordis), including using the stiff end of a 0.035" stiff hydrophilic guidewire. This system was then exchanged for a 0.035" Quick-Cross Support Catheter (Spectranetics) combined with a 0.035" stiff hydrophilic guidewire, which allowed for successful penetration of the proximal cap. After lesion crossing and confirmation of position in the true lumen, a 0.035" × 300 cm Supracore guidewire (Abbott Vascular) was advanced into the right profunda femoral artery. Pressure-only balloon angioplasty (POBA) was then performed using a 4.0 mm × 150 mm Pacific balloon (Medtronic Vascular) and 5.0 mm × 150 mm Admiral balloon (Medtronic Vascular) in the right iliofemoral artery (Figure 2B). An 8.0 mm × 80 mm Complete SE (Medtronic Vascular) self-expanding nitinol stent was placed in the right EIA and post-dilatated with a 6.0 mm × 150 mm Admiral balloon (Medtronic Vascular, Minneapolis, MN) (Figures 2C and D).
A 7F × 40 cm Flexor Balkin Sheath (Cook Medical, Bloomington, IN) was then inserted by retrograde puncture into the profunda femoral artery (PFA). Digital subtraction angiography (DSA) was then performed, which confirmed stenosis of the left ELA, flush occlusion of the left SFA, with no native vessels filling in the upper leg. The lesion of left ELA was then dilated using POBA with a 6.0 mm × 120 mm Admiral balloon (Medtronic Vascular) (Figure 3A).
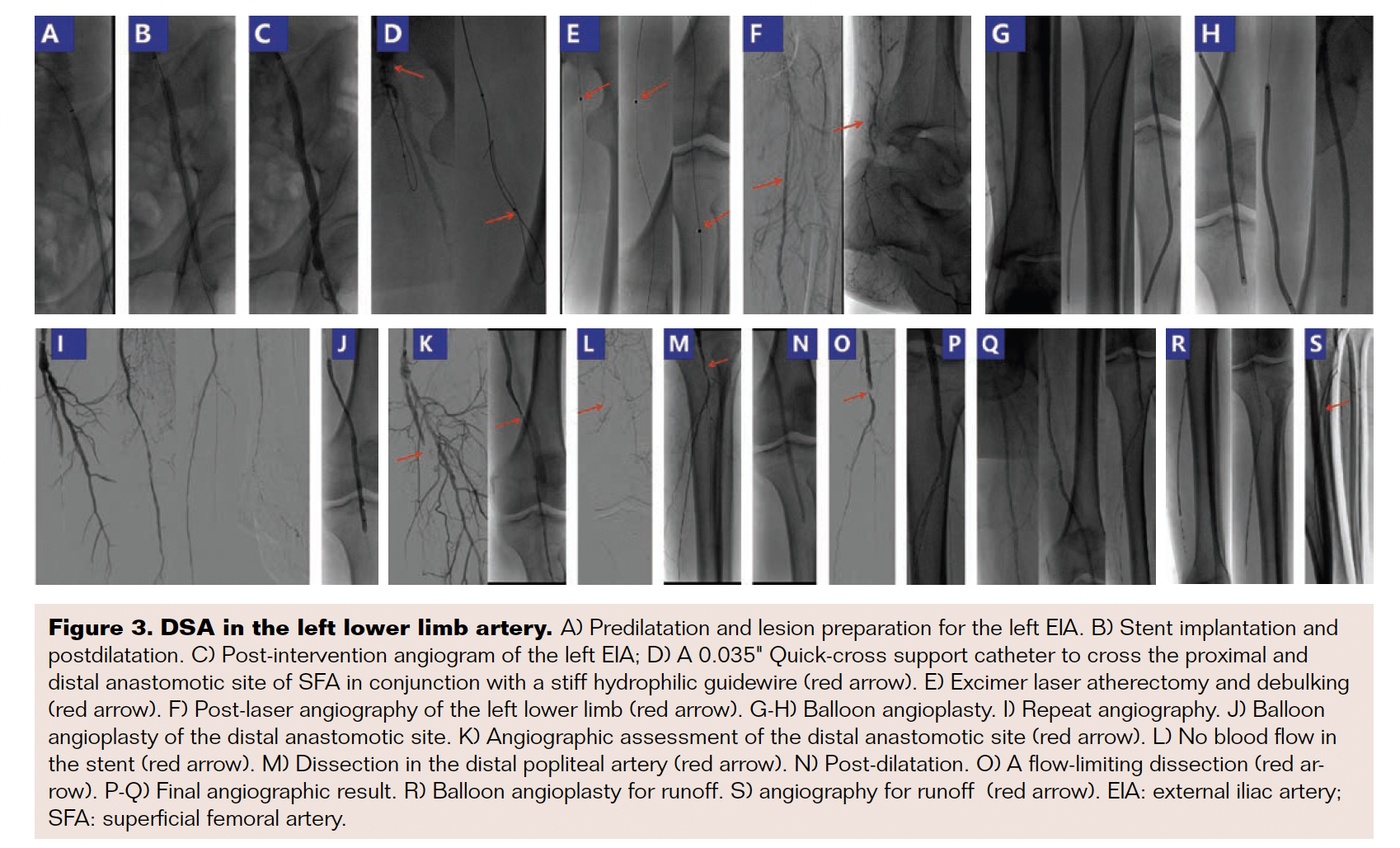 An 8 mm × 100 mm Complete SE (Medtronic Vascular) self-expanding nitinol stent was then deployed in the left EIA and post-dilated with a 7.0 mm × 80 mm Admiral balloon (Medtronic) (Figures 3B and C). A 0.035" Quick-Cross Support Catheter (Spectranetics) was then used to cross the proximal and distal anastomotic lesions of the native SFA in conjunction with a looped stiff hydrophilic guidewire (Figure 3D). The 0.035" wire was then exchanged a 0.018-inch × 300 cm V18 control wire. The CVX-300 Excimer Laser System (Figure 4) (wavelength: 308-nm) (Spectranetics) in conjunction with a 2.0-mm Turbo-Elite laser catheter (Spectranetics) was next used to debulk the SFA disease (Figure 3E). The catheter was slowly advanced through the lesion twice at a rate of 0.5 to 1 mm/second, with laser settings of 45mJ/ mm2/45HZ (Fluence/Frequency) and 50mJ/mm2/55HZ (Fluence/Frequency), respectively. The angiographic result is shown in Figure 3F. The lumen size obtained was approximately 1.5 times the size of the probe, necessitating adjunctive balloon angioplasty, including catheters ranging from diameters of 2 to 5 mm and lengths of 150 to 210 mm (Pacific/Admiral & Amphirion Deep, Medtronic Vascular) (Figures 3G, H, J, N, and R). Follow-up angiography demonstrated a flow-limiting dissection at the level of the old distal anastomosis (Figures 3K, M, and O). A 5 mm × 150 mm and a 5 mm × 60 mm Everflex self-expanding nitinol stent (Medtronic Vascular) was therefore deployed in the distal SFA and popliteal artery to address the dissection (Figures 3L and P). The final angiographic results are depicted in Figures 3Q and S. Perclose Proglide Suture-Mediated Closure System (Abbott Vascular) was used for hemostasis of the PFA access site.
An 8 mm × 100 mm Complete SE (Medtronic Vascular) self-expanding nitinol stent was then deployed in the left EIA and post-dilated with a 7.0 mm × 80 mm Admiral balloon (Medtronic) (Figures 3B and C). A 0.035" Quick-Cross Support Catheter (Spectranetics) was then used to cross the proximal and distal anastomotic lesions of the native SFA in conjunction with a looped stiff hydrophilic guidewire (Figure 3D). The 0.035" wire was then exchanged a 0.018-inch × 300 cm V18 control wire. The CVX-300 Excimer Laser System (Figure 4) (wavelength: 308-nm) (Spectranetics) in conjunction with a 2.0-mm Turbo-Elite laser catheter (Spectranetics) was next used to debulk the SFA disease (Figure 3E). The catheter was slowly advanced through the lesion twice at a rate of 0.5 to 1 mm/second, with laser settings of 45mJ/ mm2/45HZ (Fluence/Frequency) and 50mJ/mm2/55HZ (Fluence/Frequency), respectively. The angiographic result is shown in Figure 3F. The lumen size obtained was approximately 1.5 times the size of the probe, necessitating adjunctive balloon angioplasty, including catheters ranging from diameters of 2 to 5 mm and lengths of 150 to 210 mm (Pacific/Admiral & Amphirion Deep, Medtronic Vascular) (Figures 3G, H, J, N, and R). Follow-up angiography demonstrated a flow-limiting dissection at the level of the old distal anastomosis (Figures 3K, M, and O). A 5 mm × 150 mm and a 5 mm × 60 mm Everflex self-expanding nitinol stent (Medtronic Vascular) was therefore deployed in the distal SFA and popliteal artery to address the dissection (Figures 3L and P). The final angiographic results are depicted in Figures 3Q and S. Perclose Proglide Suture-Mediated Closure System (Abbott Vascular) was used for hemostasis of the PFA access site.
 The postoperative course was uneventful, and the patient was discharged on the sixth postoperative day. Discharge medications included 100 mg aspirin, 75 mg clopidogrel, and 20 mg atorvastatin daily, as well as 250 LSU sulodexide twice a day. At the 14-day follow-up appointment, the patient remained asymptomatic and his absolute walking distance improved from 0 m (rest pain) to 1000 m. His left ABI was greatly improved at 0.91, while the right ABI still was unchanged at 0.
The postoperative course was uneventful, and the patient was discharged on the sixth postoperative day. Discharge medications included 100 mg aspirin, 75 mg clopidogrel, and 20 mg atorvastatin daily, as well as 250 LSU sulodexide twice a day. At the 14-day follow-up appointment, the patient remained asymptomatic and his absolute walking distance improved from 0 m (rest pain) to 1000 m. His left ABI was greatly improved at 0.91, while the right ABI still was unchanged at 0.
Discussion
Bypass surgery is a well-established treatment for infrainguinal chronic occlusions and is considered to be the standard of therapy.13 However, late graft occlusion is one of the major known complications after bypass surgery. Progressive atherosclerosis is a significant cause of the late failure, particularly more than 1 year postprocedure.14 Our case report illustrated endovascular treatment (ET) employing ELA in CTO-PTA of the femoropopliteal artery following failed bypass grafting.
CLI is associated with high amputation and mortality rates, depending on concomitant risk factors and treatment options.15 Pomposelli et al16 reported 10 years of bypass grafting in 1032 patients with severe limb ischemia at the 5-year and 10-year limb salvage rates of 78.1% and 59.8%, respectively. Many CLI patients present as unsuitable surgical candidates due to poor conduit, poor distal runoff, and high operative risk secondary to other comorbidities. For these reasons, an endovascular-first approach is being used more frequently in treating CLI.17 ET is frequently chosen because of lower rates of morbidity and mortality in the perioperative period. In this case, a long femoropopliteal CTO was present along with stenosis of the left EIA, occlusion of the right iliofemoral artery, partial stenosis of PTA and PA, and occlusion of the ATA.
Despite the complexity of the disease, we chose ET due to prior failed bypass surgery and multiple medical comorbidities. Lesion crossing and recanalization of CTOs in the femoropopliteal arteries is often challenging. We elected to employ debulking and recanalization using ELA, which has proved to be a useful adjunct for the management of long SFA occlusions.18 The ELA technique achieves debulking of the atherosclerotic plaque by photochemical, photomechanical, and photothermal effects at the tip of the catheter. High success rates of recanalization, even in long symptomatic SFA occlusions, have been demonstrated in large earlier trials. Potential advantages of laser atherectomy include the ability to treat long occlusions and complex disease effectively, thereby providing a better angiographic result and less need for stenting. Endovascular intervention has been associated with limb salvage rates up to 93% at 6 months19 with an immediate clinical success rate of 88.2%. The patency rates of the successfully treated lesions (freedom from target lesion revascularization) were 96.6% at 12 months and 82.7% at 24 months. The expected limb-salvage rates at 12 and 24 months are 100% and 94%, respectively.20 With the increased use of an endovascular-first strategy, ELA has shown promising results with excellent technical success rates and low complication rates in the treatment of TASC C and D lesions.12
In contrast to other reports in the literature, the disease in our patient was more complex, including not only the left femoropopliteal CTO, but also diseased run-off vessels and occlusion of the right iliofemoral system. Therefore, we decided to establish the left brachial arterial access to open the right iliofemoral artery occlusion and then establish PFA access to intervene in the left lower limb artery. Self-expanding nitinol stents were placed in the right EIA and left EIA, respectively. We used ELA to debulk and ablate tissue (thrombus or plaque) of the femoropopliteal artery and remodelled the vessel lumen. However, DSA showed that the left distal anastomotic site was severely stenosed and that the distal popliteal artery had a flow-limiting dissection. Due to stenosis and flow-limiting dissection, 2 bail-out self-expanding nitinol stents were placed.
Dissections after ELA may occur for a number of reasons.12 Laser action may result in high energy shock waves and cavitation if contrast is used to flush the catheter. Therefore, saline flushing prior to and during laser activation is mandatory. Second, a dissection due to an earlier intervention may be reopened during laser recanalization. Third, the advancement of the excimer laser has to be performed very slowly at <1 mm/second to allow real photoablation. Rapid advancement may result in “Dottering” the occlusion without plaque ablation.
In this case example, the final angiographic result was quite satisfactory. This case demonstrates that ELA approach may be valuable and ultimately successful even in very long, complex occlusive lesions. We have demonstrated that excimer laser atherectomy-assisted angioplasty is safe and effective as a first-line endovascular treatment of CLI. Based on this result, we believe that large scale randomized studies addressing this complex femoropopliteal should be encouraged.
Acknowledgement
The authors acknowledge Craig M. Walker, MD, of Cardiovascular Institute of the South, Tulane University School of Medicine, New Orleans, Louisiana, and Richard C Kovach, MD, of Deborah Heart and Lung Center of Browns Mills, NJ. The authors also acknowledge support by Spectranetics. FUNDING The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest and report report no conflicts of interest regarding the content therein.
Manuscript submitted on May 5, 2018; accepted on June 14, 2018.
Address for correspondence: Ju He, MD, Department of Vascular Surgery, Nankai, University Affiliated First Central Hospital, No. 24, Fukang Road, Nankai District, Tianjin, 300192, China. Email: tfhvascular@sina.cn
REFERENCES
1. Gallino A, Aboyans V, Diehm C, et al. Non-coronary atherosclerosis. Eur Heart J. 2014;35(17):1112-1119.
2. Fowkes FG, Rudan D, Rudan I, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013;382(9901): 1329-1340.
3. Bradbury AW, Adam DJ, Bell J, et al. BASIL trial Participants. Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial: an intention-to-treat analysis of amputation-free and overall survival in patients randomized to a bypass surgery-first or a balloon angioplasty-first revascularization strategy. J Vasc Surg. 2010; 51(5 Suppl):5S-17S.
4. Malyar N, Fürstenberg T, Wellmann J,et al. Recent trends in morbidity and in-hospital outcomes of in-patients with peripheral arterial disease: a nationwide population-based analysis. Eur Heart J. 2013;34(34): 2706-2714.
5. Norgren L, Hiatt WR, Dormandy JA, et al. InterSociety Consensus for the Management of Peripheral Arterial Disease (TASC II ). Eur J Vasc Endovasc Surg. 2007;33 Suppl 1:S1–S75.
6. Darling RC 3rd, Chang BB, Shah DM, et al. Choice of peroneal or dorsalis pedis artery bypass for limb salvage. Semin Vasc Surg. 1997;10(1):17-22.
7. Desiron Q, Detry O, Van Damme H, et al. Comparison of results of carotid artery surgery after either direct closure or use of a vein patch. Cardiovasc Surg. 1997;5(93):295-303.
8. Klinkert P, Schepers A, Burger DH, et al.Vein versus polytetrafluoroethylene in above-knee femoropopliteal bypass grafting: five-year results of a randomized controlled trial. J Vasc Surg. 2003;37(1):149-166.
9. Nolan B, Finlayson S,Tosteson A, et al.The treatment of disabling intermittent claudication in patients with superficial femoral artery occlusive disease--decision analysis. J Vasc Surg. 2007;45(6):1179-1184.
10. Edwards JE, Taylor Jr LM, Porter JM.Treatment of failed lower extremity bypass grafts with new autogenous vein bypass grafting. J Vasc Surg. 1990;11(1):136-144.
11. European Stroke Organization, Tendera M, Aboyans V, et al. ESC Committee for Practice Guidelines. ESC Guidelines on the diagnosis and treatment of peripheral artery diseases: document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries: the Task Force on the Diagnosis and Treatment of Peripheral Artery Diseases of the European Society of Cardiology (ESC). Eur Heart J. 2011;32(22): 2851-906.
12. Wissgott C, Kamusella P, Lüdtke C, Andresen R. Excimer laser atherectomy after unsuccessful angioplasty of TASC C and D lesions in femoropopliteal arteries. J Cardiovasc Surg (Torino). 2013; 54(3):359–365.
13. Dormandy JA, Rutherford RB. Management of peripheral arterial disease (PAD). TASC Working Group. TransAtlantic Inter-Society Consensus (TASC). J Vasc Surg. 2000;31(1 Pt 2):S1–S296.
14. Lumsden AB, Rice TW, Chen C, et al. Peripheral arterial occlusive disease: magnetic resonance imaging and the role of aggressive medical management. World J Surg. 2007;31(4):695-704.
15. Golomb BA, Dang TT, Criqui MH. Peripheral arterial disease: morbidity and mortality implications. Circulation. 2006;114(7): 688-699.
16. Pomposelli FB, Kansal N, Hamdan AD, et al. A decade of experience with dorsalis pedis artery bypass: analysis of outcome in more than 1000 cases. J Vasc Surg. 2003;37(2):307-315.
17. Walker CM, Mustapha J, Zeller T, et al. Tibiopedal access for crossing of infrainguinal artery occlusions: a prospective multicenter observational study. J Endovasc Ther. 2016;23(6):839-846.
18. Scheinert D, Laird Jr JR, Schröder M, Steinkamp H, Balzer JO, Bi-amino G. Excimer laser-assisted recanalization of long, chronic superficial femoral artery occlusions. J Endovasc Ther. 2001;8(2):156-166.
19. Laird JR, Zeller T, Gray BH, et al. Limb salvage following laser-assisted angioplasty for critical limb ischemia: results of the LACI multicenter trial. J Endovasc Ther. 2006;13(1):1-11.
20. Serino F, Cao Y, Renzi C, et al. Excimer laser ablation in the treatment of total chronic obstructions in critical limb ischaemia in diabetic patients. Sustained efficacy of plaque recanalisation in mid-term results. Eur J Vasc Endovasc Surg. 2010;39(2):234-238.
